
Effects of Physical Exercises Alone on the Functional Capacity of Individuals with Obesity and Knee Osteoarthritis: A Systematic Review
 , ,
, ,  ,
,  ,
,  ,
, 
Abstract
Simple Summary
Abstract
1. Introduction
2. Material and Methods
2.1. Protocol and Registration
2.2. Research Question
2.3. Inclusion and Exclusion Criteria
2.4. Search Strategies
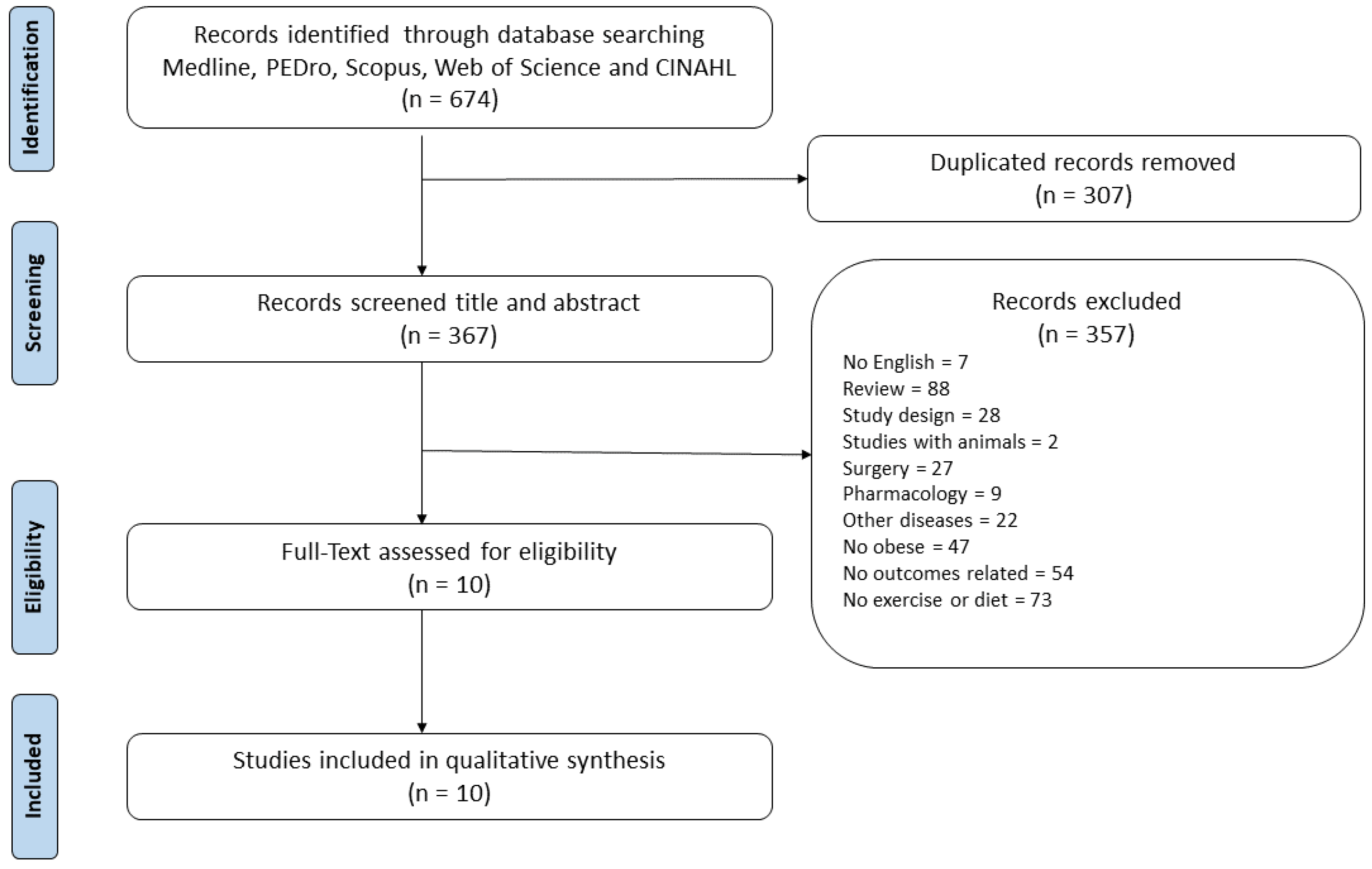
2.5. Study Selection
2.6. Methodological Quality, Risk of Bias and Levels of Evidence (LE) of the Selected Papers
2.7. Data Synthesis
3. Results
3.1. Study Population
Interventions
3.2. Functional Capacity Assessments
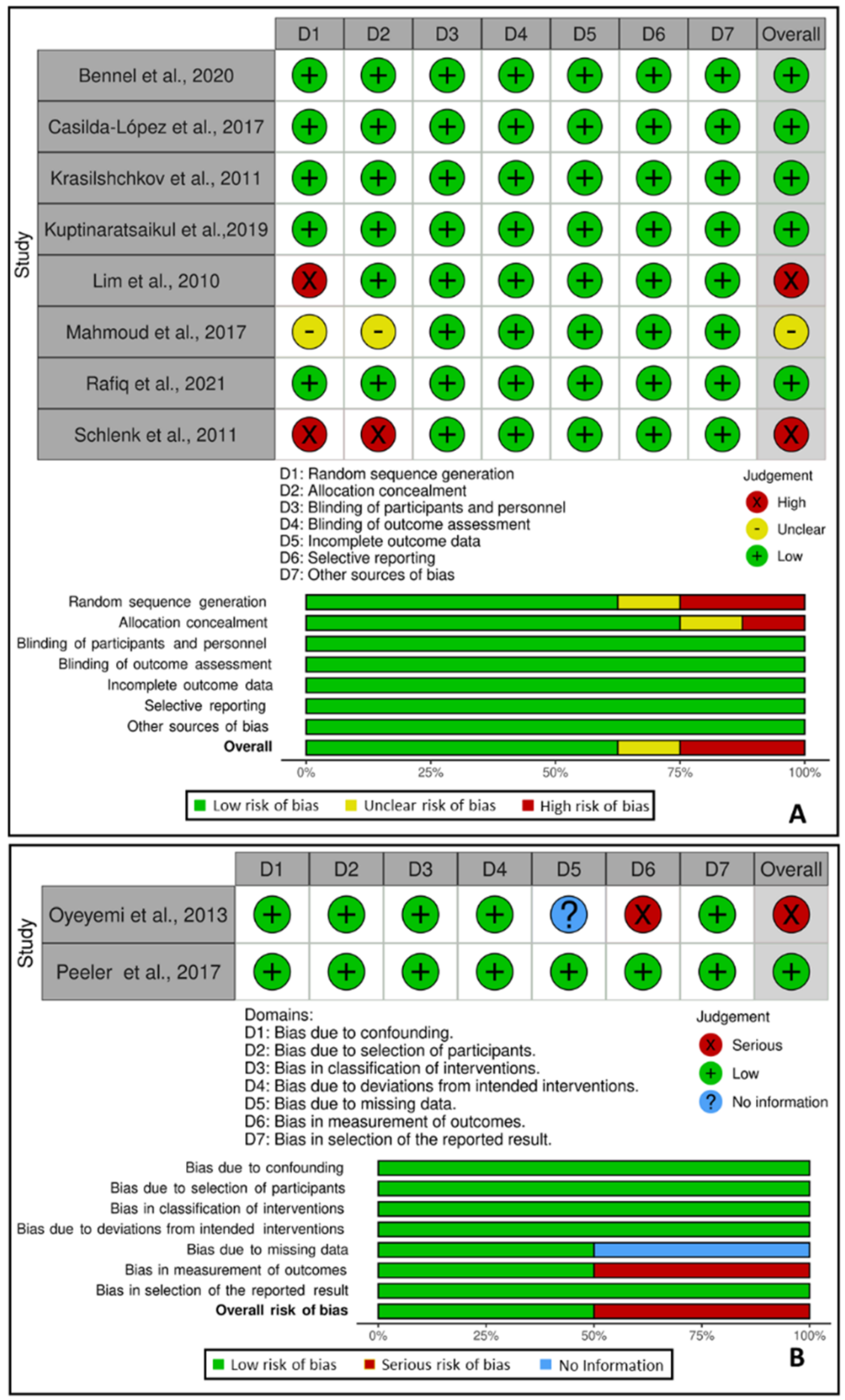
3.3. Methodological Quality
3.4. Risk of Bias
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Standardization of Osteoarthritis Definitions|Osteoarthritis Research Society International (OARSI). Available online: https://www.oarsi.org/research/standardization-osteoarthritis-definitions (accessed on 8 July 2020).
- Staines, K.; Hardy, R.; Samvelyan, H.; Ward, K.; Cooper, R. Life course longitudinal growth and risk of knee osteoarthritis at age 53 years: Evidence from the 1946 British birth cohort study. Osteoarthr. Cartil. 2020, 29, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Roos, E.; Arden, N.K. Strategies for the prevention of knee osteoarthritis. Nat. Rev. Rheumatol. 2015, 12, 92–101. [Google Scholar] [CrossRef]
- Murphy, L.; Schwartz, T.A.; Helmick, C.G.; Renner, J.B.; Tudor, G.; Koch, G.; Dragomir, A.; Kalsbeek, W.D.; Luta, G.; Jordan, J.M. Lifetime risk of symptomatic knee osteoarthritis. Arthritis Care Res. 2008, 59, 1207–1213. [Google Scholar] [CrossRef] [PubMed]
- Obesity. Available online: https://www.who.int/health-topics/obesity#tab=tab_1 (accessed on 8 July 2020).
- Yázigi, F.; Espanha, M.; Marques, A.; Teles, J.; Teixeira, P. Predictors of walking capacity in obese adults with knee osteoarthritis. Acta Reum. Port. 2019, 43, 256–263. Available online: http://www.ncbi.nlm.nih.gov/pubmed/30641533 (accessed on 20 July 2021).
- Ventura, J.; Welikson, T.; Ered, A.; Subotnik, K.L.; Keefe, R.S.E.; Hellemann, G.S.; Nuechterlein, K.H. Virtual reality assessment of functional capacity in the early course of schizophrenia: Associations with cognitive performance and daily functioning. Early Interv. Psychiatry 2019, 14, 106–114. [Google Scholar] [CrossRef]
- Stokes, J.W.; Wanderer, J.P.; McEvoy, M.D. Significant discrepancies exist between clinician assessment and patient self-assessment of functional capacity by validated scoring tools during preoperative evaluation. Perioper. Med. 2016, 5, 18. [Google Scholar] [CrossRef]
- Gomes-Neto, M.; Araujo, A.D.; Junqueira, I.D.A.; Oliveira, D.; Brasileiro, A.; Arcanjo, F.L. Comparative study of functional capacity and quality of life among obese and non-obese elderly people with knee osteoarthritis. Rev. Bras. Reum. 2016, 56, 126–130. [Google Scholar] [CrossRef][Green Version]
- Abramoff, B.; Caldera, F.E. Osteoarthritis: Pathology, Diagnosis, and Treatment Options. Med. Clin. N. Am. 2020, 104, 293–311. [Google Scholar] [CrossRef]
- Kolasinski, S.L.; Neogi, T.; Hochberg, M.C.; Oatis, C.; Guyatt, G.; Block, J.; Callahan, L.; Copenhaver, C.; Dodge, C.; Felson, D.; et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Rheumatol. 2020, 72, 220–233. [Google Scholar] [CrossRef]
- Lee, J.; Song, J.; Hootman, J.M.; Semanik, P.A.; Chang, R.W.; Sharma, L.; Van Horn, L.; Bathon, J.M.; Eaton, C.; Hochberg, M.C.; et al. Obesity and other modifiable factors for physical inactivity measured by accelerometer in adults with knee osteoarthritis. Arthritis Care Res. 2012, 65, 53–61. [Google Scholar] [CrossRef]
- Mahmoud, W.S.; Elnaggar, R.K.; Ahmed, A.S. Influence of Isometric Exercise Training on Quadriceps Muscle Architecture and Strength in Obese Subjects with Knee Osteoarthritis. Int. J. Med. Res. Health Sci. 2017, 6, 1–9. Available online: http://www.ijmrhs.com (accessed on 20 November 2021).
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, R.B. PEDro: A Physiotherapy Evidence Database. Med. Ref. Serv. Q. 2008, 27, 188–197. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]
- Bennell, K.; Nelligan, R.; Kimp, A.; Schwartz, S.; Kasza, J.; Wrigley, T.; Metcalf, B.; Hodges, P.; Hinman, R. What type of exercise is most effective for people with knee osteoarthritis and co-morbid obesity?: The TARGET randomized controlled trial. Osteoarthr. Cartil. 2020, 28, 755–765. [Google Scholar] [CrossRef]
- Casilda-López, J.; Valenza, M.C.; Cabrera-Martos, I.; Díaz-Pelegrina, A.; Moreno-Ramírez, M.P.; Valenza-Demet, G. Effects of a dance-based aquatic exercise program in obese postmenopausal women with knee osteoarthritis: A randomized controlled trial. Menopause 2017, 24, 768–773. [Google Scholar] [CrossRef]
- Lim, J.-Y.; Tchai, E.; Jang, S.-N. Effectiveness of Aquatic Exercise for Obese Patients with Knee Osteoarthritis: A Randomized Controlled Trial. PMR 2010, 2, 723–731. [Google Scholar] [CrossRef]
- Oyeyemi, A.L. Body mass index, pain and function in individuals with knee osteoarthritis. Niger. Med. J. 2013, 54, 230–235. [Google Scholar] [CrossRef]
- Krasilshchikov, O.; Sungkit, N.; Shihabudin, T.; Shaw, I.; Shaw, B. Effects of an eight-week training programme on pain relief and physical condition of overweight and obese women with early stage primary knee osteoarthritis. Afr. J. Phys. Health Educ. Recreat. Danc. 2011, 17, 328–339. [Google Scholar] [CrossRef]
- Schlenk, E.A.; Lias, J.L.; Sereika, S.M.; Dunbar-Jacob, J.; Kwoh, K.C. Improving Physical Activity and Function in Overweight and Obese Older Adults with Osteoarthritis of the Knee: A Feasibility Study. Rehabil. Nurs. 2011, 36, 32–42. [Google Scholar] [CrossRef] [PubMed]
- Peeler, J.; Ripat, J. The effect of low-load exercise on joint pain, function, and activities of daily living in patients with knee osteoarthritis. Knee 2018, 25, 135–145. [Google Scholar] [CrossRef] [PubMed]
- Kuptniratsaikul, V.; Kittichaikarn, C.; Suntornpiyapan, P.; Kovintaset, K.; Inthibal, S. Is four-week underwater treadmill exercise regimen compared to home exercise efficacious for pain relief and functional improvement in obese patients with knee osteoarthritis? A randomized controlled trial. Clin. Rehabil. 2018, 33, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Rafiq, M.T.; Hamid, M.S.A.; Hafiz, E. Short-Term Effects of Strengthening Exercises of the Lower Limb Rehabilitation Protocol on Pain, Stiffness, Physical Function, and Body Mass Index among Knee Osteoarthritis Participants Who Were Overweight or Obese: A Clinical Trial. Sci. World J. 2021, 2021, 6672274. [Google Scholar] [CrossRef] [PubMed]
- Paineiras-Domingos, L.L.; Sá-Caputo, D.D.C.; Reis, A.; Santos, A.F.; Sousa-Gonçalves, C.R.; dos Anjos, E.M.; Pereira, M.J.D.S.; Sartorio, A.; Bernardo-Filho, M. Assessment Through the Short Physical Performance Battery of the Functionality in Individuals With Metabolic Syndrome Exposed to Whole-Body Vibration Exercises. Dose-Response 2018, 16, 155932581879453. [Google Scholar] [CrossRef] [PubMed]
- Riebe, D.; Ehrman, J.; Liguori, G.M.M. American College of Sports Medicine’s Guidelines for Exercise Testing and Prescription, 10th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2018. [Google Scholar]
- Brosseau, L.; Wells, G.A.; Tugwell, P.; Egan, M.; Dubouloz, C.J.; Casimiro, L.; Bugnariu, N.; Welch, V.A.; De Angelis, G.; Francoeur, L.; et al. Ottawa Panel evidence-based linical practice guidelines for the anagement of osteoarthritis in dults who are obese or overweight. Phys. Ther. 2011, 91, 843–861. [Google Scholar] [CrossRef]
- Inam, S.H.A.; Riaz, B.; Jamil, H.; Rafique, D.; Siddiqi, U.A.; Iqbal, M.; Sherwani, N.Z.F.; Khan, W. Do Patients With Osteoarthritis get Weight Loss Counseling? Cureus 2020, 12, e11502. [Google Scholar] [CrossRef]
- Messier, S.P.; Loeser, R.F.; Miller, G.D.; Morgan, T.M.; Rejeski, W.J.; Sevick, M.A.; Ettinger, W.H.; Pahor, M.; Williamson, J.D. Exercise and dietary weight loss in overweight and obese older adults with knee osteoarthritis: The arthritis, diet, and activity promotion trial. Arthritis Care Res. 2004, 50, 1501–1510. [Google Scholar] [CrossRef]
- Kabiri, S.; Halabchi, F.; Angoorani, H.; Yekaninejad, S. Comparison of three modes of aerobic exercise combined with resistance training on the pain and function of patients with knee osteoarthritis: A randomized controlled trial. Phys. Ther. Sport 2018, 32, 22–28. [Google Scholar] [CrossRef]
- McAlindon, T.E.; Bannuru, R.; Sullivan, M.C.; Arden, N.K.; Berenbaum, F.; Bierma-Zeinstra, S.M.; Hawker, G.A.; Henrotin, Y.; Hunter, D.J.; Kawaguchi, H.; et al. OARSI guidelines for the non-surgical management of knee osteoarthritis. Osteoarthr. Cartil. 2014, 22, 363–388. [Google Scholar] [CrossRef]
- Taglietti, M.; Facci, L.M.; Trelha, C.S.; De Melo, F.C.; Da Silva, D.W.; Sawczuk, G.; Ruivo, T.M.; De Souza, T.B.; Sforza, C.; Cardoso, J.R. Effectiveness of aquatic exercises compared to patient-education on health status in individuals with knee osteoarthritis: A randomized controlled trial. Clin. Rehabil. 2018, 32, 766–776. [Google Scholar] [CrossRef]
- Wang, T.-J.; Lee, S.-C.; Liang, S.-Y.; Tung, H.-H.; Wu, S.-F.V.; Lin, Y.-P. Comparing the efficacy of aquatic exercises and land-based exercises for patients with knee osteoarthritis. J. Clin. Nurs. 2011, 20, 2609–2622. [Google Scholar] [CrossRef]
- Matt Denning, W.; Winward, J.G.; Pardo, M.B.; Hopkins, J.T.; Seeley, M.K. Body weight independently affects articular cartilage catabolism. J. Sport Sci. Med. 2015, 14, 290–296. [Google Scholar]
- Liang, J.; Guo, Y.; Zheng, Y.; Lang, S.; Chen, H.; You, Y.; O’Young, B.; Ou, H.; Lin, Q. The Lower Body Positive Pressure Treadmill for Knee Osteoarthritis Rehabilitation. J. Vis. Exp. 2019, 149, e59829. [Google Scholar] [CrossRef] [PubMed]
- Takacs, J.; Anderson, J.E.; Leiter, J.R.S.; MacDonald, P.B.; Peeler, J.D. Lower body positive pressure: An emerging technology in the battle against knee osteoarthritis? Clin. Interv. Aging 2013, 8, 983–991. [Google Scholar] [PubMed]
- Jenkinson, C.M.; Doherty, M.; Avery, A.; Read, A.; Taylor, M.; Sach, T.; Silcocks, P.; Muir, K.R. Effects of dietary intervention and quadriceps strengthening exercises on pain and function in overweight people with knee pain: Randomised controlled trial. BMJ 2009, 339, b3170. [Google Scholar] [CrossRef]
- Huang, L.; Guo, B.; Xu, F.; Zhao, J. Effects of quadriceps functional exercise with isometric contraction in the treatment of knee osteoarthritis. Int. J. Rheum. Dis. 2017, 21, 952–959. [Google Scholar] [CrossRef]
- Semanik, P.; Chang, R.; Dunlop, D. Aerobic Activity in Prevention & Sympton Control of Osteoarthritis. Natl. Inst. Health 2012, 29, 997–1003. [Google Scholar]
- Mihalko, S.L.; Cox, P.; Beavers, D.P.; Miller, G.D.; Nicklas, B.J.; Lyles, M.; Hunter, D.J.; Eckstein, F.; Guermazi, A.; Loeser, R.F.; et al. Effect of intensive diet and exercise on self-efficacy in overweight and obese adults with knee osteoarthritis: The IDEA randomized clinical trial. Transl. Behav. Med. 2018, 9, 227–235. [Google Scholar] [CrossRef]
- Haleva, Y.; Dunsky, A.; Meckel, Y.; Kleinöder, H.; Bar-eli, M.; Mester, J. Original article The effect of long-term whole-body vibration on muscular performance. Braz. J. Health Biomed. Sci. 2020, 19, 100–107. [Google Scholar]



{kind=link}
{kind=link}
| Author/Year | Aim | Participants/ Groups/ Mean Age | BMI (kg/m2–Mean ± SD) | Physical Exercise Program | Functional Capacity Assessment | PEDro Scale | Results (PF) |
|---|---|---|---|---|---|---|---|
| Bennel et al., 2020 | To directly compare the effects of two exercise programs on primary outcomes of pain and PF | N: 128 Female Age: ≥ 50 years NWB exercise (62.4 ± 6.7) WB exercise (60.9 ± 6.8) Groups: NWB exercise and WB exercise | NWB exercise (37.3 ± 6.8) WB exercise (37.8 ± 6.0) | 12 weeks Total of 5 individual sessions 30–40 min for each session Home program: 12 weeks/4 times per week NWB exercises group—Five exercises performed in sitting or supine positions aimed at QS. Three sets of 10 repetitions for each exercise. Resistance applied with an ankle cuff weight or resistance band. WB exercises group—5 exercises performed in a WB position, aimed to strengthen hip abductors, hip extensors, quadriceps and hamstrings | WOMAC KOOS 30-s CSS 40-m FPWT 6-step SCDT | 8/10 (high) | Clinically relevant benefits on the primary outcomes of pain (NWB 4.1; WB 3.4) and PF (NWB 21.2; WB 18.8) in both groups over 12 weeks, however, WB exercise may be preferred over NWB exercise |
| Mahmoud et al., 2017 | To evaluate the effects of ITE on quadricep muscle architecture and strength | N: 44 Male Age: 40–65 years IET (54.6 ± 8.6) Control (53.2 ± 9.6) Groups: IET and CG | IET (35 ± 4.1) CG (34.8 ± 4.2) | 12 weeks and 3 times per week Exercise: IET (3–5 sets of 5–10 repetitions of 5 s unilateral isometric knee extensions, with 30 s rest between repetitions and 1 min between sets) Both Groups: CPTP (hot packs and therapeutic ultrasonic) | WOMAC | 8/10 (high) | ↓ WOMAC scores IET Pre: 35.8 ± 4.59 Post: 19.2 ± 7.28 p < 0.05 |
| Casilda-López, et al., 2017 | To evaluate the effects of a dance-based AEP on functionality, cardiorespiratory capacity, post-exercise heart rate and fatigue in obese postmenopausal women | N: 34 Female Age ≥ 50 years Dance-based AEP (65.62 ± 7.15) Control (66 ± 6.35) Groups: dance-based AEP and CG | Dance-based AEP (31.69 ± 2.44) CG (33.65 ± 3.04) | 8 weeks and 3 times per week Exercise: Heated chest-high swimming pool; dance protocol with a 12 min warm-up, followed by 5 min of slow rhythm music, 3 min of fast rhythm music, 5 min slow, 3 min fast and 5 min slow (total 21 min). A 12 min cool-down after the last rhythm CG performed conventional aquatic exercises | WOMAC | 8/10 (high) | ↓ WOMAC Aggregate score Post-treatment: Dance: 37.30 ± 16.61 CG: 41.83 ± 13.69 p = 0.048 Follow-up: Dance: 38.60 ± 13.61 CG: 42.60 ± 9.05 p = 0.038 |
| Schlenk, et al., 2011 | To examine the effects of a 6-month self-efficacy-based, individually delivered, lower-extremity exercise and fitness walking intervention with a 6-month follow-up on PF | N: 26 Male and Female Age (mean ± SD): 63.2 ± 9.8 years Groups: Staying Active with Arthritis (STAR) group and CG | 33.3 ± 6.0 | 24 weeks 6 weekly sessions + 9 biweekly telephone counseling sessions + HPE lower-extremity flexibility and strengthening; walking toward a goal of 150 min per week + HP CG received usual care and after 6 months received no self-efficacy-based adherence counseling | 6-min aerobic endurance walk test SPPB 4-m walk test Standing balance test WOMAC | 5/10 (fair) | From baseline to the end of the 6 month follow up: ANOVA HPE: time effect p = 0.028 6-min aerobic: ↑ distance p = 0.006 SPPB: ↑ scores p = 0.002 |
| Kuptinaratsaikul et al., 2019 | To investigate the efficacy of a four-week UTE regimen compared to a home exercise regimen relative to pain relief and functional improvement in obese patients with KOA | N: 80 Male and Female Age 50–80 years HPE (61.7 ± 6.9) UTE (62.1 ± 6.4) Groups: Daily quadricep exercise at home HPE N: 40 (CG) or UTE N: 40 | HPE (28.4 ±3.0) UTE (28.9 ± 3.2) | 4 weeks Study Group: UTE with moderate intensity (NRS 5–6/10) 16 for 30 min, including warm up and cool down, three times per week (12 total sessions) HPE: brochures advising them how to use their knee joints in daily practice + regular quadricep exercise (10–20 repetitions set with a 1–2-min rest) and then to repeat this exercise–rest cycle. Seven days per week/thirty min daily | 6MWD QS | 8/10 (high) | Improvements in both groups Mean differences (95% CI) 6MWD: 10.81 (−11.90, 3.53) p = 0.345 QS: 0.67(−0.10, 1.44) p = 0.088 |
| Krasilshchikov et al., 2011 | To determine the effect of PCRAE on early primary KOA in overweight and obese | N: 16 Female Age 50–64 PCRAE N: 8 (58.38 ± 4.9) CG N: 8 (58.25 ± 5.1) | PCRAE (28.6 ± 5.6) Non-exercising CG (26.5 ± 4.1) | 8 weeks PCRAE training grouped in a single one-hour training session 3 times per week, two sets of isometric quadricep and hamstring contraction, isotonic quadricep contractions, chair squats and dynamic stepping. Resistance: walking for 15 min progressively | WOMAC PF score KECPT right and left 120°/s and 180°/s 6MWD | 7/10 (high) | Pretest × Post test PCRAE ↓ WOMAC PF score 21.13 ± 7.9 × 9.50 ± 4.3; p < 0.05 KECPT right and left p < 0.05 6MWD: 337.65 ± 55.1 × 385.81 ± 32.8 p < 0.05 |
| Lim et al., 2010 | To design an AEP and LBEP to enhance knee function and reduce body fat in patients with obesity and KOA | N: 75 Male +Female AEP N: 26; Age: 65.7 ± 8.9 LBEP: N: 25; Age: 67.7 ± 7.8 CG: N: 24; Age: 63.3 ± 5.3 | AEP (27.9 ± 1.5) LBEP (27.6 ± 1.7) CG: (27.7 ± 2.0) | 3 times per week 8 weeks AEP: 40-min duration per session LBEP: 40 min per session, intensity of LBEP began from 40% or 60% of the one repetition maximum for the beginner or advanced classes, respectively | WOMAC PTKE PTKF | 7/10 (high) | Before × after ↓ WOMAC PF score AEP:35.1 ± 11.3 × 20.9 ± 9.9 p < 0.05 LBEP: 33.6 ± 12.6 × 23.6 ± 12.8 p < 0.05 GC: 30.4 ± 19.1 × 27.6 ± 18.3 PTKE and PTKF both with improvement but without statistical significance |
| Rafiq et al., 2021 | To determine the short-term effects of the home protocol of strengthening exercises in NWB positions on the functional capacity of overweight and obese people with KOA | N: 50 Male + Female LLRP: N:25 Age (53.40 ± 5.18) CG: N: 25 Age (52.84 ± 5.74) | LLRP: (32.18 ± 4.49) CG: (32.01 ± 3.89) | 3 times per week 4 weeks LLRP: 45–60 min of lower limb resistance training following the IDC in sitting and lying positions CG: whole body ROM exercises following the IDC | WOMAC | 8/10 (high) | LLRP and CG: WOMAC PF score p > 0.05 (p = 0.104) |
| Peeler et al., 2017 | Evaluate the effect of a 12-week LBPP-supported low-load treadmill walking program on knee pain, joint function and performance of daily activities in patients with KOA | N: 35 Age: 50–75 Female:22 63.1 ± 5.9 (53–72) Male: 9 67.1 ± 6.4 (59–75) Single Group | 32.8 ± 6.5 | 12 week-LBPP-supported low-load treadmill walking program. Two times per week for 30 min on a treadmill at a set speed of 3.1 mph at a 0° incline LBPP increased by 5% per min LBPP support was restricted to a maximum of 40% body weight | KOOS COPM Isokinetic muscle strength | Pedro Scale N/A | KOOS (daily living) Female ↑ scores (p = 0.0016) 58 ± 15 × 67 ± 15 Male: no statistical difference COPM (performance) Female (p = 0.0003) 4.3 ± 1.5 × 5.3 ± 1.6 Male (p = 0.0415) 5.0 ± 1.6 × 6.2 ± 2.5 Improvement of Isokinetic muscle strength Female (p = 0.0002) 2.9 ± 2.2 × 1.0 ± 1.3 Male (p = 0.0490) 4.0 ± 2.0 × 2.8 ± 2.1 |
| Oyeyemi et al.,2013 | To investigate the effects of BMI on pain and PF during a four-week exercise program in patients with KOA | N: 46 31 Male 15 Female Age: 34–69 years ± 55 years Groups: normal weight (N: 15) age (56.93 ± 9.56); overweight (N: 13) age (55.31 ± 8.07) obese (N: 18) age (55.2 ± 9.04) | Not mentioned | 10 bouts of 10 repetitions of isometric exercise of the quadriceps (10 s of work and 5 s of rest) and 2 min of rest between bouts (total of 100 contractions). Riding the SBE with an initial resistance set at 25 W for 6 min. The resistance was increased to 35, 45 and 55 W in the second, third and fourth week, respectively 2 times per week | WOMAC | Pedro Scale N/A | ↓ PF WOMAC scores (week 1 × week 4) Overweight: 40.66 ± 15.6 × 19.81 ± 5.02 Obese: 52.87 ± 12.76 × 19.58 ± 4.56 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caiado, V.S.; Santos, A.C.G.; Moreira-Marconi, E.; Moura-Fernandes, M.C.; Seixas, A.; Taiar, R.; Lacerda, A.C.R.; Sonza, A.; Mendonça, V.A.; Sá-Caputo, D.C.; et al. Effects of Physical Exercises Alone on the Functional Capacity of Individuals with Obesity and Knee Osteoarthritis: A Systematic Review. Biology 2022, 11, 1391. https://doi.org/10.3390/biology11101391
Caiado VS, Santos ACG, Moreira-Marconi E, Moura-Fernandes MC, Seixas A, Taiar R, Lacerda ACR, Sonza A, Mendonça VA, Sá-Caputo DC, et al. Effects of Physical Exercises Alone on the Functional Capacity of Individuals with Obesity and Knee Osteoarthritis: A Systematic Review. Biology. 2022; 11(10):1391. https://doi.org/10.3390/biology11101391
Chicago/Turabian StyleCaiado, Vanessa Silva, Aline Cristina Gomes Santos, Eloá Moreira-Marconi, Marcia Cristina Moura-Fernandes, Adérito Seixas, Redha Taiar, Ana Cristina Rodrigues Lacerda, Anelise Sonza, Vanessa Amaral Mendonça, Danúbia Cunha Sá-Caputo, and et al. 2022. "Effects of Physical Exercises Alone on the Functional Capacity of Individuals with Obesity and Knee Osteoarthritis: A Systematic Review" Biology 11, no. 10: 1391. https://doi.org/10.3390/biology11101391
APA StyleCaiado, V. S., Santos, A. C. G., Moreira-Marconi, E., Moura-Fernandes, M. C., Seixas, A., Taiar, R., Lacerda, A. C. R., Sonza, A., Mendonça, V. A., Sá-Caputo, D. C., & Bernardo-Filho, M. (2022). Effects of Physical Exercises Alone on the Functional Capacity of Individuals with Obesity and Knee Osteoarthritis: A Systematic Review. Biology, 11(10), 1391. https://doi.org/10.3390/biology11101391