
The Side Effects of Therapeutic Radioiodine-131 on the Structure of Enamel and Dentin in Permanent Human Teeth

 , , ,
, , ,  ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Specimen Preparation
2.2. Radioiodine Irradiation Protocol
2.3. Histological Assessment of Dental Tissues
2.4. Scanning Electron Microscopy and Atomic Force Microscopy Analysis of Dental Tissues
3. Results
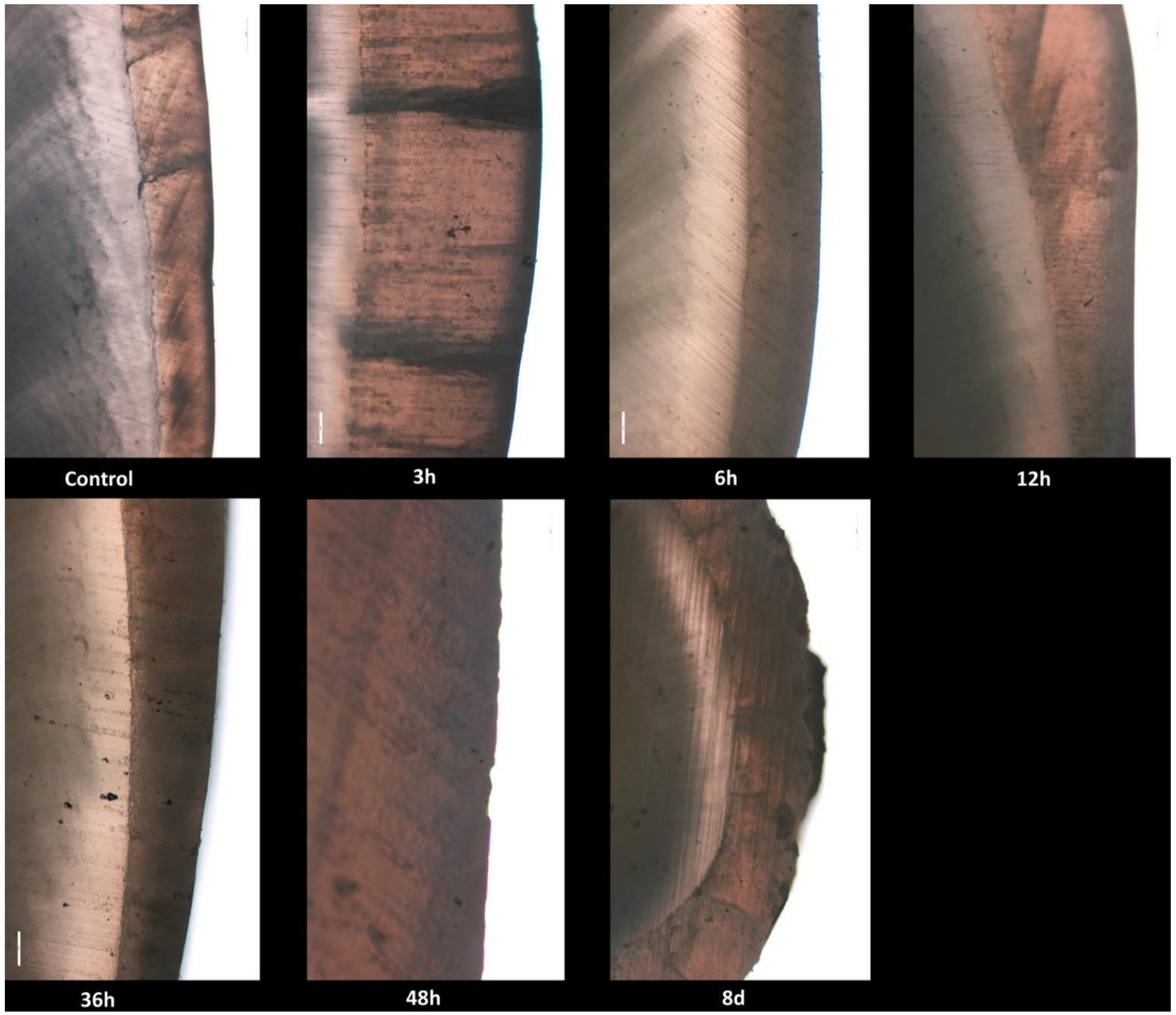
3.1. Histological Findings
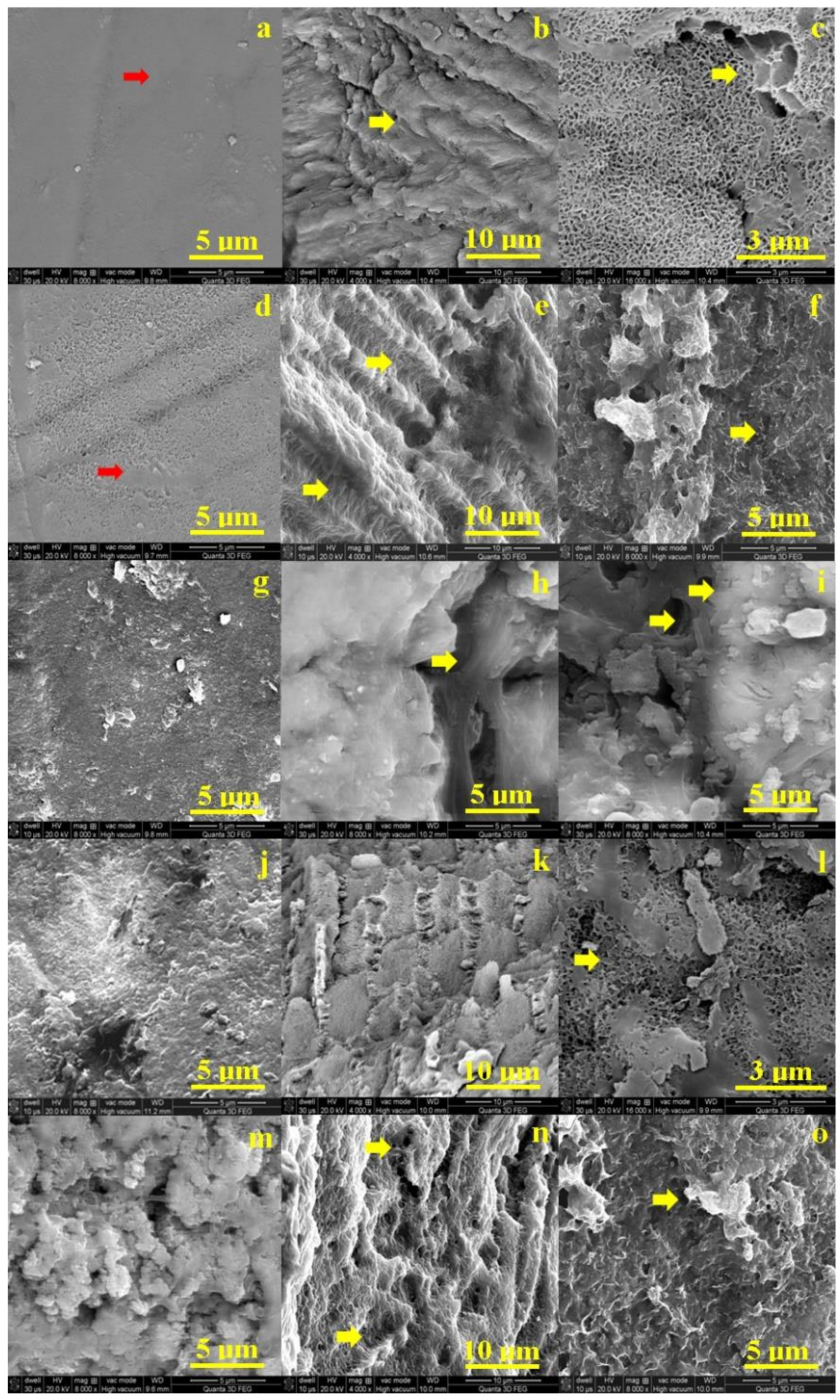
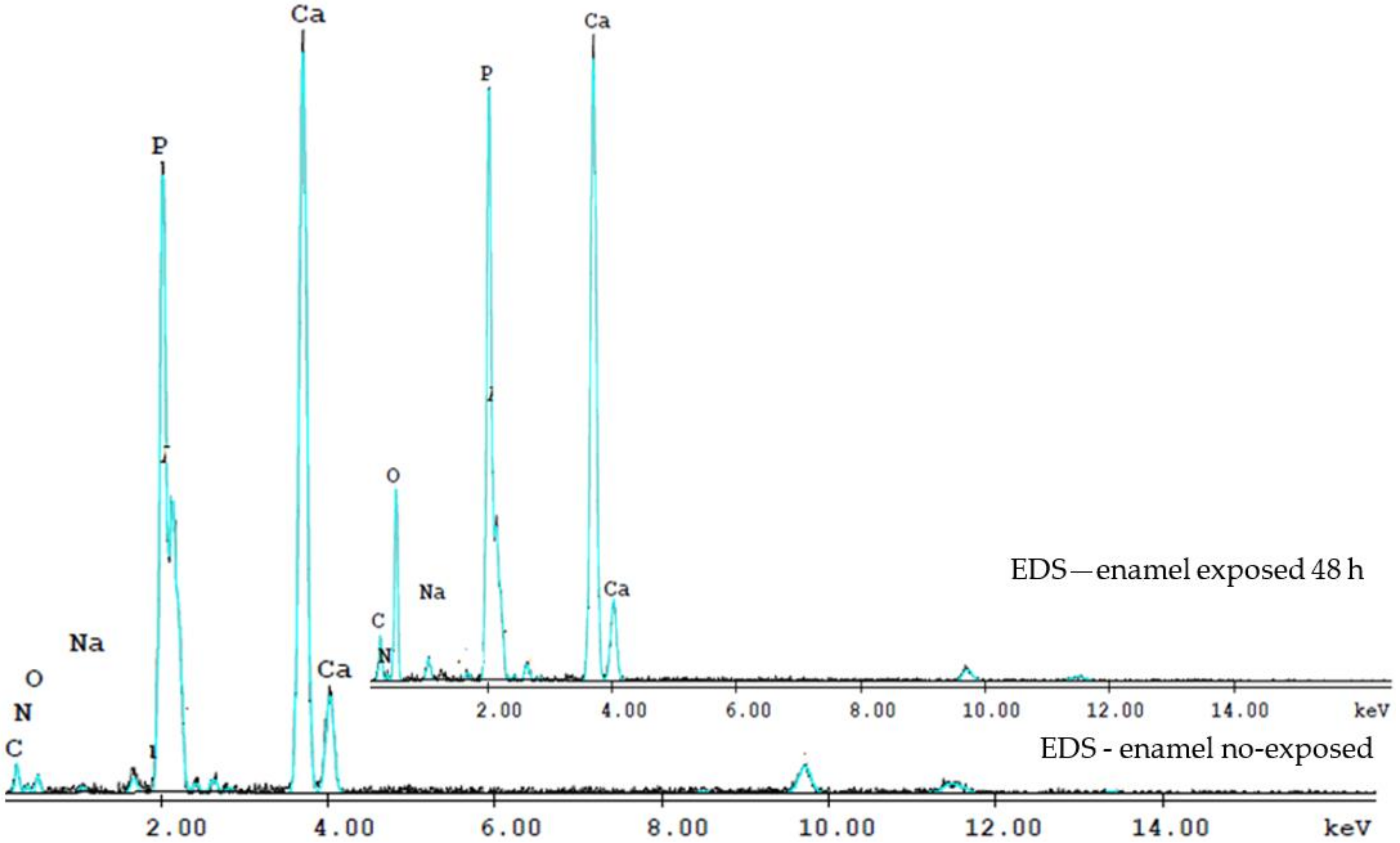
3.2. SEM Findings
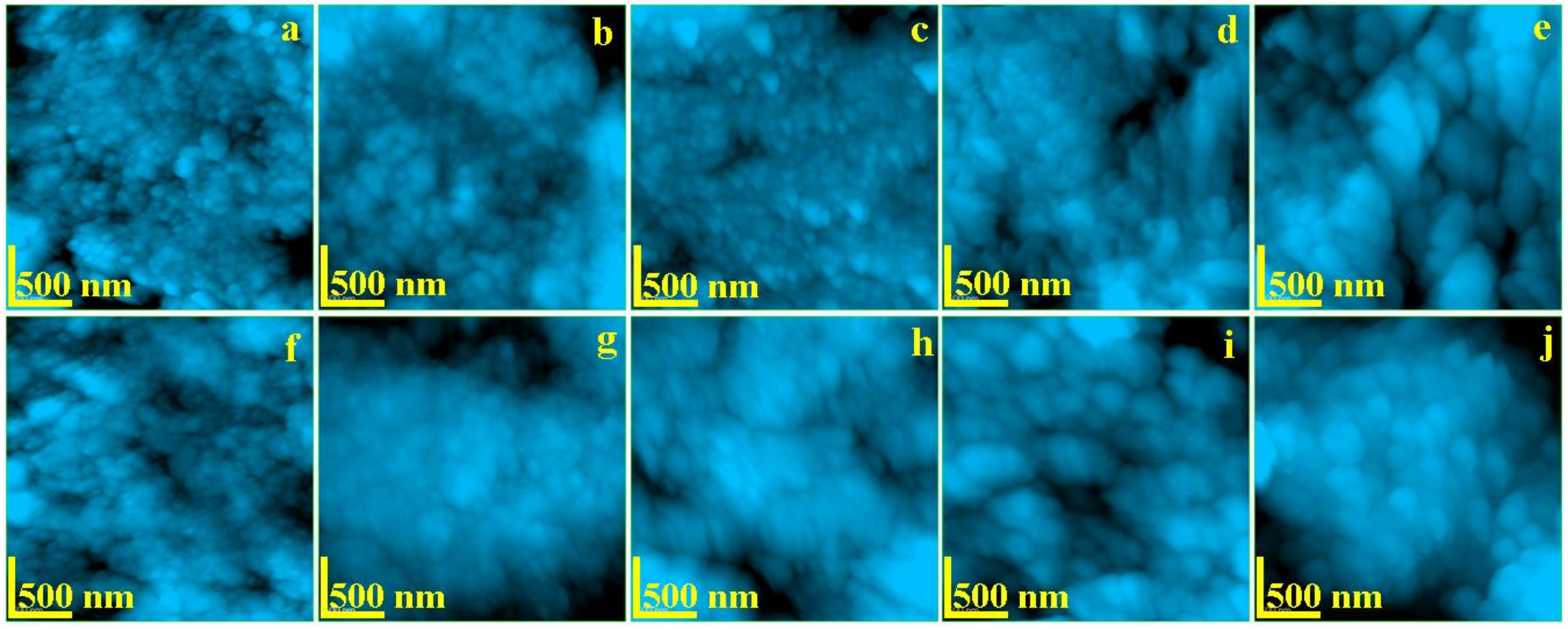
3.3. AFM Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ross, D.S. Radioiodine therapy for hyperthyroidism. N. Engl. J. Med. 2011, 364, 542–550. [Google Scholar] [CrossRef] [PubMed]
- Kobe, C.; Weber, I.; Eschner, W.; Sudbrock, F.; Schmidt, M.; Dietlein, M.; Schicha, H. Graves’ disease and radioiodine therapy. Is success of ablation dependent on the choice of thyreostatic medication? Nuklearmedizin 2008, 47, 153–156. [Google Scholar] [PubMed]
- Tuttle, R.M.; Ahuja, S.; Avram, A.M.; Bernet, V.J.; Bourguet, P.; Daniels, G.H.; Dillehay, G.; Draganescu, C.; Flux, G.; Führer, D.; et al. Controversies, Consensus, and Collaboration in the Use of (131)I Therapy in Differentiated Thyroid Cancer: A Joint Statement from the American Thyroid Association, the European Association of Nuclear Medicine, the Society of Nuclear Medicine and Molecula. Thyroid 2019, 29, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Bonnema, S.J.; Hegedüs, L. Radioiodine Therapy in Benign Thyroid Diseases: Effects, Side Effects, and Factors Affecting Therapeutic Outcome. Endocr. Rev. 2012, 33, 920–980. [Google Scholar] [CrossRef]
- Agbaje, J.O.; Jacobs, R.; Michiels, K.; Abu-Ta’a, M.; van Steenberghe, D. Bone healing after dental extractions in irradiated patients: A pilot study on a novel technique for volume assessment of healing tooth sockets. Clin. Oral Investig. 2009, 13, 257–261. [Google Scholar] [CrossRef]
- Mandel, S.J.; Mandel, L. Radioactive iodine and the salivary glands. Thyroid 2003, 13, 265–271. [Google Scholar] [CrossRef]
- Wang, X.; Fang, W.; Wei, L.; Li, B.; Cheng, Y. Clinical and Sialographic Imaging Features of (131)I Radiation-induced Submandibular Gland Sialadenitis. J. Oral Maxillofac. Surg. 2021, 79, 376–382. [Google Scholar] [CrossRef]
- Canzi, P.; Cacciola, S.; Capaccio, P.; Pagella, F.; Occhini, A.; Pignataro, L.; Benazzo, M. Interventional sialendoscopy for radioiodine-induced sialadenitis: Quo vadis? Acta Otorhinolaryngol. Ital. 2017, 37, 155–159. [Google Scholar]
- Sunavala-Dossabhoy, G. Radioactive iodine: An unappreciated threat to salivary gland function. Oral Dis. 2018, 24, 198–201. [Google Scholar] [CrossRef]
- Mandel, L.; Greene, L.W. Differentiating (131)I Radiation Sialadenitis From Autoimmune (Sjögren Syndrome) Sialadenitis: Case Report. J. Oral Maxillofac. Surg. 2017, 75, 2379–2382. [Google Scholar] [CrossRef]
- Dietlein, M.; Drzezga, A. Taste dysfunction (dysgeusia) and radioiodine therapy of thyroid cancer—Be aware of side effects by antidepressants and sedatives. Vorschädigung durch Antidepressiva und Sedativa beachten. Nuklearmedizin 2017, 56, 125–131. [Google Scholar]
- Maruoka, Y.; Baba, S.; Isoda, T.; Kitamura, Y.; Abe, K.; Sasaki, M.; Honda, H. A Functional Scoring System Based on Salivary Gland Scintigraphy for Evaluating Salivary Gland Dysfunction Secondary to (131)I therapy in Patients with Differentiated Thyroid Carcinoma. J. Clin. Diagn. Res. 2017, 11, TC23–TC28. [Google Scholar]
- Mester, A.; Piciu, A.; Lucaciu, O.; Apostu, D.; Piciu, D.; Voina-Tonea, A. Assessment and Care of Oral Lesions for Patients Who Undergo Radioiodine Treatment for Thyroid Cancer. Am. J. Med. Sci. 2021, 361, 8–13. [Google Scholar] [CrossRef]
- Palmier, N.R.; Madrid, C.C.; de Paglioni, M.P.; Rivera, C.; Martins, B.N.F.L.; Araújo, A.L.D.; Salvajoli, J.V.; de Goes, M.F.; Lopes, M.A.; Ribeiro, A.C.P.; et al. Cracked tooth syndrome in irradiated patients with head and neck cancer. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 126, 335–341.e2. [Google Scholar] [CrossRef]
- Lu, H.; Zhao, Q.; Guo, J.; Zeng, B.; Yu, X.; Yu, D.; Zhao, W. Direct radiation-induced effects on dental hard tissue. Radiat. Oncol. 2019, 14, 5. [Google Scholar] [CrossRef]
- Bartelstone, H.J. Radioiodine penetration through intact enamel with uptake by bloodstream and thyroid gland. J. Dent. Res. 1951, 30, 728–733. [Google Scholar] [CrossRef]
- Mester, A.; Piciu, A.; Piciu, D.; Petean, I.; Lucaciu, P.O.; Apostu, D.; Moisescu-Goia, C.; Voina-Tonea, A.; Moldovan, M. Disorders of Dental Hard Tissues Induced by Radioiodine-131 (I-131) Therapy Used in Differentiated Thyroid Cancer: An In Vitro Study. Biomedicines 2020, 8, 475. [Google Scholar] [CrossRef]
- Lassmann, M.; Reiners, C.; Luster, M. Dosimetry and thyroid cancer: The individual dosage of radioiodine. Endocr. Relat. Cancer 2010, 17, R161–R172. [Google Scholar] [CrossRef]
- Lee, S.M.; Lee, J.W.; Kim, S.Y.; Han, S.W.; Bae, W.K. Prediction of risk for symptomatic sialadenitis by post-therapeutic dual (131)I scintigraphy in patients with differentiated thyroid cancer. Ann. Nucl. Med. 2013, 27, 700–709. [Google Scholar] [CrossRef]
- Mandair, G.S.; Oest, M.E.; Mann, K.A.; Morris, M.D.; Damron, T.A.; Kohn, D.H. Radiation-induced changes to bone composition extend beyond periosteal bone. Bone Rep. 2020, 12, 100262. [Google Scholar] [CrossRef]
- Oltean-Dan, D.; Dogaru, G.-B.; Tomoaia-Cotisel, M.; Apostu, D.; Mester, A.; Benea, H.-R.-C.; Paiusan, M.-G.; Jianu, E.-M.; Mocanu, A.; Balint, R.; et al. Enhancement of bone consolidation using high-frequency pulsed electromagnetic short-waves and titanium implants coated with biomimetic composite embedded into PLA matrix: In vivo evaluation. Int. J. Nanomed. 2019, 14, 5799–5816. [Google Scholar] [CrossRef] [PubMed]
- Mester, A.; Apostu, D.; Ciobanu, L.; Piciu, A.; Lucaciu, O.; Campian, R.S.; Taulescu, M.; Bran, S. The impact of proton pump inhibitors on bone regeneration and implant osseointegration. Drug Metab. Rev. 2019, 51, 330–339. [Google Scholar] [CrossRef] [PubMed]
- Costa, S.; Reagan, M.R. Therapeutic Irradiation: Consequences for Bone and Bone Marrow Adipose Tissue. Front. Endocrinol. 2019, 10, 587. [Google Scholar] [CrossRef] [PubMed]
- Mitsimponas, K.T.; Moebius, P.; Amann, K.; Stockmann, P.; Schlegel, K.-A.; Neukam, F.-W.; Wehrhan, F. Osteo-radio-necrosis (ORN) and bisphosphonate-related osteonecrosis of the jaws (BRONJ): The histopathological differences under the clinical similarities. Int. J. Clin. Exp. Pathol. 2014, 7, 496–508. [Google Scholar] [PubMed]
- Walter, M.A.; Turtschi, C.P.; Schindler, C.; Minnig, P.; Müller-Brand, J.; Müller, B. The dental safety profile of high-dose radioiodine therapy for thyroid cancer: Long-term results of a longitudinal cohort study. J. Nucl. Med. 2007, 48, 1620–1625. [Google Scholar] [CrossRef]
- Epstein, J.B.; Beier Jensen, S. Management of Hyposalivation and Xerostomia: Criteria for Treatment Strategies. Compend. Contin. Educ. Dent. 2015, 36, 600–603. [Google Scholar]
- Amdur, R.J.; Sandow, P.L.; Mendenhall, W.M.; Mazzaferri, E.L. Management of Xerostomia, Taste Impairment and Dental Prophlaxis BT—Essentials of Thyroid Cancer Management. In Essentials of Thyroid Cancer Management; Amdur, R.J., Mazzaferri, E.L., Eds.; Springer: Boston, MA, USA, 2005; pp. 281–283. ISBN 978-0-387-25714-3. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Treatment Time, Hours | ||||
|---|---|---|---|---|---|
| 0 | 6 | 12 | 48 | 192 | |
| Enamel | |||||
| Ra (nm) | 19.2 | 26.5 | 28.3 | 40.0 | 73.4 |
| Rq (nm) | 26.6 | 36.3 | 39.4 | 50.2 | 52.4 |
| Diameter (nm) | 40 | 60 | 75 | 80 | 85 |
| Dentine | |||||
| Ra (nm) | 19.4 | 29.7 | 31.8 | 35.3 | 40.2 |
| Rq (nm) | 24.0 | 36.1 | 39.6 | 40.6 | 50.4 |
| Diameter (nm) | 40 | 40 | 45 | 65 | 70 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mester, A.; Moldovan, M.; Taulescu, M.; Sarosi, C.; Petean, I.; Vulpoi, A.; Piciu, A.; Voina-Tonea, A.; Moisescu-Goia, C.; Barbus, E.; et al. The Side Effects of Therapeutic Radioiodine-131 on the Structure of Enamel and Dentin in Permanent Human Teeth. Biology 2021, 10, 284. https://doi.org/10.3390/biology10040284
Mester A, Moldovan M, Taulescu M, Sarosi C, Petean I, Vulpoi A, Piciu A, Voina-Tonea A, Moisescu-Goia C, Barbus E, et al. The Side Effects of Therapeutic Radioiodine-131 on the Structure of Enamel and Dentin in Permanent Human Teeth. Biology. 2021; 10(4):284. https://doi.org/10.3390/biology10040284
Chicago/Turabian StyleMester, Alexandru, Marioara Moldovan, Marian Taulescu, Codruta Sarosi, Ioan Petean, Adriana Vulpoi, Andra Piciu, Andrada Voina-Tonea, Cristina Moisescu-Goia, Elena Barbus, and et al. 2021. "The Side Effects of Therapeutic Radioiodine-131 on the Structure of Enamel and Dentin in Permanent Human Teeth" Biology 10, no. 4: 284. https://doi.org/10.3390/biology10040284
APA StyleMester, A., Moldovan, M., Taulescu, M., Sarosi, C., Petean, I., Vulpoi, A., Piciu, A., Voina-Tonea, A., Moisescu-Goia, C., Barbus, E., & Piciu, D. (2021). The Side Effects of Therapeutic Radioiodine-131 on the Structure of Enamel and Dentin in Permanent Human Teeth. Biology, 10(4), 284. https://doi.org/10.3390/biology10040284