The Impacts of Animal Health Service Providers on Antimicrobial Use Attitudes and Practices: An Examination of Poultry Layer Farmers in Ghana and Kenya


 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
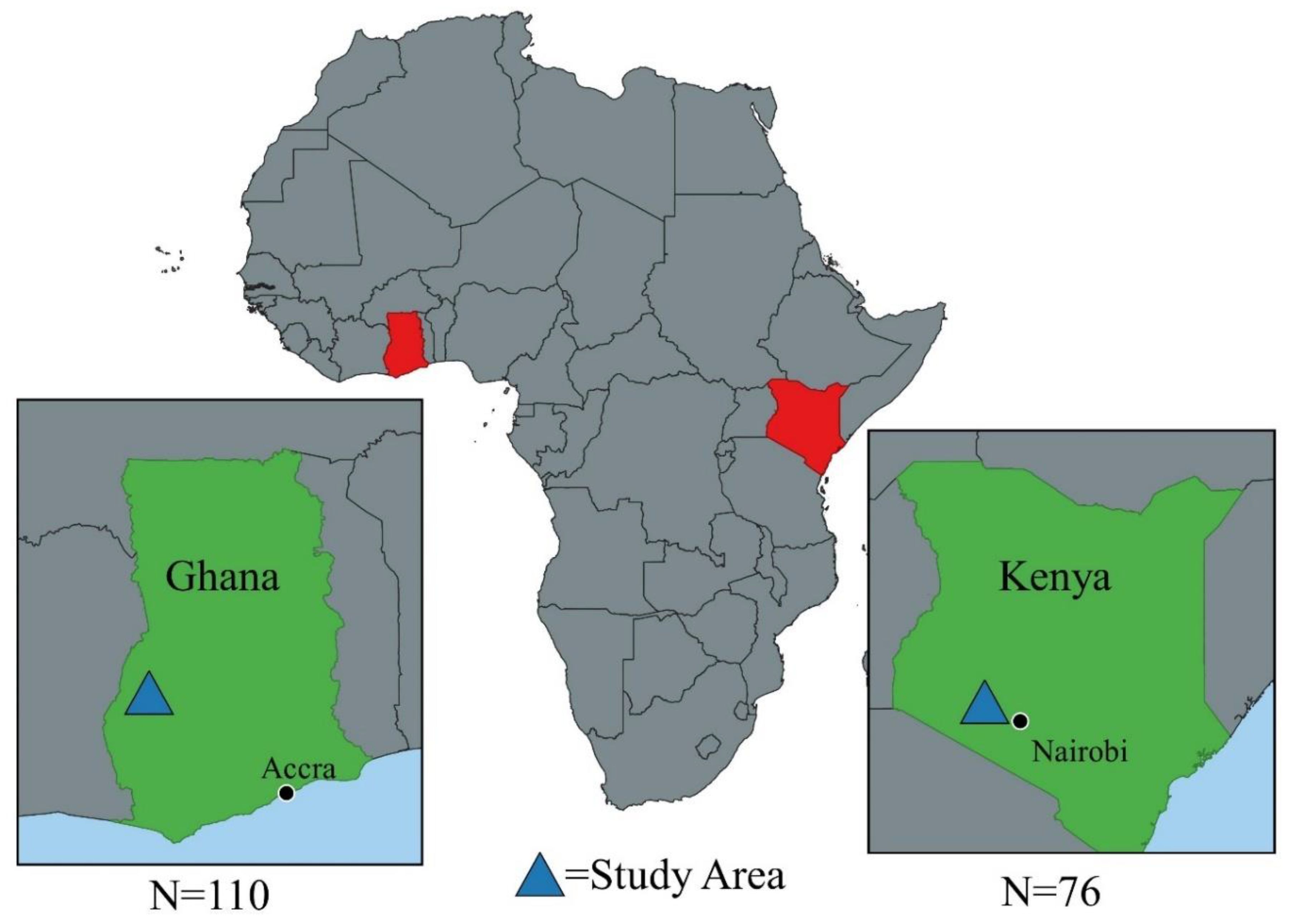
2.1. Study Locations
2.2. Survey Development
2.3. Sampling Procedure
2.4. Ethical Approvals
2.5. Analysis
3. Results
3.1. Results: Descriptive
3.2. Results: Qualitative
3.3. Quantitative Analysis
3.3.1. Impact of Animal Health Seeking Practices on Non-Prudent Practices and Knowledge and Perception
3.3.2. Impact of Animal Health Seeking Practices on Antimicrobial Use
4. Discussion
Future Work and Study Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
References
- OIE. The OIE Strategy on Antimicrobial Resistance and the Prudent Use of Antimicrobials; World Organisation for Animal Health: Paris, France, 2016. [Google Scholar]
- FAO. The FAO Action Plan on Antimicrobial Resistance 2016–2020; Food and Agriculture Organization: Rome, Italy, 2016. [Google Scholar]
- World Health Organization. Global Action Plan on Antimicrobial Resistance; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Barbosa, T.M.; Levy, S.B. The impact of antibiotic use on resistance development and persistence. Drug Resist. Updat. 2000, 3, 303–311. [Google Scholar] [CrossRef] [Green Version]
- Levy, S.B.; Marshall, B. Antibacterial resistance worldwide: Causes, challenges and responses. Nat. Med. 2004, 10, S122–S129. [Google Scholar] [CrossRef] [PubMed]
- Regula, G.; Torriani, K.; Gassner, B.; Stucki, F.; Müntener, C.R. Prescription patterns of antimicrobials in veterinary practices in Switzerland. J. Antimicrob. Chemother. 2009, 63, 805–811. [Google Scholar] [CrossRef] [PubMed]
- Speksnijder, D.C.; Mevius, D.J.; Bruschke, C.J.M.; Wagenaar, J.A. Reduction of Veterinary Antimicrobial Use in the Netherlands. The Dutch Success Model. Zoonoses Public Health 2014, 62, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Lopes Antunes, A.C.; Jensen, V.F. Close to a Decade of Decrease in Antimicrobial Usage in Danish Pig Production–Evaluating the Effect of the Yellow Card Scheme. Front. Vet. Sci. 2020, 7, 109. [Google Scholar] [CrossRef] [PubMed]
- Gozdzielewska, L.; King, C.; Flowers, P.; Mellor, D.; Dunlop, P.; Price, L. Scoping review of approaches for improving antimicrobial stewardship in livestock farmers and veterinarians. Prev. Vet. Med. 2020, 180, 105025. [Google Scholar] [CrossRef]
- Odetokun, I.A.; Akpabio, U.; Alhaji, N.B.; Biobaku, K.T.; Oloso, N.O.; Ghali-Mohammed, I.; Biobaku, A.J.; Adetunji, V.O.; Fasina, F.O. Knowledge of Antimicrobial Resistance among Veterinary Students and Their Personal Antibiotic Use Practices: A National Cross-Sectional Survey. Antibiotics 2019, 8, 243. [Google Scholar] [CrossRef] [Green Version]
- Smith, P.W.; Agbaje, M.; LeRoux-Pullen, L.; van Dyk, D.; Debusho, L.K.; Shittu, A.; Sirdar, M.M.; Fasanmi, O.G.; Adebowale, O.; Fasina, F.O. Implication of the knowledge and perceptions of veterinary students of antimicrobial resistance for future prescription of antimicrobials in animal health, South Africa. J. S. Afr. Vet. Assoc. 2019, 90, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Peeling, D.; Holden, S. The effectiveness of community-based animal health workers, for the poor, for communities and for public safety. Rev. Sci. Tech. Off. Int. Épizooties 2004, 23, 253–276. [Google Scholar] [CrossRef] [Green Version]
- Busani, L.; Graziani, C.; Binkin, N.; Franco, A.; Di Egidio, A.; Battisti, A. Survey of the knowledge, attitudes and practice of Italian beef and dairy cattle veterinarians concerning the use of antibiotics. Vet. Rec. 2004, 155, 733–738. [Google Scholar]
- Mbugua, M.W. Analysis of Demand for Antibiotics in Poultry Production in Kiambu County, Kenya. Master’s Thesis, Masters of Science, Department of Agricultural Economics, University of Nairobi, Nairobi, Kenya, 5 May 2014. [Google Scholar]
- Adelaide, O.; Bii, C.; Okemo, P. Antibiotic resistance and virulence factors in Escherichia coli from broiler chicken slaughtered at Tigoni processing plant in Limuru, Kenya. E. Afr. Med. J. 2008, 85, 597–606. [Google Scholar]
- Johnson, S.; Bugyei, K.; Nortey, P.; Tasiame, W. Antimicrobial drug usage and poultry production: Case study in Ghana. Anim. Prod. Sci. 2019, 59, 177–182. [Google Scholar] [CrossRef]
- Veterinary Services Directorate. Annual Report; Ministry of Food and Agriculture: Accra, Ghana, 2017.
- StataCorp. Stata Statistical Software: Release 16; Stata Corp LP; StataCorp LLC.: College Station, TX, USA, 2019. [Google Scholar]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. Ser. B (Methodol.) 1995, 57, 289–300. [Google Scholar] [CrossRef]
- RStudio Team. RStudio: Integrated Development for R; PBC: Boston, MA, USA, 2020. [Google Scholar]
- Shah, A. ASDOC: Stata Module to Create High-Quality Tables in MS Word from Stata Output; Statistical Software Components S458466; Boston College Department of Economics: Boston, MA, USA, 2018. [Google Scholar]
- Caudell, M.A.; Dorado-Garcia, A.; Eckford, S.; Creese, C.; Byarugaba, D.K.; Afakye, K.; Chansa-Kabali, T.; Fasina, F.O.; Kabali, E.; Kiambi, S.; et al. Towards a bottom-up understanding of antimicrobial use and resistance on the farm: A knowledge, attitudes, and practices survey across livestock systems in five African countries. PLoS ONE 2020, 15, e0220274. [Google Scholar] [CrossRef] [Green Version]
- Peeling, D.; Holden, W. Community Based Animal Health Workers-Threat or Opportunity? An Overview; IDL Group: Brighton, UK, 2003. [Google Scholar]
- Pearson, M.; Chandler, C. Knowing antimicrobial resistance in practice: A multi-country qualitative study with human and animal healthcare professionals. Glob. Health Action 2019, 12, 1599560. [Google Scholar] [CrossRef] [Green Version]
- Caudell, M.A.; Quinlan, M.B.; Subbiah, M.; Call, D.R.; Roulette, C.J.; Roulette, J.W.; Roth, A.; Matthews, L.; Quinlan, R.J. Antimicrobial Use and Veterinary Care among Agro-Pastoralists in Northern Tanzania. PLoS ONE 2017, 12, e0170328. [Google Scholar] [CrossRef] [Green Version]
- Althubaiti, A. Information bias in health research: Definition, pitfalls, and adjustment methods. J. Multidiscip. Healthc. 2016, 9, 211–217. [Google Scholar] [CrossRef] [Green Version]
- Gauthier, J.; Simeon, M.; De Haan, C. The Effect of Structural Adjustment Programmes on the Delivery of Veterinary Services in Africa; World Bank: Washington, DC, USA, 1999. [Google Scholar]
- Riddell, J.B. Things fall apart again:Structural adjustment programmes in sub-Saharan Africa. J. Mod. Afr. Stud. 1992, 30, 53–68. [Google Scholar] [CrossRef]
- Forman, S.; Plante, C.; Murray, G.; Rey, B.; Belton, D.; Evans, B.; Steinmetz, P. Position paper: Improving governance for effective veterinary services in developing countries—A priority for donor funding. Rev. Sci. Tech. 2012, 31, 647–660. [Google Scholar] [CrossRef]
- Weaver, J.; Leon, E.; Edan, M.; D’Alessio, F. Initial assessment of strategic plans for improving the performance of veterinary services in developing countries: A review of OIE PVS gap analysis reports. Rev. Sci. Tech. Off. Int. Epiz. 2012, 31, 631–645. [Google Scholar] [CrossRef]
- Nonga, H.; Simon, C.; Karimuribo, E.; Mdegela, R. Assessment of antimicrobial usage and residues in commercial chicken eggs from smallholder poultry keepers in Morogoro municipality, Tanzania. Zoonoses Public Health 2010, 57, 339–344. [Google Scholar] [CrossRef]
- Turkson, P. Use of drugs and antibiotics in poultry production in Ghana. Ghana J. Agric. Sci. 2008, 41. [Google Scholar] [CrossRef]
- Roderick, S.; Stevenson, P.; Mwendia, C.; Okech, G. The Use of Trypanocides and Antibiotics by Maasai Pastoralists. Trop. Anim. Heal. Prod. 2000, 32, 361–374. [Google Scholar] [CrossRef] [PubMed]
- Boamah, V.E.; Agyare, C.; Odoi, H.; Dalsgaard, A. Practices and factors influencing the use of antibiotics in selected poultry farms in Ghana. J. Antimicrob. Agents 2016, 2. [Google Scholar] [CrossRef]
- Mubito, E.P.; Shahada, F.; Kimanya, M.E.; Buza, J.J. Antimicrobial use in the poultry industry in Dar-es-Salaam, Tanzania and public health implications. Am. J. Res. Commun. 2014, 2, 51–63. [Google Scholar]
- Gehring, R.; Swan, G.; Sykes, R. Supply of veterinary medicinal products to an emerging farming community in the North West Province of South Africa. J. S. Afr. Vet. Assoc. 2002, 73, 185–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ojo, O.E.; Fabusoro, E.; Majasan, A.A.; Dipeolu, M.A. Antimicrobials in animal production: Usage and practices among livestock farmers in Oyo and Kaduna States of Nigeria. Trop. Anim. Health Prod. 2016, 48, 189–197. [Google Scholar] [CrossRef]
- Auta, A.; Hadi, M.A.; Oga, E.; Adewuyi, E.O.; Abdu-Aguye, S.N.; Adeloye, D.; Strickland-Hodge, B.; Morgan, D.J. Global access to antibiotics without prescription in community pharmacies: A systematic review and meta-analysis. J. Infect. 2018, 78, 8–18. [Google Scholar] [CrossRef]

{kind=link}
| Variable and Role in Model | Definition | Levels |
|---|---|---|
| Practices | ||
| AM USE -Outcome | The number of times antimicrobials were reported to be used in an average production month. | Frequency of use 0 = Never 1= 1–2 times 2 = 3–5 times |
| Agrovet Advice-Predictor | Whether an agrovet was sought for advice | 0 = Advice not sought 1 = Advice Sought |
| Feed Distributor Advice-Predictor | Whether a feed distributor was sought for advice | 0 = Advice not sought 1 = Advice Sought |
| Community/Extension Advice-Predictor | Whether a community animal health worker was sought for advice | 0 = Advice not sought 1 = Advice Sought |
| Govt. Veterinarian Advice-Predictor | Whether a government veterinarian was sought for advice | 0 = Advice not sought 1 = Advice Sought |
| Private Veterinarian Advice-Predictor | Whether a private veterinarian was sought for advice | 0 = Advice not sought 1 = Advice Sought |
| Farm Size Standardized-Control | The number of layers on the farm standardized | Continuous |
| Number of Diseases Impacting Flock-Control | The number of diseases a farmer reported as “common” on the farm | Continuous |
| Total Number of Diseases Vaccinated against-Control | The number of diseases a flock was vaccinated against | Continuous |
| Biosecurity Scale-Control | A linear scale indicating the level of biosecurity on the farm. See text above for additional information | Continuous |
| Variable | Definition | Levels |
|---|---|---|
| Practices | ||
| Promoters | Respondent reported using antimicrobials to promote faster or larger growth | 1 = Yes 0 = No |
| Boost eggs | Respondent reported using antimicrobials to boost egg production | 1 = Yes 0 = No |
| Prevention | Respondent reported using antimicrobials to prevent animal getting diseases in the future | 1 = Yes 0 = No |
| Group_treat | Respondents reported using the strategy of treating all birds if a few became sick | 1= Yes 0 = No |
| Stop treat | Respondent reported stopping the recommended treatment period early if animal health improved | 1 = Yes 0 = No |
| Prescrip | Respondent reported almost always getting a prescription before buying antimicrobials | 1 = Yes 0 = No |
| Am docs | Respondent reported giving day old chicks antibiotics upon arrival to the farm | 1 = Yes 0 = No |
| Consume | Respondent reported that products within the withdrawal period (eggs and meat) were consumed at home | 1 = Yes 0 = No |
| Share | Respondent reported that products within the withdrawal period (eggs and meat) were shared with friends and family outside the home | 1 = Yes 0 = No |
| Sell | Respondent reported that products within the withdrawal period (eggs and meat) were sold | 1 = Yes 0 = No |
| Knowledge/perception | ||
| Explain ams | Respondent explained the antimicrobials killed disease | 1 = Yes 0 = No |
| Explain amr | Respondent explained antimicrobial resistance occurred when disease/germs could not be killed by drugs | 1 = Yes 0 = No |
| Amr impact | How much a respondent believed that AMR would impact their future livelihood. (The question was only asked to respondents who could explain AMR (n = 56)). | 0 = No Impact 1 = A little Impact 2 = A large Impact |
| Ghana n = 110 | Kenya n = 76 | |||||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Min | Max | Mean | SD | Min | Max | |
| Age | 36.67 | 13.02 | 18.00 | 64.00 | 49.34 | 14.95 | 23.00 | 80.00 |
| Gender (1 = Female) | 0.23 | 0.42 | - | - | 0.53 | 0.50 | - | - |
| Household Size | 5.28 | 2.89 | 2.00 | 22.00 | 4.80 | 2.98 | 0.00 | 20.00 |
| Employees | 4.23 | 3.25 | 0.00 | 15.00 | 0.97 | 1.07 | 0.00 | 4.00 |
| Years Keeping Layers | 9.35 | 7.30 | 0.10 | 33.00 | 10.88 | 8.39 | 0.25 | 38.00 |
| Flock Size | 9037 | 14,795 | 10.00 | 10,000 | 1079 | 2292 | 90.00 | 19,000 |
| Cage System (1 = Yes) | 0.26 | 0.44 | 0.00 | 1.00 | 0.04 | 0.20 | 0.00 | 1.00 |
| Deep Litter (1 = Yes) | 0.77 | 0.42 | 0.00 | 1.00 | 0.99 | 0.11 | 0.00 | 1.00 |
| Layer Houses | 11.34 | 15.78 | 1.00 | 127.00 | 2.39 | 1.68 | 1.00 | 11.00 |
| Keep Multiple Cohorts | 0.44 | 0.50 | 0.00 | 1.00 | 0.88 | 0.33 | 0.00 | 1.00 |
| Other Animals | 0.71 | 0.46 | 0.00 | 1.00 | 0.95 | 0.22 | 0.00 | 1.00 |
| Keep Records | 0.98 | 0.13 | 0.00 | 1.00 | 0.59 | 0.49 | 0.00 | 1.00 |
| Farm Size (std) | 0.27 | 1.22 | −0.48 | 7.78 | −0.39 | 0.19 | −0.47 | 1.09 |
| Diseases Reported | 2.85 | 1.69 | 0.00 | 9.00 | 2.64 | 1.84 | 0.00 | 7.00 |
| Vaccines Reported | 2.58 | 1.14 | 0.00 | 5.00 | 3.93 | 0.50 | 2.00 | 5.00 |
| Biosecurity Steps | 8.85 | 2.15 | 5.00 | 12.00 | 9.71 | 1.67 | 3.00 | 12.00 |
| Ghana | Kenya | |||
|---|---|---|---|---|
| % Reporting | n | % Reporting | n | |
| Coccidiosis | 63 | 69 | 64 | 49 |
| Infectious Coryza | 21 | 23 | 14 | 11 |
| Chronic Respiratory Disease | 85 | 94 | 63 | 48 |
| Fowl Pox | 14 | 15 | 14 | 11 |
| Fowl Typhoid | 2 | 2 | 13 | 10 |
| Gumboro | 31 | 34 | 34 | 26 |
| Helminthiasis (Worms) | 18 | 20 | 14 | 11 |
| Infectious Bronchitis | 3 | 3 | 8 | 6 |
| Marek’s Disease | 5 | 6 | 4 | 3 |
| Newcastle Diseases | 43 | 47 | 34 | 26 |
| My Birds Never Get Diseases | 2 | 2 | 3 | 2 |
| I Do Not Know Any Diseases | 3 | 3 | 8 | 6 |
| Ghana n = 110 | Kenya n = 76 | |||
|---|---|---|---|---|
| % of HH | n | % of HH | n | |
| AM USE: NEVER | 9 | 10 | 63 | 48 |
| AM USE: 1 to 2 times | 77 | 85 | 33 | 25 |
| AM Use: 3 to 5 times | 14 | 15 | 4 | 3 |
| PROMOTE | 13 | 14 | 11 | 8 |
| BOOST EGGS | 35 | 39 | 11 | 8 |
| PREVENTION | 53 | 58 | 37 | 28 |
| GROUP TREAT | 82 | 90 | 92 | 70 |
| STOP TREAT | 30 | 33 | 12 | 9 |
| NO PRESCRIP | 35 | 39 | 66 | 50 |
| AM DOCs | 69 | 76 | 74 | 56 |
| CONSUME | 75 | 83 | 39 | 30 |
| SHARE | 33 | 36 | 18 | 14 |
| SOLD | 93 | 102 | 87 | 66 |
| EXPLAIN AMs | 84 | 92 | 83 | 63 |
| EXPLAIN AMR | 58 | 64 | 53 | 40 |
| AMR IMPACT Not Worried (=0) | 9 | 10 | 4 | 3 |
| AMR IMPACT A Little Worried (=1) | 25 | 28 | 3 | 2 |
| AMR IMPACT Very Worried (=2) | 24 | 26 | 46 | 35 |
| AHSP: Seeking Frequency | Practice/Attitude | % Responding “Yes” | Letter |
|---|---|---|---|
| Agrovet: never/rarely | Always get prescription | 11.83 | a |
| Agrovet: sometimes | Always get prescription | 10.75 | ab |
| Agrovet: almost always | Always get prescription | 24.73 | b |
| Extension: never/rarely | Consume withdrawal products | 27.96 | a |
| Extension: sometimes | Consume withdrawal products | 17.20 | b |
| Extension: almost always | Consume withdrawal products | 15.59 | b |
| Extension: never/rarely | Can explain AMR | 29.35 | a |
| Extension: sometimes | Can explain AMR | 11.96 | a |
| Extension: almost always | Can explain AMR | 15.22 | b |
| Feed company: never/rarely | Share withdrawal products | 17.20 | a |
| Feed company: sometimes | Share withdrawal products | 9.14 | b |
| Feed company: almost always | Share withdrawal products | 0.54 | a |
| Govt. veterinarian: never/rarely | Always get prescription | 26.34 | ab |
| Govt. veterinarian: sometimes | Always get prescription | 3.76 | a |
| Govt. veterinarian: almost always | Always get prescription | 17.20 | b |
| Priv. veterinarian: never/rarely | Give AMs to boost egg production | 20.43 | a |
| Priv. veterinarian: sometimes | Give AMs to boost egg production | 3.76 | a |
| Priv. veterinarian: almost always | Give AMs to boost egg production | 1.08 | b |
| Priv. veterinarian: never/rarely | Always get prescription | 27.96 | a |
| Priv. veterinarian: sometimes | Always get prescription | 5.91 | ab |
| Priv. veterinarian: almost always | Always get prescription | 13.44 | b |
| Priv. veterinarian: never/rarely | Use AM as growth promoters | 8.06 | ab |
| Priv. veterinarian: sometimes | Use AM as growth promoters | 3.23 | a |
| Priv. veterinarian: almost always | Use AM as growth promoters | 0.54 | b |
| Variables | AMU Odds Ratio (95% CI) |
|---|---|
| Agrovet Advice | 0.68 (0.34–1.35) |
| Feed Distributor Advice | 1.65 (0.78–3.51) |
| Community/Extension Advice | 0.63 (0.29–1.40) |
| Govt. Veterinarian Advice | 1.86 (0.86–4.01) |
| Private Veterinarian Advice | 1.08 (0.54–2.17) |
| Farm Size Standardized | 1.13 (0.83–1.55) |
| Number of Diseases Impacting Flock | 1.31 *** (1.09–1.58) |
| Total Number of Diseases Vaccinated Against | 0.46 *** (0.33–0.63) |
| Biosecurity Scale | 0.81 ** (0.69–0.96) |
| Observations | 186 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Afakye, K.; Kiambi, S.; Koka, E.; Kabali, E.; Dorado-Garcia, A.; Amoah, A.; Kimani, T.; Adjei, B.; Caudell, M.A. The Impacts of Animal Health Service Providers on Antimicrobial Use Attitudes and Practices: An Examination of Poultry Layer Farmers in Ghana and Kenya. Antibiotics 2020, 9, 554. https://doi.org/10.3390/antibiotics9090554
Afakye K, Kiambi S, Koka E, Kabali E, Dorado-Garcia A, Amoah A, Kimani T, Adjei B, Caudell MA. The Impacts of Animal Health Service Providers on Antimicrobial Use Attitudes and Practices: An Examination of Poultry Layer Farmers in Ghana and Kenya. Antibiotics. 2020; 9(9):554. https://doi.org/10.3390/antibiotics9090554
Chicago/Turabian StyleAfakye, Kofi, Stella Kiambi, Eric Koka, Emmanuel Kabali, Alejandro Dorado-Garcia, Ann Amoah, Tabitha Kimani, Benjamin Adjei, and Mark A Caudell. 2020. "The Impacts of Animal Health Service Providers on Antimicrobial Use Attitudes and Practices: An Examination of Poultry Layer Farmers in Ghana and Kenya" Antibiotics 9, no. 9: 554. https://doi.org/10.3390/antibiotics9090554
APA StyleAfakye, K., Kiambi, S., Koka, E., Kabali, E., Dorado-Garcia, A., Amoah, A., Kimani, T., Adjei, B., & Caudell, M. A. (2020). The Impacts of Animal Health Service Providers on Antimicrobial Use Attitudes and Practices: An Examination of Poultry Layer Farmers in Ghana and Kenya. Antibiotics, 9(9), 554. https://doi.org/10.3390/antibiotics9090554