Influence of Probiotics on the Salivary Microflora Oral Streptococci and Their Integration into Oral Biofilm

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample Size Calculation
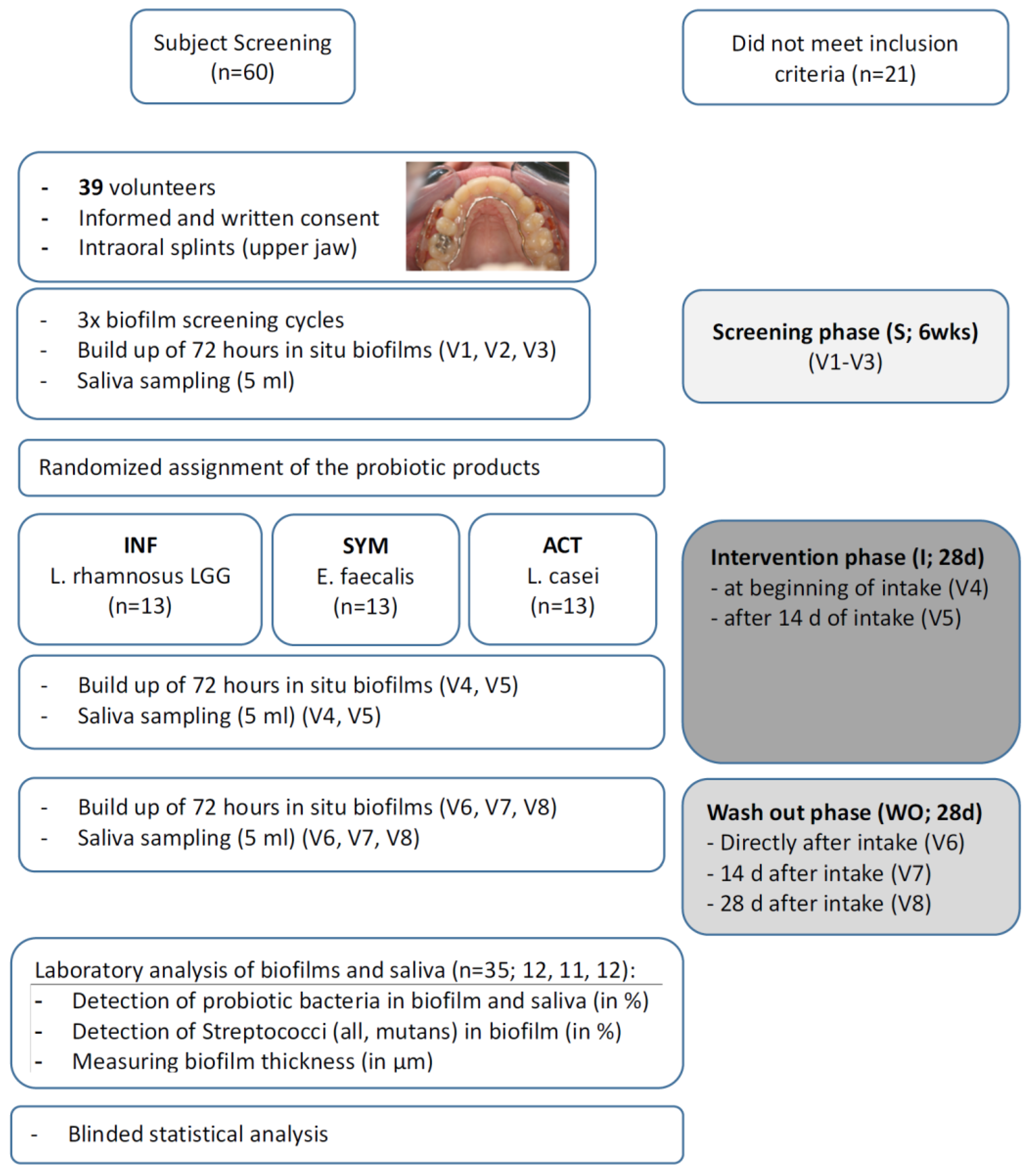
2.2. Study Design and Population
2.3. Grow-up of In Situ Biofilms
2.4. Study Course and Products
- Treatment 1: Enterococcus faecalis (SYM), Symbioflor 1 (SymbioPharm GmbH, Herborn, Germany); 30 drops, three times daily (=5 × 50 mL bottles);
- Treatment 2: Lactobacillus casei DN-114 001 (ACT), Actimel Classic (Danone GmbH, Munich, Germany); once daily, before lunch (=28 bottles during intervention);
- Treatment 3: Lactobacillus rhamnosus GG (INF); InfectoDiarrstop (InfectoPharm GmbH, Heppenheim, Germany), twice daily (morning and evening), diluted in water (=56 sachets).
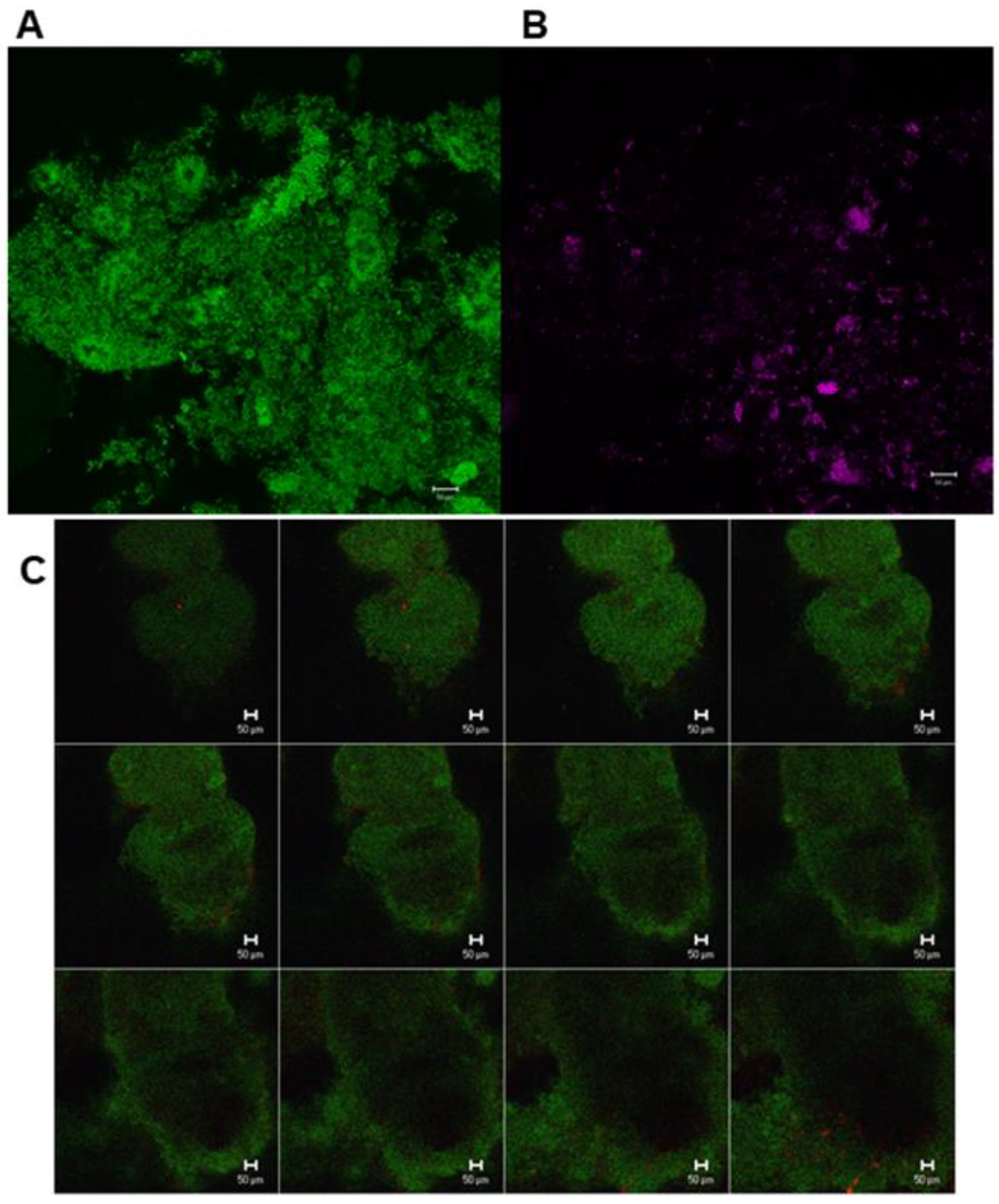
2.5. Fluorescence In Situ Hybridization (FISH)
- EUB 338 (5′-GCTGCCTCCGTAGGAGT-3′) for eubacteria (total count of all bacteria, [34]);
- LGC358a (5′-CCA TTG TGG AAG ATT CCC T-3′) for Lactobacillus spp. [35];
- Efs 129 (5′-CCCTCTGATGGGTAGGTT-3′) for Enterococcus faecalis [36];
- STR 405 (5′-TAG CCG TCC CTT TCT GGT-3′) for Streptococcus spp. [37];
- L-Ssob440-2 (5′ CAC ACG TTC TTC CCC TAC-3′) for S. sobrinus [35].
2.6. CLSM Analysis
2.7. Confirmation of Probiotic Bacteria by Culture Technique, MALDI-TOF and DNA Fingerprinting
2.8. Statistical Analysis
3. Results
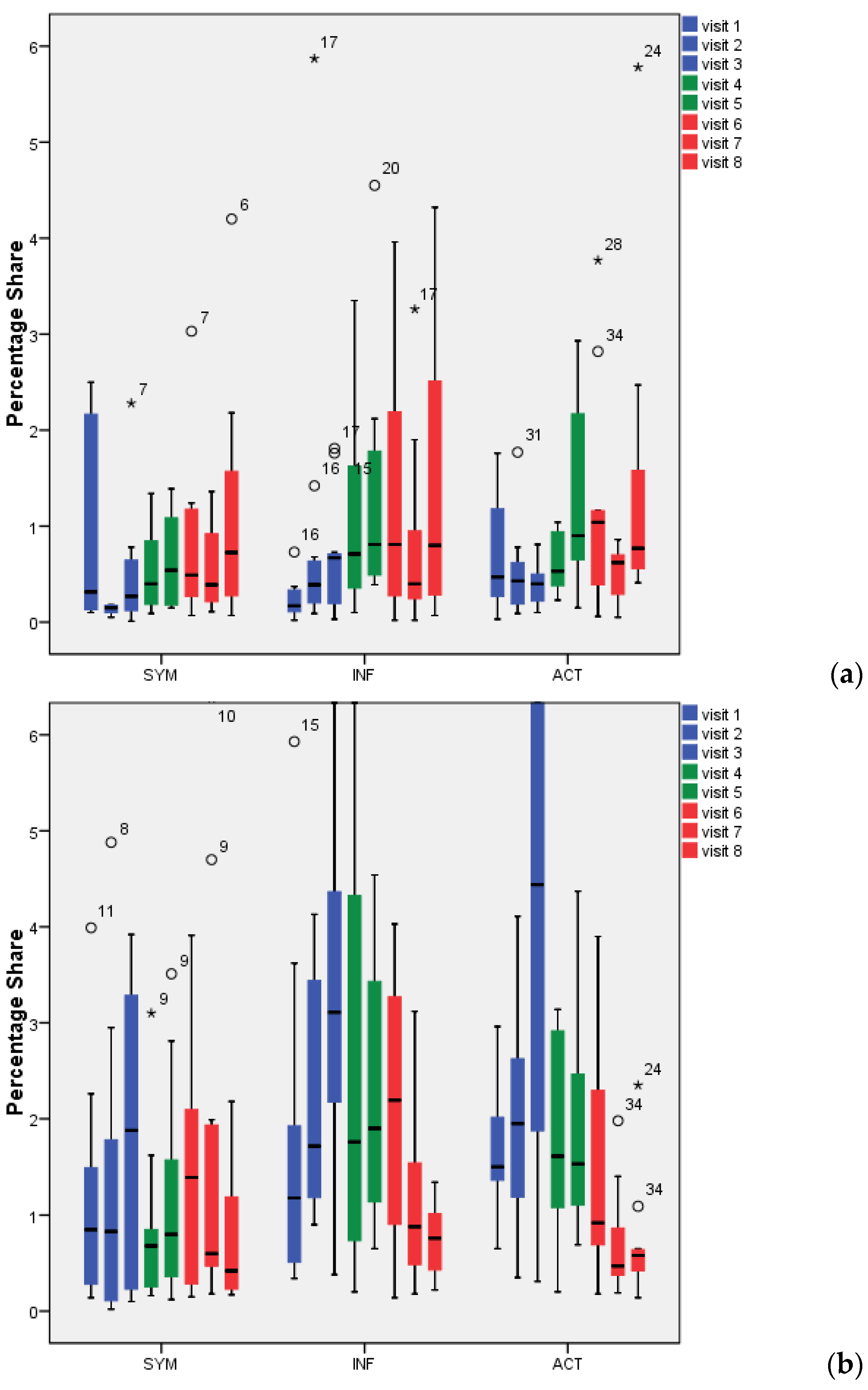
3.1. Detection and Percentage of Probiotic Bacteria by Multiplex FISH in Biofilm
3.2. Detection and Percentage of Probiotic Bacteria by Multiplex FISH in Saliva
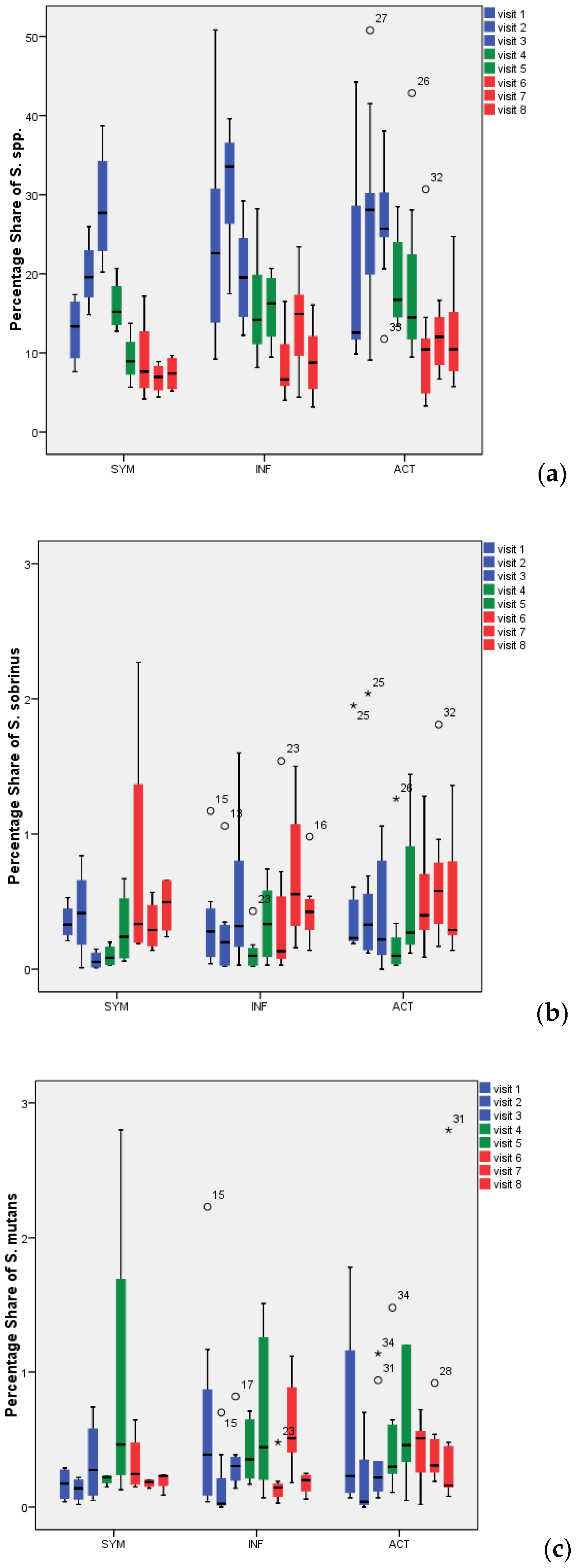
3.3. Detection and Percentage of Streptococci by Multiplex FISH in Biofilm
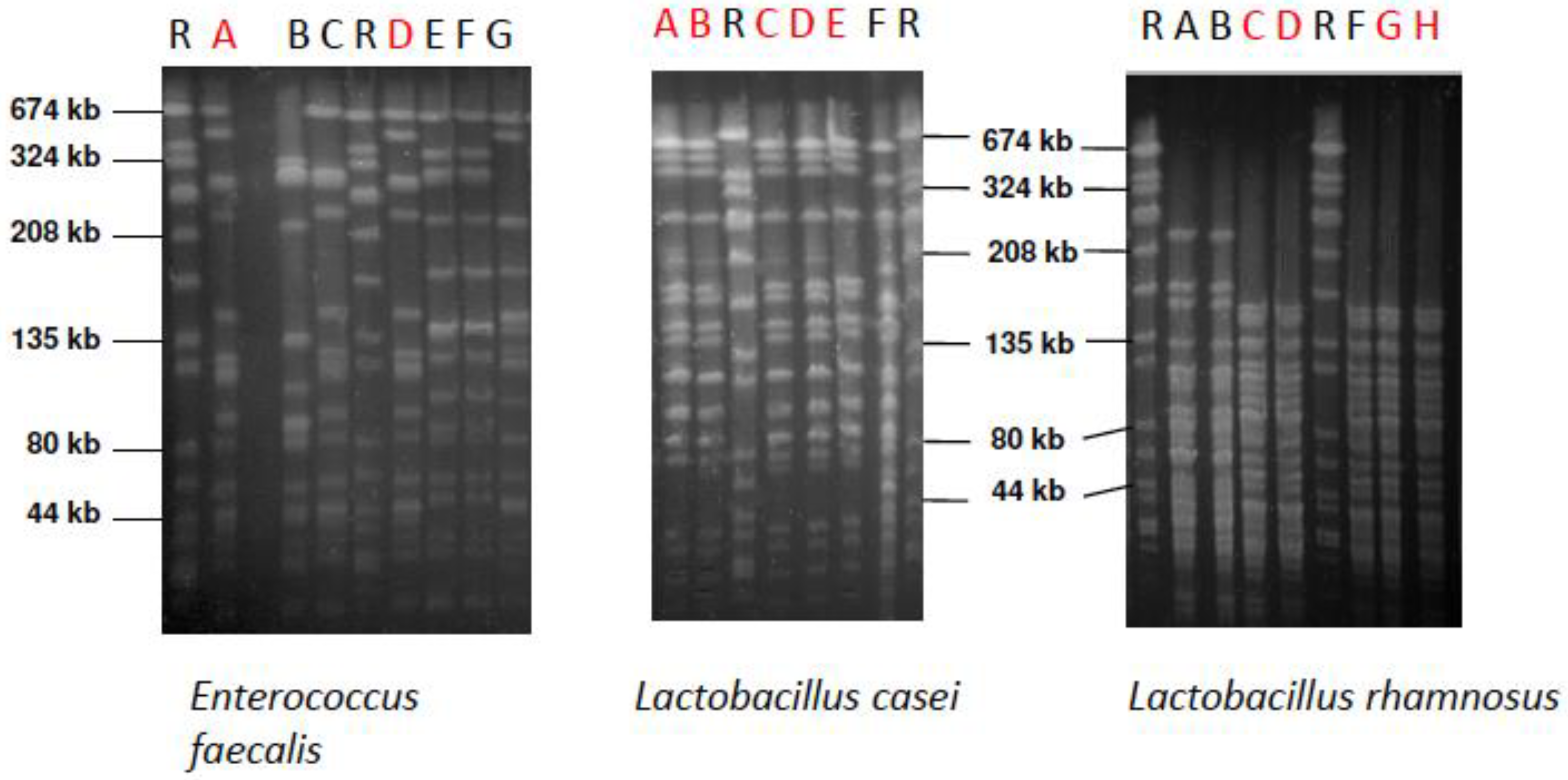
3.4. Culture Technique and DNA Fingerprinting
3.5. Biofilm Thickness (in µm)
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Available online: https://www.fortunebusinessinsights.com/industry-reports/probiotics-market-100083 (accessed on 12 November 2020).
- Sanders, M.E.; Merenstein, D.J.; Reid, G. Probiotics and prebiotics in intestinal health and disease: From biology to the clinic. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 605–616. [Google Scholar] [CrossRef] [PubMed]
- Vitetta, L.; Vitetta, G.; Hall, S. Immunological tolerance and function: Associations between intestinal bacteria, probiotics, prebiotics, and phages. Front. Immunol. 2018, 9, 2240. [Google Scholar] [CrossRef] [PubMed]
- Forsberg, A.; West, C.E.; Prescott, S.L.; Jenmalm, M.C. Pre- and probiotics for allergy prevention: Time to revisit recommendations? Clin. Exp. Allergy J. Br. Soc. Allergy Clin. Immunol. 2016, 46, 1506–1521. [Google Scholar] [CrossRef] [PubMed]
- Haß, U.; Herpich, C.; Norman, K. Anti-inflammatory diets and fatigue. Nutrients 2019, 11, 2315. [Google Scholar] [CrossRef]
- Kanauchi, O.; Andoh, A.; AbuBakar, S.; Yamamoto, N. Probiotics and paraprobiotics in viral infection: Clinical application and effects on the innate and acquired immune systems. Curr. Pharm. Des. 2018, 24, 710–717. [Google Scholar] [CrossRef]
- Vuotto, C.; Longo, F.; Donelli, G. Probiotics to counteract biofilm-associated infections: Promising and conflicting data. Int. J. Oral Sci. 2014, 6, 189–194. [Google Scholar] [CrossRef]
- Gruner, D.; Paris, S.; Schwendicke, F. Probiotics for managing caries and periodontitis: Systematic review and meta-analysis. J. Dent. 2016, 48, 16–25. [Google Scholar] [CrossRef]
- Laleman, I.; Detailleur, V.; Slot, D.E.; Slomka, V.; Quirynen, M.; Teughels, W. Probiotics reduce mutans streptococci counts in humans: A systematic review and meta-analysis. Clin. Oral Investig. 2014, 18, 1539–1552. [Google Scholar] [CrossRef]
- Schwendicke, F.; Dörfer, C.; Kneist, S.; Meyer-Lueckel, H.; Paris, S. Cariogenic effects of probiotic lactobacillus rhamnosus gg in a dental biofilm model. Caries Res. 2014, 48, 186–192. [Google Scholar] [CrossRef]
- Schwendicke, F.; Korte, F.; Dörfer, C.E.; Kneist, S.; Fawzy El-Sayed, K.; Paris, S. Inhibition of streptococcus mutans growth and biofilm formation by probiotics in vitro. Caries Res. 2017, 51, 87–95. [Google Scholar] [CrossRef]
- Teughels, W.; Loozen, G.; Quirynen, M. Do probiotics offer opportunities to manipulate the periodontal oral microbiota? J. Clin. Periodontol. 2011, 38 (Suppl. 11), 159–177. [Google Scholar] [CrossRef] [PubMed]
- Xu, F.; Fu, Y.; Sun, T.-Y.; Jiang, Z.; Miao, Z.; Shuai, M.; Gou, W.; Ling, C.W.; Yang, J.; Wang, J.; et al. The interplay between host genetics and the gut microbiome reveals common and distinct microbiome features for complex human diseases. Microbiome 2020, 8, 145. [Google Scholar] [CrossRef] [PubMed]
- Costalonga, M.; Herzberg, M.C. The oral microbiome and the immunobiology of periodontal disease and caries. Immunol. Lett. 2014, 162, 22–38. [Google Scholar] [CrossRef] [PubMed]
- Sampaio-Maia, B.; Caldas, I.M.; Pereira, M.L.; Pérez-Mongiovi, D.; Araujo, R. The Oral Microbiome in Health and Its Implication in Oral and Systemic Diseases. Adv. Appl. Microbiol. 2016, 97, 171–210. [Google Scholar] [PubMed]
- Willis, J.R.; Gabaldón, T. The Human Oral Microbiome in Health and Disease: From Sequences to Ecosystems. Microorganisms 2020, 8, 308. [Google Scholar] [CrossRef]
- Khumaedi, A.I.; Purnamasari, D.; Wijaya, I.P.; Soeroso, Y. The relationship of diabetes, periodontitis and cardiovascular disease. Diabetes Metab. Syndr. 2019, 13, 1675–1678. [Google Scholar] [CrossRef]
- Sanz, M.; Marco Del Castillo, A.; Jepsen, S.; Gonzalez-Juanatey, J.R.; D’Aiuto, F.; Bouchard, P.; Chapple, I.; Dietrich, T.; Gotsman, I.; Graziani, F.; et al. Periodontitis and cardiovascular diseases: Consensus report. J. Clin. Periodontol. 2020, 47, 268–288. [Google Scholar] [CrossRef]
- Sapey, E.; Yonel, Z.; Edgar, R.; Parmar, S.; Hobbins, S.; Newby, P.; Crossley, D.; Usher, A.; Johnson, S.; Walton, G.M.; et al. The clinical and inflammatory relationships between periodontitis and chronic obstructive pulmonary disease. J. Clin. Periodontol. 2020, 47, 1040–1052. [Google Scholar] [CrossRef]
- Jepsen, S.; Suvan, J.; Deschner, J. The association of periodontal diseases with metabolic syndrome and obesity. Periodontology 2020, 83, 125–153. [Google Scholar] [CrossRef]
- Anderson, A.C.; Rothballer, M.; Altenburger, M.J.; Woelber, J.P.; Karygianni, L.; Lagkouvardos, I.; Hellwig, E.; Al-Ahmad, A. In-vivo shift of the microbiota in oral biofilm in response to frequent sucrose consumption. Sci. Rep. 2018, 8, 14202. [Google Scholar] [CrossRef]
- Pihlstrom, B.L.; Michalowicz, B.S.; Johnson, N.W. Periodontal diseases. Lancet Lond. Engl. 2005, 366, 1809–1820. [Google Scholar] [CrossRef]
- Arweiler, N.B.; Auschill, T.M.; Sculean, A. Patient self-care of periodontal pocket infections. Periodontology 2000 2018, 76, 164–179. [Google Scholar] [CrossRef] [PubMed]
- Zandbergen, D.; Slot, D.E.; Cobb, C.M.; Van der Weijden, F.A. The clinical effect of scaling and root planing and the concomitant administration of systemic amoxicillin and metronidazole: A systematic review. J. Periodontol. 2013, 84, 332–351. [Google Scholar] [CrossRef]
- Teughels, W.; Van Essche, M.; Sliepen, I.; Quirynen, M. Probiotics and oral healthcare. Periodontology 2000 2008, 48, 111–147. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, M.; Tsuji, M.; Sasaki, H.; Fujita, K.; Nomura, R.; Nakano, K.; Shintani, S.; Ooshima, T. Cariogenicity of the probiotic bacterium lactobacillus salivarius in rats. Caries Res. 2005, 39, 479–483. [Google Scholar] [CrossRef]
- Twetman, L.; Larsen, U.; Fiehn, N.E.; Stecksén-Blicks, C.; Twetman, S. Coaggregation between probiotic bacteria and caries-associated strains: An in vitro study. Acta Odontol. Scand. 2009, 67, 284–288. [Google Scholar] [CrossRef]
- Willcox, M.D.; Patrikakis, M.; Harty, D.W.; Loo, C.Y.; Knox, K.W. Coaggregation of oral lactobacilli with streptococci from the oral cavity. Oral Microbiol. Immunol. 1993, 8, 319–321. [Google Scholar] [CrossRef]
- Lodi, C.S.; Oliveira, L.V.; Brighenti, F.L.; Delbem, A.C.; Martinhon, C.C. Effects of probiotic fermented milk on biofilms, oral microbiota, and enamel. Braz. Oral Res. 2015, 29. [Google Scholar] [CrossRef]
- Ravn, I.; Dige, I.; Meyer, R.L.; Nyvad, B. Colonization of the oral cavity by probiotic bacteria. Caries Res. 2012, 46, 107–112. [Google Scholar] [CrossRef]
- Arweiler, N.B.; Netuschil, L.; Beier, D.; Grunert, S.; Heumann, C.; Altenburger, M.J.; Sculean, A.; Nagy, K.; Al-Ahmad, A.; Auschill, T.M. Action of food preservatives on 14-days dental biofilm formation, biofilm vitality and biofilm-derived enamel demineralisation in situ. Clin. Oral Investig. 2014, 18, 829–838. [Google Scholar] [CrossRef]
- Fan, X.; Peters, B.A.; Min, D.; Ahn, J.; Hayes, R.B. Comparison of the oral microbiome in mouthwash and whole saliva samples. PLoS ONE 2018, 13, e0194729. [Google Scholar] [CrossRef] [PubMed]
- Jo, R.; Nishimoto, Y.; Umezawa, K.; Yama, K.; Aita, Y.; Ichiba, Y.; Murakami, S.; Kakizawa, Y.; Kumagai, T.; Yamada, T.; et al. Comparison of oral microbiome profiles in stimulated and unstimulated saliva, tongue, and mouth-rinsed water. Sci. Rep. 2019, 9, 16124. [Google Scholar] [CrossRef] [PubMed]
- Amann, R.I.; Binder, B.J.; Olson, R.J.; Chisholm, S.W.; Devereux, R.; Stahl, D.A. Combination of 16s rrna-targeted oligonucleotide probes with flow cytometry for analyzing mixed microbial populations. Appl. Environ. Microbiol. 1990, 56, 1919–1925. [Google Scholar] [CrossRef]
- Quevedo, B.; Giertsen, E.; Zijnge, V.; Lüthi-Schaller, H.; Guggenheim, B.; Thurnheer, T.; Gmür, R. Phylogenetic group- and species-specific oligonucleotide probes for single-cell detection of lactic acid bacteria in oral biofilms. BMC Microbiol. 2011, 11, 14. [Google Scholar] [CrossRef] [PubMed]
- Behr, T.; Koob, C.; Schedl, M.; Mehlen, A.; Meier, H.; Knopp, D.; Frahm, E.; Obst, U.; Schleifer, K.; Niessner, R.; et al. A nested array of rrna targeted probes for the detection and identification of enterococci by reverse hybridization. Syst. Appl. Microbiol. 2000, 23, 563–572. [Google Scholar] [CrossRef]
- Paster, B.J.; Bartoszyk, I.M.; Dewhirst, F.E. Identification of oral streptococci using pcr-based, reverse-capture, checkerboard hybridization. Methods Cell Sci. 1998, 20, 223–231. [Google Scholar] [CrossRef]
- Thurnheer, T.; Gmür, R.; Giertsen, E.; Guggenheim, B. Automated fluorescent in situ hybridization for the specific detection and quantification of oral streptococci in dental plaque. J. Microbiol. Methods 2001, 44, 39–47. [Google Scholar] [CrossRef]
- Al-Ahmad, A.; Roth, D.; Wolkewitz, M.; Wiedmann-Al-Ahmad, M.; Follo, M.; Ratka-Krüger, P.; Deimling, D.; Hellwig, E.; Hannig, C. Change in diet and oral hygiene over an 8-week period: Effects on oral health and oral biofilm. Clin. Oral Investig. 2010, 14, 391–396. [Google Scholar] [CrossRef]
- Al-Ahmad, A.; Wunder, A.; Auschill, T.M.; Follo, M.; Braun, G.; Hellwig, E.; Arweiler, N.B. The in vivo dynamics of streptococcus spp., actinomyces naeslundii, fusobacterium nucleatum and veillonella spp. In dental plaque biofilm as analysed by five-colour multiplex fluorescence in situ hybridization. J. Med. Microbiol. 2007, 56, 681–687. [Google Scholar] [CrossRef]
- Anderson, A.C.; Sanunu, M.; Schneider, C.; Clad, A.; Karygianni, L.; Hellwig, E.; Al-Ahmad, A. Rapid species-level identification of vaginal and oral lactobacilli using maldi-tof ms analysis and 16s rdna sequencing. BMC Microbiol. 2014, 14, 312. [Google Scholar] [CrossRef]
- Matushek, M.G.; Bonten, M.J.; Hayden, M.K. Rapid preparation of bacterial DNA for pulsed-field gel electrophoresis. J. Clin. Microbiol. 1996, 34, 2598–2600. [Google Scholar] [CrossRef] [PubMed]
- Klare, I.; Konstabel, C.; Mueller-Bertling, S.; Werner, G.; Strommenger, B.; Kettlitz, C.; Borgmann, S.; Schulte, B.; Jonas, D.; Serr, A.; et al. Spread of ampicillin/vancomycin-resistant enterococcus faecium of the epidemic-virulent clonal complex-17 carrying the genes esp and hyl in German hospitals. Eur. J. Clin. Microbiol. Infect. Dis. Off. Publ. Eur. Soc. Clin. Microbiol. 2005, 24, 815–825. [Google Scholar] [CrossRef] [PubMed]
- Al-Ahmad, A.; Maier, J.; Follo, M.; Spitzmüller, B.; Wittmer, A.; Hellwig, E.; Hübner, J.; Jonas, D. Food-borne enterococci integrate into oral biofilm: An in vivo study. J. Endod. 2010, 36, 1812–1819. [Google Scholar] [CrossRef] [PubMed]
- Comelli, E.M.; Guggenheim, B.; Stingele, F.; Neeser, J.R. Selection of dairy bacterial strains as probiotics for oral health. Eur. J. Oral Sci. 2002, 110, 218–224. [Google Scholar] [CrossRef] [PubMed]
- Stamatova, I.; Kari, K.; Vladimirov, S.; Meurman, J.H. In vitro evaluation of yoghurt starter lactobacilli and lactobacillus rhamnosus gg adhesion to saliva-coated surfaces. Oral Microbiol. Immunol. 2009, 24, 218–223. [Google Scholar] [CrossRef]
- Seerangaiyan, K.; Jüch, F.; Winkel, E.G. Tongue coating: Its characteristics and role in intra-oral halitosis and general health-a review. J. Breath Res. 2018, 12, 034001. [Google Scholar] [CrossRef]
- Danser, M.M.; Gómez, S.M.; Van der Weijden, G.A. Tongue coating and tongue brushing: A literature review. Int. J. Dent. Hyg. 2003, 1, 151–158. [Google Scholar] [CrossRef]
- Bernardi, S.; Karygianni, L.; Filippi, A.; Anderson, A.; Zurcher, A.; Hellwig, E.; Vach, K.; Macchiarelli, G.; Al-Ahmad, A. Combining culture and culture independent methods reveals new microbial composition of Halitosis patients’ tongue biofilm. Microbiol. Open 2020, 9, e958. [Google Scholar] [CrossRef]
- Michalek, S.M.; Hirasawa, M.; Kiyono, H.; Ochiai, K.; McGhee, J.R. Oral ecology and virulence of lactobacillus casei and streptococcus mutans in gnotobiotic rats. Infect. Immun. 1981, 33, 690–696. [Google Scholar] [CrossRef]
- Näse, L.; Hatakka, K.; Savilahti, E.; Saxelin, M.; Pönkä, A.; Poussa, T.; Korpela, R.; Meurman, J.H. Effect of long-term consumption of a probiotic bacterium, lactobacillus rhamnosus gg, in milk on dental caries and caries risk in children. Caries Res. 2001, 35, 412–420. [Google Scholar] [CrossRef]
- Stecksén-Blicks, C.; Sjöström, I.; Twetman, S. Effect of long-term consumption of milk supplemented with probiotic lactobacilli and fluoride on dental caries and general health in preschool children: A cluster-randomized study. Caries Res. 2009, 43, 374–381. [Google Scholar] [CrossRef] [PubMed]
- Keller, M.K.; Hasslöf, P.; Stecksén-Blicks, C.; Twetman, S. Co-aggregation and growth inhibition of probiotic lactobacilli and clinical isolates of mutans streptococci: An in vitro study. Acta Odontol. Scand. 2011, 69, 263–268. [Google Scholar] [CrossRef] [PubMed]
- Simark-Mattsson, C.; Emilson, C.G.; Håkansson, E.G.; Jacobsson, C.; Roos, K.; Holm, S. Lactobacillus-mediated interference of mutans streptococci in caries-free vs. Caries-active subjects. Eur. J. Oral Sci. 2007, 115, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Koliarakis, I.; Messaritakis, I.; Nikolouzakis, T.K.; Hamilos, G.; Souglakos, J.; Tsiaoussis, J. Oral Bacteria and Intestinal Dysbiosis in Colorectal Cancer. Int. J. Mol. Sci. 2019, 20, 4146. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter (in Comparison to Screening) | SYM | INF | ACT |
|---|---|---|---|
| Biofilm | |||
| % PB V4 | 0.477; n.s. | 0.754; n.s. | 0.347; n.s. |
| % PB V5 | 0.241; n.s. | 0.286; n.s. | 0.155; n.s. |
| % PB V6 | 0.477; n.s. | 0.209; n.s. | 0.286; n.s. |
| % PB V7 | 0.594; n.s. | 0.530; n.s. | 0.110; n.s. |
| % PB V8 | 0.959; n.s. | 0.308; n.s. | 0.239; n.s. |
| Saliva | |||
| % PB V4 | 0.328; n.s. | 0.433; n.s. | 0.182; n.s. |
| % PB V5 | 0.534; n.s. | 0.388; n.s. | 0.091; n.s. |
| % PB V6 | 0.790; n.s. | 0.272; n.s. | 0.034; * |
| % PB V7 | 0.790; n.s. | 0.010; ** | 0.003; ** |
| % PB V8 | 0.142; n.s. | 0.002; ** | 0.003; ** |
| Biofilm | |||
| % Streptococcus spp. V4 | 0.028; * | 0.003; ** | 0.091; n.s. |
| % Streptococcus spp. V5 | 0.008; ** | 0.002; ** | 0.328; n.s. |
| % Streptococcus spp. V6 | 0.008; ** | 0.002; ** | 0.010; ** |
| % Streptococcus spp. V7 | 0.011; * | 0.005; ** | 0.003; ** |
| % Streptococcus spp. V8 | 0.012; * | 0.003; ** | 0.007; ** |
| % S. mutans V4 | 0.028; * | 0.754; n.s. | 0.657; n.s. |
| % S. mutans V5 | 0.021; ** | 0.099; n.s. | 0.286; n.s. |
| % S. mutans V6 | 0.038; * | 0.099; n.s. | 0.424; n.s. |
| % S. mutans V7 | 0.260; n.s. | 0.114; n.s. | 1.000; n.s. |
| % S. mutans V8 | 0.327; n.s. | 0.110; n.s. | 0.838; n.s. |
| % S. sobrinus V4 | 0.333; n.s. | 0.008; **. | 0.182; n.s. |
| % S. sobrinus V5 | 0.260; n.s. | 0.695; n.s. | 0.824; n.s. |
| % S. sobrinus V6 | 0.123; n.s. | 0.583; n.s. | 0.959; n.s. |
| % S. sobrinus V7 | 0.260; n.s. | 0.114; n.s. | 0.213; n.s. |
| % S. sobrinus V8 | 0.036; * | 0.477; n.s. | 0.314; n.s. |
| BT (in µm) V4 | 0.047; * | 0.092; n.s. | 0.575; n.s. |
| BT (in µm) V5 | 0.015; * | 0.505; n.s. | 0.131; n.s. |
| BT (in µm) V6 | 0.021; * | 0.814; n.s. | 1.000; n.s. |
| BT (in µm) V7 | 0.086; n.s. | 0.959; n.s. | 0.062; n.s. |
| BT (in µm) V8 | 0.401; n.s. | 0.110; n.s. | 0.374; n.s. |
| Lactobacillus casei | Lactobacillus rhamnosus | Enterococcus faecalis | ||||
|---|---|---|---|---|---|---|
| Participant # | Range/BES * | Participant # | Range/BES * | Participant # | Range/BES * | |
| Screening (S) /Biofilm | 1 | 10–500 | 2 | 10–40 | ||
| Ingestion (I)/Biofilm | 6 | 20–700 | 3 | 10–100 | ||
| Wash out (WO)/Biofilm | 2 | 500 | 2 | 20–100 | 1 | 2 × 103 |
| Screening (S)/Saliva | 2 | 200–104 | 3 | 40–1000 | 1 | 10 |
| Ingestion (I)/Saliva | 4 | 200–105 | 7 | 100–104 | ||
| Wash out (WO)/Saliva | 5 | 30–2.2 × 103 | 4 | 20–2000 | ||
| SYM | INF | ACT | |
|---|---|---|---|
| Screening (V1–V3) | 15.59 ± 5.41 | 15.54 ± 5.50 | 14.10 ± 4.54 |
| Intake (V4) | 11.00 ± 3.04 | 12.45 ± 3.34 | 13.03 ± 4.04 |
| Intake (V5) | 11.85 ± 5.44 | 14.89 ± 5.71 | 12.09 ± 5.42 |
| Wash-out (V6) | 11.18 ± 2.40 | 15.22 ± 6.57 | 13.82 ± 5.56 |
| Wash-out (V7) | 12.93 ± 5.05 | 15.93 ± 5.16 | 19.27 ± 6.77 |
| Wash-out (V8) | 16.75 ± 4.40 | 20.85 ± 7.71 | 18.76 ± 11.85 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arweiler, N.B.; Auschill, T.M.; Heumann, C.; Hellwig, E.; Al-Ahmad, A. Influence of Probiotics on the Salivary Microflora Oral Streptococci and Their Integration into Oral Biofilm. Antibiotics 2020, 9, 803. https://doi.org/10.3390/antibiotics9110803
Arweiler NB, Auschill TM, Heumann C, Hellwig E, Al-Ahmad A. Influence of Probiotics on the Salivary Microflora Oral Streptococci and Their Integration into Oral Biofilm. Antibiotics. 2020; 9(11):803. https://doi.org/10.3390/antibiotics9110803
Chicago/Turabian StyleArweiler, Nicole B., Thorsten M. Auschill, Christian Heumann, Elmar Hellwig, and Ali Al-Ahmad. 2020. "Influence of Probiotics on the Salivary Microflora Oral Streptococci and Their Integration into Oral Biofilm" Antibiotics 9, no. 11: 803. https://doi.org/10.3390/antibiotics9110803
APA StyleArweiler, N. B., Auschill, T. M., Heumann, C., Hellwig, E., & Al-Ahmad, A. (2020). Influence of Probiotics on the Salivary Microflora Oral Streptococci and Their Integration into Oral Biofilm. Antibiotics, 9(11), 803. https://doi.org/10.3390/antibiotics9110803