Tedizolid Versus Linezolid for the Treatment of Acute Bacterial Skin and Skin Structure Infection: A Systematic Review and Meta-Analysis

 , and
, and
Abstract
:1. Introduction
2. Methods
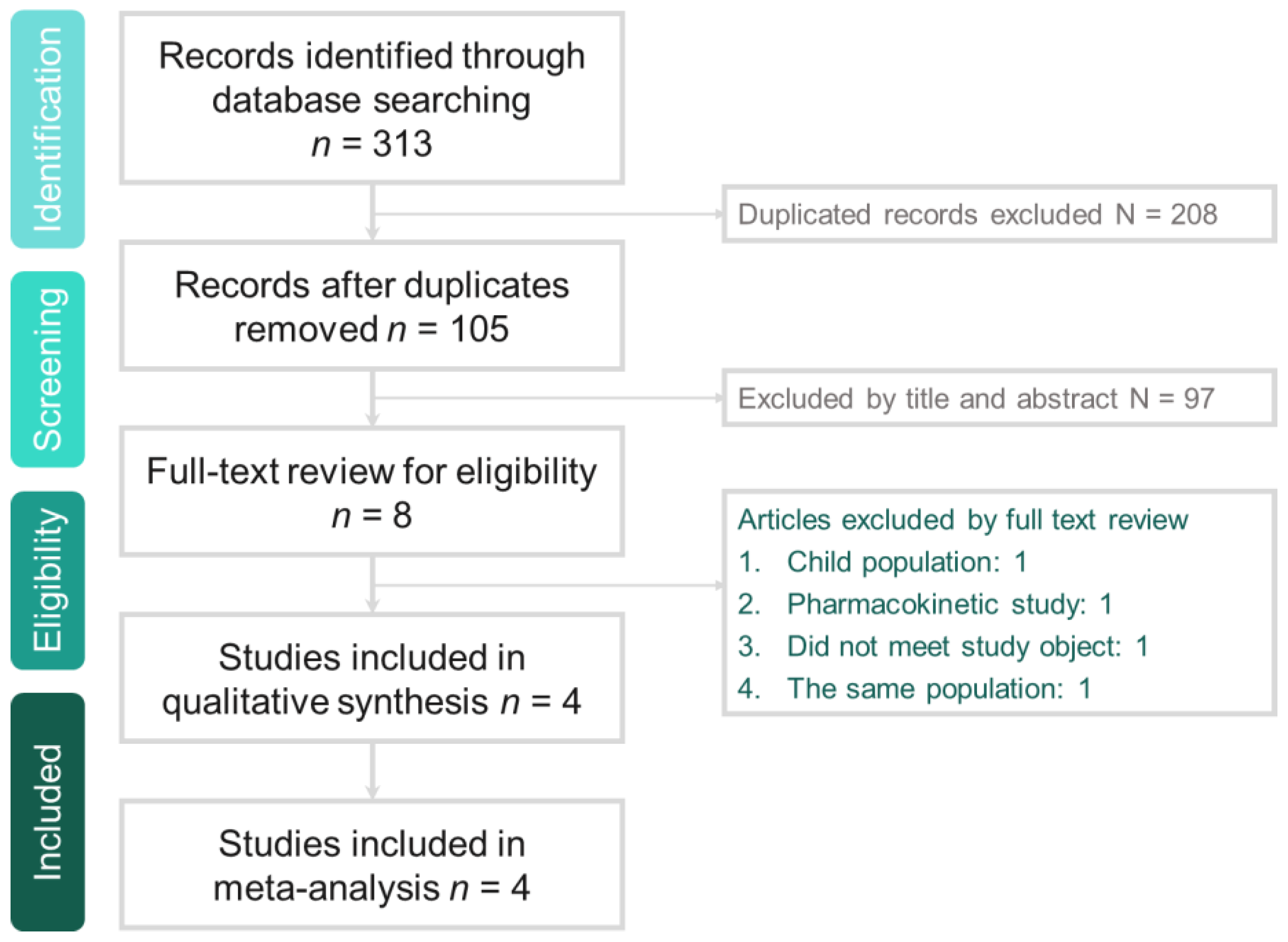
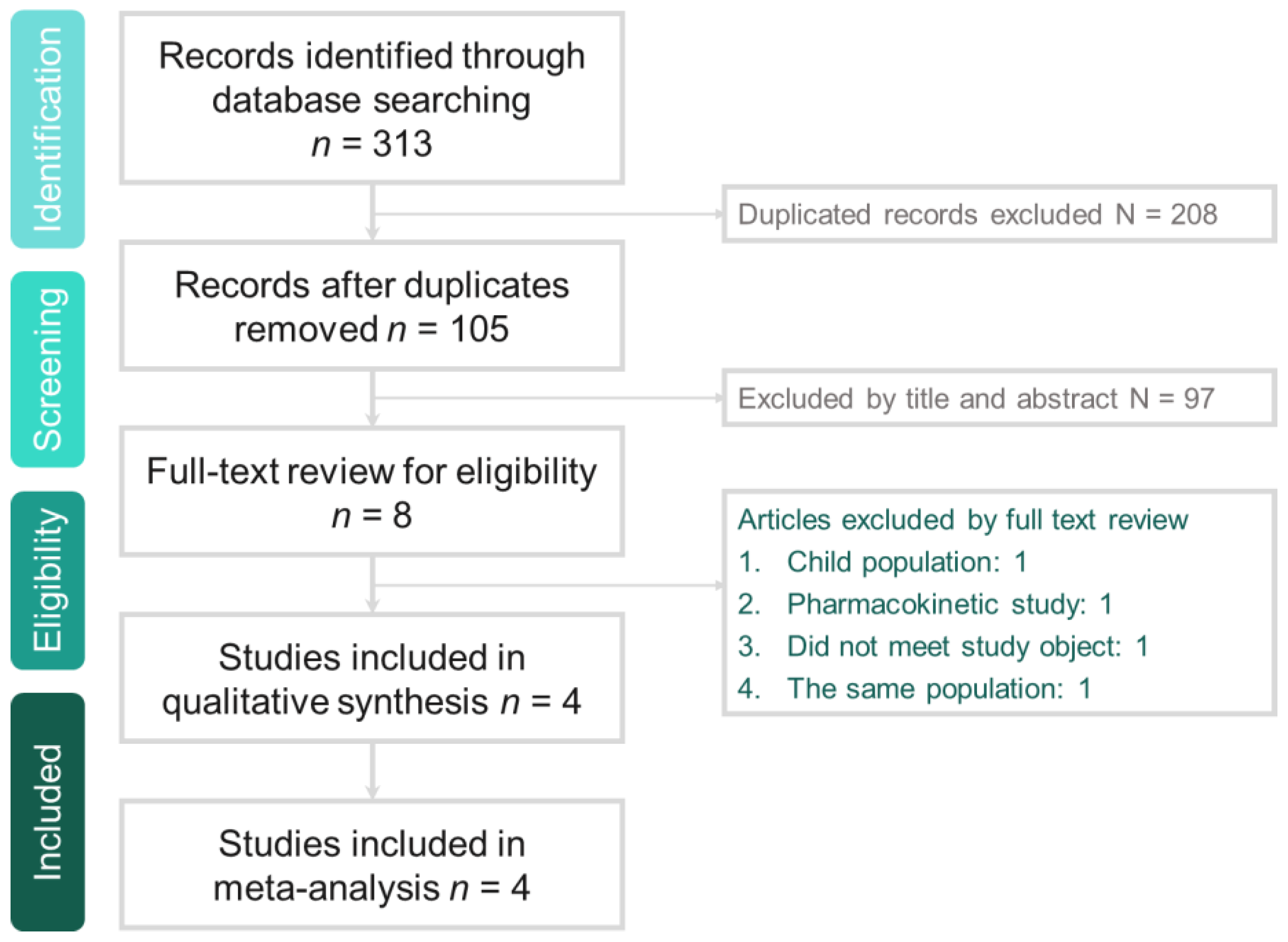
2.1. Study Search and Selection
2.2. Definition and Outcome
2.3. Statistical Analysis
3. Results
3.1. Study Selection and Characteristics
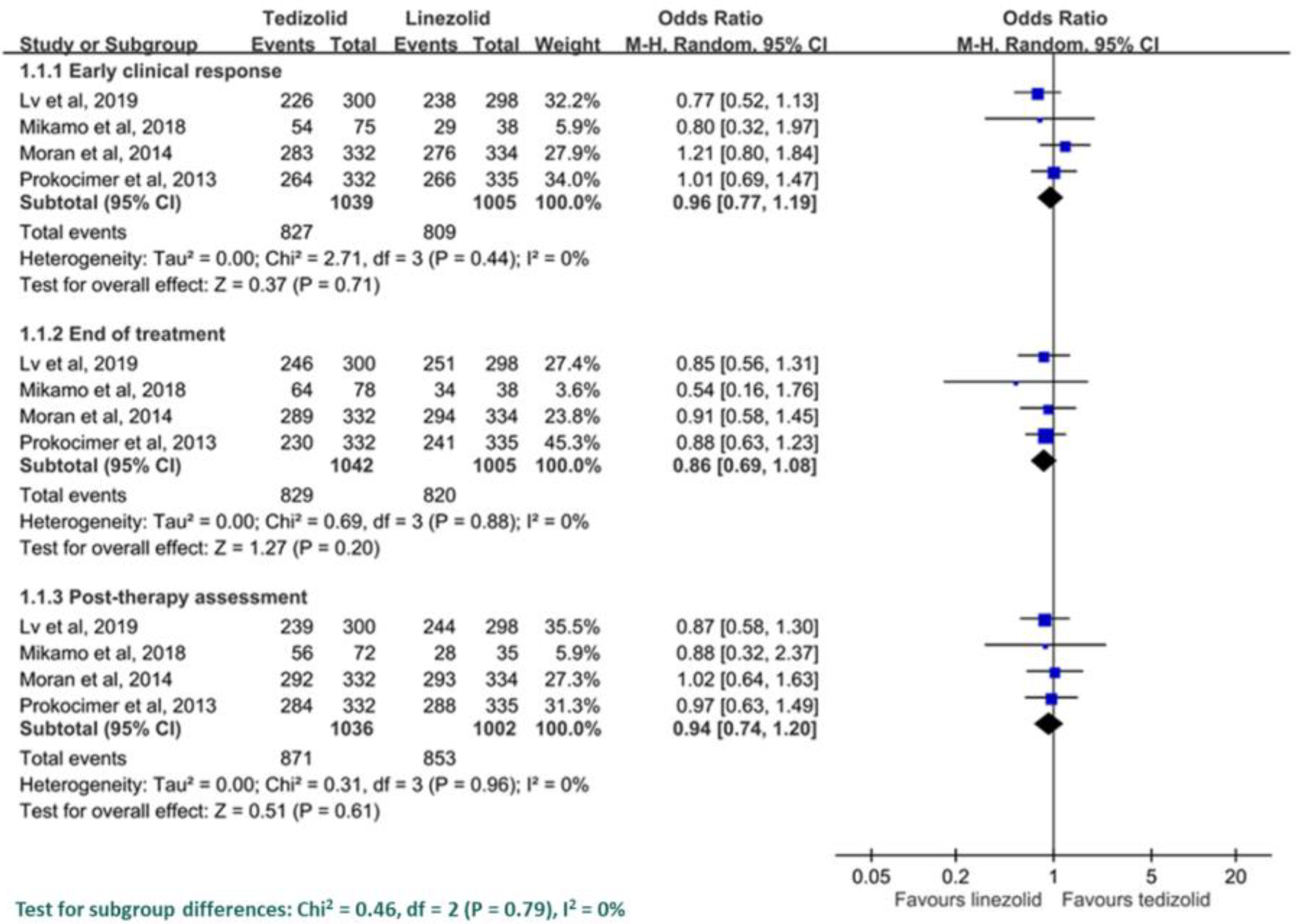
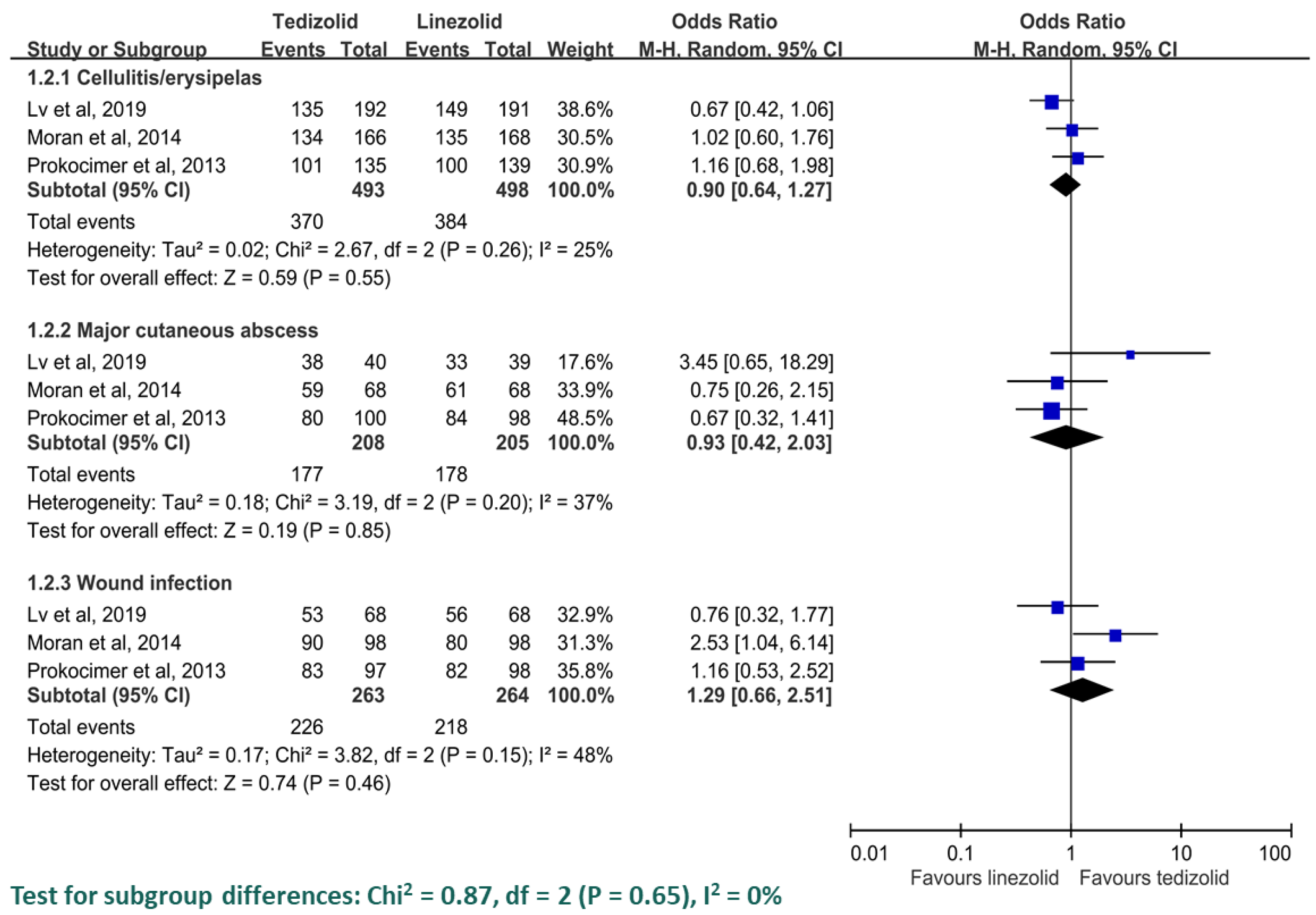
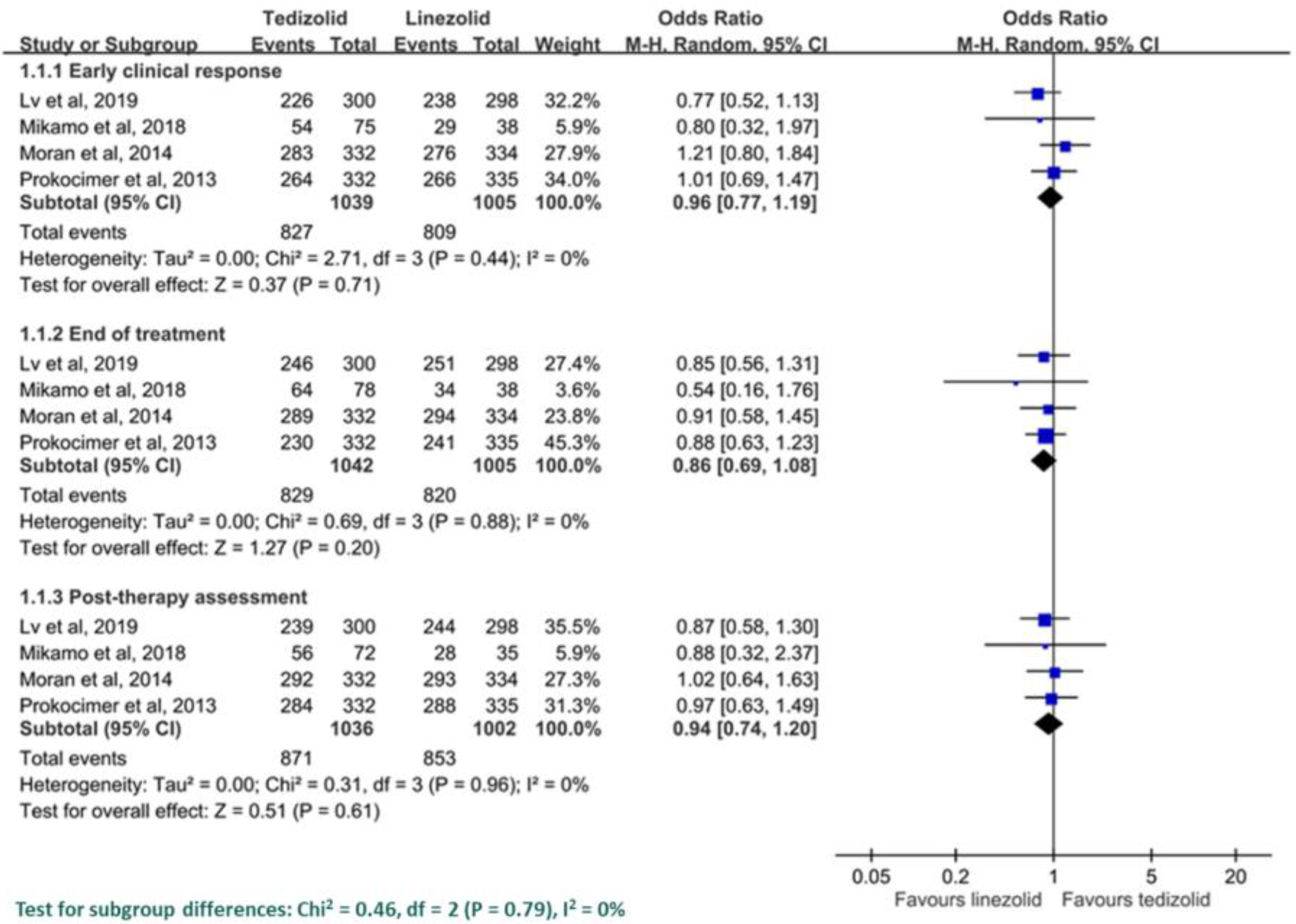
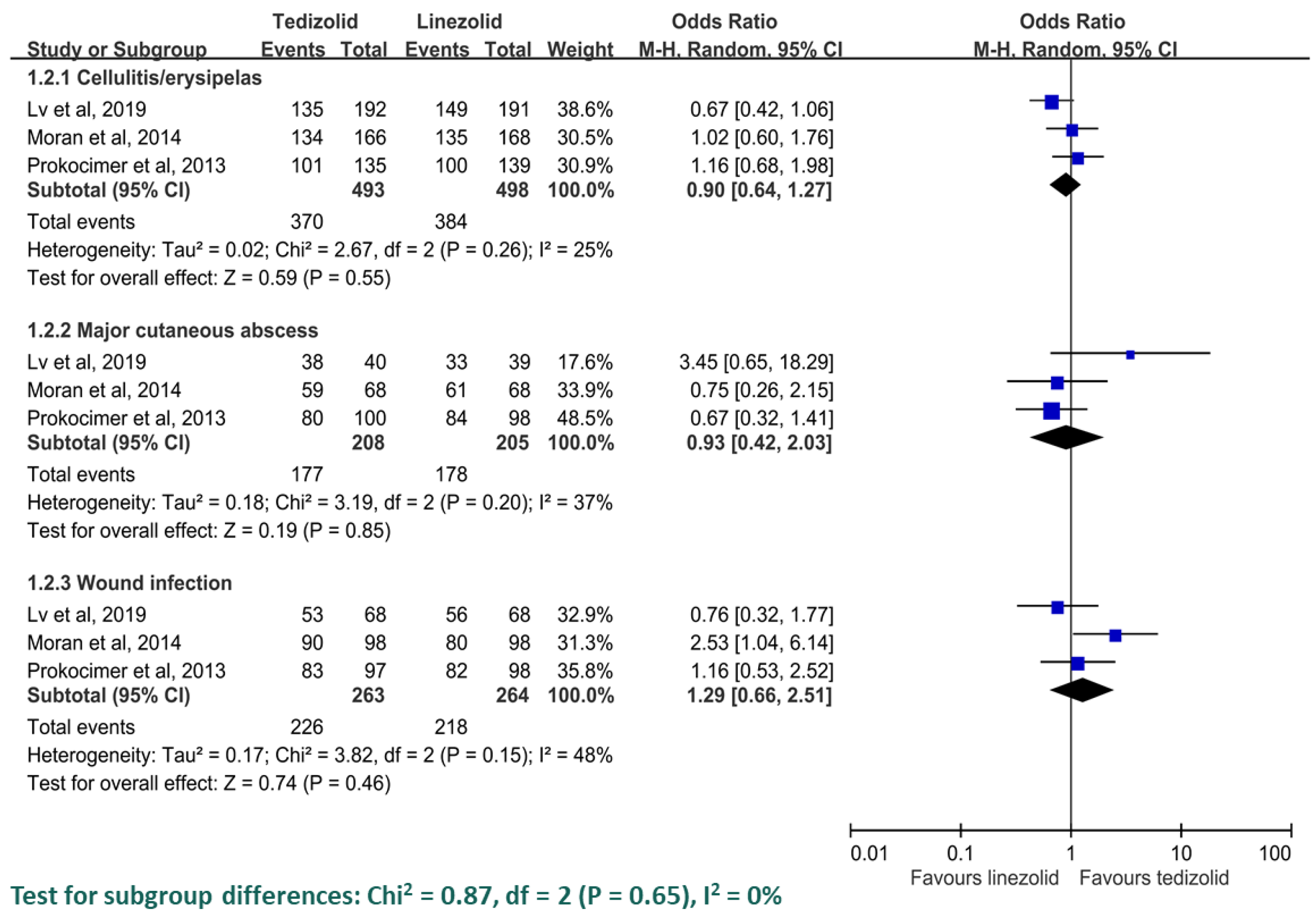
3.2. Clinical Efficacy
3.3. Minimum Inhibitory Concentration (MIC) and Microbiological Response among the MRSA Population
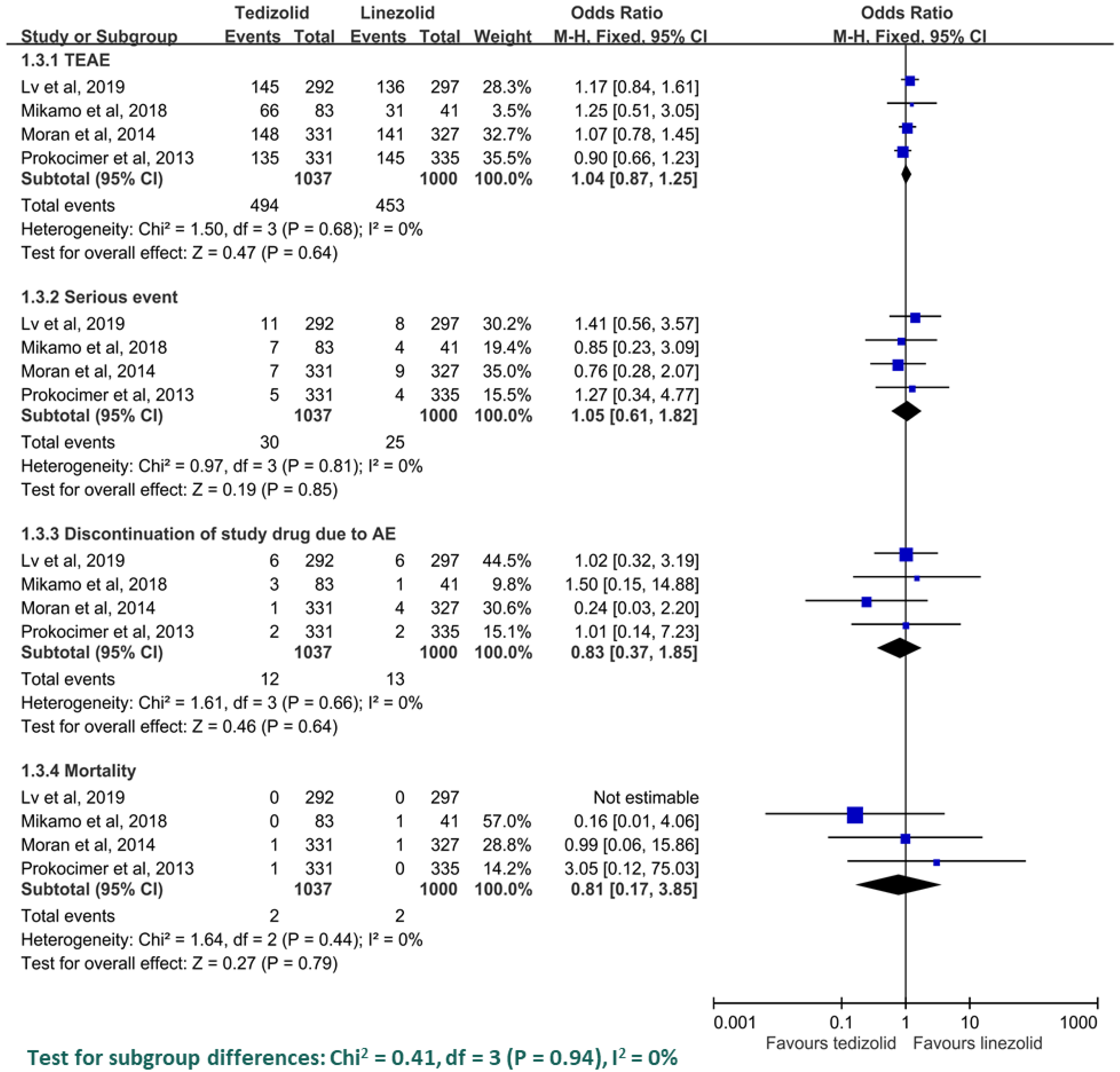
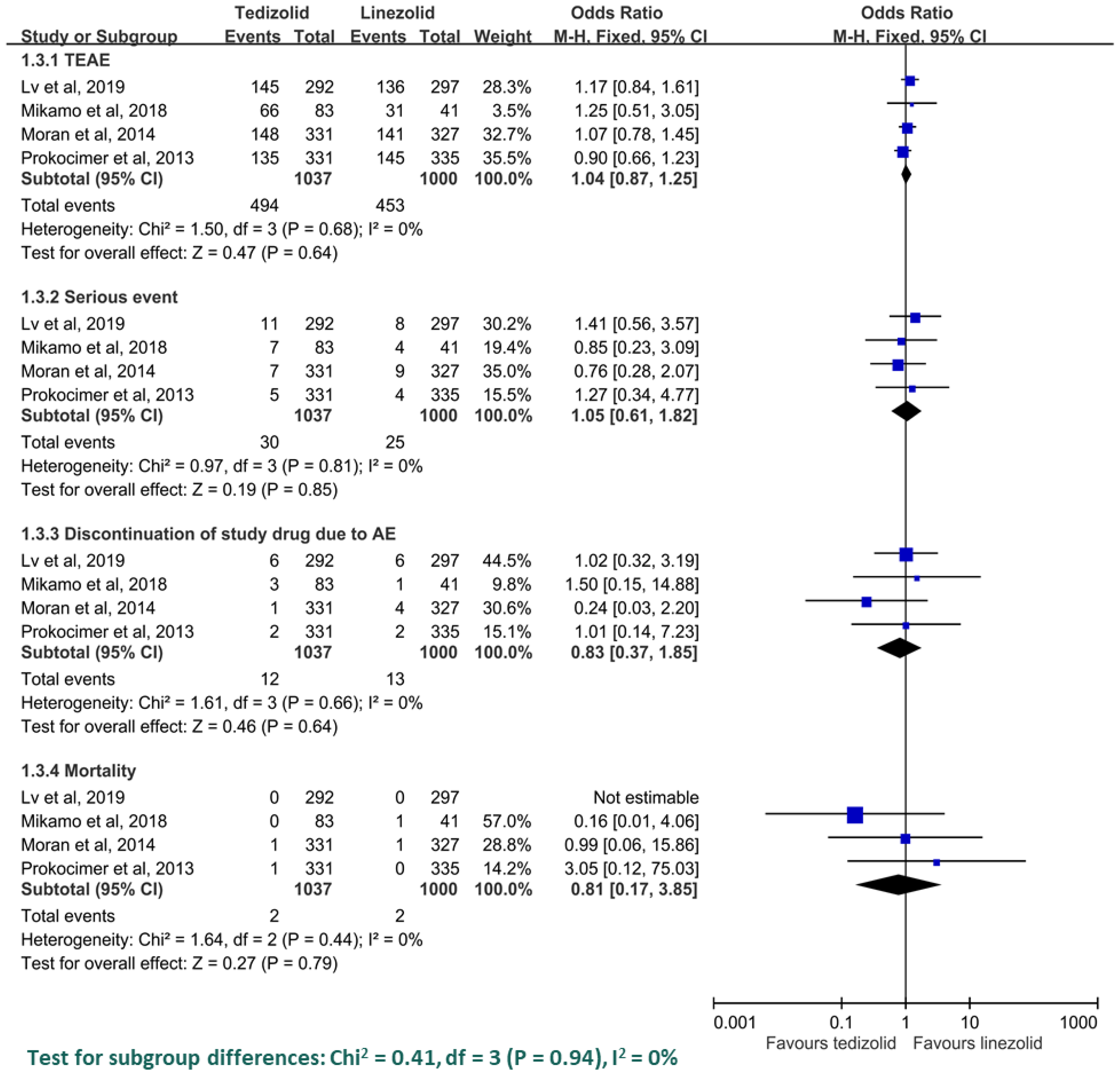
3.4. Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A. Search Strategy
| PubMed search strategy—last searched on 18 July 2019 | Results | |
| 1 | Search Search ((Sivextro[Title/Abstract]) OR Tedizolid[Title/Abstract]) OR Torezolid[Title/Abstract] | 269 |
| 2 | Search ((Acute Bacterial Skin[Title/Abstract] AND Skin Structure Infection[Title/Abstract])) OR ABSSSI[Title/Abstract] | 178 |
| 3 | 1 AND 2 | |
| 4 | Search ((((“acute bacterial skin[Title/Abstract] AND skin structure infections”[Title/Abstract])) OR ABSSSI[Title/Abstract])) AND (((Sivextro[Title/Abstract]) OR Tedizolid[Title/Abstract]) OR Torezolid[Title/Abstract]) | 34 |
| Web of Science search strategy—last searched on 18 July 2019 | Results | |
| 1 | Topic: (Sivextro) OR Topic: (Torezolid) OR Topic: (Tedizolid) | 277 |
| 2 | Topic: (“acute bacterial skin and skin structure infections”) OR Topic: (ABSSSI) | 321 |
| 3 | 1 AND 2 | |
| 4 | #1 AND #2 | 60 |
| EBSCO search strategy—last searched on 18 July 2019 | Results | |
| 1 | AB Sivextro OR AB Torezolid OR AB Tedizolid | 95 |
| 2 | AB (acute bacterial skin and skin structure infections) OR AB ABSSSI | 136 |
| 3 | 1 AND 2 | |
| 4 | S1 AND S2 | 24 |
| Cochrane Library search strategy—last searched on 18 July 2019 | Results | |
| 1 | (Sivextro): ti,ab,kw OR (Torezolid):ti,ab,kw OR (Tedizolid): ti,ab,kw | 59 |
| 2 | (acute bacterial skin and skin structure infections): ti,ab,kw OR (ABSSSI): ti,ab,kw | 160 |
| 3 | 1 AND 2 | |
| 4 | #1 AND #2 | 27 |
| Ovid Medline search strategy—last searched on 18 July 2019 | Results | |
| 1 | (Sivextro or Torezolid or Tedizolid).ab | 324 |
| 2 | ((Acute bacterial skin and skin structure infections) or ABSSSI).ab. | 433 |
| 3 | 1 AND 2 | |
| 4 | 1 and 2 | 74 |
| Embase search strategy—last searched on 18 July 2019 | Results | |
| 1 | Sivextro: ti,ab,kw OR torezolid: ti,ab,kw OR tedizolid: ti,ab,kw | 362 |
| 2 | ‘acute bacterial skin’: ti,ab,kw AND ‘skin structure infections’: ti,ab,kw OR absssi: ti,ab,kw | 534 |
| 3 | 1 AND 2 | |
| 4 | #1 AND #2 | 93 |
References
- Garau, J.; Ostermann, H.; Medina, J.; Avila, M.; McBride, K.; Blasi, F. Current management of patients hospitalized with complicated skin and soft tissue infections across Europe (2010–2011): Assessment of clinical practice patterns and real-life effectiveness of antibiotics from the REACH study. Clin. Microbiol. Infect. 2013, 19, E377–E385. [Google Scholar] [CrossRef] [PubMed]
- Falcone, M.; Concia, E.; Giusti, M.; Mazzone, A.; Santini, C.; Stefani, S.; Violi, F. Acute bacterial skin and skin structure infections in internal medicine wards: Old and new drugs. Intern. Emerg. Med. 2016, 11, 637–648. [Google Scholar] [CrossRef] [PubMed]
- Ray, G.T.; Suaya, J.A.; Baxter, R. Incidence, microbiology, and patient characteristics of skin and soft-tissue infections in a U.S. population: A retrospective population-based study. BMC Infect. Dis. 2013, 13, 252. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Carnelutti, A.; Righi, E. The role of methicillin-resistant Staphylococcus aureus in skin and soft tissue infections. Curr. Opin. Infect. Dis. 2017, 30, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Baguneid, M.; Bouza, E.; Dryden, M.; Nathwani, D.; Wilcox, M. European perspective and update on the management of complicated skin and soft tissue infections due to methicillin-resistant Staphylococcus aureus after more than 10 years of experience with linezolid. Clin. Microbiol. Infect. 2014, 20 (Suppl. 4), 3–18. [Google Scholar] [CrossRef] [PubMed]
- Stevens, D.L.; Bisno, A.L.; Chambers, H.F.; Dellinger, E.P.; Goldstein, E.J.; Gorbach, S.L.; Hirschmann, J.V.; Kaplan, S.L.; Montoya, J.G.; Wade, J.C. Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2014, 59, e10–e52. [Google Scholar] [CrossRef] [PubMed]
- Lan, S.H.; Chang, S.P.; Lai, C.C.; Lu, L.C.; Chao, C.M. Ceftaroline efficacy and safety in treatment of complicated skin and soft tissue infection: A systemic review and meta-analysis of randomized controlled trials. J. Clin. Med. 2019, 8, 776. [Google Scholar] [CrossRef] [PubMed]
- Righi, E.; Carnelutti, A.; Bassetti, M. Current role of oxazolidinones and lipoglycopeptides in skin and soft tissue infections. Curr. Opin. Infect. Dis. 2019, 32, 123–129. [Google Scholar] [CrossRef]
- Lv, X.; Alder, J.; Li, L.; O’Riordan, W.; Rybak, M.J.; Ye, H.; Zhang, R.; Zhang, Z.; Zhu, X.; Wilcox, M.H. Efficacy and safety of tedizolid phosphate versus linezolid in a randomized phase 3 trial in patients with acute bacterial skin and skin structure infection. Antimicrob. Agents Chemother. 2019, 63, e02252-18. [Google Scholar] [CrossRef]
- Mikamo, H.; Takesue, Y.; Iwamoto, Y.; Tanigawa, T.; Kato, M.; Tanimura, Y.; Kohno, S. Efficacy, safety and pharmacokinetics of tedizolid versus linezolid in patients with skin and soft tissue infections in Japan—Results of a randomised, multicentre phase 3 study. J. Infect. Chemother. 2018, 24, 434–442. [Google Scholar] [CrossRef]
- Moran, G.J.; Fang, E.; Corey, G.R.; Das, A.F.; De Anda, C.; Prokocimer, P. Tedizolid for 6 days versus linezolid for 10 days for acute bacterial skin and skin-structure infections (ESTABLISH-2): A randomised, double-blind, phase 3, non-inferiority trial. Lancet Infect. Dis. 2014, 14, 696–705. [Google Scholar] [CrossRef]
- Prokocimer, P.; Bien, P.; Surber, J.; Mehra, P.; DeAnda, C.; Bulitta, J.B.; Corey, G.R. Phase 2, randomized, double-blind, dose-ranging study evaluating the safety, tolerability, population pharmacokinetics, and efficacy of oral torezolid phosphate in patients with complicated skin and skin structure infections. Antimicrob. Agents Chemother. 2011, 55, 583–592. [Google Scholar] [CrossRef] [PubMed]
- Prokocimer, P.; De Anda, C.; Fang, E.; Mehra, P.; Das, A. Tedizolid phosphate vs linezolid for treatment of acute bacterial skin and skin structure infections: The ESTABLISH-1 randomized trial. JAMA 2013, 309, 559–569. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Shorr, A.F.; Lodise, T.P.; Corey, G.R.; De Anda, C.; Fang, E.; Das, A.F.; Prokocimer, P. Analysis of the phase 3 ESTABLISH trials of tedizolid versus linezolid in acute bacterial skin and skin structure infections. Antimicrob. Agents Chemother. 2015, 59, 864–871. [Google Scholar] [CrossRef] [PubMed]
- Sandison, T.; De Anda, C.; Fang, E.; Das, A.F.; Prokocimer, P. Clinical Response of Tedizolid versus linezolid in acute bacterial skin and skin structure infections by severity measure using a pooled analysis from two phase 3 double-blind trials. Antimicrob. Agents Chemother. 2017, 61, e02687-16. [Google Scholar] [CrossRef] [PubMed]
- Joseph, W.S.; Culshaw, D.; Anuskiewicz, S.; De Anda, C.; Prokocimer, P. Tedizolid and linezolid for treatment of acute bacterial skin and skin structure infections of the lower extremity versus non-lower-extremity infections: Pooled analysis of two phase 3 trials. J. Am. Podiatr. Med. Assoc. 2017, 107, 264–271. [Google Scholar] [CrossRef] [PubMed]
- Hasannejad-Bibalan, M.; Mojtahedi, A.; Biglari, H.; Halaji, M.; Sedigh Ebrahim-Saraie, H. Antibacterial activity of tedizolid, a novel oxazolidinone against methicillin-resistant Staphylococcus aureus: A systematic review and meta-analysis. Microb. Drug Resist. 2019. [Google Scholar] [CrossRef] [PubMed]
- Pfaller, M.A.; Sader, H.S.; Rhomberg, P.R.; Flamm, R.K.; Mendes, R.E. In vitro activity of tedizolid in comparison with other oral and intravenous agents against a collection of community-acquired methicillin-resistant Staphylococcus aureus (2014–2015) in the United States. Microb. Drug Resist. 2019, 25, 938–943. [Google Scholar] [CrossRef] [PubMed]
- Vanegas Munera, J.M.; Ocampo Rios, A.M.; Urrego, D.M.; Jimenez Quiceno, J.N. In vitro susceptibility of methicillin-resistant Staphylococcus aureus isolates from skin and soft tissue infections to vancomycin, daptomycin, linezolid and tedizolid. Braz. J. Infect. Dis. 2017, 21, 493–499. [Google Scholar] [CrossRef] [PubMed]
- Penuelas, M.; Candel, F.J.; Lejarraga, C.; Lopez-Gonzalez, L.; Vinuela-Prieto, J.M.; Lopez de Mendoza, D. Activity of linezolid and tedizolid against clinical isolates of methicillin-resistant and methicillin and linezolid resistant Staphylococcus aureus: An in vitro comparison. Rev. Esp. Quimioter. 2016, 29, 255–258. [Google Scholar] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| The Study, Published Year | Study Design | Study Period | Number of Patients | Dose Regimen | ||
|---|---|---|---|---|---|---|
| Tedizolid | Linezolid | Tedizolid | Linezolid | |||
| Prokocimer et al., 2013 [13] | Randomized, double-blind, multicenter, multinational, non-inferiority trial | 2010–2011 | 332 | 335 | oral 200 mg daily × 6 days | oral 600 mg twice daily × 10 days |
| Moran et al., 2014 [11] | Randomized, double-blind, multinational, non-inferiority trial | 2011–2013 | 332 | 334 | intravenous 200 mg daily × 6 days with optional step-down | intravenous 600 mg twice daily × 10 days with optional step down |
| Mikamo et al., 2018 [10] | Prospective, randomized, open-label, multicenter trial | 2013–2016 | 84 | 41 | intravenous /oral 200 mg daily × 6 days | intravenous /oral 600 mg twice daily × 10 days |
| Lv et al., 2019 [9] | Randomized, double-blind, multicenter, non-inferiority trial | 2014–2016 | 300 | 298 | intravenous /oral 200 mg daily × 6 days | intravenous /oral 600 mg twice daily × 10 days |
| Study, Year | Age | Male Sex, Number (%) | Bacteremia, Number (%) | Number with MRSA at Baseline | ||||
|---|---|---|---|---|---|---|---|---|
| Tedizolid | Linezolid | Tedizolid | Linezolid | Tedizolid | Linezolid | Tedizolid | Linezolid | |
| Prokocimer et al., 2013 [13] | 43.6 (14.96) | 43.1 (15.06) | 204 (61.4) | 198 (59.1) | NA | NA | 88 | 90 |
| Moran et al., 2014 [11] | 46 (17–86) | 46 (15–89) | 225 (68) | 214 (64) | 7 (2) | 12 (4) | 53 | 56 |
| Mikamo et al., 2018 [10] | 63.4 (16.5) | 63.3 (16.2) | 55 (65.5) | 28 (68.3) | 4 (4.8) | 2 (4.9) | 32 | 13 |
| Lv et al., 2019 [9] | 45.7 (18–85) | 47.5 (18–85) | 209 (69.7) | 192 (64.4) | 5 (1.7) | 3 (1.0) | 29 | 32 |
| Study | Cellulitis/Erysipelas, Number (%) | Major Cutaneous Abscess, Number (%) | Wound, Number (%) | |||
|---|---|---|---|---|---|---|
| Tedizolid | Linezolid | Tedizolid | Linezolid | Tedizolid | Linezolid | |
| Prokocimer et al., 2013 [13] | 135 (40.4) | 139 (41.5) | 100 (30.1) | 98 (29.3) | 97 (29.2) | 98 (29.3) |
| Moran et al., 2014 [11] | 166 (50) | 168 (50) | 68 (20) | 68 (20) | 98 (30) | 98 (29) |
| Mikamo et al., 2018 [10] | 44 (52.4) | 22 (53.7) | 3 (3.6) | 2 (4.9) | 16 (19.0) | 10 (24.4) |
| Lv et al., 2019 [9] | 192 (64.0) | 191 (64.1) | 40 (13.3) | 39 (13.1) | 68 (22.7) | 68 (22.8) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lan, S.-H.; Lin, W.-T.; Chang, S.-P.; Lu, L.-C.; Chao, C.-M.; Lai, C.-C.; Wang, J.-H. Tedizolid Versus Linezolid for the Treatment of Acute Bacterial Skin and Skin Structure Infection: A Systematic Review and Meta-Analysis. Antibiotics 2019, 8, 137. https://doi.org/10.3390/antibiotics8030137
Lan S-H, Lin W-T, Chang S-P, Lu L-C, Chao C-M, Lai C-C, Wang J-H. Tedizolid Versus Linezolid for the Treatment of Acute Bacterial Skin and Skin Structure Infection: A Systematic Review and Meta-Analysis. Antibiotics. 2019; 8(3):137. https://doi.org/10.3390/antibiotics8030137
Chicago/Turabian StyleLan, Shao-Huan, Wei-Ting Lin, Shen-Peng Chang, Li-Chin Lu, Chien-Ming Chao, Chih-Cheng Lai, and Jui-Hsiang Wang. 2019. "Tedizolid Versus Linezolid for the Treatment of Acute Bacterial Skin and Skin Structure Infection: A Systematic Review and Meta-Analysis" Antibiotics 8, no. 3: 137. https://doi.org/10.3390/antibiotics8030137
APA StyleLan, S.-H., Lin, W.-T., Chang, S.-P., Lu, L.-C., Chao, C.-M., Lai, C.-C., & Wang, J.-H. (2019). Tedizolid Versus Linezolid for the Treatment of Acute Bacterial Skin and Skin Structure Infection: A Systematic Review and Meta-Analysis. Antibiotics, 8(3), 137. https://doi.org/10.3390/antibiotics8030137