Interventions to Reduce Antibiotic Prescribing in LMICs: A Scoping Review of Evidence from Human and Animal Health Systems

Abstract
1. Introduction
- -
- What supply-side interventions have been tried in LMICs to reduce inappropriate antibiotic prescribing and sale?
- -
- Where have interventions been implemented e.g., country and kind of health care settings?
- -
- Which kinds of interventions have shown promise in reducing inappropriate prescribing?
- -
- What information exists on the contexts of interventions and attempts to influence antibiotic use and prescribing?
2. Methods
2.1. Search Strategy
2.2. Study Selection
- Reports on an intervention aiming to influence the prescribing and sale of antibiotics (formal and informal), including the use of antibiotics to treat existing and suspected infections or to prevent infection (e.g., antibiotic prophylaxis)
- Any healthcare setting in a LMIC country
- Outcomes:
- Externally measured change in antibiotic use/sale/prescribing
- Externally measured change in knowledge and attitudes around antibiotic use
- Self-reported change in antibiotic use/sale/prescribing
- Self-reported change in knowledge and attitudes around antibiotic use
- Observed change in the quality of antibiotics prescribed/sold
Or for “context studies”- Studies that describe the contextual factors that influenced the effectiveness of interventions
- -
- Studies of other ways of addressing antibiotic resistance, e.g., hygiene and infection and prevention control such as vaccines, etc.
- -
- Studies assessing adherence to antibiotics or medicine
- -
- Studies of environmental transmission of antibiotics and antibiotic resistance
- -
- Studies targeting other antimicrobials, and not targeting antibiotic use
- -
- Studies reporting on/intervening in patient demand for antibiotics and self-use
- -
- Studies evaluating effectiveness of antibiotic treatment in clinical care, e.g., comparing different treatments or ways of administering antibiotics, and reporting on clinical outcomes.
- -
- For “context studies”, those studies that only described the context and not the implementation or outcome of an intervention, e.g., a situation analysis
3. Results
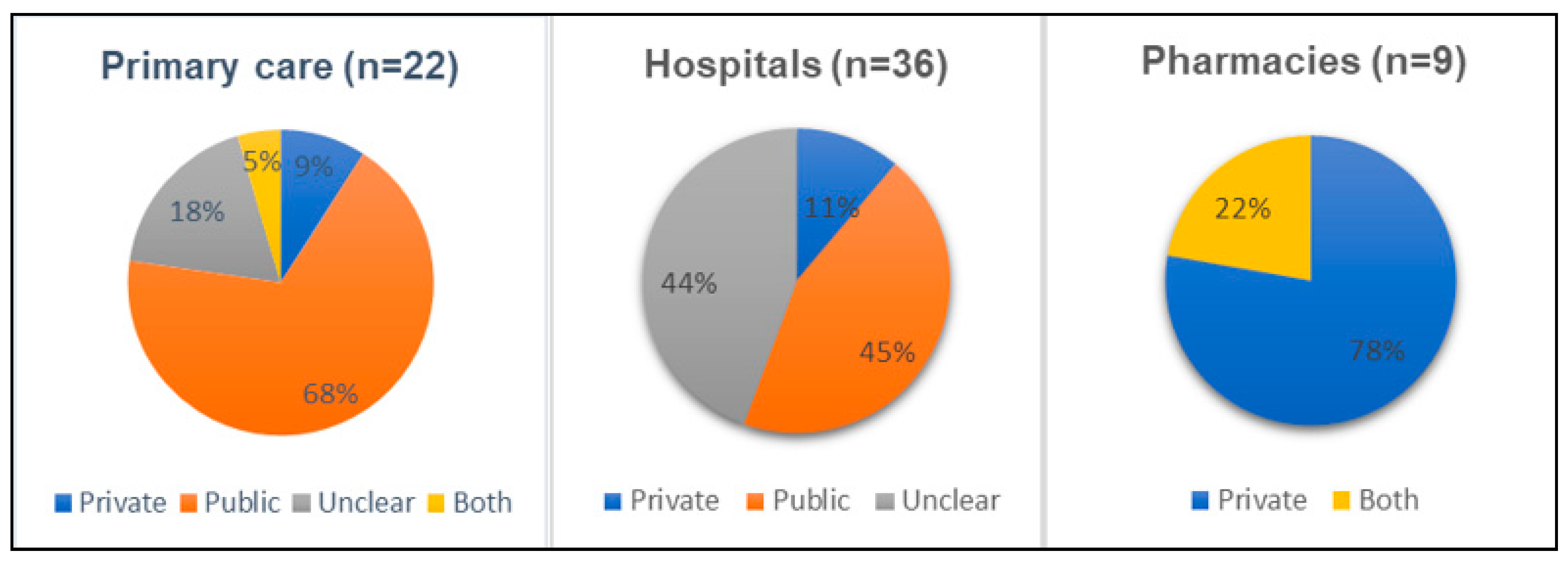
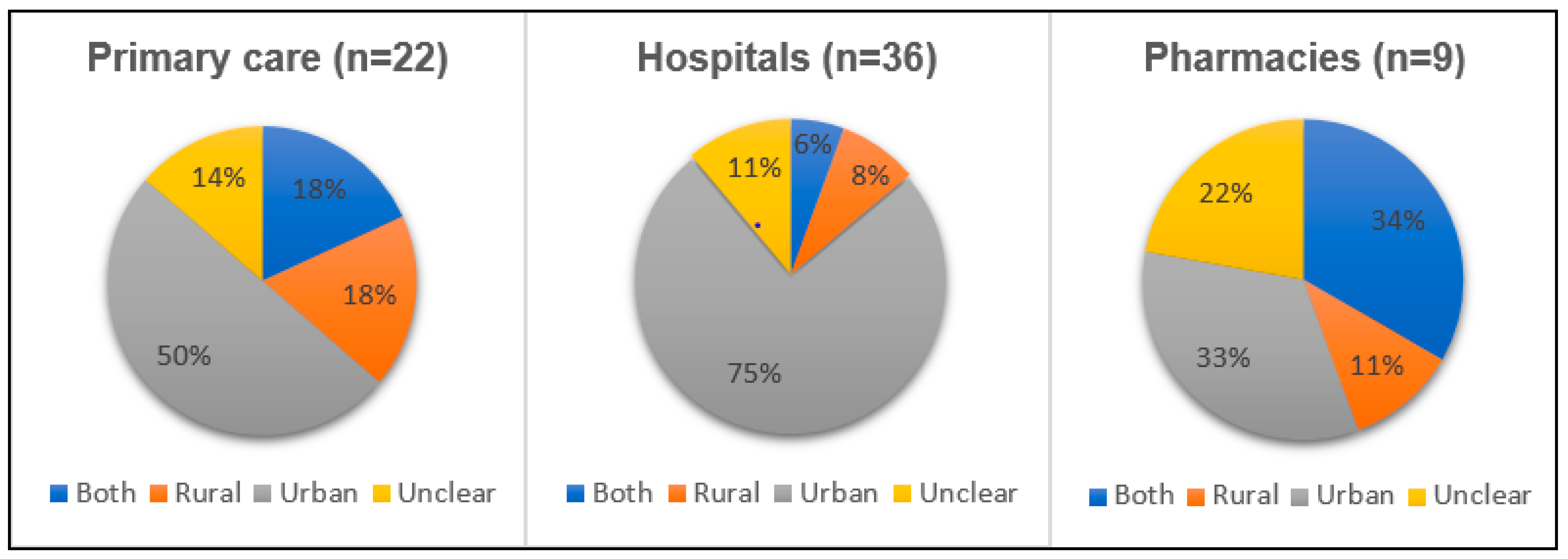
3.1. Intervention Settings
3.2. Types of Intervention
3.3. Intervention Impact
3.4. Prescribing and Intervention Contexts
3.4.1. Knowledge of Antimicrobial Resistance and Appropriate Antibiotic Use
3.4.2. Practical Concerns and Diverse Influences on Antibiotic Prescribing
3.4.3. Industry Influence
3.4.4. Care and Responsibility
3.4.5. Perceptions of Public Perception
3.4.6. Perspectives on Interventions
3.4.7. Policy Coordination
3.4.8. Unintended Consequences
3.4.9. Animal Health
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Parameter | Definition |
|---|---|
| Population | People who supply antibiotics to sick people or animals, e.g., doctors and other healthcare prescribers, drug sellers, informal doctors, pharmacists, community health workers, veterinarians, farmers, community animal health workers |
| Problem | Unnecessary or inappropriate use of antibiotics |
| Intervention | Any intervention aiming to influence the prescribing or sale of antibiotics (formal and informal), e.g., communication and education, stewardship programmes, treatment algorithms, delayed treatment, alternative treatments, incentives, pricing, packaging, legislation, peer or community oversight. |
| Comparison | Not applicable. The review is not limited to controlled or comparative research designs. Studies which report on interventions with or without comparison groups are included |
| Context | Hospital, outpatients, community, online, formal and informal systems in LMICs only. |
| Outcome | Primary: Measured improvement in antibiotic use (e.g., reduction in unnecessary antibiotic prescribing, improved adherence to guidelines) Other outcomes could include: Reported changes in knowledge and attitudes around antibiotic use, e.g. health outcomes (improved, unaffected, or adverse), levels of antibiotic resistance and unintended consequences |
Appendix B
- (1)
- Activity/Outcome of interest:
- -
- antibiotic AND (prescribing OR sale OR prescribing OR prescription OR selling OR availability OR consumption or dosage OR use)
- (2)
- Type of intervention:
- -
- “Behaviour change”
- -
- stewardship
- -
- drug policy
- -
- drug financing
- -
- drug committee
- -
- Marketing / social marketing
- -
- Communication
- -
- Outreach
- -
- “community engagement”
- -
- Evaluation
- -
- Training
- -
- Guideline$
- -
- Algorithm
- -
- curriculum
- -
- “mass media”
- -
- Information
- -
- Television
- -
- Radio
- -
- Newspapers
- -
- Booklets
- -
- Pamphlet
- -
- Posters
- -
- Leaflets
- -
- Advocacy
- -
- Advice
- -
- Fines
- -
- Incentive$
- -
- “financial incentive$”
- -
- “financial intervention$”
- -
- Fees
- -
- formularies
- -
- Tax
- -
- Taxation
- -
- Prohibit
- -
- Prohibition
- -
- Ban
- -
- Regulation
- -
- Legislation
- -
- Reform
- -
- Restrict
- -
- Restriction
- -
- Reminder$
- -
- “Peer supervision”
- -
- Subsidy
- -
- Subsidi$ation
- -
- Peer support
- -
- Reward$
- -
- Targets$
- -
- Feedback
- -
- Planning
- -
- Oversight
- -
- “Goal setting”
- -
- Audit$
- -
- Monitoring
- -
- Intervention OR Impact OR Pilot OR evaluation
Appendix C
Appendix D
References
- Klein, E.Y.; van Boeckel, T.P.; Martinez, E.M.; Pant, S.; Gandra, S.; Levin, S.A.; Goossens, H.; Laxminarayan, R. Global increase and geographic convergence in antibiotic consumption between 2000 and 2015. Proc. Natl. Acad. Sci. USA 2018, 115, E3463–E3470. [Google Scholar] [CrossRef] [PubMed]
- Buckland-Merrett, G.; Bloom, G.; Wilkinson, A.; MacGregor, H.M. Towards the just and sustainable use of antibiotics. J. Pharm. Policy Pract. 2016, 9, 31. [Google Scholar] [CrossRef] [PubMed]
- Malhotra-Kumar, S.; Lammens, C.; Coenen, S.; Van Herck, K.; Goossens, H. Effect of azithromycin and clarithromycin therapy on pharyngeal carriage of macrolide resistant streptococci in healthy volunteers: A randomised, double-blind, placebo controlled study. Lancet 2007, 369, 482–490. [Google Scholar] [CrossRef]
- Davey, P.; Marwick, C.A.; Scott, C.L.; Charani, E.; Mcneil, K.; Brown, E.; Gould, I.M.; Ramsay, C.R.; Michie, S. Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane Database Syst. Rev. 2017, 2, CD003543. [Google Scholar] [CrossRef] [PubMed]
- Arnold, S.R.; Straus, S.E. Interventions to improve antibiotic prescribing practices in ambulatory care. Cochrane Database Syst. Rev. 2005, 4. [Google Scholar] [CrossRef] [PubMed]
- Ivanovska, V.; Holloway, K.A. Interventions to improve antibiotic prescribing in upper middle income countries: A systematic review of the literature 1990–2009. Maced. J. Med. Sci. 2013, 6, 84–91. [Google Scholar]
- Bloom, G.; Wilkinson, A.; Tomson, G.; Awor, P.; Zhang, X.; Masud Ahmed, S.; Wasif Ali Khan, B. Addressing Resistance to Antibiotics in Pluralistic Health Systems; STEPS Working Paper; STEPS Centre: Brighton, UK, 2015. [Google Scholar]
- Chandler, C.; Webb, E.; Maiteki-Sebuguzi, C.L.; Nayiga, S.; Nabirye, C.; Liberto, D.; Ssemmondo, E.; Dorsey, G.; Kamya, M.; Staedke, S. The impact of an intervention to introduce malaria rapid diagnostic tests on fever case management in a high transmission setting in Uganda: A mixed-methods cluster-randomized trial (PRIME). PLoS ONE 2017, 12, e0170998. [Google Scholar] [CrossRef] [PubMed]
- Hutchinson, E.; Hutchison, C.; Lal, S.; Hansen, K.; Kayendeke, M.; Nabirye, C.; Magnussen, P.; Clarke, S.E.; Mbonye, A.; Chandler, C.I.R. Introducing rapid tests for malaria into the retail sector: What are the unintended consequences? BMJ Glob. Health 2017, 2, e000067. [Google Scholar] [CrossRef]
- Colquhoun, H.L.; Levac, D.; O’Brien, K.K.; Straus, S.; Tricco, A.C.; Perrier, L.; Kastner, M.; Moher, D. Scoping reviews: Time for clarity in definition, methods, and reporting. J. Clin. Epidemiol. 2014, 67, 1291–1294. [Google Scholar] [CrossRef]
- Miake-Lye, I.M.; Hempel, S.; Shanman, R.; Shekelle, P.G. What is an evidence map? A systematic review of published evidence maps and their definitions, methods, and products. Syst. Rev. 2016, 5, 28. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Howard, P.; Pulcini, C.; Levy, H.G.; West, R.M.; Gould, I.M.; Harbarth, S.; Nathwani, D. ESCMID Study Group for Antimicrobial Policies (ESGAP); ISC Group on Antimicrobial Stewardship. An international cross-sectional survey of antimicrobial stewardship programmes in hospitals. J. Antimicrob. Chemother. 2015, 70, 1245–1255. [Google Scholar] [CrossRef] [PubMed]
- Al-Azzam, S.I.; Alzoubi, K.H.; Mhaidat, N.M.; Haddadin, R.D.; Masadeh, M.M.; Tumah, H.N.; Magableh, A.; Maraqa, N.K. Preoperative antibiotic prophylaxis practice and guideline adherence in Jordan: A multi-centre study in Jordanian hospitals. J. Infect. Dev. Ctries. 2012, 6, 715–720. [Google Scholar] [CrossRef] [PubMed]
- Bai, Y.; Wang, S.; Yin, X.; Bai, J.; Gong, Y.; Lu, Z. Factors associated with doctors’ knowledge on antibiotic use in China. Sci. Rep. 2016, 6, 23429. [Google Scholar] [CrossRef] [PubMed]
- Quet, F.; Vlieghe, E.; Leyer, C.; Buisson, Y.; Newton, P.N.; Naphayvong, P.; Keoluangkhot, V.; Chomarat, M.; Longuet, C.; Steenkeste, N.; et al. Antibiotic prescription behaviours in Lao People’s Democratic Republic: A knowledge, attitude and practice survey. Bull. World Health Organ. 2015, 93, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Chandy, S.J.; Mathai, E.; Thomas, K.; Faruqui, A.R.; Holloway, K.; Lundborg, C.S. Antibiotic use and resistance: Perceptions and ethical challenges among doctors, pharmacists and the public in Vellore, South India. Indian J. Med. Ethics 2013, 10, 20–27. [Google Scholar] [CrossRef]
- Nga, D.T.T.; Chuc, N.T.K.; Hoa, N.P.; Hoa, N.Q.; Nguyen, N.T.T.; Loan, H.T.; Toan, T.K.; Phuc, H.D.; Horby, P.; Van Yen, N.; et al. Antibiotic sales in rural and urban pharmacies in northern Vietnam: An observational study. BMC Pharmacol. Toxicol. 2014, 15, 6. [Google Scholar] [CrossRef]
- Reynolds, L.; Mckee, M. Factors influencing antibiotic prescribing in China: An exploratory analysis. Health Policy 2009, 90, 32–36. [Google Scholar] [CrossRef]
- Kotwani, A.; Wattal, C.; Joshi, P.C.; Holloway, K. Irrational use of antibiotics and role of the pharmacist: An insight from a qualitative study in New Delhi, India. J. Clin. Pharm. Ther. 2012, 37, 308–312. [Google Scholar] [CrossRef]
- Salim, A.M.A.; Elgizoli, B. Exploring the reasons why pharmacists dispense antibiotics without prescriptions in Khartoum state, Sudan. Int. J. Pharm. Pract. 2017, 25, 59–65. [Google Scholar] [CrossRef]
- Dillip, A.; Embrey, M.; Shekalaghe, E.; Ross-Degnan, D.; Vialle-Valentin, C.; Kimatta, S.; Liana, J.; Rutta, E.; Valimba, R.; Chalker, J. What motivates antibiotic dispensing in accredited drug dispensing outlets in Tanzania? A qualitative study. Antimicrob. Resist. Infect. Control 2015, 4, 30. [Google Scholar] [CrossRef] [PubMed]
- Akoria, O.A.; Isah, A.O. An evaluation of doctors’ prescribing performance in Nigeria. Pak. J. Med. Sci. 2009, 25, 533–538. [Google Scholar]
- Giri, B.R.; Shankar, P.R. Learning how drug companies promote medicines in Nepal: An educational initiative looks critically at the drug industry’s promotional tactics. PLoS Med. 2005, 2, 0710–0711. [Google Scholar] [CrossRef] [PubMed]
- Riaz, H.; Godman, B.; Hussain, S.; Malik, F.; Mahmood, S.; Shami, A.; Bashir, S. Prescribing of bisphosphonates and antibiotics in Pakistan: Challenges and opportunities for the future. J. Pharm. Health Serv. Res. 2015, 6, 111–121. [Google Scholar] [CrossRef]
- Hussain, S.; Malik, F.; Hameed, A.; Parveen, G.; Raja, F.Y.; Riaz, H.; Shafaat, S.; Wajid, A.; Channa, R.A. Pharmacoepidemiological studies of prescribing practices of health care providers of Pakistan: A cross sectional survey. Afr. J. Pharm. Pharmacol. 2011, 5, 1484–1493. [Google Scholar] [CrossRef]
- Kotwani, A.; Wattal, C.; Katewa, S.; Joshi, P.C.; Holloway, K. Factors influencing primary care physicians to prescribe antibiotics in Delhi India. Fam. Pract. 2010, 27, 684–690. [Google Scholar] [CrossRef] [PubMed]
- Tillekeratne, L.G.; Bodinayake, C.K.; Dabrera, T.; Nagahawatte, A.; Arachchi, W.K.; Sooriyaarachchi, A.; Stewart, K.; Watt, M.; Østbye, T.; Woods, C.W. Antibiotic overuse for acute respiratory tract infections in Sri Lanka: A qualitative study of outpatients and their physicians. BMC Fam. Pract. 2017, 18, 37. [Google Scholar] [CrossRef]
- Zhang, Z.; Zhan, X.; Zhou, H.; Sun, F.; Zhang, H.; Zwarenstein, M.; Liu, Q.; Li, Y.; Yan, W. Antibiotic prescribing of village doctors for children under 15 years with upper respiratory tract infections in rural China: A qualitative study. Medicine 2016, 95, e3803. [Google Scholar] [CrossRef]
- Wasserman, S.; Potgieter, S.; Shoul, E.; Constant, D.; Stewart, A.; Mendelson, M.; Boyles, T.H. South African medical students’ perceptions and knowledge about antibiotic resistance and appropriate prescribing: Are we providing adequate training to future prescribers? S. Afr. Med. J. (Suid-Afrikaanse tydskrif vir geneeskunde) 2017, 107, 405–410. [Google Scholar] [CrossRef]
- Ahmed, S.M.; Islam, Q.S. Availability and rational use of drugs in primary healthcare facilities following the national drug policy of 1982: Is Bangladesh on right track? J. Health Popul. Nutr. 2012, 30, 99–108. [Google Scholar] [CrossRef]
- Kibuule, D.; Mubita, M.; Naikaku, E.; Kalemeera, F.; Godman, B.B.; Sagwa, E. An analysis of policies for cotrimoxazole, amoxicillin and azithromycin use in Namibia’s public sector: Findings and therapeutic implications. Int. J. Clin. Pract. 2017, 71, e12918. [Google Scholar] [CrossRef] [PubMed]
- Senn, N.; Rarau, P.; Salib, M.; Manong, D.; Siba, P.; Rogerson, S.; Mueller, I.; Genton, B. Use of antibiotics within the IMCI guidelines in outpatient settings in Papua New Guinean children: An observational and effectiveness study. PLoS ONE 2014, 9, e90990. [Google Scholar] [CrossRef] [PubMed]
- Biswas, R.; Dineshan, V.; Narasimhamurthy, N.S.; Kasthuri, A.S. Integrating hospital-acquired lessons into community health practice: Optimizing antimicrobial use in Bangalore. J. Contin. Educ. Health Prof. 2007, 27, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Kazaura, M.; Lugangira, K.; Kalokola, F. Prescription practices for non-malaria febrile illnesses among under-fives in the Lake Zone, Tanzania. Asian Pac. J. Trop. Dis. 2016, 6, 759–764. [Google Scholar] [CrossRef]
- Pham, D.K.; Chu, J.; Do, N.T.; Brose, F.; Degand, G.; Delahaut, P.; De Pauw, E.; Douny, C.; Nguyen, K.V.; Vu, T.D.; et al. Monitoring Antibiotic Use and Residue in Freshwater Aquaculture for Domestic Use in Vietnam. EcoHealth 2015, 12, 480–489. [Google Scholar] [CrossRef] [PubMed]
- Paredes, P.; de la Peña, M.; Flores-Guerra, E.; Diaz, J.; Trostle, J. Factors influencing physicians’ prescribing behaviour in the treatment of childhood diarrhoea: Knowledge may not be the clue. Soc. Sci. Med. 1996, 42, 1141–1153. [Google Scholar] [CrossRef]
- Himmel, W.; Lippert-Urbanke, E.; Kochen, M.M. Are patients more satisfied when they receive a prescription? The effect of patient expectations in general practice. Scand. J. Prim. Health Care 1997, 15, 118–122. [Google Scholar] [CrossRef]
- Coenen, S.; Francis, N.; Kelly, M.; Hood, K.; Nuttall, J. Are Patient Views about Antibiotics Related to Clinician Perceptions, Management and Outcome? A Multi-Country Study in Outpatients with Acute Cough. PLoS ONE 2013, 8, e76691. [Google Scholar] [CrossRef]
- Tomson, G.; Vlad, I. The need to look at antibiotic resistance from a health systems perspective. Ups J. Med. Sci. 2014, 119, 117–124. [Google Scholar] [CrossRef]
- Hargreaves, T. Practice-ing behaviour change: Applying social practice theory to pro-environmental behaviour change. J. Consum. Cult. 2011, 11, 79–99. [Google Scholar] [CrossRef]
- Caldwell, S.E.M.; Mays, N. Studying policy implementation using a macro, meso and micro frame analysis: The case of the Collaboration for Leadership in Applied Health Research & Care (CLAHRC) programme nationally and in North West London. Health Res. Policy Syst. 2012, 10, 32. [Google Scholar] [PubMed]
- Grace, D. Review of Evidence on Antimicrobial Resistance and Animal Agriculture in Developing Countries. 2015. Available online: https://www.gov.uk/dfid-research-outputs/review-of-evidence-on-antimicrobial-resistance-and-animal-agriculture-in-developing-countries-201309 (accessed on 20 December 2018).
- Cross, J.; MacGregor, H. Knowledge, Legitimacy and Economic Practice in Informal Markets for Medicine: A Critical Review of Research. Soc. Sci. Med. 2010, 71, 1593–1600. [Google Scholar] [CrossRef] [PubMed]
- Edwards, R.; Charani, E.; Sevdalis, N.; Alexandrou, B. Optimisation of infection prevention and control in acute health care by use of behaviour change: A systematic review. Lancet Infect. Dis. 2012, 12, 318–329. [Google Scholar] [CrossRef]
- Bloom, G.; Henson, G.; Peters, D. Innovation in regulation of rapidly changing health markets. Glob. Health 2014, 10, 53. [Google Scholar] [CrossRef] [PubMed]
- Hoa, N.Q.; Thi Lan, P.; Phuc, H.D.; Chuc, N.T.K.; Stalsby-Lundborg, C. Antibiotic prescribing and dispensing for acute respiratory infections in children: Effectiveness of a multi-faceted intervention for health-care providers in Vietnam. Glob. Health Action 2017, 10, 1327638. [Google Scholar] [CrossRef] [PubMed]
- Nhung, N.T.; Cuong, N.V.; Campbell, J.; Hoa, N.T.; Bryant, J.E.; Truc, V.N.; Kiet, B.T.; Jombart, T.; Trung, N.V.; Hien, V.B.; et al. High levels of antimicrobial resistance among escherichia coli isolates from livestock farms and synanthropic rats and shrews in the Mekong Delta of Vietnam. Appl. Environ. Microbiol. 2015, 81, 812–820. [Google Scholar] [CrossRef]
- Liu, Y.Y.; Wang, Y.; Walsh, T.R.; Yi, L.X.; Zhang, R.; Spencer, J.; Doi, Y.; Tian, G.; Dong, B.; Huang, X.; et al. Emergence of plasmid-mediated colistin resistance mechanism MCR-1 in animals and human beings in China: A microbiological and molecular biological study. Lancet Infect. Dis. 2016, 16, 161–168. [Google Scholar] [CrossRef]
- Nguyen, N.T.; Nguyen, H.M.; Nguyen, C.V.; Nguyen, T.V.; Nguyen, M.T.; Thai, H.Q.; Mai, H.H.; Thwaites, G.; Ngo, H.T.; Baker, S.; et al. Use of colistin and other critical antimicrobials on pig and chicken farms in southern Vietnam and its association with resistance in commensal Escherichia coli bacteria. Appl. Environ. Microbiol. 2016, 82, 3727–3735. [Google Scholar] [CrossRef]
- Holloway, K.A.; Rosella, L.; Henry, D. The Impact of WHO Essential Medicines Policies on Inappropriate Use of Antibiotics. PLoS ONE 2016, 11, e0152020. [Google Scholar] [CrossRef]
- Leach, M.; Bett, B.; Said, M.; Bukachi, S.; Sang, R.; Anderson, N.; Machila, N.; Kuleszo, J.; Schaten, K.; Dzingirai, V.; et al. Local disease—Ecosystem—Livelihood dynamics: Reflections from comparative case studies in Africa. Philos. Trans. R. Soc. B Biol. Sci. 2017, 372, 1725. [Google Scholar] [CrossRef]
- Liverani, M.; Waage, J.; Barnett, T.; Pfeiffer, D.U.; Rushton, J.; Rudge, J.W.; Loevinsohn, M.E.; Scoones, I.; Smith, R.D.; Cooper, B.S.; et al. Understanding and managing zoonotic risk in the new livestock industries. Environ. Health Perspect. 2013. [Google Scholar] [CrossRef] [PubMed]
- Bloom, G.; Standing, H.; Lucas, H.; Bhuiya, A.; Oladepo, O.; Peters, D.H. Making health markets work better for poor people: The case of informal providers. Health Policy Plan. 2011, 26, i45–i52. [Google Scholar] [CrossRef] [PubMed]
- Gautham, M.; Shyamprasad, K.M.; Singh, R.; Zachariah, A.; Singh, R.; Bloom, G. Informal rural healthcare providers in North and South India. Health Policy Plan. 2014, 29, i20–i29. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Shen, X.; Wang, Y.; Chen, Y.; Huang, M.; Zeng, Q.; Yang, Y. Antibiotic use in five children’s hospitals during 2002–2006: The impact of antibiotic guidelines issued by the Chinese Ministry of Health. Pharmacoepidemiol. Drug Saf. 2008, 17, 306–311. [Google Scholar] [CrossRef] [PubMed]
- Ristić, S.; Miljković, B.; Vezmar, S.; Stanojević, D. Are local clinical guidelines useful in promoting rational use of antibiotic prophylaxis in caesarean delivery? Pharm. World Sci. 2010, 32, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Zhang, X.; Wang, X.; Zhang, X.; Wan, J.; Zhong, F. Does public reporting influence antibiotic and injection prescribing to all patients? A cluster-randomized matched-pair trial in china. Medicine 2016, 95, e3965. [Google Scholar] [CrossRef]
- Tang, Y.; Liu, C.; Zhang, X. Public reporting as a prescriptions quality improvement measure in primary care settings in China: Variations in effects associated with diagnoses. Sci. Rep. 2016, 6, 39361. [Google Scholar] [CrossRef]
- Tang, Y.; Liu, C.; Zhang, X. Performance associated effect variations of public reporting in promoting antibiotic prescribing practice: A cluster randomized-controlled trial in primary healthcare settings. Prim. Health Care Res. Dev. 2017, 18, 482–491. [Google Scholar] [CrossRef]
- Yang, L.; Liu, C.; Wang, L.; Yin, X.; Zhang, X. Public reporting improves antibiotic prescribing for upper respiratory tract infections in primary care: A matched-pair cluster-randomized trial in China. Health Res. Policy Syst. 2014, 12, 61. [Google Scholar] [CrossRef]
- Santa-Ana-Tellez, Y.; Mantel-Teeuwisse, A.K.; Leufkens, H.G.M.; Wirtz, V.J. Seasonal variation in penicillin use in Mexico and Brazil: Analysis of the impact of over-the-counter restrictions. Antimicrob. Agents Chemother. 2015, 59, 105–110. [Google Scholar] [CrossRef]
- Moura, M.L.; Boszczowski, I.; Mortari, N.; Barrozo, L.V.; Chiaravalloti Neto, F.; Lobo, R.D.; Levin, A.S. The Impact of Restricting Over-the-Counter Sales of Antimicrobial Drugs: Preliminary Analysis of National Data. Medicine 2015, 94, e1605. [Google Scholar] [CrossRef] [PubMed]
- Minzi, O.; Manyilizu, V. Application of basic pharmacology and dispensing practice of antibiotics in accredited drug-dispensing outlets in Tanzania. Drug Healthc. Patient Saf. 2013, 5, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Awad, A.I.; Eltayeb, I.B.; Baraka, O.Z. Changing antibiotics prescribing practices in health centers of Khartoum State, Sudan. Eur. J. Clin. Pharmacol. 2006, 62, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Eltayeb, I.B.; Awad, A.I.; Mohamed-Salih, M.S.; Daffa-Alla, M.A.; Ahmed, M.B.; Ogail, M.A.; Matowe, L. Changing the prescribing patterns of sexually transmitted infections in the White Nile Region of Sudan. Sex. Transm. Infect. 2005, 81, 426–427. [Google Scholar] [CrossRef] [PubMed]
- Messina, A.P.; van den Bergh, D.; Goff, D.A. Antimicrobial Stewardship with Pharmacist Intervention Improves Timeliness of Antimicrobials Across Thirty-three Hospitals in South Africa. Infect. Dis. Ther. 2015, 4, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Shen, J.; Sun, Q.; Zhou, X.; Wei, Y.; Qi, Y.; Zhu, J.; Yan, T. Pharmacist interventions on antibiotic use in inpatients with respiratory tract infections in a Chinese hospital. Int. J. Clin. Pharm. 2011, 33, 929–933. [Google Scholar] [CrossRef]
- Apisarnthanarak, A.; Danchaivijitr, S.; Khawcharoenporn, T.; Limsrivilai, J.; Warachan, B.; Bailey, T.C.; Fraser, V.J. Effectiveness of education and an antibiotic-control program in a tertiary care hospital in Thailand. Clin. Infect. Dis. 2006, 42, 768–775. [Google Scholar] [CrossRef]
- Bantar, C.; Sartori, B.; Vesco, E.; Heft, C.; Saúl, M.; Salamone, F.; Oliva, M.E. A hospitalwide intervention program to optimize the quality of antibiotic use: Impact on prescribing practice, antibiotic consumption, cost savings, and bacterial resistance. Clin. Infect. Dis. 2003, 37, 180–186. [Google Scholar] [CrossRef]
- Kafle, K.K.; Bhuju, G.B.; Karkee, S.B.; Prasad, R.R.; Shrestha, N.; Shrestha, A.D.; Daud, M. An intervention improving prescribing practices and monitoring drugs availability in a district. Nepal Med. Coll. J. NMCJ 2009, 11, 217–221. [Google Scholar]
- Opondo, C.; Ayieko, P.; Ntoburi, S.; Wagai, J.; Opiyo, N.; Irimu, G.; English, M. Effect of a multi-faceted quality improvement intervention on inappropriate antibiotic use in children with non-bloody diarrhoea admitted to district hospitals in Kenya. BMC Pediatr. 2011, 11, 109. [Google Scholar] [CrossRef]
- Chuc, N.T.K.; Larsson, M.; Do, N.T.; Diwan, V.K.; Tomson, G.B.; Falkenberg, T. Improving private pharmacy practice: A multi-intervention experiment in Hanoi, Vietnam. J. Clin. Epidemiol. 2002, 55, 1148–1155. [Google Scholar] [CrossRef]
- Shrestha, N.; Samir, K.; Baltussen, R.; Kafle, K.; Bishai, D.; Niessen, L. Practical approach to lung health in Nepal: Better prescribing and reduction of cost. Trop. Med. Int. Health 2006, 11, 765–772. [Google Scholar] [CrossRef] [PubMed]
- Sun, Q.; Dyar, O.J.; Zhao, L.; Tomson, G.; Nilsson, L.E.; Grape, M.; Lundborg, C.S. Overuse of antibiotics for the common cold—Attitudes and behaviors among doctors in rural areas of Shandong Province, China. BMC Pharmacol. Toxicol. 2015, 16, 6. [Google Scholar] [CrossRef] [PubMed]
- Esmaily, H.; Silver, I.; Shiva, S.; Gargani, A.; Maleki-Dizaji, N.; Al-Maniri, A.; Wahlstrom, R. Can rational prescribing be improved by an outcome-based educational approach? A randomized trial completed in Iran. J. Contin. Educ. Health Prof. 2010, 30, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Shao, A.F.; Rambaud-Althaus, C.; Samaka, J.; Faustine, A.F.; Perri-Moore, S.; Swai, N.; D’Acremont, V. New Algorithm for Managing Childhood Illness Using Mobile Technology (ALMANACH): A controlled non-inferiority study on clinical outcome and antibiotic use in Tanzania. PLoS ONE 2015, 10, e0132316. [Google Scholar] [CrossRef] [PubMed]
- Rambaud-Althaus, C.; Shao, A.; Samaka, J.; Swai, N.; Perri, S.; Kahama-Maro, J.; Genton, B. Performance of Health workers using an Electronic Algorithm for the Management of Childhood Illness in Tanzania: A pilot implementation study. Am. J. Trop. Med. Hyg. 2017, 96, 249–257. [Google Scholar] [CrossRef]
- Bhavnani, D.; Phatinawin, L.; Chantra, S.; Olsen, S.J.; Simmerman, J.M. The influence of rapid influenza diagnostic testing on antibiotic prescribing patterns in rural Thailand. Int. J. Infect. Dis. 2007, 11, 355–359. [Google Scholar] [CrossRef]
- Yip, W.; Powell-Jackson, T.; Chen, W.; Hu, M.; Fe, E.; Hu, M.; Hsiao, W. Capitation combined with pay-for-performance improves antibiotic prescribing practices in rural China. Health Aff. 2014, 33, 502–510. [Google Scholar] [CrossRef]
- Kallel, H.; Abboud, P.; Nkouka, S.; Mahamat, A.; Moreau, B.; Nkont Cho, F.; Saint-Lorant, G.; Djossou, F. Effectiveness of postprescription antibiotic stewardship to reduce carbapenem consumption: A quantitative study. J. Hosp. Infect. 2017, 97, 294–295. [Google Scholar] [CrossRef]
- Ma, X.; Xie, J.; Yang, Y.; Guo, F.; Gao, Z.; Shao, H.; Huang, Y.; Yang, C.; Qiu, H. Antimicrobial stewardship of Chinese ministry of health reduces multidrug-resistant organism isolates in critically ill patients: A pre-post study from a single center. BMC Infect. Dis. 2016, 16, 704. [Google Scholar] [CrossRef]
- Ozkurt, Z.; Erol, S.; Kadanali, A.; Ertek, M.; Ozden, K.; Tasyaran, M.A. Changes in antibiotic use, cost and consumption after an antibiotic restriction policy applied by infectious disease specialists. Jpn. J. Infect. Dis. 2005, 58, 338–343. [Google Scholar] [PubMed]
- Zhang, H.H.; Du, Y.; Liu, W.; Song, S.D.; Zhao, W.; Huang, G.W.; Wang, H.S. Effectiveness of Antibiotic Use Management in Tianjin (2011–2013): A Quasi-Experimental Study. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2017, 23, 725–731. [Google Scholar] [CrossRef]
- Marković-Peković, V.; Grubiša, N.; Burger, J.; Bojanić, L.; Godman, B. Initiatives to reduce nonprescription sales and dispensing of antibiotics: Findings and implications. J. Res. Pharm. Pract. 2017, 6, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Magedanz, L.; Silliprandi, E.M.; dos Santos, R.P. Impact of the pharmacist on a multidisciplinary team in an antimicrobial stewardship program: A quasi-experimental study. Int. J. Clin. Pharm. 2012, 34, 290–294. [Google Scholar] [CrossRef] [PubMed]
- Ding, D.; Pan, Q.; Shan, L.; Liu, C.; Gao, L.; Hao, Y.; Liu, G. Prescribing patterns in outpatient clinics of township hospitals in China: A comparative study before and after the 2009 health system reform. Int. J. Environ. Res. Public Health 2016, 13, 679. [Google Scholar] [CrossRef] [PubMed]
- Wei, X.; Yin, J.; Walley, J.D.; Zhang, Z.; Hicks, J.P.; Zhou, Y.; Sun, Q.; Zeng, J.; Lin, M. Impact of China’s essential medicines scheme and zero-mark-up policy on antibiotic prescriptions in county hospitals: A mixed methods study. Trop. Med. Int. Health 2017, 22, 1166–1174. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Bian, Y.; Petzold, M.; Li, L.; Yin, A. The impact of China’s national essential medicine system on improving rational drug use in primary health care facilities: An empirical study in four provinces. BMC Health Serv. Res. 2014, 14, 507. [Google Scholar] [CrossRef]
- Yao, Q.; Liu, C.; Ferrier, J.A.; Liu, Z.; Sun, J. Urban-rural inequality regarding drug prescriptions in primary care facilities—A pre-post comparison of the National Essential Medicines Scheme of China. Int. J. Equity Health 2015, 14, 58. [Google Scholar] [CrossRef]
- Yang, L.; Liu, C.; Ferrier, J.A.; Zhou, W.; Zhang, X. The impact of the National Essential Medicines Policy on prescribing behaviours in primary care facilities in Hubei province of China. Health Policy Plan. 2013, 28, 750–760. [Google Scholar] [CrossRef]
- Uzochukwu, B.S.C.; Onwujekwe, O.E.; Akpala, C.O. Effect of the Bamako-Initiative drug revolving fund on availability and rational use of essential drugs in primary health care facilities in south-east Nigeria. Health Policy Plan. 2002, 17, 378–383. [Google Scholar] [CrossRef]
- Sun, X.; Jackson, S.; Carmichael, G.A.; Sleigh, A.C. Prescribing behaviour of village doctors under China’s New Cooperative Medical Scheme. Soc. Sci. Med. 2009, 68, 1775–1779. [Google Scholar] [CrossRef] [PubMed]
- Holloway, K.A.; Karkee, S.; Tamang, A.; Gurung, Y.B.; Pradhan, R.; Reeves, B.C. The effect of user fees on prescribing quality in rural Nepal: Two controlled pre-post studies to compare a fee per drug unit vs. a fee per drug item. Trop. Med. Int. Health 2009, 13, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Johansson, E.W.; Selling, K.E.; Nsona, H.; Mappin, B.; Gething, P.W.; Petzold, M.; Peterson, S.S.; Hildenwall, H. Integrated paediatric fever management and antibiotic over-treatment in Malawi health facilities: Data mining a national facility census. Malar. J. 2016, 15, 396. [Google Scholar] [CrossRef] [PubMed]
- Potharaju, H.R.; Kabra, S.G. Prescription audit of outpatient attendees of secondary level government hospitals in Maharashtra. Indian J. Pharmacol. 2011, 43, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Ravi, N.; Laha, A.; Hmar, L.; Chatterjee, S.; Goswami, J.; Goel, G.; Dhar, K.; Ghosh, T.; Chatterjee, S.; Datta, S.S.; et al. Exploring the prescribing behaviours and the mind of antibiotic prescribers is critical for a successful antibiotic stewardship programme: Results of a survey from Eastern India. Indian J. Med. Microbiol. 2017, 35, 299–301. [Google Scholar] [PubMed]
- Zaidi, M.B.; Dreser, A.; Figueroa, I.M. A collaborative initiative for the containment of antimicrobial resistance in Mexico. Zoonoses Public Health 2015, 62, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Embrey, M.; Vialle-Valentin, C.; Dillip, A.; Kihiyo, B.; Mbwasi, R.; Semali, I.A.; Chalker, J.C.; Liana, J.; Lieber, R.; Johnson, K.; et al. Understanding the Role of Accredited Drug Dispensing Outlets in Tanzania’s Health System. PLoS ONE 2016, 11, e0164332. [Google Scholar] [CrossRef]
- Shao, A.F.; Rambaud-Althaus, C.; Swai, N.; Kahama-Maro, J.; Genton, B.; D’acremont, V.; Pfeiffer, C. Can smartphones and tablets improve the management of childhood illness in Tanzania? A qualitative study from a primary health care worker’s perspective. BMC Health Serv. Res. 2015, 15, 135. [Google Scholar] [CrossRef]
- Saengcharoen, W.; Chongsuvivatwong, V.; Lerkiatbundit, S.; Wongpoowarak, P. Factors influencing dispensing of antibiotics for upper respiratory infections among Southern Thai community pharmacists. J. Clin. Pharm. Ther. 2008, 33, 123–129. [Google Scholar] [CrossRef]
- Karabay, O.; Hoşoğlu, S.; Güçlü, E.; Akalin, Ş.; Altay, F.A.; Aydin, E.; Ceylan, B.; Çelik, A.; Çelik, İ.; Demirdal, T.; et al. Impact of antimicrobial drug restrictions on doctors’ behaviors. Turk. J. Med. Sci. 2016, 46, 133–138. [Google Scholar] [CrossRef]
- Ozgenç, O.; Genç, V.E.; Ari, A.A.; Sibel, E.; Saçar, S.; Ozunlu, H.; Akgul, A.; Demirturk, N.; Cetin, C.B.; Sungur, M.; et al. Evaluation of the therapeutic use of antibiotics in Aegean Region hospitals of Turkey: A multicentric study. Indian J. Med. Microbiol. 2011, 29, 124–129. [Google Scholar] [CrossRef] [PubMed]


| Database | Result |
|---|---|
| Scopus | 20,083 |
| Cochrane Central Register of Controlled Trials (CENTRAL) | 3823 |
| 3ie Impact Evaluations | 26 |
| World Organisation for Animal Health (OIE) | 0 |
| Total | 32,066 |
| Total after duplicates removed | 17,716 |
| Total 2000–2017 | 15,142 |
| Stages | |
|---|---|
| Abstract review | 15,142 |
| Excluded (did not meet inclusion criteria) | 14,734 |
| Included- | 408 |
| Full text review | 408 |
| Excluded—did not meet inclusion criteria on review | 289 |
| Duplicates (e.g., studies reporting same data) | 4 |
| Full text not available/not in English | 13 |
| Included—context studies | 32 |
| Included—intervention studies | 70 |
| Total—context and intervention | 102 |
| Country, by World Health Organisation Region | |
|---|---|
| African region | 15 |
| Kenya | 3 |
| Mali | 1 |
| Malawi | 1 |
| Nigeria | 3 |
| South Africa | 2 |
| Sudan | 2 |
| Tanzania | 3 |
| Region of the Americas | 5 |
| Argentina | 1 |
| Brazil | 2 |
| Brazil and Mexico | 1 |
| French Guiana | 1 |
| European region | 7 |
| Republic of Srpska, Bosnia and Herzegovina | 1 |
| Serbia | 2 |
| Turkey | 4 |
| Eastern Mediterranean region | 3 |
| Pakistan | 1 |
| Iran | 2 |
| South-East Asian region | 13 |
| India | 6 |
| Indonesia | 1 |
| Nepal | 3 |
| Thailand | 2 |
| Thailand and Vietnam | 1 |
| Western Pacific Region | 27 |
| China | 25 |
| Vietnam | 2 |
| Total | 70 |
| Type of Intervention | Hospital | Primary Care | Pharmacies | Mixed Settings | Total |
|---|---|---|---|---|---|
| Norms and standards (formal and informal) | |||||
| Accreditation | 1 | 1 | |||
| Guidelines | 3 | 3 | |||
| Public reporting | 4 | 4 | |||
| Restrict over-the-counter sales | 2 | 2 | |||
| Prescription control | 1 | 1 | |||
| Knowledge | |||||
| Audit/Feedback | 8 | 2 | 10 | ||
| Education | 2 | 3 | 2 | 2 | 9 |
| Education/Feedback | 3 | 2 | 5 | ||
| Education/Feedback/Regulation | 2 | 2 | |||
| Information | 1 | 1 | |||
| Decision support | |||||
| Algorithms | 1 | 2 | 3 | ||
| Diagnostics | 2 | 1 | 3 | ||
| Supply chain | |||||
| Decentralisation of Supply | 1 | 1 | |||
| Drug Delivery | 1 | 1 | |||
| Economic | |||||
| Financial incentives | 1 | 1 | |||
| Pricing strategy | 1 | 1 | |||
| Health Insurance | 2 | 1 | 3 | ||
| Organisational/management systems | |||||
| Essential Medicine Policy | 2 | 5 | 1 | 8 | |
| Stewardship Programme | 10 | 1 | 11 | ||
| Total | 36 | 22 | 9 | 3 | 70 |
 .
.| Type of Intervention | Reported Impact | Total | |||
|---|---|---|---|---|---|
| Positive | Mixed | Negative | No Effect | ||
| Norms and standards (formal and informal) | |||||
| Accreditation | 1 | 1 | |||
| Guidelines | 2 | 2 | |||
| Public reporting | 4 | 4 | |||
| Restrict over-the-counter sales | 2 | 2 | |||
| Prescription control | 0 | ||||
| Knowledge | |||||
| Audit/Feedback | 4 | 4 | |||
| Education | 2 | 1 | 4 | ||
| Education/Feedback | 4 | 1 | 4 | ||
| Education/Feedback/Regulation | 1 | 1 | |||
| Information | 0 | ||||
| Decision support | |||||
| Algorithms | 1 | 1 | 2 | ||
| Diagnostics | 1 | 1 | 2 | ||
| Supply chain | |||||
| Decentralisation of Supply | 0 | ||||
| Drug Delivery | 0 | ||||
| Economic | |||||
| Financial incentives | 1 | 1 | |||
| Pricing strategy | 1 | 1 | |||
| Health Insurance | 1 | 1 | |||
| Organisational/management systems | |||||
| Essential Medicine Policy | 4 | 1 | 1 | 6 | |
| Stewardship Programme | 5 | 1 | 6 | ||
| Total | 21 | 13 | 4 | 3 | 41 |
.| Reported Results | Intervention Pathway | Total | |
|---|---|---|---|
| Single | Mixed/Multifaceted | ||
| Positive | 8 | 12 | 20 |
| Mixed | 5 | 8 | 13 |
| Negative | 4 | 0 | 4 |
| No effect | 2 | 1 | 3 |
| Total | 19 | 21 | 40 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wilkinson, A.; Ebata, A.; MacGregor, H. Interventions to Reduce Antibiotic Prescribing in LMICs: A Scoping Review of Evidence from Human and Animal Health Systems. Antibiotics 2019, 8, 2. https://doi.org/10.3390/antibiotics8010002
Wilkinson A, Ebata A, MacGregor H. Interventions to Reduce Antibiotic Prescribing in LMICs: A Scoping Review of Evidence from Human and Animal Health Systems. Antibiotics. 2019; 8(1):2. https://doi.org/10.3390/antibiotics8010002
Chicago/Turabian StyleWilkinson, Annie, Ayako Ebata, and Hayley MacGregor. 2019. "Interventions to Reduce Antibiotic Prescribing in LMICs: A Scoping Review of Evidence from Human and Animal Health Systems" Antibiotics 8, no. 1: 2. https://doi.org/10.3390/antibiotics8010002
APA StyleWilkinson, A., Ebata, A., & MacGregor, H. (2019). Interventions to Reduce Antibiotic Prescribing in LMICs: A Scoping Review of Evidence from Human and Animal Health Systems. Antibiotics, 8(1), 2. https://doi.org/10.3390/antibiotics8010002