

Medical-Grade Honey as a Potential New Therapy for Bacterial Vaginosis
 ,
, 
Abstract
1. Introduction
2. Can MGH Create a Paradigm Shift in the Treatment of BV?
3. Broad-Spectrum Antimicrobial Activity of MGH
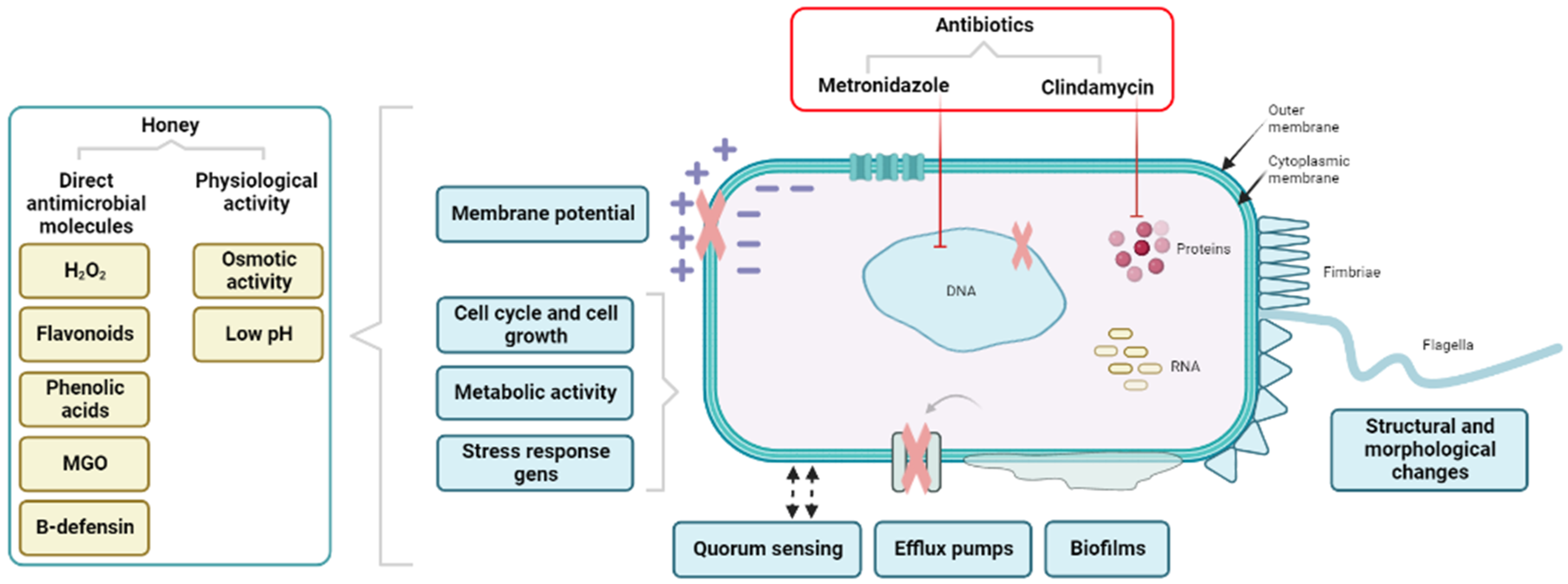
4. In Contrast to Antibiotics, MGH Acts via Multiple Molecular Mechanisms on Bacterial Cells
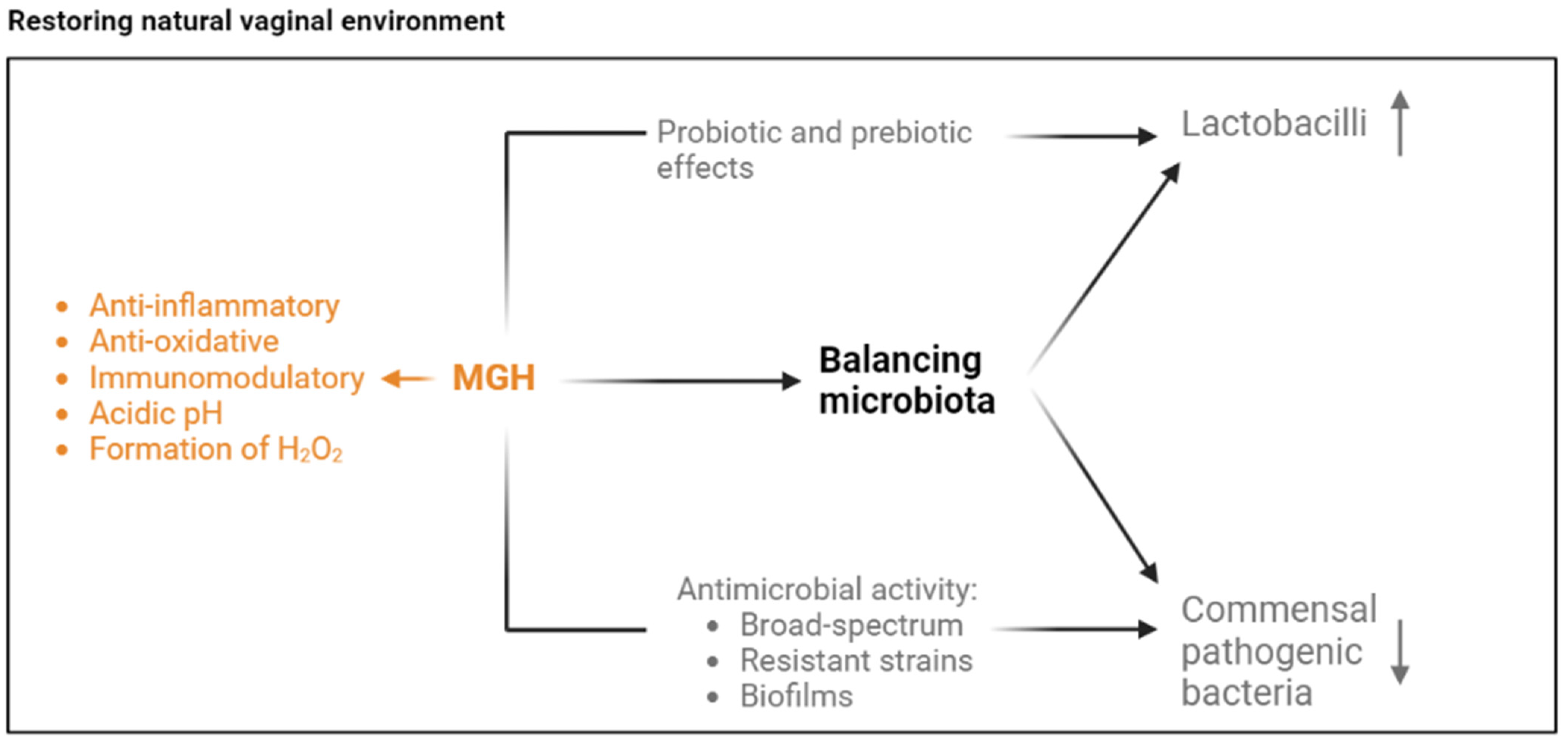
5. MGH Likely Has a Positive Effect on the Vaginal Microbiota
6. MGH Exerts Anti-Inflammatory, Anti-Oxidant, and Immunomodulatory Activity
7. Discussion of the Clinical Evidence of the Concept of MGH for Treating BV
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Peebles, K.; Velloza, J.; Balkus, J.E.; McClelland, R.S.; Barnabas, R.V. High Global Burden and Costs of Bacterial Vaginosis: A Systematic Review and Meta-Analysis. Sex. Transm. Dis. 2019, 46, 304–311. [Google Scholar] [CrossRef] [PubMed]
- Muzny, C.A.; Taylor, C.M.; Swords, W.E.; Tamhane, A.; Chattopadhyay, D.; Cerca, N.; Schwebke, J.R. An Updated Conceptual Model on the Pathogenesis of Bacterial Vaginosis. J. Infect. Dis. 2019, 220, 1399–1405. [Google Scholar] [CrossRef] [PubMed]
- Vodstrcil, L.A.; Muzny, C.A.; Plummer, E.L.; Sobel, J.D.; Bradshaw, C.S. Bacterial vaginosis: Drivers of recurrence and challenges and opportunities in partner treatment. BMC Med. 2021, 19, 194. [Google Scholar] [CrossRef] [PubMed]
- Sobel, J.D.; Mitchell, C. Bacterial Vaginosis: Clinical Manifestations and Diagnosis; UpToDate: Wellesley, MA, USA, 2022. [Google Scholar]
- Kairys, N.; Garg, M. Bacterial Vaginosis. In StatPearls; StatPearls Publishing: St. Petersburg, FL, USA, 2023. [Google Scholar]
- Isik, G.; Demirezen, S.; Donmez, H.G.; Beksac, M.S. Bacterial vaginosis in association with spontaneous abortion and recurrent pregnancy losses. J. Cytol. 2016, 33, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Haahr, T.; Zacho, J.; Brauner, M.; Shathmigha, K.; Skov Jensen, J.; Humaidan, P. Reproductive outcome of patients undergoing in vitro fertilisation treatment and diagnosed with bacterial vaginosis or abnormal vaginal microbiota: A systematic PRISMA review and meta-analysis. BJOG 2019, 126, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Abou Chacra, L.; Ly, C.; Hammoud, A.; Iwaza, R.; Mediannikov, O.; Bretelle, F.; Fenollar, F. Relationship between Bacterial Vaginosis and Sexually Transmitted Infections: Coincidence, Consequence or Co-Transmission? Microorganisms 2023, 11, 2470. [Google Scholar] [CrossRef] [PubMed]
- Abou Chacra, L.; Fenollar, F.; Diop, K. Bacterial Vaginosis: What Do We Currently Know? Front. Cell Infect. Microbiol. 2021, 11, 672429. [Google Scholar] [CrossRef] [PubMed]
- Forcey, D.S.; Vodstrcil, L.A.; Hocking, J.S.; Fairley, C.K.; Law, M.; McNair, R.P.; Bradshaw, C.S. Factors Associated with Bacterial Vaginosis among Women Who Have Sex with Women: A Systematic Review. PLoS ONE 2015, 10, e0141905. [Google Scholar] [CrossRef]
- Koumans, E.H.; Sternberg, M.; Bruce, C.; McQuillan, G.; Kendrick, J.; Sutton, M.; Markowitz, L.E. The prevalence of bacterial vaginosis in the United States, 2001–2004; associations with symptoms, sexual behaviors, and reproductive health. Sex. Transm. Dis. 2007, 34, 864–869. [Google Scholar] [CrossRef] [PubMed]
- Muzny, C.A.; Laniewski, P.; Schwebke, J.R.; Herbst-Kralovetz, M.M. Host-vaginal microbiota interactions in the pathogenesis of bacterial vaginosis. Curr. Opin. Infect. Dis. 2020, 33, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Muller, P.; Alber, D.G.; Turnbull, L.; Schlothauer, R.C.; Carter, D.A.; Whitchurch, C.B.; Harry, E.J. Synergism between Medihoney and rifampicin against methicillin-resistant Staphylococcus aureus (MRSA). PLoS ONE 2013, 8, e57679. [Google Scholar] [CrossRef] [PubMed]
- Koumans, E.H.; Markowitz, L.E.; Hogan, V.; Group, C.B.W. Indications for therapy and treatment recommendations for bacterial vaginosis in nonpregnant and pregnant women: A synthesis of data. Clin. Infect. Dis. 2002, 35, S152–S172. [Google Scholar] [CrossRef] [PubMed]
- Vodstrcil, L.A.; Hocking, J.S.; Law, M.; Walker, S.; Tabrizi, S.N.; Fairley, C.K.; Bradshaw, C.S. Hormonal contraception is associated with a reduced risk of bacterial vaginosis: A systematic review and meta-analysis. PLoS ONE 2013, 8, e73055. [Google Scholar] [CrossRef] [PubMed]
- Oduyebo, O.O.; Anorlu, R.I.; Ogunsola, F.T. The effects of antimicrobial therapy on bacterial vaginosis in non-pregnant women. Cochrane Database Syst. Rev. 2009, 8, CD006055. [Google Scholar] [CrossRef] [PubMed]
- Bradshaw, C.S.; Morton, A.N.; Hocking, J.; Garland, S.M.; Morris, M.B.; Moss, L.M.; Horvath, L.B.; Kuzevska, I.; Fairley, C.K. High recurrence rates of bacterial vaginosis over the course of 12 months after oral metronidazole therapy and factors associated with recurrence. J. Infect. Dis. 2006, 193, 1478–1486. [Google Scholar] [CrossRef] [PubMed]
- Bradshaw, C.S.; Sobel, J.D. Current Treatment of Bacterial Vaginosis-Limitations and Need for Innovation. J. Infect. Dis. 2016, 214 (Suppl. S1), S14–S20. [Google Scholar] [CrossRef] [PubMed]
- Joseph, R.J.; Ser, H.L.; Kuai, Y.H.; Tan, L.T.; Arasoo, V.J.T.; Letchumanan, V.; Wang, L.; Pusparajah, P.; Goh, B.H.; Ab Mutalib, N.S.; et al. Finding a Balance in the Vaginal Microbiome: How Do We Treat and Prevent the Occurrence of Bacterial Vaginosis? Antibiotics 2021, 10, 719. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Li, R.; Qing, W.; Zhang, Y.; Zhou, Z.; Hou, Y.; Shi, Y.; Zhou, H.; Chen, M. Probiotics are a good choice for the treatment of bacterial vaginosis: A meta-analysis of randomized controlled trial. Reprod. Health 2022, 19, 137. [Google Scholar] [CrossRef] [PubMed]
- Tan, H.; Fu, Y.; Yang, C.; Ma, J. Effects of metronidazole combined probiotics over metronidazole alone for the treatment of bacterial vaginosis: A meta-analysis of randomized clinical trials. Arch. Gynecol. Obstet. 2017, 295, 1331–1339. [Google Scholar] [CrossRef] [PubMed]
- Senok, A.C.; Verstraelen, H.; Temmerman, M.; Botta, G.A. Probiotics for the treatment of bacterial vaginosis. Cochrane Database Syst. Rev. 2009, CD006289. [Google Scholar] [CrossRef]
- Majno, G. The Healing Hand: Man and Wound in the Ancient World, 1st ed.; Harvard University Press: Cambridge, MA, USA, 1975; p. 571. [Google Scholar]
- Metwaly, A.M.; Ghoneim, M.M.; Eissa, I.H.; Elsehemy, I.A.; Mostafa, A.E.; Hegazy, M.M.; Afifi, W.M.; Dou, D. Traditional ancient Egyptian medicine: A review. Saudi J. Biol. Sci. 2021, 28, 5823–5832. [Google Scholar] [CrossRef]
- Postmes, T.; van den Bogaard, A.E.; Hazen, M. Honey for wounds, ulcers, and skin graft preservation. Lancet 1993, 341, 756–757. [Google Scholar] [CrossRef]
- Hermanns, R.; Mateescu, C.; Thrasyvoulou, A.; Tananaki, C.; Wagener, F.A.; Cremers, N.A. Defining the standards for medical grade honey. J. Apic. Res. 2020, 59, 125–135. [Google Scholar] [CrossRef]
- Smaropoulos, E.; Cremers, N.A.J. Medical-Grade Honey for the Treatment of Extravasation-Induced Injuries in Preterm Neonates: A Case Series. Adv. Neonatal Care 2021, 21, 122–132. [Google Scholar] [CrossRef] [PubMed]
- van Riel, S.; Lardenoije, C.; Oudhuis, G.J.; Cremers, N.A.J. Treating (Recurrent) Vulvovaginal Candidiasis with Medical-Grade Honey-Concepts and Practical Considerations. J. Fungi 2021, 7, 664. [Google Scholar] [CrossRef] [PubMed]
- Cremers, N.A. Something old, something new: Does medical grade honey target multidrug resistance? J. Wound Care 2021, 30, 160–161. [Google Scholar] [CrossRef] [PubMed]
- Kontogiannis, T.; Dimitriou, T.G.; Didaras, N.A.; Mossialos, D. Antiviral Activity of Bee Products. Curr. Pharm. Des. 2022, 28, 2867–2878. [Google Scholar] [CrossRef] [PubMed]
- Schell, K.R.; Fernandes, K.E.; Shanahan, E.; Wilson, I.; Blair, S.E.; Carter, D.A.; Cokcetin, N.N. The Potential of Honey as a Prebiotic Food to Re-engineer the Gut Microbiome Toward a Healthy State. Front. Nutr. 2022, 9, 957932. [Google Scholar] [CrossRef] [PubMed]
- Mohan, A.; Quek, S.-Y.; Gutierrez-Maddox, N.; Gao, Y.; Shu, Q. Effect of honey in improving the gut microbial balance. Food Qual. Saf. 2017, 1, 107–115. [Google Scholar] [CrossRef]
- Mandal, M.D.; Mandal, S. Honey: Its medicinal property and antibacterial activity. Asian Pac. J. Trop. Biomed. 2011, 1, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Ranneh, Y.; Akim, A.M.; Hamid, H.A.; Khazaai, H.; Fadel, A.; Zakaria, Z.A.; Albujja, M.; Bakar, M.F.A. Honey and its nutritional and anti-inflammatory value. BMC Complement. Med. Ther. 2021, 21, 30. [Google Scholar] [CrossRef] [PubMed]
- Rao, P.V.; Krishnan, K.T.; Salleh, N.; Gan, S.H. Biological and therapeutic effects of honey produced by honey bees and stingless bees: A comparative review. Rev. Bras. Farmacogn. 2016, 26, 657–664. [Google Scholar] [CrossRef]
- Le Marrec, C. Responses of Lactic Acid Bacteria to Osmotic Stress. In Stress Responses of Lactic Acid Bacteria. Food Microbiology and Food Safety; Tsakalidou, E., Papadimitriou, K., Eds.; Springer: Boston, MA, USA, 2011. [Google Scholar] [CrossRef]
- Chen, L.; Gu, Q.; Li, P.; Chen, S.; Li, Y. Genomic analysis of Lactobacillus reuteri WHH1689 reveals its probiotic properties and stress resistance. Food Sci. Nutr. 2019, 7, 844–857. [Google Scholar] [CrossRef] [PubMed]
- Haddaji, N.; Mahdhi, A.K.; Krifi, B.; Ismail, M.B.; Bakhrouf, A. Change in cell surface properties of Lactobacillus casei under heat shock treatment. FEMS Microbiol. Lett. 2015, 362, fnv047. [Google Scholar] [CrossRef] [PubMed]
- Bremer, E.; Kramer, R. Responses of Microorganisms to Osmotic Stress. Annu. Rev. Microbiol. 2019, 73, 313–334. [Google Scholar] [CrossRef] [PubMed]
- Glaasker, E.; Tjan, F.S.; Ter Steeg, P.F.; Konings, W.N.; Poolman, B. Physiological response of Lactobacillus plantarum to salt and nonelectrolyte stress. J. Bacteriol. 1998, 180, 4718–4723. [Google Scholar] [CrossRef] [PubMed]
- Almasaudi, S. The antibacterial activities of honey. Saudi J. Biol. Sci. 2021, 28, 2188–2196. [Google Scholar] [CrossRef] [PubMed]
- Combarros-Fuertes, P.; Fresno, J.M.; Estevinho, M.M.; Sousa-Pimenta, M.; Tornadijo, M.E.; Estevinho, L.M. Honey: Another Alternative in the Fight against Antibiotic-Resistant Bacteria? Antibiotics 2020, 9, 774. [Google Scholar] [CrossRef] [PubMed]
- Corcoran, B.M.; Stanton, C.; Fitzgerald, G.F.; Ross, R.P. Survival of probiotic lactobacilli in acidic environments is enhanced in the presence of metabolizable sugars. Appl. Environ. Microbiol. 2005, 71, 3060–3067. [Google Scholar] [CrossRef] [PubMed]
- Collins, E.B.; Aramaki, K. Production of Hydrogen peroxide by Lactobacillus acidophilus. J. Dairy. Sci. 1980, 63, 353–357. [Google Scholar] [CrossRef] [PubMed]
- Strus, M.; Brzychczy-Wloch, M.; Gosiewski, T.; Kochan, P.; Heczko, P.B. The in vitro effect of hydrogen peroxide on vaginal microbial communities. FEMS Immunol. Med. Microbiol. 2006, 48, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Imlay, J.A. How oxygen damages microbes: Oxygen tolerance and obligate anaerobiosis. Adv. Microb. Physiol. 2002, 46, 111–153. [Google Scholar] [CrossRef] [PubMed]
- Barynin, V.V.; Whittaker, M.M.; Antonyuk, S.V.; Lamzin, V.S.; Harrison, P.M.; Artymiuk, P.J.; Whittaker, J.W. Crystal structure of manganese catalase from Lactobacillus plantarum. Structure 2001, 9, 725–738. [Google Scholar] [CrossRef] [PubMed]
- Smaropoulos, E.; Cremers, N.A.J. Treating severe wounds in pediatrics with medical grade honey: A case series. Clin. Case Rep. 2020, 8, 469–476. [Google Scholar] [CrossRef] [PubMed]
- Combarros-Fuertes, P.; Estevinho, L.M.; Dias, L.G.; Castro, J.M.; Tomas-Barberan, F.A.; Tornadijo, M.E.; Fresno-Baro, J.M. Bioactive Components and Antioxidant and Antibacterial Activities of Different Varieties of Honey: A Screening Prior to Clinical Application. J. Agric. Food Chem. 2019, 67, 688–698. [Google Scholar] [CrossRef] [PubMed]
- Samarghandian, S.; Farkhondeh, T.; Samini, F. Honey and Health: A Review of Recent Clinical Research. Pharmacogn. Res. 2017, 9, 121–127. [Google Scholar] [CrossRef]
- Combarros-Fuertes, P.; Estevinho, L.M.; Teixeira-Santos, R.; Rodrigues, A.G.; Pina-Vaz, C.; Fresno, J.M.; Tornadijo, M.E. Antibacterial Action Mechanisms of Honey: Physiological Effects of Avocado, Chestnut, and Polyfloral Honey upon Staphylococcus aureus and Escherichia coli. Molecules 2020, 25, 1252. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, A.; Kaleem, M.; Ahmed, Z.; Shafiq, H. Therapeutic potential of flavonoids and their mechanism of action against microbial and viral infections—A review. Food Res. Int. 2015, 77, 221–235. [Google Scholar] [CrossRef]
- de Groot, T.; Janssen, T.; Faro, D.; Cremers, N.A.J.; Chowdhary, A.; Meis, J.F. Antifungal Activity of a Medical-Grade Honey Formulation against Candida auris. J. Fungi 2021, 7, 50. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, K.; Rahmasari, R.; Matsunaga, A.; Haruyama, T.; Kobayashi, N. Anti-influenza viral effects of honey in vitro: Potent high activity of manuka honey. Arch. Med. Res. 2014, 45, 359–365. [Google Scholar] [CrossRef] [PubMed]
- Naik, P.P.; Mossialos, D.; Wijk, B.V.; Novakova, P.; Wagener, F.; Cremers, N.A.J. Medical-Grade Honey Outperforms Conventional Treatments for Healing Cold Sores-A Clinical Study. Pharmaceuticals 2021, 14, 1264. [Google Scholar] [CrossRef] [PubMed]
- Rohmatin, E.; Patmawati, N.M.; Yuliastuti, S.; Sahlan, M. Topical effect of tetragonula sapiens honey on the healing process of post-caesarean section wounds. Int. J. Appl. Pharm. 2022, 14, 18–21. [Google Scholar] [CrossRef]
- Ranneh, Y.; Akim, A.M.; Hamid, H.A.; Khazaai, H.; Fadel, A.; Mahmoud, A.M. Stingless bee honey protects against lipopolysaccharide induced-chronic subclinical systemic inflammation and oxidative stress by modulating Nrf2, NF-kappaB and p38 MAPK. Nutr. Metab. 2019, 16, 15. [Google Scholar] [CrossRef] [PubMed]
- Antimicrobial Resistance, C. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- Regmi, A.; Ojha, N.; Singh, M.; Ghimire, A.; Kharel, N. Risk Factors Associated with Surgical Site Infection following Cesarean Section in Tertiary Care Hospital, Nepal. Int. J. Reprod. Med. 2022, 2022, 4442453. [Google Scholar] [CrossRef] [PubMed]
- Ayukekbong, J.A.; Ntemgwa, M.; Atabe, A.N. The threat of antimicrobial resistance in developing countries: Causes and control strategies. Antimicrob. Resist. Infect. Control 2017, 6, 47. [Google Scholar] [CrossRef] [PubMed]
- Ventola, C.L. The antibiotic resistance crisis: Part 1: Causes and threats. Pharm. Ther. 2015, 40, 277–283. [Google Scholar]
- Majtan, J.; Sojka, M.; Palenikova, H.; Bucekova, M.; Majtan, V. Vitamin C Enhances the Antibacterial Activity of Honey against Planktonic and Biofilm-Embedded Bacteria. Molecules 2020, 25, 992. [Google Scholar] [CrossRef] [PubMed]
- Pleeging, C.C.F.; Coenye, T.; Mossialos, D.; de Rooster, H.; Chrysostomou, D.; Wagener, F.; Cremers, N.A.J. Synergistic Antimicrobial Activity of Supplemented Medical-Grade Honey against Pseudomonas aeruginosa Biofilm Formation and Eradication. Antibiotics 2020, 9, 866. [Google Scholar] [CrossRef]
- Roy, R.; Tiwari, M.; Donelli, G.; Tiwari, V. Strategies for combating bacterial biofilms: A focus on anti-biofilm agents and their mechanisms of action. Virulence 2018, 9, 522–554. [Google Scholar] [CrossRef] [PubMed]
- Limoli, D.H.; Jones, C.J.; Wozniak, D.J. Bacterial Extracellular Polysaccharides in Biofilm Formation and Function. Microbiol. Spectr. 2015, 3, 223–247. [Google Scholar] [CrossRef] [PubMed]
- Sharma, D.; Misba, L.; Khan, A.U. Antibiotics versus biofilm: An emerging battleground in microbial communities. Antimicrob. Resist. Infect. Control 2019, 8, 76. [Google Scholar] [CrossRef] [PubMed]
- Hoiby, N.; Bjarnsholt, T.; Moser, C.; Bassi, G.L.; Coenye, T.; Donelli, G.; Hall-Stoodley, L.; Hola, V.; Imbert, C.; Kirketerp-Moller, K.; et al. ESCMID guideline for the diagnosis and treatment of biofilm infections 2014. Clin. Microbiol. Infect. 2015, 21 (Suppl. S1), S1–S25. [Google Scholar] [CrossRef] [PubMed]
- Versey, Z.; da Cruz Nizer, W.S.; Russell, E.; Zigic, S.; DeZeeuw, K.G.; Marek, J.E.; Overhage, J.; Cassol, E. Biofilm-Innate Immune Interface: Contribution to Chronic Wound Formation. Front. Immunol. 2021, 12, 648554. [Google Scholar] [CrossRef] [PubMed]
- Mirzaei, R.; Mohammadzadeh, R.; Alikhani, M.Y.; Shokri Moghadam, M.; Karampoor, S.; Kazemi, S.; Barfipoursalar, A.; Yousefimashouf, R. The biofilm-associated bacterial infections unrelated to indwelling devices. IUBMB Life 2020, 72, 1271–1285. [Google Scholar] [CrossRef] [PubMed]
- Swidsinski, A.; Mendling, W.; Loening-Baucke, V.; Ladhoff, A.; Swidsinski, S.; Hale, L.P.; Lochs, H. Adherent biofilms in bacterial vaginosis. Obstet. Gynecol. 2005, 106, 1013–1023. [Google Scholar] [CrossRef] [PubMed]
- Adinortey, C.A.; Wilson, M.; Kwofie, S.K. Honey as a Natural Product Worthy of Re-Consideration in Treating MRSA Wound Infections; Intech Open: London, UK, 2022. [Google Scholar]
- Scepankova, H.; Combarros-Fuertes, P.; Fresno, J.M.; Tornadijo, M.E.; Dias, M.S.; Pinto, C.A.; Saraiva, J.A.; Estevinho, L.M. Role of Honey in Advanced Wound Care. Molecules 2021, 26, 4784. [Google Scholar] [CrossRef] [PubMed]
- Pleeging, C.C.F.; Wagener, F.; de Rooster, H.; Cremers, N.A.J. Revolutionizing non-conventional wound healing using honey by simultaneously targeting multiple molecular mechanisms. Drug Resist. Updates 2022, 62, 100834. [Google Scholar] [CrossRef] [PubMed]
- Dryden, M.; Goddard, C.; Madadi, A.; Heard, M.; Saeed, K.; Cooke, J. Using antimicrobial surgihoneyto prevent caesarean wound infection. Br. J. Midwifery 2014, 22, 111–115. [Google Scholar] [CrossRef]
- Gustafsson, K.; Tatz, A.J.; Slavin, R.A.; Sutton, G.A.; Dahan, R.; Abu Ahmad, W.; Kelmer, G. Intra-incisional medical grade honey decreases the prevalence of incisional infection in horses undergoing colic surgery: A prospective randomised controlled study. Equine Vet. J. 2021, 53, 1112–1118. [Google Scholar] [CrossRef] [PubMed]
- Ng, W.J.; Sit, N.W.; Ooi, P.A.; Ee, K.Y.; Lim, T.M. The Antibacterial Potential of Honeydew Honey Produced by Stingless Bee (Heterotrigona itama) against Antibiotic Resistant Bacteria. Antibiotics 2020, 9, 871. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, R.; Cooper, R. Improving antibiotic activity against wound pathogens with manuka honey in vitro. PLoS ONE 2012, 7, e45600. [Google Scholar] [CrossRef] [PubMed]
- Campeau, M.E.; Patel, R. Antibiofilm Activity of Manuka Honey in Combination with Antibiotics. Int. J. Bacteriol. 2014, 2014, 795281. [Google Scholar] [CrossRef] [PubMed]
- Reygaert, W.C. An overview of the antimicrobial resistance mechanisms of bacteria. AIMS Microbiol. 2018, 4, 482–501. [Google Scholar] [CrossRef] [PubMed]
- Maddocks, S.E.; Jenkins, R.E. Honey: A sweet solution to the growing problem of antimicrobial resistance? Future Microbiol. 2013, 8, 1419–1429. [Google Scholar] [CrossRef] [PubMed]
- Schencke, C.; Vasconcellos, A.; Sandoval, C.; Torres, P.; Acevedo, F.; Del Sol, M. Morphometric evaluation of wound healing in burns treated with Ulmo (Eucryphia cordifolia) honey alone and supplemented with ascorbic acid in guinea pig (Cavia porcellus). Burn. Trauma 2016, 4, 25. [Google Scholar] [CrossRef] [PubMed]
- Dingsdag, S.A.; Hunter, N. Metronidazole: An update on metabolism, structure-cytotoxicity and resistance mechanisms. J. Antimicrob. Chemother. 2018, 73, 265–279. [Google Scholar] [CrossRef] [PubMed]
- Dhand, A.; Snydman, D.R. Antimicrobial Drug Resistance; Mayers, D.L., Ed.; Humana Press: New York, NY, USA, 2009. [Google Scholar]
- Kulczycka-Mierzejewska, K.; Sadlej, J.; Trylska, J. Molecular dynamics simulations suggest why the A2058G mutation in 23S RNA results in bacterial resistance against clindamycin. J. Mol. Model. 2018, 24, 191. [Google Scholar] [CrossRef] [PubMed]
- Spizek, J.; Rezanka, T. Lincosamides: Chemical structure, biosynthesis, mechanism of action, resistance, and applications. Biochem. Pharmacol. 2017, 133, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Ng, W.J.; Hing, C.L.; Loo, C.B.; Hoh, E.K.; Loke, I.L.; Ee, K.Y. Ginger-Enriched Honey Attenuates Antibiotic Resistant Pseudomonas aeruginosa Quorum Sensing Virulence Factors and Biofilm Formation. Antibiotics 2023, 12, 1123. [Google Scholar] [CrossRef] [PubMed]
- Tsavea, E.; Tzika, P.; Katsivelou, E.; Adamopoulou, A.; Nikolaidis, M.; Amoutzias, G.D.; Mossialos, D. Impact of Mt. Olympus Honeys on Virulence Factors Implicated in Pathogenesis Exerted by Pseudomonas aeruginosa. Antibiotics 2023, 12, 998. [Google Scholar] [CrossRef] [PubMed]
- Shamala, T.R.; Shri Jyothi, Y.; Saibaba, P. Stimulatory effect of honey on multiplication of lactic acid bacteria under in vitro and in vivo conditions. Lett. Appl. Microbiol. 2000, 30, 453–455. [Google Scholar] [CrossRef] [PubMed]
- Macedo, L.N.; Luchese, R.H.; Guerra, A.F.; Barbosa, C.G. Prebiotic effect of honey on growth and viability of Bifidobacterium spp. and Lactobacillus spp. in milk. Ciência e Tecnol. Aliment. 2008, 28, 935–942. [Google Scholar] [CrossRef]
- Greenbaum, A.; Aryana, K.J. Effect of Honey a Natural Sweetener with Several Medicinal Properties on the Attributes of a Frozen Dessert Containing the Probiotic Lactobacillus acidophilus. Open J. Med. Microbiol. 2013, 3, 95–99. [Google Scholar] [CrossRef][Green Version]
- Bhola, J.; Gokhale, M.; Prajapati, S.; Bhadekar, R. Enhanced probiotic attributes of lactobacilli in honey supplemented media. J. Appl. Biol. Biotechnol. 2023, 11, 200–207. [Google Scholar] [CrossRef]
- Chick, H.; Shin, H.S.; Ustunol, Z. Growth and Acid Production by Lactic Acid Bacteria and Bifidobacteria Grown in Skim Milk Containing Honey. J. Food Sci. 2001, 66, 478–481. [Google Scholar] [CrossRef]
- Mathew, C.; Tesfaye, W.; Rasmussen, P.; Peterson, G.M.; Bartholomaeus, A.; Sharma, M.; Thomas, J. Manuka Oil-A Review of Antimicrobial and Other Medicinal Properties. Pharmaceuticals 2020, 13, 343. [Google Scholar] [CrossRef] [PubMed]
- Hillitt, K.L.; Jenkins, R.E.; Spiller, O.B.; Beeton, M.L. Antimicrobial activity of Manuka honey against antibiotic-resistant strains of the cell wall-free bacteria Ureaplasma parvum and Ureaplasma urealyticum. Lett. Appl. Microbiol. 2017, 64, 198–202. [Google Scholar] [CrossRef] [PubMed]
- Safii, S.H.; Tompkins, G.R.; Duncan, W.J. Periodontal Application of Manuka Honey: Antimicrobial and Demineralising Effects In Vitro. Int. J. Dent. 2017, 2017, 9874535. [Google Scholar] [CrossRef] [PubMed]
- Podrzaj, S. Antibacterial Effectiveness of Different Types of Honey on Parodontopathogenic Bacteria and Oral Streptococci. Thesis, University of Ljubljana, Ljubljana, Slovenia, 2011. Available online: https://repozitorij.uni-lj.si/IzpisGradiva.php?lang=slv&id=118397 (accessed on 24 January 2024).
- Eick, S.; Schafer, G.; Kwiecinski, J.; Atrott, J.; Henle, T.; Pfister, W. Honey—A potential agent against Porphyromonas gingivalis: An in vitro study. BMC Oral Health 2014, 14, 24. [Google Scholar] [CrossRef] [PubMed]
- Otreba, M.; Marek, L.; Tyczynska, N.; Stojko, J.; Rzepecka-Stojko, A. Bee Venom, Honey, and Royal Jelly in the Treatment of Bacterial Infections of the Oral Cavity: A Review. Life 2021, 11, 1311. [Google Scholar] [CrossRef] [PubMed]
- Hammond, E.N.; Donkor, E.S. Antibacterial effect of Manuka honey on Clostridium difficile. BMC Res. Notes 2013, 6, 188. [Google Scholar] [CrossRef] [PubMed]
- Hussain, M.B.; Aly, Y.M.K.M.; Jiman-Fatani, A.A.M.; Ullah, Z.; Qureshi, I.A.; Bakarman, M.A.; Yasir, M.; Al-Maaqar, S.M. Screening of lactic acid bacteria from selected Saudi honey produced by apis mellifera jementica . J. Anim. Plant Sci. 2023, 33, 5. [Google Scholar] [CrossRef]
- Sharma, M.; Wasan, A.; Sharma, R.K. Recent developments in probiotics: An emphasis on Bifidobacterium. Food Biosci. 2021, 41, 100993. [Google Scholar] [CrossRef]
- Raymann, K.; Moran, N.A. The role of the gut microbiome in health and disease of adult honey bee workers. Curr. Opin. Insect Sci. 2018, 26, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Lashani, E.; Davoodabadi, A.; Soltan Dallal, M.M. Some probiotic properties of Lactobacillus species isolated from honey and their antimicrobial activity against foodborne pathogens. Vet. Res. Forum 2020, 11, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Mustar, S.; Ibrahim, N. A Sweeter Pill to Swallow: A Review of Honey Bees and Honey as a Source of Probiotic and Prebiotic Products. Foods 2022, 11, 2102. [Google Scholar] [CrossRef] [PubMed]
- Majtan, J.; Bucekova, M.; Kafantaris, I.; Szweda, P.; Hammer, K.; Mossialos, D. Honey antibacterial activity: A neglected aspect of honey quality assurance as functional food . Trends Food Sci. Technol. 2021, 118, 870–886. [Google Scholar] [CrossRef]
- Nair, H.K.R.; Tatavilis, N.; Pospisilova, I.; Kucerova, J.; Cremers, N.A.J. Medical-Grade Honey Kills Antibiotic-Resistant Bacteria and Prevents Amputation in Diabetics with Infected Ulcers: A Prospective Case Series. Antibiotics 2020, 9, 529. [Google Scholar] [CrossRef]
- Nelson, T.M.; Borgogna, J.L.; Brotman, R.M.; Ravel, J.; Walk, S.T.; Yeoman, C.J. Vaginal biogenic amines: Biomarkers of bacterial vaginosis or precursors to vaginal dysbiosis? Front. Physiol. 2015, 6, 253. [Google Scholar] [CrossRef]
- Srinivasan, S.; Morgan, M.T.; Fiedler, T.L.; Djukovic, D.; Hoffman, N.G.; Raftery, D.; Marrazzo, J.M.; Fredricks, D.N. Metabolic signatures of bacterial vaginosis. mBio 2015, 6. [Google Scholar] [CrossRef] [PubMed]
- Borgogna, J.C.; Shardell, M.D.; Grace, S.G.; Santori, E.K.; Americus, B.; Li, Z.; Ulanov, A.; Forney, L.; Nelson, T.M.; Brotman, R.M.; et al. Biogenic Amines Increase the Odds of Bacterial Vaginosis and Affect the Growth of and Lactic Acid Production by Vaginal Lactobacillus spp. Appl. Environ. Microbiol. 2021, 87, e03068-20. [Google Scholar] [CrossRef] [PubMed]
- Mondal, A.S.; Sharma, R.; Trivedi, N. Bacterial vaginosis: A state of microbial dysbiosis. Med. Microecol. 2023, 16, 100082. [Google Scholar] [CrossRef]
- Chee, W.J.Y.; Chew, S.Y.; Than, L.T.L. Vaginal microbiota and the potential of Lactobacillus derivatives in maintaining vaginal health. Microb. Cell Fact. 2020, 19, 203. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Liu, Z.; Chen, T. Role of Vaginal Microbiota Dysbiosis in Gynecological Diseases and the Potential Interventions. Front. Microbiol. 2021, 12, 643422. [Google Scholar] [CrossRef]
- Lennard, K.; Dabee, S.; Barnabas, S.L.; Havyarimana, E.; Blakney, A.; Jaumdally, S.Z.; Botha, G.; Mkhize, N.N.; Bekker, L.G.; Lewis, D.A.; et al. Microbial Composition Predicts Genital Tract Inflammation and Persistent Bacterial Vaginosis in South African Adolescent Females. Infect. Immun. 2018, 86. [Google Scholar] [CrossRef] [PubMed]
- Kalia, N.; Singh, J.; Kaur, M. Immunopathology of Recurrent Vulvovaginal Infections: New Aspects and Research Directions. Front. Immunol. 2019, 10, 2034. [Google Scholar] [CrossRef] [PubMed]
- Cianciosi, D.; Forbes-Hernandez, T.Y.; Afrin, S.; Gasparrini, M.; Reboredo-Rodriguez, P.; Manna, P.P.; Zhang, J.; Bravo Lamas, L.; Martinez Florez, S.; Agudo Toyos, P.; et al. Phenolic Compounds in Honey and Their Associated Health Benefits: A Review. Molecules 2018, 23, 2322. [Google Scholar] [CrossRef] [PubMed]
- Silva, B.; Biluca, F.C.; Gonzaga, L.V.; Fett, R.; Dalmarco, E.M.; Caon, T.; Costa, A.C.O. In vitro anti-inflammatory properties of honey flavonoids: A review. Food Res. Int. 2021, 141, 110086. [Google Scholar] [CrossRef]
- Yaghoobi, R.; Kazerouni, A.; Kazerouni, O. Evidence for Clinical Use of Honey in Wound Healing as an Anti-bacterial, Anti-inflammatory Anti-oxidant and Anti-viral Agent: A Review. Jundishapur J. Nat. Pharm. Prod. 2013, 8, 100–104. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, L.; Ribeiro, H.; Oliveira, A.; Sanches Silva, A.; Freitas, A.; Henriques, M.; Rodrigues, M.E. Portuguese honeys as antimicrobial agents against Candida species. J. Tradit. Complement. Med. 2021, 11, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Bogdanov, S.; Jurendic, T.; Sieber, R.; Gallmann, P. Honey for nutrition and health: A review. J. Am. Coll. Nutr. 2008, 27, 677–689. [Google Scholar] [CrossRef] [PubMed]
- Vaday, G.G.; Franitza, S.; Schor, H.; Hecht, I.; Brill, A.; Cahalon, L.; Hershkoviz, R.; Lider, O. Combinatorial signals by inflammatory cytokines and chemokines mediate leukocyte interactions with extracellular matrix. J. Leukoc. Biol. 2001, 69, 885–892. [Google Scholar] [CrossRef] [PubMed]
- Sokol, C.L.; Luster, A.D. The chemokine system in innate immunity. Cold Spring Harb. Perspect. Biol. 2015, 7, a016303. [Google Scholar] [CrossRef] [PubMed]
- Miguel, M.G.; Antunes, M.D.; Faleiro, M.L. Honey as a Complementary Medicine. Integr. Med. Insights 2017, 12, 1178633717702869. [Google Scholar] [CrossRef] [PubMed]
- Mesaik, M.A.; Dastagir, N.; Uddin, N.; Rehman, K.; Azim, M.K. Characterization of immunomodulatory activities of honey glycoproteins and glycopeptides. J. Agric. Food Chem. 2015, 63, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, K.; Tatz, A.M.; Slavin, R.A.; Dahan, R.; Ahmad, W.A.; Sutton, G.A.; Kelmer, G. Will local intraoperative application of Medical Grade Honey in the incision protect against incisional infection in horses undergoing colic surgery? AAEP Proc. 2019, 65, 387–388. [Google Scholar]
- Mandel, H.H.; Sutton, G.A.; Abu, E.; Kelmer, G. Intralesional application of medical grade honey improves healing of surgically treated lacerations in horses. Equine Vet. J. 2020, 52, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Papanikolaou, G.E.; Gousios, G.; Cremers, N.A.J. Use of Medical-Grade Honey to Treat Clinically Infected Heel Pressure Ulcers in High-Risk Patients: A Prospective Case Series. Antibiotics 2023, 12, 605. [Google Scholar] [CrossRef] [PubMed]
- Bocoum, A.; Riel, S.; Traore, S.O.; Ngo Oum Ii, E.F.; Traore, Y.; Thera, A.T.; Fane, S.; Dembele, B.T.; Cremers, N.A.J. Medical-Grade Honey Enhances the Healing of Caesarean Section Wounds and Is Similarly Effective to Antibiotics Combined with Povidone-Iodine in the Prevention of Infections-A Prospective Cohort Study. Antibiotics 2023, 12, 92. [Google Scholar] [CrossRef] [PubMed]
- Lanza, M.; Scuderi, S.A.; Capra, A.P.; Casili, G.; Filippone, A.; Campolo, M.; Cuzzocrea, S.; Esposito, E.; Paterniti, I. Effect of a combination of pea protein, grape seed extract and lactic acid in an in vivo model of bacterial vaginosis. Sci. Rep. 2023, 13, 2849. [Google Scholar] [CrossRef] [PubMed]
- Boon, M.E. Honey proves attractive for vaginal use. Jaarversl. LCPL 2003, 32–39. Available online: https://docplayer.net/43938553-A4-honey-cream-proves-attractive-for-vaginal-use-the-vaginal-smear-as-a-test-3.html (accessed on 5 February 2024).
- Nabimeybodi, R.; Meyari, A.; Vahiddastjerdi, M.; Hajimehdipoor, H.; Ghasemi, E.; Bioos, S.; Tansaz, M. The Effect of Flixweed-Honey Vaginal Product on Cervicitis: A Clinical Trial. Res. J. Pharmacogn. 2018, 5, 41–49. [Google Scholar] [CrossRef]
- Hatami, R.; Soltani, N.; Forouzideh, N.; Robati, A.K.; Tavakolizadeh, M. Vaginal Honey as an Adjuvant Therapy for Standard Antibiotic Protocol of Cervicitis: A Randomized Clinical Trial. Res. J. Pharmacogn. 2022, 9, 45–51. [Google Scholar] [CrossRef]
- Hu, K.T.; Zheng, J.X.; Yu, Z.J.; Chen, Z.; Cheng, H.; Pan, W.G.; Yang, W.Z.; Wang, H.Y.; Deng, Q.W.; Zeng, Z.M. Directed shift of vaginal microbiota induced by vaginal application of sucrose gel in rhesus macaques. Int. J. Infect. Dis. 2015, 33, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Ismail, N.H.; Osman, K.; Zulkefli, A.F.; Mokhtar, M.H.; Ibrahim, S.F. The Physicochemical Characteristics of Gelam Honey and Its Outcome on the Female Reproductive Tissue of Sprague-Dawley Rats: A Preliminary Stuy. Molecules 2021, 26, 3346. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Bacterial Strain | Honey | References |
|---|---|---|
| Lactobacilli | ||
| Lactobacilli | Feeding 2 g/day of local Indian honey to rats increased the counts of lactic acid bacteria in their intestines | [88] |
| L. acidophilus (strong probiotic; commonly found in the gastrointestinal tract, oral cavity, and vagina) | Local Indian honey (1% sugar) increased bacterial count in vitro 3% w/v pasteurized Brazilian honey increased the number of viable Lactobacilli in milk 46 days after storage Unknown % honey (light, amber, and dark) increased bacterial count in ice cream 5% w/v honey (Dabur, India) showed an increased bacterial count in milk | [88,89,90,91,92] |
| 5% w/v clover honey showed no effect on bacterial count in milk | ||
| L. casei var. rhamnosus (probiotic vagina) | 5% w/v honey (Dabur, India) increased bacterial count in milk | [91] |
| L. plantarum (probiotic bowel) | 5% w/v honey (Dabur, India) increased bacterial count in milk | [91] |
| L. delbrukeii subsp. bulgaricus (yoghurt production) | 5% w/v clover honey did not affect the bacterial count in milk | [92] |
| Facultative pathogenic bacteria | ||
| G. vaginalis | 7% w/v, formulation, manuka honey decreased the number of bacteria | [93] |
| Atopobium vaginae | 7% w/v, formulation, manuka honey decreased the number of bacteria | [93] |
| Ureaplasma parvum | 20% w/v, manuka honey decreased the number of bacteria | [94] |
| Ureaplasma urealyticum | 20% w/v, manuka honey decreased the number of bacteria | [94] |
| Prevotella intermedia | 50% w/v, different honey types decreased the number of bacteria | [95,96] |
| Pophyromonas gingivitis | Manuka, MGO, and hydrogen peroxide decreased the number of bacteria | [97] |
| Fusobacterium spp. | 6.3–25% w/v Manuka, 25% w/v citrus honey, 5.9 ± 0.9% (w/v) Saturja spp. honey, 6.25% w/v oregano and sage honey decreased the number of bacteria | [98] |
| Clostridiales spp. | Clostridium difficile: 6.25% v/v MIC (Manuka) | [99] |
| Bacteroides species/ P. oris | Different undiluted honey types tested in disc diffusion assay: 8.9–12.1 mm zone of inhibition Bacteroides spp. and 8.5–14.9 mm zone of inhibition P. oris | [96] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lardenoije, C.M.J.G.; van Riel, S.J.J.M.; Peters, L.J.F.; Wassen, M.M.L.H.; Cremers, N.A.J. Medical-Grade Honey as a Potential New Therapy for Bacterial Vaginosis. Antibiotics 2024, 13, 368. https://doi.org/10.3390/antibiotics13040368
Lardenoije CMJG, van Riel SJJM, Peters LJF, Wassen MMLH, Cremers NAJ. Medical-Grade Honey as a Potential New Therapy for Bacterial Vaginosis. Antibiotics. 2024; 13(4):368. https://doi.org/10.3390/antibiotics13040368
Chicago/Turabian StyleLardenoije, Céline M. J. G., Senna J. J. M. van Riel, Linsey J. F. Peters, Martine M. L. H. Wassen, and Niels A. J. Cremers. 2024. "Medical-Grade Honey as a Potential New Therapy for Bacterial Vaginosis" Antibiotics 13, no. 4: 368. https://doi.org/10.3390/antibiotics13040368
APA StyleLardenoije, C. M. J. G., van Riel, S. J. J. M., Peters, L. J. F., Wassen, M. M. L. H., & Cremers, N. A. J. (2024). Medical-Grade Honey as a Potential New Therapy for Bacterial Vaginosis. Antibiotics, 13(4), 368. https://doi.org/10.3390/antibiotics13040368