
COVID-19 and Clostridioides difficile Coinfection Analysis in the Intensive Care Unit

 ,
,  ,
,  ,
,
Abstract
1. Introduction
2. Results
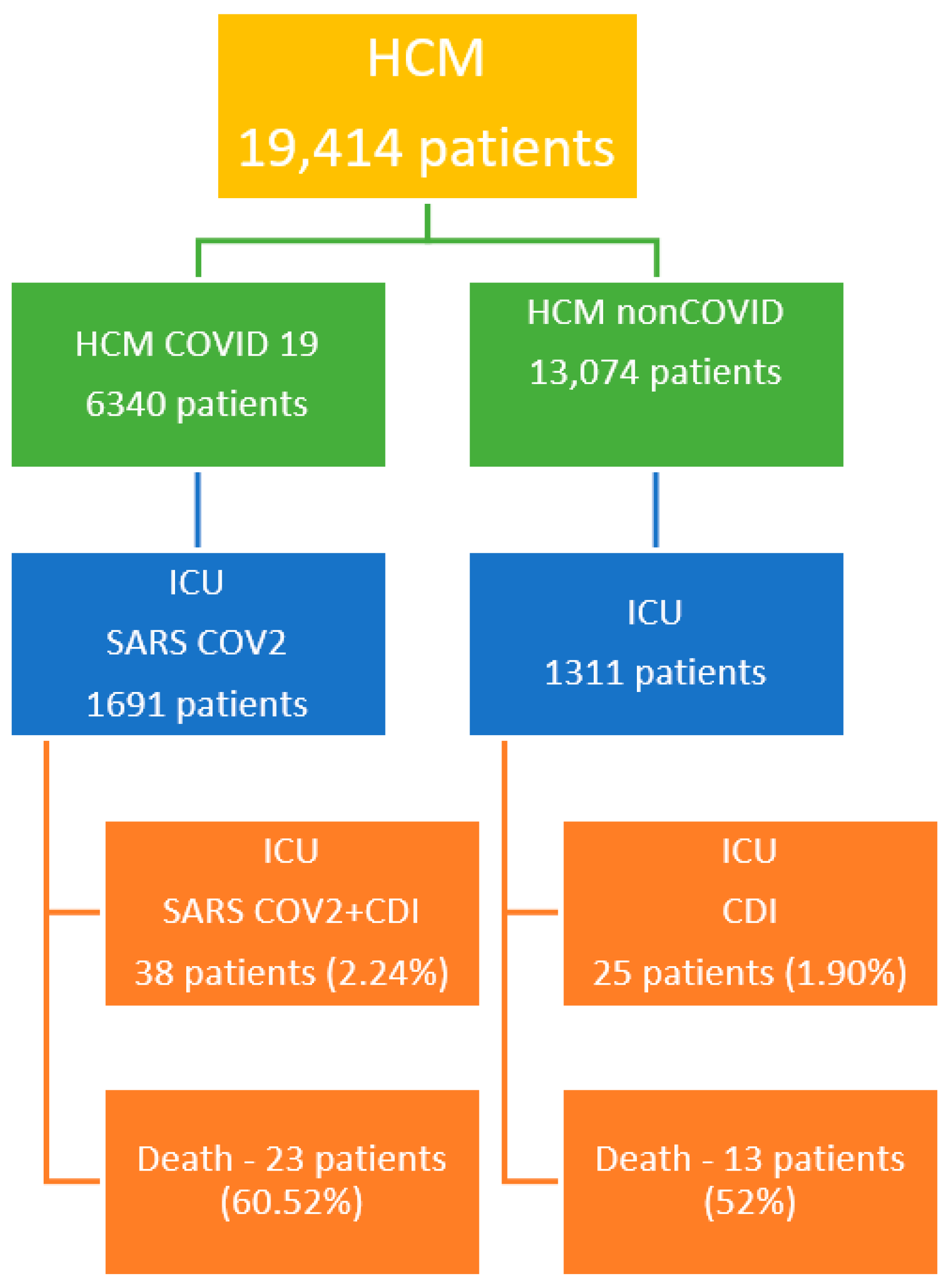
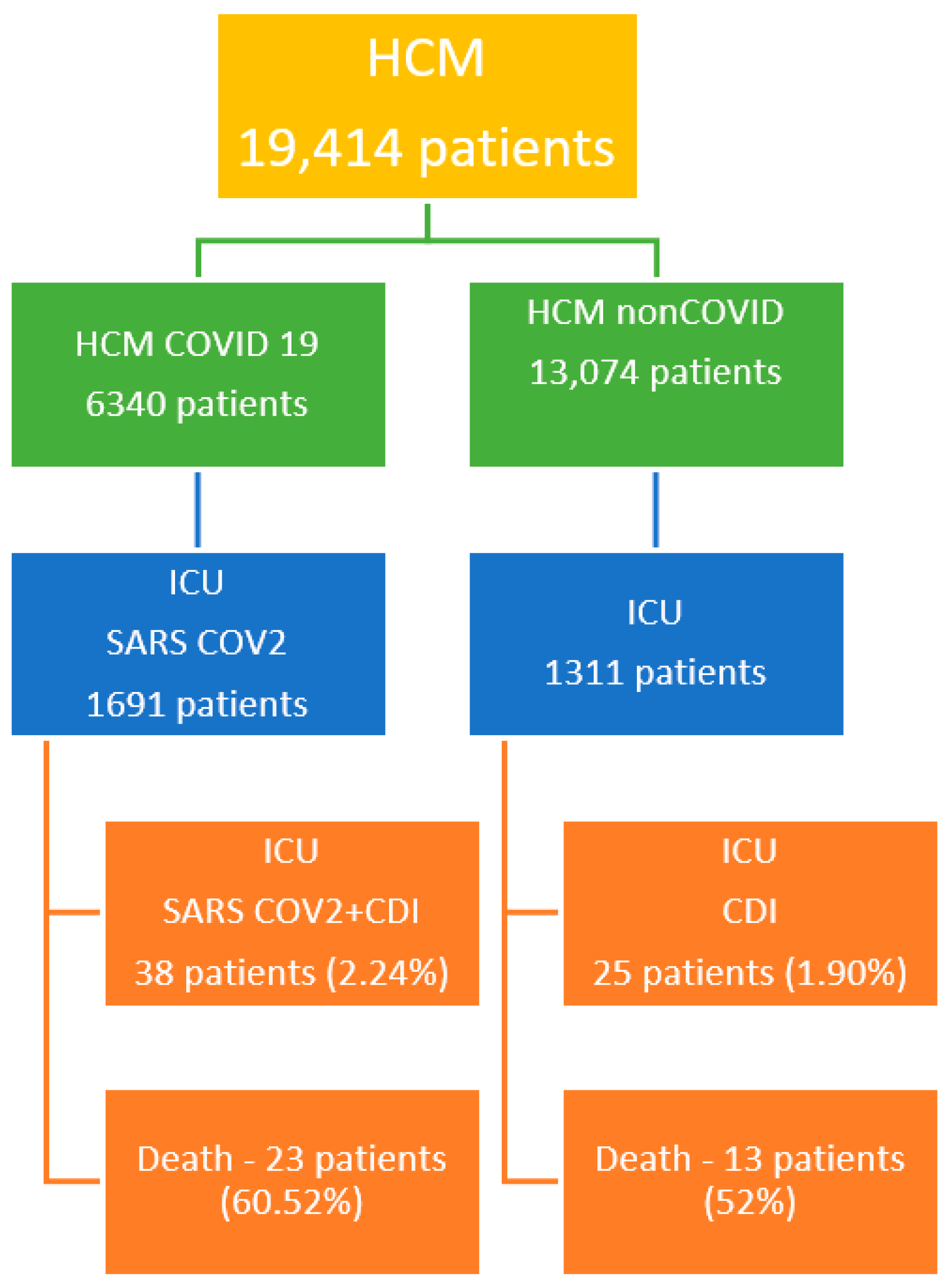
2.1. Hospital Characteristics
2.2. CDI Patient Characteristics
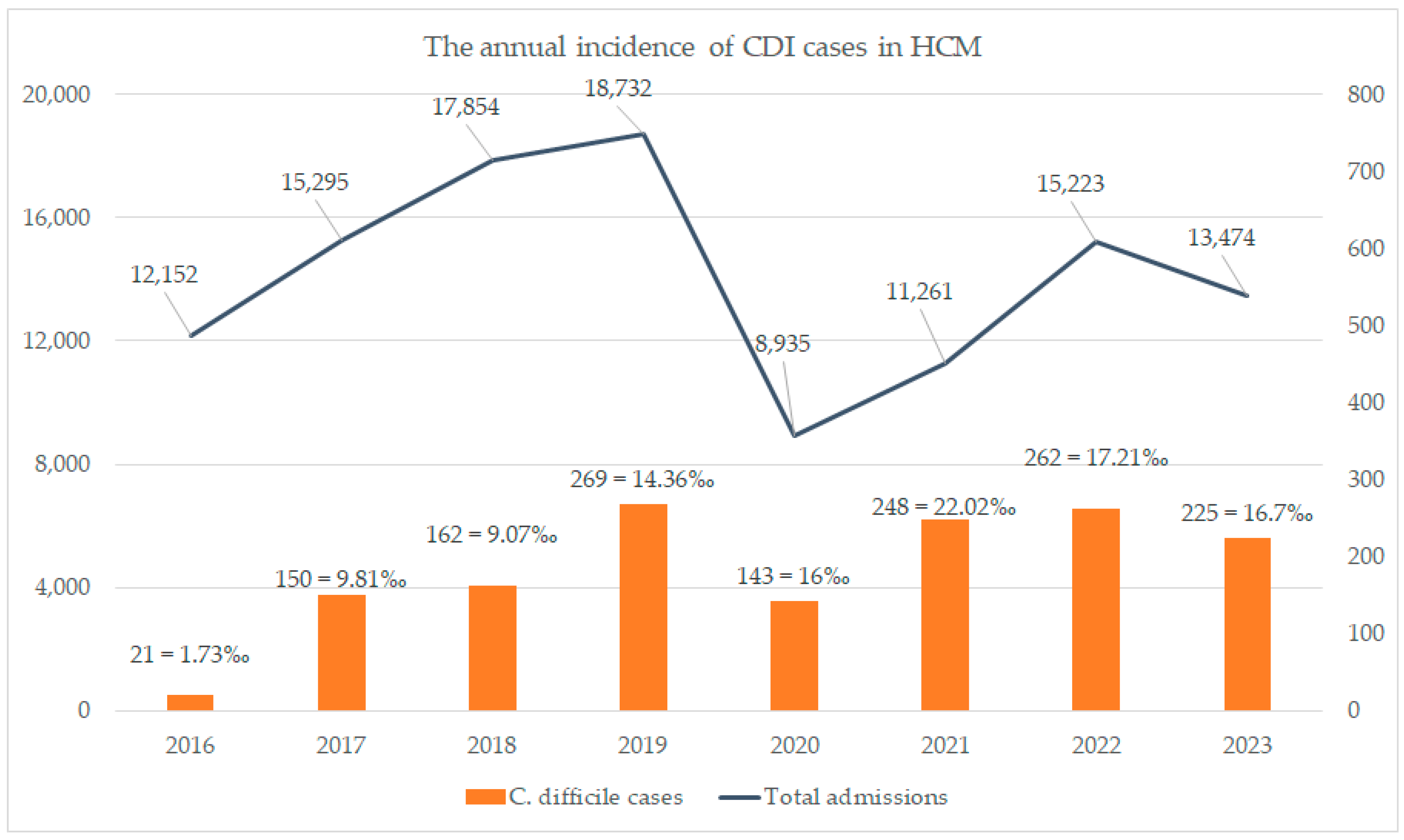
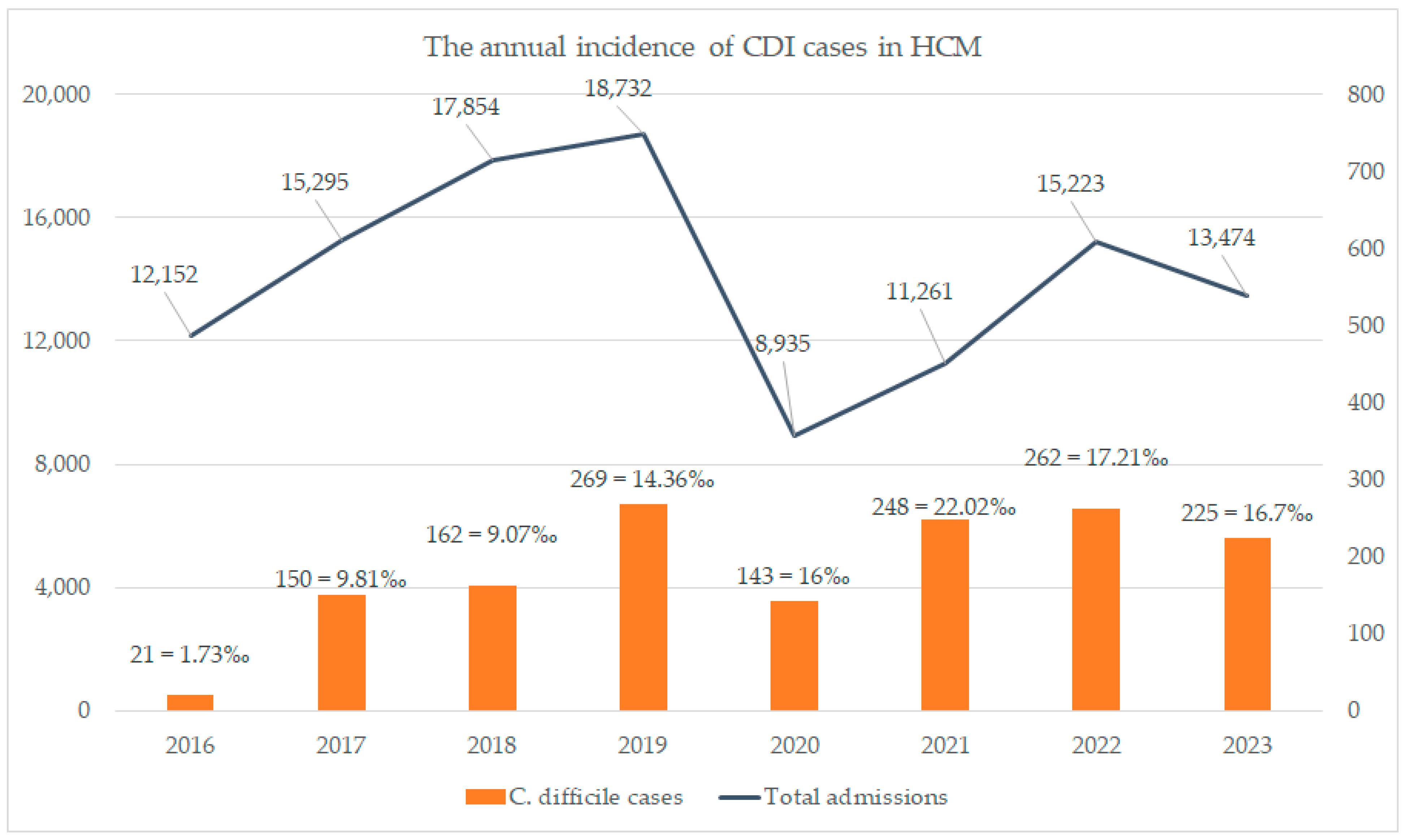
2.3. Incidence Analysis
2.4. Comorbidities Analysis
2.5. Severity Score Analysis
3. Discussion
Study Limitations
4. Materials and Methods
4.1. Data Collection and Analysis
- -
- Critical patients admitted to the ICU department;
- -
- SARS-CoV-2 infection, confirmed by RT-PCR SARS-CoV-2;
- -
- Diagnosis of CDI, confirmed by toxin A + B C. difficile.
4.2. Ethics Statement
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ALT | alanine aminotransferase |
| APACHE II | Acute Physiology and Chronic Health Evaluation II |
| AST | aspartate aminotransferase |
| CAD | coronary artery disease |
| CDI | Clostridioides Difficile Infection |
| CHF | cardiac heart failure |
| GGT | gamma-glutamyl transferase |
| HCM | Hospital County Mures |
| HTN | hypertension |
| GDH | glutamate dehydrogenase |
| ICU | intensive care units |
| LDH | lactate dehydrogenase |
| MDR | multidrug resistance |
| RT PCR SARS-CoV-2 | Real-Time Polymerase Chain Reaction SARS SARS-CoV-2 |
| PPI | proton-pump inhibitors |
| PACU | Post-Anesthesia Care Unit |
| PCR | polymerase chain reaction |
| PCT | procalcitonin |
| SOFA | Sequential Organ Failure Assessment |
| VSH (ESR) | Erythrocyte Sedimentation Rate |
References
- World Health Organization. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 19 December 2023).
- European Centre for Disease Prevention and Control. Clinical Characteristics of COVID-19. 7 September 2021. Available online: https://www.ecdc.europa.eu/en/covid-19/latest-evidence/clinical (accessed on 12 June 2023).
- Long, B.; Carius, B.M.; Chavez, S.; Liang, S.Y.; Brady, W.J.; Koyfman, A.; Gottlieb, M. Clinical update on COVID-19 for the emergency clinician: Presentation and evaluation. Am. J. Emerg. Med. 2022, 54, 46–57. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients with 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Stoian, M.; Roman, A.; Boeriu, A.; Onișor, D.; Bandila, S.R.; Babă, D.F.; Cocuz, I.; Niculescu, R.; Costan, A.; Laszlo, S.Ș.; et al. Long-Term Radiological Pulmonary Changes in Mechanically Ventilated Patients with Respiratory Failure due to SARS-CoV-2 Infection. Biomedicines 2023, 11, 2637. [Google Scholar] [CrossRef] [PubMed]
- Klok, F.A.; Kruip, M.J.H.A.; van der Meer, N.J.M.; Arbous, M.S.; Gommers, D.A.M.P.J.; Kant, K.M.; Kaptein, F.H.J.; van Paassen, J.; Stals, M.A.M.; Huisman, M.V.; et al. Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb. Res. 2020, 191, 145–147. [Google Scholar] [CrossRef]
- Xie, Y.; Xu, E.; Bowe, B.; Al-Aly, Z. Long-term cardiovascular outcomes of COVID-19. Nat. Med. 2022, 28, 583–590. [Google Scholar] [CrossRef]
- Javed, N.; Ijaz, Z.; Khair, A.H.; Dar, A.A.; Lopez, E.D.; Abbas, R.; Sheikh, A.B. COVID-19 loss of taste and smell: Potential psychological repercussions. Pan Afr. Med. J. 2022, 43, 38. [Google Scholar] [CrossRef]
- Tana, C.; Bentivegna, E.; Cho, S.-J.; Harriott, A.M.; García-Azorín, D.; Labastida-Ramirez, A.; Ornello, R.; Raffaelli, B.; Beltrán, E.R.; Ruscheweyh, R.; et al. Long COVID headache. J. Headache Pain 2022, 23, 93. [Google Scholar] [CrossRef] [PubMed]
- Korres, G.; Kitsos, D.K.; Kaski, D.; Tsogka, A.; Giannopoulos, S.; Giannopapas, V.; Sideris, G.; Tyrellis, G.; Voumvourakis, K. The Prevalence of Dizziness and Vertigo in COVID-19 Patients: A Systematic Review. Brain Sci. 2022, 12, 948. [Google Scholar] [CrossRef] [PubMed]
- Nikbakht, F.; Mohammadkhanizadeh, A.; Mohammadi, E. How does the COVID-19 cause seizure and epilepsy in patients? The potential mechanisms. Mult. Scler. Relat. Disord. 2023, 46, 102535. [Google Scholar] [CrossRef] [PubMed]
- Siow, I.; Lee, K.S.; Zhang, J.J.Y.; Saffari, S.E.; Ng, A. Encephalitis as a neurological complication of COVID-19: A systematic review and meta-analysis of incidence, outcomes, and predictors. Eur. J. Neurol. 2023, 28, 3491–3502. [Google Scholar] [CrossRef]
- Khan, F.; Sharma, P.; Pandey, S.; Sharma, D.; Vijayavarman, V.; Kumar, N.; Shukla, S.; Dandu, H.; Jain, A.; Garg, R.K.; et al. COVID-19-associated Guillain-Barre syndrome: Postinfectious alone or neuroinvasive too? J. Med. Virol. 2023, 93, 6045–6049. [Google Scholar] [CrossRef] [PubMed]
- Groff, A.; Kavanaugh, M.; Ramgobin, D.; McClafferty, B.; Aggarwal, C.S.; Golamari, R.; Jain, R. Gastrointestinal Manifestations of COVID-19: A Review of What We Know. Ochsner J. 2021, 21, 177–180. [Google Scholar] [CrossRef] [PubMed]
- Akter, S.; Tasnim, S.; Barua, R.; Choubey, M.; Arbee, S.; Mohib, M.M.; Minhaz, N.; Choudhury, A.; Sarker, P.; Mohiuddin, M.S. The Effect of COVID-19 on Gut Microbiota: Exploring the Complex Interplay and Implications for Human Health. Gastrointest. Disord. 2023, 5, 340–355. [Google Scholar] [CrossRef]
- Awan, R.U.; Gangu, K.; Nguyen, A.; Chourasia, P.; Borja Montes, O.F.; Butt, M.A.; Muzammil, T.S.; Afzal, R.M.; Nabeel, A.; Shekhar, R.; et al. COVID-19 and Clostridioides difficile Coinfection Outcomes among Hospitalized Patients in the United States: An Insight from National Inpatient Database. Infect. Dis. Rep. 2023, 15, 279–291. [Google Scholar] [CrossRef] [PubMed]
- Bentivegna, E.; Alessio, G.; Spuntarelli, V.; Luciani, M.; Santino, I.; Simmaco, M.; Martelletti, P. Impact of COVID-19 prevention measures on risk of health care-associated Clostridium difficile infection. Am. J. Infect. Control 2021, 49, 640–642. [Google Scholar] [CrossRef] [PubMed]
- Granata, G.; Petrosillo, N.; Al Moghazi, S.; Caraffa, E.; Puro, V.; Tillotson, G.; Cataldo, M.A. The burden of Clostridioides difficile infection in COVID-19 patients: A systematic review and meta-analysis. Anaerobe 2022, 74, 102484. [Google Scholar] [CrossRef] [PubMed]
- Langford, B.J.; So, M.; Raybardhan, S.; Leung, V.; Soucy, J.-P.R.; Westwood, D.; Daneman, N.; MacFadden, D.R. Antibiotic prescribing in patients with COVID-19: Rapid review and meta-analysis. Clin. Microbiol. Infect. 2021, 27, 520–531. [Google Scholar] [CrossRef] [PubMed]
- Linares-García, L.; Cárdenas-Barragán, M.E.; Hernández-Ceballos, W.; Pérez-Solano, C.S.; Morales-Guzmán, A.S.; Miller, D.S.; Schmulson, M. Bacterial and Fungal Gut Dysbiosis and Clostridium difficile in COVID-19: A Review. J. Clin. Gastroenterol. 2022, 56, 285–298. [Google Scholar] [CrossRef] [PubMed]
- Rupnik, M.; Wilcox, M.H.; Gerding, D.N. Clostridium difficile infection: New developments in epidemiology and pathogenesis. Nat. Rev. Microbiol. 2009, 7, 526–536. [Google Scholar] [CrossRef]
- Laszkowska, M.; Kim, J.; Faye, A.S.; Joelson, A.M.; Ingram, M.; Truong, H.; Silver, E.R.; May, B.; Greendyke, W.G.; Zucker, J.; et al. Prevalence of Clostridioides difficile and Other Gastrointestinal Pathogens in Patients with COVID-19. Dig. Dis. Sci. 2021, 66, 4398–4405. [Google Scholar] [CrossRef]
- Lewandowski, K.; Rosołowski, M.; Kaniewska, M.; Kucha, P.; Meler, A.; Wierzba, W.; Rydzewska, G. Clostridioides difficile infection in coronavirus disease 2019 (COVID-19): An underestimated problem? Pol. Arch. Intern. Med. 2021, 131, 121–127. [Google Scholar]
- Israel, S.; Harpaz, K.; Radvogin, E.; Schwartz, C.; Gross, I.; Mazeh, H.; Cohen, M.J.; Benenson, S. Dramatically improved hand hygiene performance rates at time of coronavirus pandemic. Clin. Microbiol. Infect. 2020, 26, 1566–1568. [Google Scholar] [CrossRef] [PubMed]
- Kakiuchi, S.; Livorsi, D.J.; Perencevich, E.N.; Diekema, D.J.; Ince, D.; Prasidthrathsint, K.; Kinn, P.; Percival, K.; Heintz, B.H.; Goto, M. Days of Antibiotic Spectrum Coverage: A Novel Metric for Inpatient Antibiotic Consumption. Clin. Infect. Dis. 2022, 75, 567–576. [Google Scholar] [CrossRef] [PubMed]
- Dieringer, T.D.; Furukawa, D.; Graber, C.J.; Stevens, V.W.; Jones, M.M.; Rubin, M.A.; Goetz, M.B. Inpatient antibiotic utilization in the Veterans’ Health Administration during the coronavirus disease 2019 (COVID-19) pandemic. Infect. Control Hosp. Epidemiol. 2021, 42, 751–753. [Google Scholar] [CrossRef] [PubMed]
- Sipos, S.; Vlad, C.; Prejbeanu, R.; Haragus, H.; Vlad, D.; Cristian, H.; Dumitrascu, C.; Popescu, R.; Dumitrascu, V.; Predescu, V. Impact of COVID-19 prevention measures on Clostridioides difficile infections in a regional acute care hospital. Exp. Ther. Med. 2021, 22, 1215. [Google Scholar] [CrossRef] [PubMed]
- Zouridis, S.; Sangha, M.; Feustel, P.; Richter, S. Clostridium difficile Infection Rates during the Pandemic in New York Capital Area: A Single-Center Study. Cureus 2023, 15, e37576. [Google Scholar] [CrossRef] [PubMed]
- Cojocariu, C.; Girleanu, I.; Trifan, A.; Olteanu, A.; Muzica, C.M.; Huiban, L.; Chiriac, S.; Singeap, A.M.; Cuciureanu, T.; Sfarti, C.; et al. Did the severe acute respiratory syndrome-coronavirus 2 pandemic cause an endemic Clostridium difficile infection? World J. Clin. Cases 2021, 9, 10180–10188. [Google Scholar] [CrossRef] [PubMed]
- Markovic-Denic, L.; Nikolic, V.; Toskovic, B.; Brankovic, M.; Crnokrak, B.; Popadic, V.; Radojevic, A.; Radovanovic, D.; Zdravkovic, M. Incidence and Risk Factors for Clostridioides difficile Infections in Non-COVID and COVID-19 Patients: Experience from a Tertiary Care Hospital. Microorganisms 2023, 11, 435. [Google Scholar] [CrossRef] [PubMed]
- Kuijper, E.J.; Coignard, B.; Tüll, P.; ESCMID Study Group for Clostridium difficile; EU Member States; European Centre for Disease Prevention and Control. Emergence of Clostridium difficile-associated disease in North America and Europe. Clin. Microbiol. Infect. 2006, 12 (Suppl. 6), 2–18. [Google Scholar] [CrossRef]
- Mu, Y.; Dudeck, M.; Jones, K.; Li, Q.; Soe, M.; Nkwata, A.; Edwards, J. Trends in Hospital Onset Clostridioides difficile Infection Incidence, National Healthcare Safety Network, 2010–2018. Infect. Control Hosp. Epidemiol. 2020, 41, S53–S54. [Google Scholar] [CrossRef]
- Boeriu, A.; Roman, A.; Dobru, D.; Stoian, M.; Voidăzan, S.; Fofiu, C. The Impact of Clostridioides Difficile Infection in Hospitalized Patients: What Changed during the Pandemic? Diagnostics 2022, 12, 3196. [Google Scholar] [CrossRef] [PubMed]
- Gavrielatou, E.; Tsimaras, M. 707. Hospital-Onset Clostridioides difficile Infection Rates during COVID-19 Pandemic in the ICU Patients. Open Forum Infect. Dis. 2021, 8 (Suppl. 1), S453. [Google Scholar] [CrossRef] [PubMed Central]
- Buetti, N.; Ruckly, S.; de Montmollin, E.; Reignier, J.; Terzi, N.; Cohen, Y.; Siami, S.; Dupuis, C.; Timsit, J.F. COVID-19 increased the risk of ICU-acquired bloodstream infections: A case-cohort study from the multicentric OUTCOMEREA network. Intensive Care Med. 2021, 47, 180–187. [Google Scholar] [CrossRef] [PubMed]
- Granata, G.; Bartoloni, A.; Codeluppi, M.; Contadini, I.; Cristini, F.; Fantoni, M.; Ferraresi, A.; Fornabaio, C.; Grasselli, S.; Lagi, F.; et al. The Burden of Clostridioides Difficile Infection during the COVID-19 Pandemic: A Retrospective Case-Control Study in Italian Hospitals (CloVid). J. Clin. Med. 2020, 9, 3855. [Google Scholar] [CrossRef]
- Allegretti, J.R.; Nije, C.; McClure, E.; Redd, W.D.; Wong, D.; Zhou, J.C.; Bazarbashi, A.N.; McCarty, T.R.; Hathorn, K.E.; Shen, L.; et al. Prevalence and Impact of Clostridioides difficile Infection among Hospitalized Patients with Coranavirus Disease 2019. JGH Open 2021, 5, 622–625. [Google Scholar] [CrossRef] [PubMed]
- Sandhu, A.; Tillotson, G.; Polistico, J.; Salimnia, H.; Cranis, M.; Moshos, J.; Cullen, L.; Jabbo, L.; Diebel, L.; Chopra, T. Clostridioides Difficile in COVID-19 Patients, Detroit, Michigan, USA, March–April 2020. Emerg. Infect. Dis. 2020, 26, 2272–2274. [Google Scholar] [CrossRef] [PubMed]
- van Rossen, T.M.; Ooijevaar, R.E.; Vandenbroucke-Grauls, C.M.J.E.; Dekkers, O.M.; Kuijper, E.J.; Keller, J.J.; van Prehn, J. Prognostic factors for severe and recurrent Clostridioides difficile infection: A systematic review. Clin. Microbiol. Infect. 2022, 28, 321–331. [Google Scholar] [CrossRef] [PubMed]
- Despotović, A.; Barać, A.; Cucanić, T.; Cucanić, K.; Stevanović, G. Antibiotic (Mis)Use in COVID-19 Patients before and after Admission to a Tertiary Hospital in Serbia. Antibiotics 2022, 11, 847. [Google Scholar] [CrossRef]
- Lima-Martínez, M.M.; Carrera Boada, C.; Madera-Silva, M.D.; Marín, W.; Contreras, M. COVID-19 and diabetes: A bidirectional relationship. Clínica Investig. Arterioscler. (Engl. Ed.) 2021, 33, 151–157. [Google Scholar] [CrossRef]
- Marjot, T.; Webb, G.J.; Barritt, A.S.; Moon, A.M.; Stamataki, Z.; Wong, V.W.; Barnes, E. COVID-19 and liver disease: Mechanistic and clinical perspectives. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 348–364. [Google Scholar] [CrossRef]
- Zuin, M.; Rigatelli, G.; Bilato, C.; Rigatelli, A.; Roncon, L.; Ribichini, F. Preexisting coronary artery disease among coronavirus disease 2019 patients: A systematic review and meta-analysis. J. Cardiovasc. Med. 2022, 23, 535–545. [Google Scholar] [CrossRef] [PubMed]
- Micek, S.T.; Schramm, G.; Morrow, L.; Frazee, E.; Personett, H.; Doherty, J.A.; Hampton, N.; Hoban, A.; Lieu, A.; McKenzie, M.; et al. Clostridium difficile infection: A multicenter study of epidemiology and outcomes in mechanically ventilated patients. Crit. Care Med. 2013, 41, 1968–1975. [Google Scholar] [CrossRef] [PubMed]
- Qu, H.Q.; Jiang, Z.D. Clostridium difficile infection in diabetes. Diabetes Res. Clin. Pract. 2014, 105, 285–294. [Google Scholar] [CrossRef] [PubMed]
- Slavcovici, A.; Streinu-Cercel, A.; Ţăţulescu, D.; Radulescu, A.; Mera, S.; Marcu, C.; Vesbianu, D.; Topan, A. The role of risk factors ‘carmeli score’ and infective endocarditis classification in the assessment of appropriate empirical therapy. Ther. Pharmacol. Clin. Toxicol. 2009, XIII, 52–56. [Google Scholar]
- Ghoshal, U.C.; Ghosal, U.; Mathur, A.; Singh, R.; Nath, A.; Garg, A.; Singh, D.; Singh, S.; Singh, J.; Pandey, A.; et al. The spectrum of gastrointestinal symptoms in patients with coronavirus disease-19: Predictors, relationship with disease severity, and outcome. Clin. Transl. Gastroenterol. 2020, 11, e00259. [Google Scholar] [CrossRef] [PubMed]
- Yibirin, M.; De Oliveira, D.; Valera, R.; Plitt, A.E.; Lutgen, S. Adverse effects associated with proton pump inhibitor use. Cureus 2021, 13, e12759. [Google Scholar] [CrossRef] [PubMed]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef] [PubMed]
- Moisa, E.; Corneci, D.; Negutu, M.I.; Filimon, C.R.; Serbu, A.; Popescu, M.; Negoita, S.; Grintescu, I.M. Development and Internal Validation of a New Prognostic Model Powered to Predict 28-Day All-Cause Mortality in ICU COVID-19 Patients-The COVID-SOFA Score. J. Clin. Med. 2022, 11, 4160. [Google Scholar] [CrossRef]
- Stoian, A.; Bajko, Z.; Maier, S.; Cioflinc, R.A.; Grigorescu, B.; Moțățăianu, A.; Bărcuțean, L.; Balașa, R.; Stoian, M. High-dose intravenous immunoglobulins as a therapeutic option in critical illness polyneuropathy accompanying SARS-CoV-2 infection: A case-based review of the literature (Review). Exp. Ther. Med. 2021, 22, 1182. [Google Scholar] [CrossRef]
- Stoian, A.; Bajko, Z.; Stoian, M.; Cioflinc, R.A.; Niculescu, R.; Arbănași, E.M.; Russu, E.; Botoncea, M.; Bălașa, R. The Occurrence of Acute Disseminated Encephalomyelitis in SARS-CoV-2 Infection/Vaccination: Our Experience and a Systematic Review of the Literature. Vaccines 2023, 11, 1225. [Google Scholar] [CrossRef]
- Marinescu, A.R.; Laza, R.; Musta, V.F.; Cut, T.G.; Dumache, R.; Tudor, A.; Porosnicu, M.; Lazureanu, V.E.; Licker, M. Clostridium Difficile and COVID-19: General Data, Ribotype, Clinical Form, Treatment-Our Experience from the Largest Infectious Diseases Hospital in Western Romania. Medicina 2021, 57, 1099. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Group | Admission | Discharge | Unpaired t-Test p | |
|---|---|---|---|---|
| CRP (mg/dL) | 1 | 36.32 ± 49.6 | 10.50 ± 11.80 | 0.731 |
| 2 | 41.83 ± 72.76 | 12.95 ± 15.90 | 0.507 | |
| Fibrinogen (mg/dL) | 1 | 475.88 ± 214.02 | 426.06 ± 187.94 | 0.374 |
| 2 | 428.28 ± 184.23 | 439.59 ± 160.63 | 0.773 | |
| Ferritin (ng/mL) | 1 | 1332.99 ± 901.43 | 2008.032 ± 2320.15 | 0.139 |
| 2 | 838.05 ± 1176.75 | 724.33 ± 1120.29 | 0.07 | |
| LDH (U/L) | 1 | 480.49 ± 231.26 | 510.43 ± 342.53 | 0.02 |
| 2 | 319.00 ± 289.69 | 249.30 ± 101.82 | 0.002 | |
| Leucocytes (/mm3) | 1 | 10.25 ± 5.06 | 16.51 ± 8.48 | 0.01 |
| 2 | 13.67 ± 5.83 | 12.40 ± 5.66 | 0.04 | |
| AST (U/L) | 1 | 57.89 ± 62.36 | 104.73 ± 268.58 | 0.08 |
| 2 | 33.88 ± 28.20 | 34.46 ± 30.62 | 0.20 | |
| ALT (U/L) | 1 | 74.43 ± 90.98 | 128.70 ± 235.63 | 0.05 |
| 2 | 35.83 ± 30.47 | 32.17 ± 25.25 | 0.05 | |
| Creatinine (mg/dL) | 1 | 1.07 ± 0.58 | 1.34 ± 1.28 | 0.001 |
| 2 | 2.65 ± 2.73 | 1.95 ± 2.18 | 0.17 | |
| Urea (mg/dL) | 1 | 70.52 ± 37.85 | 111.38 ± 93.41 | 0.06 |
| 2 | 94.15 ± 60.59 | 83.90 ± 59.43 | 0.20 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stoian, M.; Andone, A.; Boeriu, A.; Bândilă, S.R.; Dobru, D.; Laszlo, S.Ș.; Corău, D.; Arbănași, E.M.; Russu, E.; Stoian, A. COVID-19 and Clostridioides difficile Coinfection Analysis in the Intensive Care Unit. Antibiotics 2024, 13, 367. https://doi.org/10.3390/antibiotics13040367
Stoian M, Andone A, Boeriu A, Bândilă SR, Dobru D, Laszlo SȘ, Corău D, Arbănași EM, Russu E, Stoian A. COVID-19 and Clostridioides difficile Coinfection Analysis in the Intensive Care Unit. Antibiotics. 2024; 13(4):367. https://doi.org/10.3390/antibiotics13040367
Chicago/Turabian StyleStoian, Mircea, Adina Andone, Alina Boeriu, Sergio Rareș Bândilă, Daniela Dobru, Sergiu Ștefan Laszlo, Dragoș Corău, Emil Marian Arbănași, Eliza Russu, and Adina Stoian. 2024. "COVID-19 and Clostridioides difficile Coinfection Analysis in the Intensive Care Unit" Antibiotics 13, no. 4: 367. https://doi.org/10.3390/antibiotics13040367
APA StyleStoian, M., Andone, A., Boeriu, A., Bândilă, S. R., Dobru, D., Laszlo, S. Ș., Corău, D., Arbănași, E. M., Russu, E., & Stoian, A. (2024). COVID-19 and Clostridioides difficile Coinfection Analysis in the Intensive Care Unit. Antibiotics, 13(4), 367. https://doi.org/10.3390/antibiotics13040367