
Effect of Inappropriate Treatment in Hospitalized Patients with Pyelonephritis Treated with Cefuroxime: A Cohort Study


Abstract
1. Introduction
2. Results
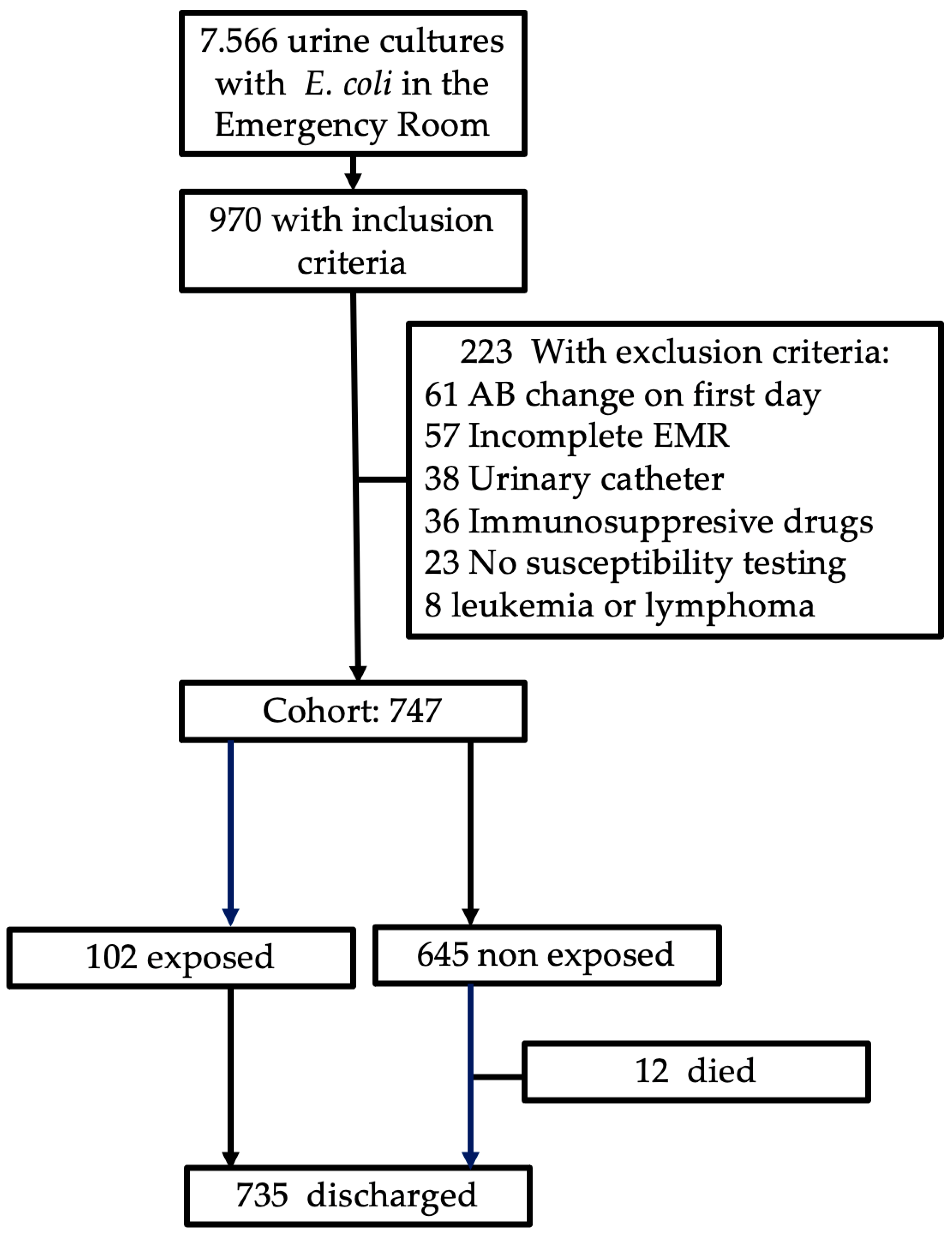
2.1. Patient Characteristics at Admission
2.2. Treatment and Outcomes
2.3. Associations between Inappropriate Therapy and Length of Stay and Readmission
3. Discussion
4. Materials and Methods
4.1. Data and Subjects
4.2. Exposure
4.3. Outcomes
4.4. Covariates
4.5. Statistical Analysis
4.6. Sensitivity Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Strassle, P.D.; Sickbert-Bennett, E.E.; Klompas, M.; Lund, J.L.; Stewart, P.W.; Marx, A.H.; DiBiase, L.M.; Weber, D.J. Incidence and risk factors of non-device-associated urinary tract infections in an acute-care hospital. Infect. Control Hosp. Epidemiol. 2019, 40, 1242–1247. [Google Scholar] [CrossRef] [PubMed]
- Carreno, J.J.; Tam, I.M.; Meyers, J.L.; Esterberg, E.; Candrilli, S.D.; Lodise, T.P., Jr. Longitudinal, Nationwide, Cohort Study to Assess Incidence, Outcomes, and Costs Associated with Complicated Urinary Tract Infection. Open Forum Infect. Dis. 2020, 7, ofz536. [Google Scholar] [CrossRef] [PubMed]
- Zilberberg, M.D.; Nathanson, B.H.; Sulham, K.; Shorr, A.F. Multiple antimicrobial resistance and outcomes among hospitalized patients with complicated urinary tract infections in the US, 2013–2018: A retrospective cohort study. BMC Infect. Dis. 2021, 21, 159. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, K.; Yamamoto, S.; Takahashi, S.; Ishikawa, K.; Yasuda, M.; Wada, K.; Hamasuna, R.; Hayami, H.; Minamitani, S.; Matsumoto, T.; et al. The third national Japanese antimicrobial susceptibility pattern surveillance program: Bacterial isolates from complicated urinary tract infection patients. J. Infect. Chemother. 2020, 26, 418–428. [Google Scholar] [CrossRef] [PubMed]
- Brown, P.; Ki, M.; Foxman, B. Acute pyelonephritis among adults: Cost of illness and considerations for the economic evaluation of therapy. Pharmacoeconomics 2005, 23, 1123–1142. [Google Scholar] [CrossRef] [PubMed]
- Sako, A.; Yasunaga, H.; Matsui, H.; Fushimi, K.; Yanai, H.; Gu, Y.; Ohmagari, N. Hospitalization for urinary tract infections in Japan, 2010–2015: A retrospective study using a national inpatient database. BMC Infect. Dis. 2021, 21, 1048. [Google Scholar] [CrossRef] [PubMed]
- Leal, A.L.; Cortes, J.A.; Arias, G.; Ovalle, M.V.; Saavedra, S.Y.; Buitrago, G.; Escobar, J.A.; Castro, B.E.; GREBO. Emergence of resistance to third generation cephalosporins by Enterobacteriaceae causing community-onset urinary tract infections in hospitals in Colombia. Enferm. Infecc. Microbiol. Clin. 2013, 31, 298–303. [Google Scholar] [CrossRef]
- Eliakim-Raz, N.; Babitch, T.; Shaw, E.; Addy, I.; Wiegand, I.; Vank, C.; Torre-Vallejo, L.; Joan-Miquel, V.; Steve, M.; Grier, S.; et al. Risk Factors for Treatment Failure and Mortality among Hospitalized Patients with Complicated Urinary Tract Infection: A Multicenter Retrospective Cohort Study (RESCUING Study Group). Clin. Infect. Dis. 2019, 68, 29–36. [Google Scholar] [CrossRef]
- Kadry, N.; Natarajan, M.; Bein, E.; Kim, P.; Farley, J. Discordant Clinical and Microbiological Outcomes Are Associated With Late Clinical Relapse in Clinical Trials for Complicated Urinary Tract Infections. Clin. Infect. Dis. 2023, 76, 1768–1775. [Google Scholar] [CrossRef]
- Wiggers, J.B.; Sehgal, P.; Pinto, R.; MacFadden, D.; Daneman, N. The association of adequate empirical treatment and time to recovery from bacteraemic urinary tract infections: A retrospective cohort study. Clin. Microbiol. Infect. 2019, 25, 1253–1258. [Google Scholar] [CrossRef]
- Park, S.H.; Choi, S.M.; Chang, Y.K.; Lee, D.G.; Cho, S.Y.; Lee, H.J.; Choi, J.H.; Yoo, J.H. The efficacy of non-carbapenem antibiotics for the treatment of community-onset acute pyelonephritis due to extended-spectrum beta-lactamase-producing Escherichia coli. J. Antimicrob. Chemother. 2014, 69, 2848–2856. [Google Scholar] [CrossRef]
- Anderson, D.T.; Albrecht, B.; Jones, K.A.; Jacob, J.T.; Sexton, M.E.; Wiley, Z.; Dube, W.C.; Lee, B.; Suchindran, S. Efficacy of Noncarbapenem beta-Lactams Compared to Carbapenems for Extended-Spectrum beta-Lactamase-Producing Enterobacterales Urinary Tract Infections. Open Forum Infect. Dis. 2022, 9, ofac034. [Google Scholar] [CrossRef]
- Lee, S.S.; Kim, Y.; Chung, D.R. Impact of discordant empirical therapy on outcome of community-acquired bacteremic acute pyelonephritis. J. Infect. 2011, 62, 159–164. [Google Scholar] [CrossRef]
- Benavides, T.M.; Aden, J.K.; Giancola, S.E. Evaluating outcomes associated with revised fluoroquinolone breakpoints for Enterobacterales urinary tract infections: A retrospective cohort study. Eur. J. Clin. Microbiol. Infect. Dis. 2022, 41, 741–749. [Google Scholar] [CrossRef]
- Vree, T.B.; Hekster, Y.A. Pharmacokinetics and tissue concentrations of cefuroxime. Pharm. Weekbl. Sci. 1990, 12, 262–266. [Google Scholar] [CrossRef] [PubMed]
- Bundtzen, R.W.; Toothaker, R.D.; Nielson, O.S.; Madsen, P.O.; Welling, P.G.; Craig, W.A. Pharmacokinetics of cefuroxime in normal and impaired renal function: Comparison of high-pressure liquid chromatography and microbiological assays. Antimicrob. Agents Chemother. 1981, 19, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Broekhuysen, J.; Deger, F.; Douchamps, J.; Freschi, E.; Mal, N.; Neve, P.; Parfait, R.; Siska, G.; Winand, M. Pharmacokinetic study of cefuroxime in the elderly. Br. J. Clin. Pharmacol. 1981, 12, 801–805. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Efstathiou, S.P.; Pefanis, A.V.; Tsioulos, D.I.; Zacharos, I.D.; Tsiakou, A.G.; Mitromaras, A.G.; Mastorantonakis, S.E.; Kanavaki, S.N.; Mountokalakis, T.D. Acute pyelonephritis in adults: Prediction of mortality and failure of treatment. Arch. Intern. Med. 2003, 163, 1206–1212. [Google Scholar] [CrossRef] [PubMed]
- Bianchini, M.L.; Kenney, R.M.; Lentz, R.; Zervos, M.; Malhotra, M.; Davis, S.L. Discharge Delays and Costs Associated with Outpatient Parenteral Antimicrobial Therapy for High-Priced Antibiotics. Clin. Infect. Dis. 2020, 71, e88–e93. [Google Scholar] [CrossRef] [PubMed]
- Chattopadhyay, A.; Hase, C.H.; Zubizarreta, J.R. Balancing vs. modeling approaches to weighting in practice. Stat. Med. 2020, 39, 3227–3254. [Google Scholar] [CrossRef] [PubMed]
- Brookhart, M.A.; Wyss, R.; Layton, J.B.; Sturmer, T. Propensity score methods for confounding control in nonexperimental research. Circ. Cardiovasc. Qual. Outcomes 2013, 6, 604–611. [Google Scholar] [CrossRef]
- Clnical Laboraotry Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing; Twentieth Informational Supplement; Clnical Laboraotry Standards Institute: Wayne, PA, USA, 2010; Volume 30. [Google Scholar]
- Rodríguez-Baño, J.; Pascual, A. Risk factors for community-acquired infections caused by extended-spectrum β-lactamase-producing Escherichia coli. Arch. Intern. Med. 2009, 169, 811–812. [Google Scholar]
- Azap, Ö.K.; Arslan, H.; Şerefhanoĝlu, K.; Çolakoĝlu, Ş.; Erdoĝan, H.; Timurkaynak, F.; Senger, S.S. Risk factors for extended-spectrum β-lactamase positivity in uropathogenic Escherichia coli isolated from community-acquired urinary tract infections. Clin. Microbiol. Infect. 2010, 16, 147–151. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.S.; Lee, C.B.; Lee, S.J. Prevalence and risk factors for extended spectrum beta-lactamase-producing uropathogens in patients with urinary tract infection. Korean J. Urol. 2010, 51, 492–497. [Google Scholar] [CrossRef] [PubMed]
- Pineda-Posada, M.; Arias, G.; Suárez-Obando, F.; Bastidas, A.; Avila-Cortés, Y. Risk factors for the development of community-acquired urinary tract infection, by extended-spectrum beta-lactamase producing microorganisms, at two hospitals in Bogotá, Colombia. Infectio 2017, 21, 141–147. [Google Scholar]
- Benedetto, U.; Head, S.J.; Angelini, G.D.; Blackstone, E.H. Statistical primer: Propensity score matching and its alternatives. Eur. J. Cardiothorac. Surg. 2018, 53, 1112–1117. [Google Scholar] [CrossRef]
- Austin, P.C.; Stuart, E.A. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat. Med. 2015, 34, 3661–3679. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Original Sample (N = 747) | After IPTW | |||||
|---|---|---|---|---|---|---|
| Inappropriate (N = 102) | Appropriate (N = 645) | SMD | Inappropriate | Appropriate | SMD | |
| Age, years, mean (SD) | 68.7 (15.3) | 63.0 (19.8) | 0.318 | 63.3 (20.3) | 63.8 (19.3) | 0.028 |
| Female, n (%) | 58 (56.9) | 444 (68.8) | 0.250 | 71 (68.4) | 434 (67.2) | 0.025 |
| Menopause, n (%) | 53 (51.9) | 317 (49.1) | 0.531 | 53 (51.8) | 320 (49.5) | 0.021 |
| Any comorbidity, n (%) | 55 (53.9) | 361 (56.0) | 0.041 | 58 (55.8) | 359 (55.7) | 0.002 |
| Charlson Comorbidity Index score, mean (SD) | 3.6 (1.8) | 3.9 (1.7) | 0.190 | 3.9 (1.7) | 3.9 (1.7) | 0.002 |
| Diabetes, n (%) | 22 (21.6) | 116 (18.0) | 0.090 | 21 (20.1) | 120 (18.5) | 0.040 |
| Solid tumor or autoimmune disease, n (%) | 17 (16.7) | 83 (12.9) | 0.107 | 12 (11.8) | 86 (13.3) | 0.048 |
| Urolithiasis, n (%) | 12 (11.8) | 81 (12.6) | 0.037 | 11 (10.8) | 80 (12.3) | 0.048 |
| Chronic pulmonary diseases, n (%) | 9 (8.8) | 51 (7.9) | 0.033 | 11 (10.3) | 49 (7.6) | 0.093 |
| Heart failure, n (%) | 7 (6.9) | 23 (3.6) | 0.192 | 4 (3.9) | 26 (4.1) | 0.010 |
| Antibiotic use | ||||||
| Previous antibiotic use, n (%) | 19 (18.6) | 122 (18.9) | 0.007 | 17 (16.4) | 123 (19.0) | 0.068 |
| Previous cephalosporin use, n (%) | 7 (6.9) | 37 (5.7) | 0.046 | 6 (5.6) | 38 (5.8) | 0.011 |
| Previous quinolone use, n (%) | 6 (5.9) | 22 (3.4) | 0.118 | 4 (4.3) | 23 (3.5) | 0.04 |
| Clinical and laboratory data | ||||||
| SIRS *, n (%) | 59 (57.8) | 382 (59.2) | 0.028 | 58 (56.4) | 381 (59.1) | 0.055 |
| Creatinine mg/dL, mean (SD), n = 730 | 1.16 (0.48) | 1.10 (0.56) | 0.116 | 1.09 (0.43) | 1.11 (0.57) | 0.038 |
| Variable | HR * | 95% CI |
|---|---|---|
| Inappropriate therapy | 0.34 | 0.23–0.49 |
| Oral treatment at discharge | 0.22 | 0.16–0.30 |
| Antimicrobial regimen change | 1.86 | 1.30–2.65 |
| ICU admission | 2.63 | 1.83–3.76 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cortés, J.A.; Sierra, C.R.; Sánchez, R. Effect of Inappropriate Treatment in Hospitalized Patients with Pyelonephritis Treated with Cefuroxime: A Cohort Study. Antibiotics 2024, 13, 274. https://doi.org/10.3390/antibiotics13030274
Cortés JA, Sierra CR, Sánchez R. Effect of Inappropriate Treatment in Hospitalized Patients with Pyelonephritis Treated with Cefuroxime: A Cohort Study. Antibiotics. 2024; 13(3):274. https://doi.org/10.3390/antibiotics13030274
Chicago/Turabian StyleCortés, Jorge Alberto, Claudia Rocío Sierra, and Ricardo Sánchez. 2024. "Effect of Inappropriate Treatment in Hospitalized Patients with Pyelonephritis Treated with Cefuroxime: A Cohort Study" Antibiotics 13, no. 3: 274. https://doi.org/10.3390/antibiotics13030274
APA StyleCortés, J. A., Sierra, C. R., & Sánchez, R. (2024). Effect of Inappropriate Treatment in Hospitalized Patients with Pyelonephritis Treated with Cefuroxime: A Cohort Study. Antibiotics, 13(3), 274. https://doi.org/10.3390/antibiotics13030274