1. Introduction
Preterm birth, defined as delivery before 37 weeks of gestation, remains a significant public health challenge globally, as approximately 15 million babies are born preterm every year, with an average of 10% of all live births, depending on regional development [
1,
2]. It is a leading cause of neonatal mortality and long-term morbidity, with profound implications for families and healthcare systems [
3,
4]. Various risk factors have been identified in the etiology of preterm birth, including demographic, genetic, environmental, and, particularly, infectious contributors [
5,
6,
7,
8,
9,
10,
11]. Among these, genital infections in pregnant women are recognized as critical factors that can disrupt the normal course of gestation and precipitate early labor [
12,
13].
Genital infections, encompassing a range of bacterial, viral, and fungal pathogens, can ascend from the lower genital tract to affect the uterus, amniotic fluid, and fetus [
8,
9]. The inflammatory response triggered by these infections, as well as systemic inflammation are well-documented causes of preterm labor [
14,
15]. Bacteria such as Group B
Streptococcus,
Trichomonas vaginalis, and bacterial vaginosis-associated organisms are frequently implicated by inducing the release of pro-inflammatory cytokines, prostaglandins, and other mediators that lead to cervical ripening, uterine contractions, and eventual premature rupture of membranes [
16,
17,
18,
19,
20,
21,
22].
However, the management of these infections during pregnancy is complicated by the need to consider both maternal and fetal safety. Antibiotics are the primary line of defense against bacterial genital infections, but their use during pregnancy is a delicate balance between eradicating the infection and preserving the health of both mother and fetus [
23,
24]. The choice of antibiotic, timing, and duration of treatment are critical factors that need careful consideration. Moreover, the emergence of antibiotic-resistant pathogens adds another layer of complexity to the management of these infections [
25,
26,
27,
28].
Despite the known association between genital infections and preterm birth, there are gaps in our understanding of the mechanistic pathways and the effectiveness of different antibiotic treatments in preventing preterm birth. Additionally, there is a need to understand the role of antibiotic stewardship in this context to prevent the overuse of antibiotics and the subsequent rise in resistant pathogens [
29,
30,
31,
32]. These gaps underscore the importance of continued research in this area to develop targeted strategies for the prevention and management of genital infections in pregnant women.
Considering the above, this study aims to explore the multifaceted relationship among genital infections, antibiotic use, and preterm birth. We hypothesize that certain genital infections significantly increase the risk of preterm birth, and that appropriate and timely antibiotic treatment can mitigate this risk. The objectives include identifying the most common genital pathogens implicated in preterm births, assessing the impact of different antibiotic therapies on pregnancy outcomes, and understanding the patterns of antibiotic resistance among these pathogens.
2. Results
In the current study, a total of 71 pregnant women were selected based on their status of genital infections during pregnancy and the preterm birth outcome, and another group of 94 pregnant women with genital infections who gave birth at term were also included. The mean age of women who gave birth preterm was 27.3 years, ranging from 18 to 40 years, while the mean age for the group of full-term births was slightly higher (28.1 years). However, this difference was not statistically significant (p = 0.341). Similarly, the distribution of age categories, with 62.0% of births occurring in women under 35 years in the preterm group and 54.3% in the full-term group, did not show a significant difference (p = 0.320).
In the preterm group, obesity was found in 16.9% of individuals, and this was slightly higher in the full-term group (19.1%), although this difference was not statistically meaningful (p = 0.710). Smoking during pregnancy occurred more frequently in the preterm group, 18.3%, compared with the full-term group, 11.7% (p = 0.233). Additionally, alcohol consumption during pregnancy was nearly the same between the preterm (11.3%) and full-term (10.6%) groups, with no statistically significant difference noted (p = 0.897). Regarding parity, the proportion of primigravida was slightly lower in the preterm group (53.5%) compared with the full-term group (57.4%). The proportion of multigravida women was correspondingly higher in the preterm group (46.5%) compared with the full-term group (42.6%), but these differences were not statistically significant (p = 0.615).
In the medical history of the participants, this study found a significantly higher prevalence of sexually transmitted diseases (STDs) in the preterm group (25.4%) compared with the full-term group (3.2%), which was statistically significant (
p < 0.001). Genital herpes also showed a higher prevalence in the preterm group (8.5%) compared with the full-term group (1.1%), a difference that was statistically significant (
p = 0.019), as presented in
Table 1. However, no significant differences were observed in the prevalence of other conditions, such as urinary tract infections (UTIs), hypertension, diabetes, anemia, respiratory infections during pregnancy, and diarrheal illnesses.
The prevalence of fever was notably higher in the preterm group, with 81.7% of women experiencing fever compared with only 25.5% in the full-term group, a difference that was statistically significant (p < 0.001). Pelvic pain was also more common in the preterm group, affecting 50.7% of the women, as opposed to 21.3% in the full-term group, another statistically significant finding (p < 0.001). Other symptoms, such as foul-smelling vaginal discharge, genital itching, and urinary frequency, though more prevalent in the preterm group, did not show statistically significant differences. The prevalence rates of foul-smelling vaginal discharge were 45.1% in the preterm group and 37.2% in the full-term group (p = 0.310), genital itching was reported by 66.2% of the preterm group compared with 55.3% of the full-term group (p = 0.158), and urinary frequency was observed in 26.8% of the preterm group against 36.2% in the full-term group (p = 0.199).
Vaginal spotting was another symptom that showed a statistically significant difference, with 40.8% of the preterm group experiencing it against 24.5% of the full-term group (
p = 0.024). However, symptoms like dyspareunia, nausea, headache, dizziness, and muscle cramps, though varied in prevalence between the two groups, did not reach statistical significance. Fatigue was significantly more prevalent in the preterm group, affecting 59.2% of the women, compared with 36.2% in the full-term group, a difference that was statistically significant (
p = 0.003), as described in
Table 2.
A key finding was the statistically significant difference in gestational weight between the two groups (p = 0.010). In the preterm group, infants with a gestational weight of 500–999 g and 1000–1499 g were represented by 2.8% and 8.5% respectively, whereas there were no infants in these weight categories in the full-term group. For infants weighing between 1500 and 2499 g, the prevalence was relatively similar in both groups (21.1% in the preterm group and 22.3% in the full-term group). Notably, a higher proportion of infants in the full-term group (77.7%) had a gestational weight of over 2500 g compared with the preterm group (67.6%).
This study also delved into gestational age categories, highlighting a stark contrast between preterm and full-term deliveries. Early preterm births (<28 weeks) constituted 11.3% of the preterm group, with no occurrences in the full-term group. Similarly, moderate preterm (28–32 weeks) and later preterm (32–36 weeks) births were exclusively observed in the preterm group, accounting for 46.5% and 42.3%, respectively. In contrast, early term (37–38 weeks) births occurred only in the full-term group (21.3%), as did full-term (38–42 weeks) and post-term (>42 weeks) births, constituting 70.2% and 8.5% of the full-term group, respectively.
Regarding the type of birth, a significant difference was observed (
p < 0.001). Vaginal births were more common in the full-term group (73.4%) compared with the preterm group (39.4%). Cesarean births were more prevalent in the preterm group (56.3%) than in the full-term group (20.2%). The rate of assisted births was similar in both groups, with 4.2% in the preterm group and 6.4% in the full-term group (
Table 3).
A key observation was the significant difference in vaginal pH levels between the two groups. The average pH level in the preterm group was 5.5, notably higher than the 4.5 observed in the full-term group, with this difference reaching statistical significance (p = 0.001). This study also evaluated the vaginal flora based on Nugent scores, finding significant differences in the prevalence of various flora types. The proportion of women with normal flora (Nugent scores of 0–3) was significantly lower in the preterm group (16.9%) compared with the full-term group (41.5%) (p = 0.003). Conversely, intermediate flora (Nugent scores of 4–6) was more common in the preterm group (49.3%) than in the full-term group (38.3%). Notably, the prevalence of bacterial vaginosis (Nugent scores of 7–10) was significantly higher in the preterm group (33.8%) compared with the full-term group (20.2%).
Regarding the findings from Gram staining, there was a significant decrease in the presence of
Lactobacillus in the preterm group (50.7%) compared with the full-term group (72.3%), which was statistically significant (
p = 0.004). The prevalence of
Gardnerella vaginalis was also significantly higher in the preterm group (40.8%) than in the full-term group (22.3%) (
p = 0.010), as described in
Table 4. However, the differences in the prevalence of
Candida spp., bacterial vaginosis combined with fungi, Gram-positive cocci, and Gram-negative bacilli between the two groups were not statistically significant.
The prevalence of Bacillus spp. and Corynebacterium spp. was slightly higher in the full-term group compared with the preterm group, but these differences were not statistically significant (Bacillus spp.: 7.0% in preterm vs. 8.5% in full-term groups, p = 0.727; Corynebacterium spp.: 8.5% in preterm vs. 10.6% in full-term groups, p = 0.638). Similarly, the presence of Enterococcus spp., Escherichia coli, Haemophilus influenzae, Klebsiella spp., Proteus mirabilis, Staphylococcus aureus, Streptococcus spp., and Trichomonas vaginalis did not show statistically significant differences between the two groups.
However, there were statistically significant differences noted in the frequency of specific pathogens. The incidence of
Chlamydia trachomatis was notably higher in the preterm group, 12.7%, versus the full-term group, merely 3.2% (
p = 0.020). In addition, the preterm group exhibited a substantially higher rate of infections by
Mycoplasma hominis (16.9%) compared with only 4.3% in the other group (
p = 0.006). The presence of
Neisseria gonorrhoeae was also significantly elevated in the preterm group, 7.0%, in contrast to the full-term group, with a significant difference (
p = 0.042). Furthermore,
Ureaplasma urealyticum was found to be much more common in the preterm group, with a rate of 19.7%, compared with 6.4% in the full-term group (
p = 0.009), as seen in
Table 5.
There was a much higher rate of ESBL presence in the preterm group (21.1%) compared with the full-term group (5.3%) (p < 0.001). In addition, VRE infections were found to be significantly more common in the preterm group (8.5%) than in the full-term group (1.1%, p = 0.034). Likewise, CRE infections were detected particularly in the preterm group (5.6%), with no presence in the full-term group (p = 0.022). Furthermore, the overall prevalence of MDR pathogens was considerably higher in the preterm group (28.2%) versus the full-term group (7.4%) (p < 0.001).
However, the prevalence of Methicillin-Resistant Staphylococcus aureus (MRSA) did not differ significantly between the preterm and full-term groups (2.8% vs. 3.2%, p = 0.891). Additionally, the resistance patterns for antibiotics such as Nitrofurantoin, Ampicillin/Sulbactam, Macrolides, Piperacillin/Tazobactam, Glycopeptides, 4th-Generation Cephalosporin, Ticarcillin/Clavulanic, and Quinolones were not significantly different between the two groups. Of 27 samples resistant to macrolides, 12 (40.7%) were Chlamydia and Mycoplasma.
On the other hand, a significant difference was observed in the resistance to Penicillin (42.3% in preterm group vs. 19.1% in full-term group,
p = 0.001) and 2nd- and 3rd-Generation Cephalosporins. The rates of resistance to 2nd-Generation Cephalosporin were 29.6% in the preterm group and 12.8% in the full-term group (
p = 0.011), and for 3rd-Generation Cephalosporin, they were 31.0% in the preterm group and 11.7% in the full-term group (
p < 0.001), as described in
Table 6.
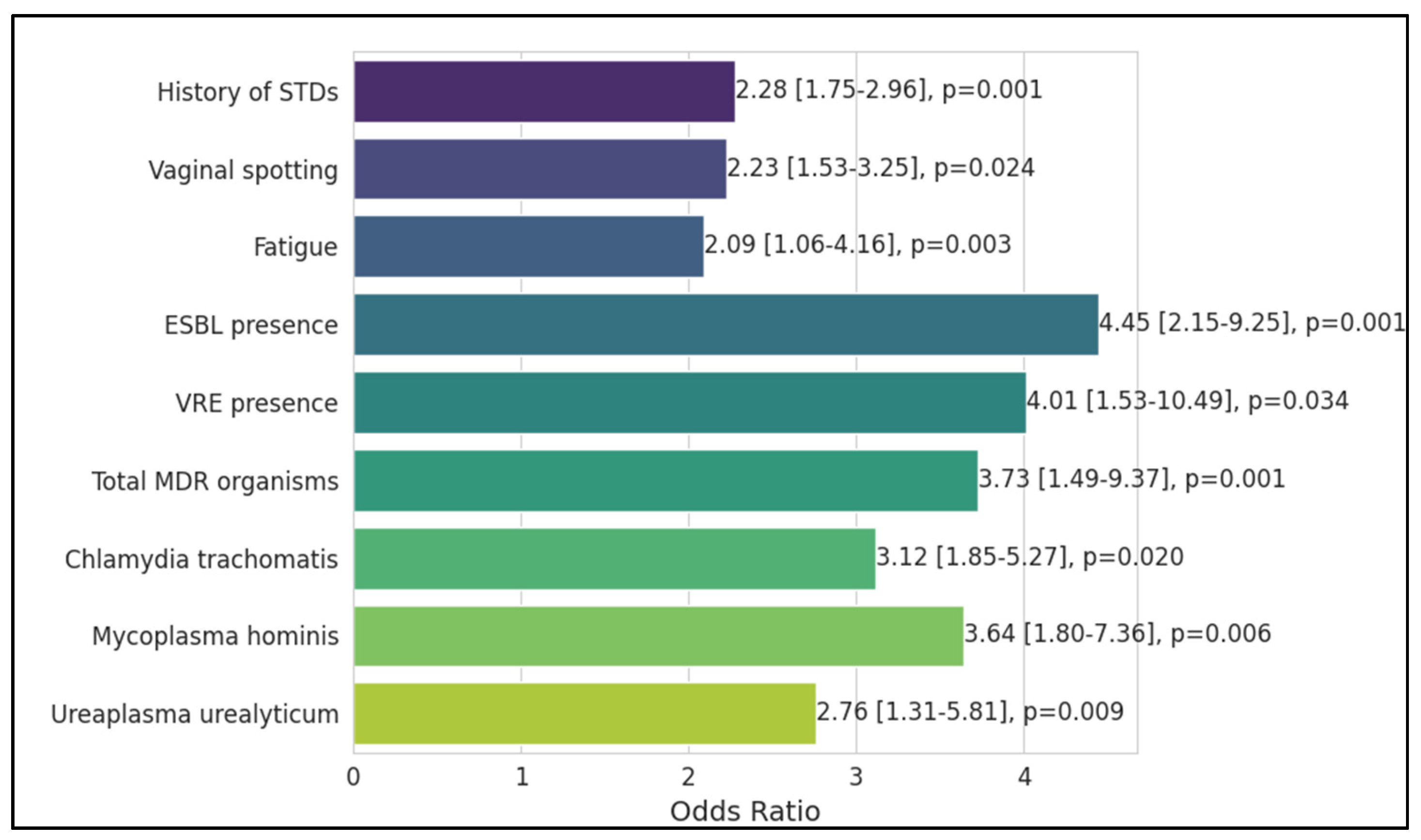
The history of sexually transmitted diseases (STDs) was a notable risk factor, with an odds ratio of 2.28, indicating more than double the odds of preterm birth, which was statistically significant (p = 0.001). Genital herpes did not emerge as a significant risk factor, nor did fever during pregnancy. Vaginal spotting was similarly significant, increasing the odds by over two times (OR = 2.23, p = 0.024). Fatigue was also associated with an increased risk of preterm birth (OR = 2.09, p = 0.003).
The presence of Extended-Spectrum Beta-Lactamases (ESBLs) was a particularly strong risk factor, more than quadrupling the odds of preterm birth (OR = 4.45,
p = 0.001). Vancomycin-Resistant Enterococci (VRE) presence was another critical factor, with a four-fold increase in the odds (OR = 4.01,
p = 0.034). The overall presence of Multidrug-Resistant (MDR) organisms significantly increased the odds of preterm birth (OR = 3.73,
p = 0.001). Specific pathogens like
Chlamydia trachomatis (OR = 3.12,
p = 0.020) and
Mycoplasma hominis (OR = 3.64,
p = 0.006) were identified as significant risk factors.
Ureaplasma urealyticum also showed a significant association with increased odds of preterm birth (OR = 2.76,
p = 0.009), as presented in
Table 7 and
Figure 1.





 ,
, 

{kind=link}