

Soluble Urokinase Plasminogen Activator Receptor (SuPAR) Analysis for Diagnosis of Periprosthetic Joint Infection
 , , , , , , ,
, , , , , , ,  and
and
Abstract
1. Introduction
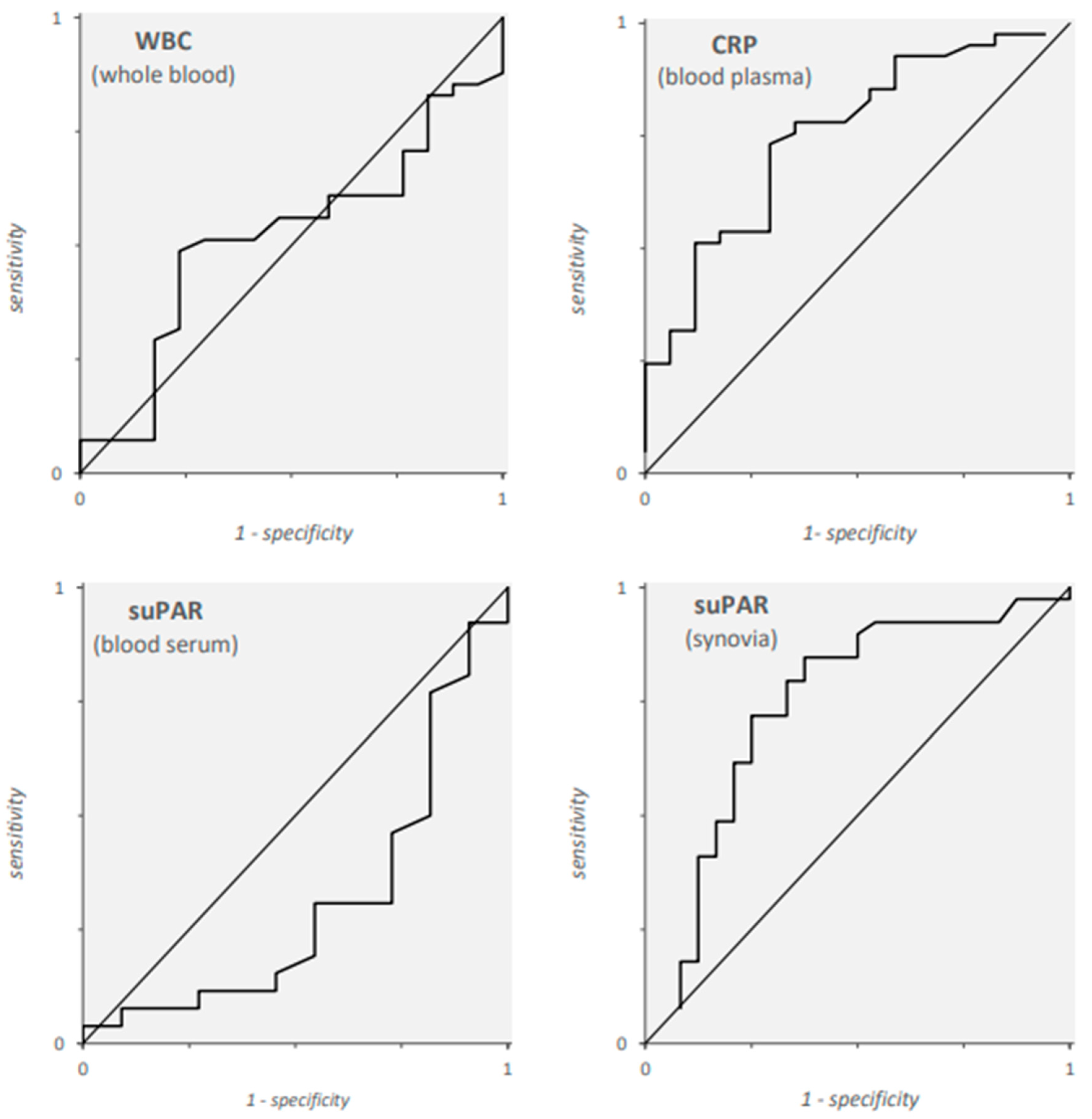
2. Results
3. Discussion
4. Materials and Methods
4.1. Sample Collection and Laboratory Analyses
4.2. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kurtz, S.M.; Ong, K.L.; Schmier, J.; Mowat, F.; Saleh, K.; Dybvik, E.; Kärrholm, J.; Garellick, G.; Havelin, L.I.; Furnes, O.; et al. Future clinical and economic impact of revision total hip and knee arthroplasty. J. Bone Jt. Surg. Am. 2007, 89 (Suppl. S3), 144–151. [Google Scholar]
- Tande, A.J.; Patel, R. Prosthetic joint infection. Clin. Microbiol. Rev. 2014, 27, 302–345. [Google Scholar] [CrossRef]
- Kapadia, B.H.; Berg, R.A.; Daley, J.A.; Fritz, J.; Bhave, A.; Mont, M.A. Periprosthetic joint infection. Lancet 2016, 387, 386–394. [Google Scholar] [CrossRef]
- McNally, M.; Sousa, R.; Wouthuyzen-Bakker, M.; Chen, A.F.; Soriano, A.; Vogely, H.C.; Clauss, M.; Higuera, C.A.; Trebše, R. The EBJIS definition of periprosthetic joint infection. Bone Jt. J. 2021, 103-B, 18–25. [Google Scholar] [CrossRef]
- Vale, J.S.; Castelo, F.S.; Barros, B.S.; Ribau, A.C.; Carvalho, A.D.; Sousa, R.J.G. Synovial Fluid Biomarkers for the Diagnosis of Periprosthetic Joint Infection-A Systematic Review and Meta-Analysis of Their Diagnostic Accuracy According to Different Definitions. J. Arthroplast. 2023, 38, 2731–2738.e3. [Google Scholar] [CrossRef]
- Behrendt, N.; Rønne, E.; Danø, K. The structure and function of the urokinase receptor, a membrane protein governing plasminogen activation on the cell surface. Biol. Chem. Hoppe Seyler 1995, 376, 269–279. [Google Scholar]
- Rønne, E.; Pappot, H.; Grøndahl-Hansen, J.; Høyer-Hansen, G.; Plesner, T.; Hansen, N.E.; Danø, K. The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria. Br. J. Haematol. 1995, 89, 576–581. [Google Scholar] [CrossRef]
- Andreasen, P.A.; Kjøller, L.; Christensen, L.; Duffy, M.J. The urokinase-type plasminogen activator system in cancer metastasis: A review. Int. J. Cancer 1997, 72, 1–22. [Google Scholar] [CrossRef]
- Wei, C.; Möller, C.C.; Altintas, M.M.; Li, J.; Schwarz, K.; Zacchigna, S.; Xie, L.; Henger, A.; Schmid, H.; Rastaldi, M.P.; et al. Modification of kidney barrier function by the urokinase receptor. Nat. Med. 2008, 14, 55–63. [Google Scholar] [CrossRef]
- Bastarache, J.A.; Ware, L.B.; Bernard, G.R. The role of the coagulation cascade in the continuum of sepsis and acute lung injury and acute respiratory distress syndrome. Semin. Respir. Crit. Care Med. 2006, 27, 365–376. [Google Scholar] [CrossRef]
- Koch, A.; Voigt, S.; Kruschinski, C.; Sanson, E.; Dückers, H.; Horn, A.; Yagmur, E.; Zimmermann, H.; Trautwein, C.; Tacke, F. Circulating soluble urokinase plasminogen activator receptor is stably elevated during the first week of treatment in the intensive care unit and predicts mortality in critically ill patients. Crit. Care 2011, 15, R63. [Google Scholar] [CrossRef]
- Wittenhagen, P.; Kronborg, G.; Weis, N.; Nielsen, H.; Obel, N.; Pedersen, S.S.; Eugen-Olsen, J. The plasma level of soluble urokinase receptor is elevated in patients with Streptococcus pneumoniae bacteraemia and predicts mortality. Clin. Microbiol. Infect. 2004, 10, 409–415. [Google Scholar] [CrossRef][Green Version]
- Chen, D.; Wu, X.; Yang, J.; Yu, L. Serum plasminogen activator urokinase receptor predicts elevated risk of acute respiratory distress syndrome in patients with sepsis and is positively associated with disease severity, inflammation and mortality. Exp. Ther. Med. 2019, 18, 2984–2992. [Google Scholar] [CrossRef]
- Slot, O.; Brünner, N.; Locht, H.; Oxholm, P.; Stephens, R.W. Soluble urokinase plasminogen activator receptor in plasma of patients with inflammatory rheumatic disorders: Increased concentrations in rheumatoid arthritis. Ann. Rheum. Dis. 1999, 58, 488–492. [Google Scholar] [CrossRef]
- Velissaris, D.; Pierrakos, C.; Karamouzos, V.; Pantzaris, N.D.; Gogos, C. The use of soluble urokinase plasminogen activator receptor (suPAR) as a marker of sepsis in the emergency department setting. A current review. Acta Clin. Belg. 2021, 76, 79–84. [Google Scholar] [CrossRef]
- Ni, W.; Han, Y.; Zhao, J.; Cui, J.; Wang, K.; Wang, R.; Liu, Y. Serum soluble urokinase-type plasminogen activator receptor as a biological marker of bacterial infection in adults: A systematic review and meta-analysis. Sci. Rep. 2016, 6, 39481. [Google Scholar] [CrossRef]
- Velissaris, D.; Zareifopoulos, N.; Koniari, I.; Karamouzos, V.; Bousis, D.; Gerakaris, A.; Platanaki, C.; Kounis, N. Soluble Urokinase Plasminogen Activator Receptor as a Diagnostic and Prognostic Biomarker in Cardiac Disease. J. Clin. Med. Res. 2021, 13, 133–142. [Google Scholar] [CrossRef]
- Baart, V.M.; Houvast, R.D.; de Geus-Oei, L.F.; Quax, P.H.A.; Kuppen, P.J.K.; Vahrmeijer, A.L.; Sier, C.F.M. Molecular imaging of the urokinase plasminogen activator receptor: Opportunities beyond cancer. EJNMMI Res. 2020, 10, 87. [Google Scholar] [CrossRef]
- Galliera, E.; Drago, L.; Marazzi, M.G.; Romanò, C.; Vassena, C.; Corsi Romanelli, M.M. Soluble urokinase-type plasminogen activator receptor (suPAR) as new biomarker of the prosthetic joint infection: Correlation with inflammatory cytokines. Clin. Chim. Acta 2015, 441, 23–28. [Google Scholar] [CrossRef]
- Rasmussen, L.J.H.; Caspi, A.; Ambler, A.; Danese, A.; Elliott, M.; Eugen-Olsen, J.; Hariri, A.R.; Harrington, H.; Houts, R.; Poulton, R.; et al. Association Between Elevated suPAR, a New Biomarker of Inflammation, and Accelerated Aging. J. Gerontol. A Biol. Sci. Med. Sci. 2021, 76, 318–327. [Google Scholar] [CrossRef]
- Enocsson, H.; Lukic, T.; Ziegelasch, M.; Kastbom, A. Serum levels of the soluble urokinase plasminogen activator receptor (suPAR) correlates with disease activity in early rheumatoid arthritis and reflects joint damage over time. Transl. Res. 2021, 232, 142–149. [Google Scholar] [CrossRef]
- Holstein, R.M.; Seppälä, S.; Kaartinen, J.; Hongisto, M.; Hyppölä, H.; Castrén, M. Soluble Urokinase Plasminogen Activator Receptor (suPAR) in the Emergency Department (Ed): A Tool for the Assessment of Elderly Patients. J. Clin. Med. 2022, 11, 3283. [Google Scholar] [CrossRef]
- Stauning, M.A.; Altintas, I.; Kallemose, T.; Eugen-Olsen, J.; Lindstrøm, M.B.; Rasmussen, L.J.H.; Gamst-Jensen, H.; Nehlin, J.O.; Andersen, O.; Tingleff, J. Soluble Urokinase Plasminogen Activator Receptor as a Decision Marker for Early Discharge of Patients with COVID-19 Symptoms in the Emergency Department. J. Emerg. Med. 2021, 61, 298–313. [Google Scholar] [CrossRef]
- Kyriazopoulou, E.; Poulakou, G.; Milionis, H.; Metallidis, S.; Adamis, G.; Tsiakos, K.; Fragkou, A.; Rapti, A.; Damoulari, C.; Fantoni, M.; et al. Early treatment of COVID-19 with anakinra guided by soluble urokinase plasminogen receptor plasma levels: A double-blind, randomized controlled phase 3 trial. Nat. Med. 2021, 27, 1752–1760. [Google Scholar] [CrossRef]
- Chu, S.C.; Yang, S.F.; Lue, K.H.; Hsieh, Y.S.; Hsiao, T.Y.; Lu, K.H. Urokinase-type plasminogen activator, receptor, and inhibitor correlating with gelatinase-B (MMP-9) contribute to inflammation in gouty arthritis of the knee. J. Rheumatol. 2006, 33, 311–317. [Google Scholar]
- Skottrup, P.D.; Dahlén, G.; Baelum, V.; Lopez, R. Soluble urokinase-type plasminogen activator receptor is associated with signs of periodontitis in adolescents. Eur. J. Oral Sci. 2018, 126, 292–299. [Google Scholar] [CrossRef]
- Matzkies, L.M.; Raggam, R.B.; Flick, H.; Rabensteiner, J.; Feierl, G.; Hoenigl, M.; Prattes, J. Prognostic and diagnostic potential of suPAR levels in pleural effusion. J. Infect. 2017, 75, 465–467. [Google Scholar] [CrossRef]
- Ozsu, S.; Oztuna, F.; Mentese, A.; Abul, Y.; Ozlu, T. Diagnostic value of suPAR in differentiating noncardiac pleural effusions from cardiac pleural effusions. Clin. Respir. J. 2016, 10, 61–66. [Google Scholar] [CrossRef]
- Idell, S.; Lee, Y.C.G. suPAR Surprises as a Biomarker of Invasive Outcomes in Pleural Infection. Am. J. Respir. Crit. Care Med. 2020, 201, 1470–1472. [Google Scholar] [CrossRef]
- Arnold, D.T.; Hamilton, F.W.; Elvers, K.T.; Frankland, S.W.; Zahan-Evans, N.; Patole, S.; Medford, A.; Bhatnagar, R.; Maskell, N.A. Pleural Fluid suPAR Levels Predict the Need for Invasive Management in Parapneumonic Effusions. Am. J. Respir. Crit. Care Med. 2020, 201, 1545–1553. [Google Scholar] [CrossRef]
- Skovsted, T.A.; Petersen, E.R.B.; Fruekilde, M.B.; Pedersen, A.K.; Pielak, T.; Eugen-Olsen, J. Validation of suPAR turbidimetric assay on Cobas® (c502 and c702) and comparison to suPAR ELISA. Scand. J. Clin. Lab. Investig. 2020, 80, 327–335. [Google Scholar] [CrossRef]
- Borrillo, F.; Panteghini, M. Current performance of C-reactive protein determination and derivation of quality specifications for its measurement uncertainty. Clin. Chem. Lab. Med. 2023, 61, 1552–1557. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Labmayr, V.; Eckhart, F.J.; Smolle, M.; Klim, S.; Fischerauer, S.F.; Bernhardt, G.; Seibert, F.J. Sterile Punktion großer Gelenke [Sterile puncture of large joints]. Oper. Orthop. Traumatol. 2023, 35, 65–80. (In German) [Google Scholar] [CrossRef]
- Chew-Harris, J.; Appleby, S.; Richards, A.M.; Troughton, R.W.; Pemberton, C.J. Analytical, biochemical and clearance considerations of soluble urokinase plasminogen activator receptor (suPAR) in healthy individuals. Clin. Biochem. 2019, 69, 36–44. [Google Scholar] [CrossRef]
- Wlazel, R.N.; Szwabe, K.; Guligowska, A.; Kostka, T. Soluble urokinase plasminogen activator receptor level in individuals of advanced age. Sci. Rep. 2020, 10, 15462. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Analysis | PJI | PJI Negative | p-Value |
|---|---|---|---|
| blood | |||
| WBC, G/L | 10 (7–12) | 9 (8–10) | 0.713 |
| CRP, mg/L | 77 (38–152) | 25 (10–70) | 0.002 |
| suPAR, ng/mL | 5 (4–6) | 8 (5–9) | 0.132 |
| synovial fluid | |||
| WBC, cells/µL | 25,000 (10,000–53,100) | 250 (100–500) | <0.001 |
| suPAR, ng/mL | 118 (59–185) | 38 (26–75) | <0.001 |
| Analyte | Cut-Off | J | TPR | TNR | PPV | NPV |
|---|---|---|---|---|---|---|
| WBC (whole blood, n = 58) | 9.6 G/L | 0.28 | 0.51 | 0.76 | 0.84 | 0.39 |
| CRP (blood plasma, n = 58) | 36 mg/L | 0.46 | 0.76 | 0.71 | 0.86 | 0.55 |
| 75 mg/L | 0.42 | 0.54 | 0.88 | 0.92 | 0.44 | |
| suPAR (blood plasma, n = 37) | 12 ng/mL | 0.04 | 0.04 | 1.00 | 1.00 | 0.31 |
| suPAR (synovial fluid, n = 63) | 54 ng/mL | 0.49 | 0.82 | 0.67 | 0.80 | 0.70 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klim, S.M.; Prattes, J.; Amerstorfer, F.; Niedrist, T.; Zurl, C.; Stradner, M.; Dreo, B.; Glehr, G.; Leithner, A.; Glehr, M.; et al. Soluble Urokinase Plasminogen Activator Receptor (SuPAR) Analysis for Diagnosis of Periprosthetic Joint Infection. Antibiotics 2024, 13, 179. https://doi.org/10.3390/antibiotics13020179
Klim SM, Prattes J, Amerstorfer F, Niedrist T, Zurl C, Stradner M, Dreo B, Glehr G, Leithner A, Glehr M, et al. Soluble Urokinase Plasminogen Activator Receptor (SuPAR) Analysis for Diagnosis of Periprosthetic Joint Infection. Antibiotics. 2024; 13(2):179. https://doi.org/10.3390/antibiotics13020179
Chicago/Turabian StyleKlim, Sebastian M., Jürgen Prattes, Florian Amerstorfer, Tobias Niedrist, Christoph Zurl, Martin Stradner, Barbara Dreo, Gunther Glehr, Andreas Leithner, Mathias Glehr, and et al. 2024. "Soluble Urokinase Plasminogen Activator Receptor (SuPAR) Analysis for Diagnosis of Periprosthetic Joint Infection" Antibiotics 13, no. 2: 179. https://doi.org/10.3390/antibiotics13020179
APA StyleKlim, S. M., Prattes, J., Amerstorfer, F., Niedrist, T., Zurl, C., Stradner, M., Dreo, B., Glehr, G., Leithner, A., Glehr, M., Reinbacher, P., Sadoghi, P., & Hauer, G. (2024). Soluble Urokinase Plasminogen Activator Receptor (SuPAR) Analysis for Diagnosis of Periprosthetic Joint Infection. Antibiotics, 13(2), 179. https://doi.org/10.3390/antibiotics13020179