
The Availability of Essential Antimicrobials in Public and Private Sector Facilities: A Cross-Sectional Survey in a District of North India


Abstract
1. Introduction
2. Results
2.1. Availability of Antimicrobials Listed in Primary (NLEM 2015) and Secondary (Selected) Lists
2.1.1. Antibiotics
2.1.2. Other Antimicrobials
2.1.3. Pediatric Formulations of Antimicrobials
2.2. Gap Analysis for the Availability of Antimicrobials in the Public Sector
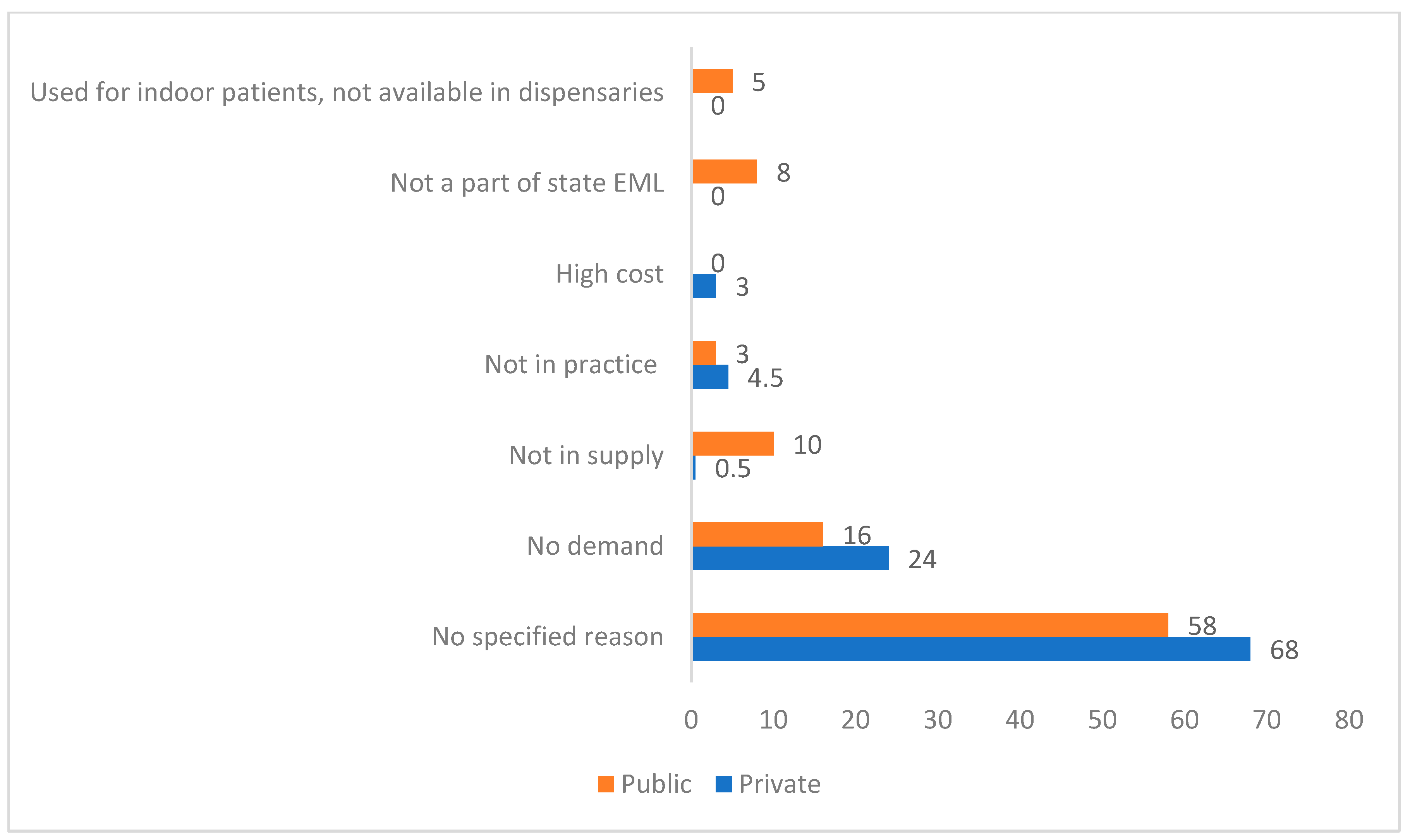
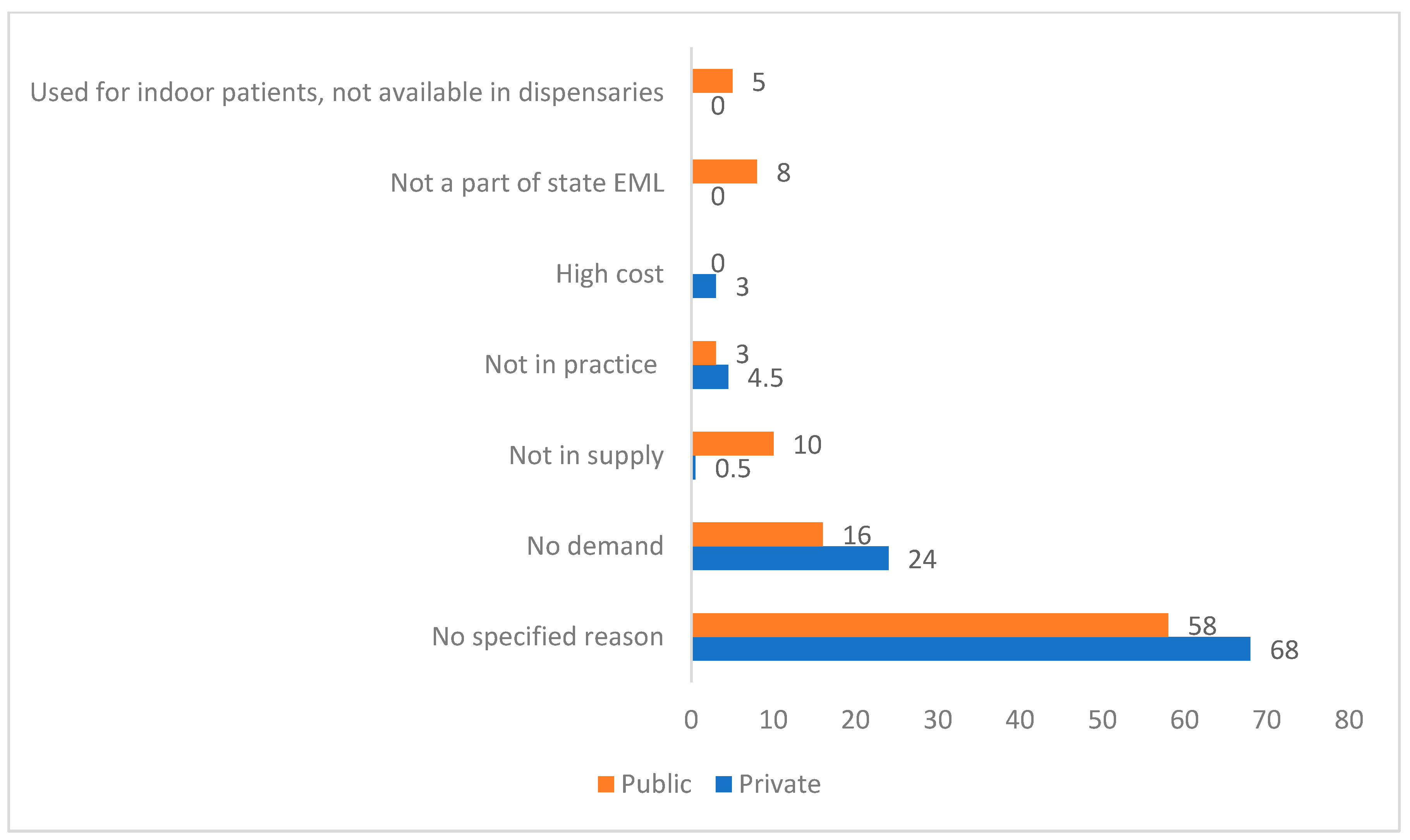
2.3. Reasons for Sub-Optimal Availability
3. Discussion
4. Materials and Methods
4.1. Study Setting
4.2. Drug Procurement Model in the District
4.3. Study Design
4.4. Survey Facilities Sampling
4.5. Data Collection
4.6. Data Analysis
4.6.1. Availability of Antimicrobials Listed in Primary (NLEM 2015) and Secondary (Selected) Lists
4.6.2. Gap Analysis for the Availability of Antimicrobials in the Public Sector
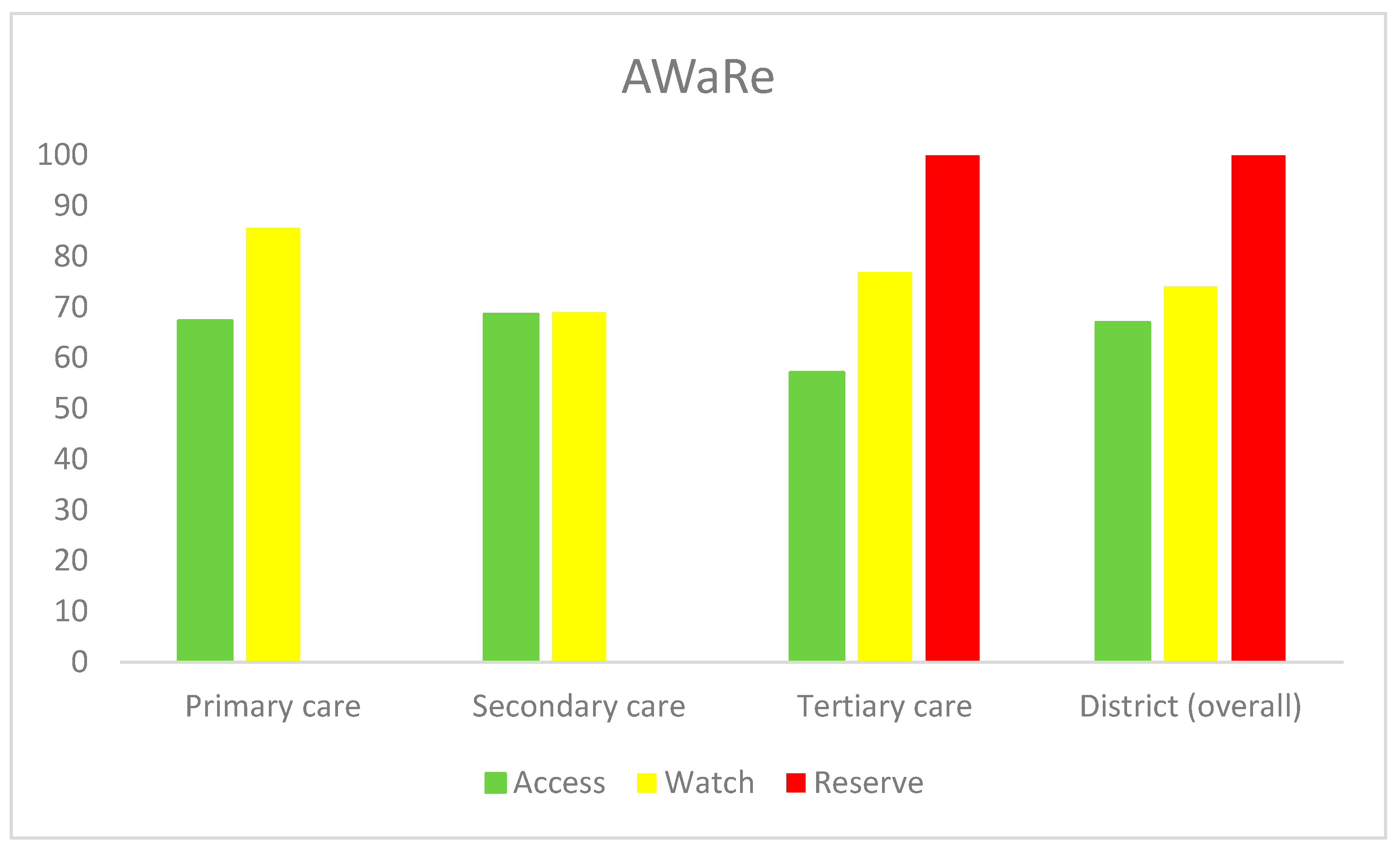
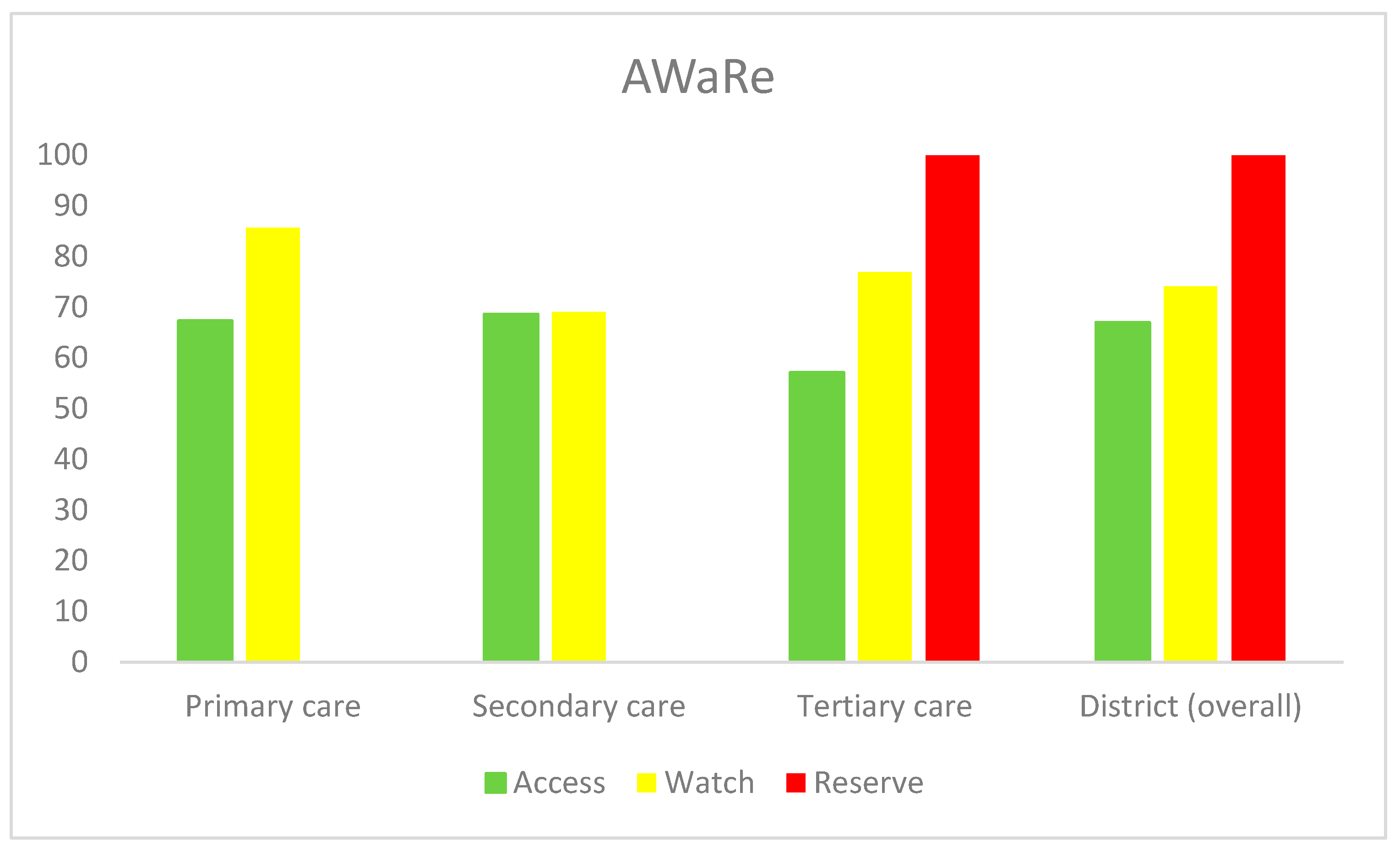
4.6.3. Gap Analysis for Availability of Antibiotics in Public Sector as per WHO Access, Watch, and Reserve (AWaRe) 2021 Classification [30]
4.6.4. Reasons for Sub-Optimal Availability of Antimicrobials
4.7. Ethical and Administrative Approvals
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO Model Lists of Essential Medicines. Available online: https://www.who.int/groups/expert-committee-on-selection-and-use-of-essential-medicines/essential-medicines-lists (accessed on 20 August 2021).
- WHO. The Selection and Use of Essential Medicines; Report of a WHO Expert Committee, WHO Technical Report Series, No. 914; World Health Organization: Geneva, Switzerland, 2002.
- National List of Essential Medicines of India. Available online: https://pharmaceuticals.gov.in/sites/default/files/NLEM.pdf (accessed on 20 August 2021).
- National List of Essential Medicines 2022. Available online: https://main.mohfw.gov.in/sites/default/files/Notification%20and%20Report%20on%20National%20List%20of%20Essential%20Medicines%2C%202022.pdf (accessed on 15 October 2022).
- Shafiq, N.; Pandey, A.K.; Malhotra, S.; Holmes, A.; Mendelson, M.; Malpani, R.; Balasegaram, M.; Charani, E. Shortage of essential antimicrobials: A major challenge to global health security. BMJ Glob. Health 2021, 6, e006961. [Google Scholar] [CrossRef] [PubMed]
- Mendelson, M.; Røttingen, J.A.; Gopinathan, U.; Hamer, D.H.; Wertheim, H.; Basnyat, B.; Butler, C.; Tomson, G.; Balasegaram, M. Maximizing access to achieve appropriate human antimicrobial use in low-income and middle-income countries. Lancet 2016, 387, 188–198. [Google Scholar] [CrossRef] [PubMed]
- Meeting Report: Antibiotic Shortages: Magnitude, Causes, and Possible Solutions. Norwegian Directorate of Health, Oslo, Norway, 10–11 December 2018. Available online: https://www.who.int/publications/i/item/meeting-report-antibiotic-shortages-magnitude-causes-and-possible-solutions (accessed on 15 March 2023).
- Pulcini, C.; Bush, K.; Craig, W.A.; Frimodt-Møller, N.; Grayson, M.L.; Mouton, J.W.; Turnidge, J.; Harbarth, S.; Gyssens, I.C.; ESCMID Study Group for Antibiotic Policies. Forgotten antibiotics: An inventory in Europe, the United States, Canada, and Australia. Clin. Infect. Dis. 2012, 54, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Pulcini, C.; Mohrs, S.; Beovic, B.; Gyssens, I.; Theuretzbacher, U.; Cars, O.; Bosevska, G.; Bruch, M.; Bush, K.; Cizmovic, L.; et al. Forgotten antibiotics: A follow-up inventory study in Europe, the USA, Canada, and Australia. Int. J. Antimicrob. Agents 2017, 49, 98–101. [Google Scholar] [CrossRef] [PubMed]
- Quadri, F.; Mazer-Amirshahi, M.; Fox, E.R.; Hawley, K.L.; Pines, J.M.; Zocchi, M.S.; May, L. Antibacterial drug shortages from 2001 to 2013: Implications for clinical practice. Clin. Infect. Dis. 2015, 60, 1737–1742. [Google Scholar] [CrossRef] [PubMed]
- Honda, H.; Murakami, S.; Tokuda, Y.; Tagashira, Y.; Takamatsu, A. Critical National Shortage of Cefazolin in Japan: Management Strategies. Clin. Infect. Dis. 2020, 71, 1783–1789. [Google Scholar] [CrossRef] [PubMed]
- Prinja, S.; Bahuguna, P.; Tripathy, J.P.; Kumar, R. Availability of medicines in public sector health facilities of two North Indian States. BMC Pharmacol. Toxicol. 2015, 16, 43. [Google Scholar] [CrossRef]
- Kotwani, A.; Holloway, K. Access to antibiotics in New Delhi, India: Implications for antibiotic policy. J. Pharm. Policy. Pract. 2013, 6, 6. [Google Scholar] [CrossRef] [PubMed]
- Cameron, A.; Ewen, M.; Ross-Degnan, D.; Ball, D.; Laing, R. Medicine prices, availability, and affordability in 36 developing and middle-income countries: A secondary analysis. Lancet. 2009, 373, 240–249. [Google Scholar] [CrossRef] [PubMed]
- Knowles, R.; Sharland, M.; Hsia, Y.; Magrini, N.; Moja, L.; Siyam, A.; Tayler, E. Measuring antibiotic availability and use in 20 low- and middle-income countries. Bull. World Health Organ. 2020, 98, 177–187C. [Google Scholar] [CrossRef] [PubMed]
- AWaRe Policy Brief. Available online: https://adoptaware.org/assets/pdf/aware_policy_brief.pdf (accessed on 5 March 2022).
- Banerjee, R.; Thurm, C.W.; Fox, E.R.; Hersh, A.L. Antibiotic Shortages in Pediatrics. Pediatrics 2018, 142, e20180858. [Google Scholar] [CrossRef]
- Swain, T.R.; Rath, B.; Dehury, S.; Tarai, A.; Das, P.; Samal, R.; Samal, S.; Nayak, H. Pricing and availability of some essential child-specific medicines in Odisha. Indian J. Pharmacol. 2015, 47, 496–501. [Google Scholar] [CrossRef] [PubMed]
- Downes, K.J.; Cowden, C.; Laskin, B.L.; Huang, Y.S.; Gong, W.; Bryan, M.; Fisher, B.T.; Goldstein, S.L.; Zaoutis, T.E. Association of acute kidney injury with concomitant vancomycin and piperacillin/tazobactam treatment among hospitalized children. JAMA Pediatr. 2017, 171, e173219. [Google Scholar] [CrossRef] [PubMed]
- Cook, K.M.; Gillon, J.; Grisso, A.G.; Banerjee, R.; Jimenez-Truque, N.; Phillips, E.J.; Van Driest, S.L. Incidence of Nephrotoxicity Among Pediatric Patients Receiving Vancomycin With Either Piperacillin-Tazobactam or Cefepime: A Cohort Study. J. Pediatric. Infect. Dis. Soc. 2019, 8, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Nishal, P.K.; Kapoor, A.; Jain, V.K.; Dayal, S.; Aggarwal, K. Changing trends in acquired syphilis at a Tertiary Care Center of North India. Indian J. Sex. Transm. Dis. AIDS 2015, 36, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Kaushal, K.; Veena, M. Two cases of Kala-azar in Haryana with no evidence of local transmission. J. Commun. Dis. 2008, 40, 87–88. [Google Scholar]
- National Center for Vector Borne Diseases Control. Available online: https://ncvbdc.mohfw.gov.in/index1.php?lang=1&level=1&sublinkid=5899&lid=3686 (accessed on 15 September 2022).
- National Viral Hepatitis Control Program. Available online: https://nvhcp.mohfw.gov.in/ (accessed on 15 September 2022).
- Essential Medicine List (2013–2014). Available online: http://nhmharyana.gov.in/files/essentialdruglist2013.pdf (accessed on 20 August 2021).
- Rohtak District Population. Available online: https://www.indiagrowing.com/Haryana/Rohtak_District (accessed on 16 November 2022).
- India Health System Review. Health Systems in Transition. 2022, Volume 11. Available online: https://apo.who.int/publications/i/item/india-health-system-review (accessed on 10 September 2023).
- Prinja, S.; Kanavos, P.; Kumar, R. Health care inequities in north India: Role of public sector in universalizing health care. Indian. J. Med. Res. 2012, 136, 421–431. [Google Scholar]
- The Medicine Procurement and Management Policy 2012. Available online: http://www.nhmharyana.gov.in/files/drugpolicyfinal.pdf (accessed on 25 July 2021).
- WHO 2021 Aware Classification. Available online: https://www.who.int/publications/i/item/2021-aware-classification (accessed on 15 September 2022).

{kind=link}
{kind=link}
| S. No. | Name of Antibiotic | WHO AWaRe (Access, Watch, Reserve) Category | Formulation | Strength | Healthcare Facility Level | Data on Availability | |||
|---|---|---|---|---|---|---|---|---|---|
| Public Sector | Private Sector | Other Sector | Total | ||||||
| Primary care (N = 7); Secondary (N = 5); Tertiary (N = 1) | Private Retailers (N = 10) | (AMRIT * Pharmacy; N = 2) | |||||||
| Antibiotics included in both NLEM 2015 and the selected (secondary) list for survey | |||||||||
| 1. | Amoxicillin | Access | Capsule | 250 mg, 500 mg | P, S, T | 7 (100)/5 (100)/A | 9 (90) | 2 (100) | 24/25 (96) |
| Suspension | 125 mg/5 mL | P, S, T | 7 (100)/5 (100)/A | 9 (90) | 1 (50) | 23/25 (92) | |||
| 2. | Amoxicillin + clavulanic acid | Access | Tablet | 500/125 mg | P, S, T | 5 (71.4)/3 (60)/A | 10 (100) | 2 (100) | 21/25 (84) |
| Injection | 0.6 g, 1.2 g | S, T | -/3 (60)/A | 8 (80) | 0 | 12/18 (66.7) | |||
| Suspension | 228.5 mg/5 mL | P, S, T | 3 (42.8)/4 (80)/A | 9 (90) | 2 (100) | 19/25 (76) | |||
| 3. | Cefazolin # | Access | Injection | 500 mg, 1 g | P, S, T | 0/0/NA | 3 (30) | 0 | 3/18 (16.7) |
| 4. | Cefixime | Watch | Tablet | 100, 200, 400 mg | S, T | -/4 (80)/A | 10 (100) | 2 (100) | 17/18 (94.4) |
| Syrup | 50 mg/5 mL | S, T | -/3 (60)/NA | 8 (80) | 2 (100) | 13/18 (72.2) | |||
| 5. | Ceftriaxone | Watch | Injection | 250 mg, 500 mg, 1 g | S, T | -/5 (100)/A | 10 (100) | 2 (100) | 18/18 (100) |
| 6. | Azithromycin | Watch | Tablet | 250 mg, 500 mg | P, S, T | 7 (100)/5 (100)/A | 10 (100) | 2 (100) | 25/25 (100) |
| Injection | 500 mg | S, T | -/1 (20)/A | 4 (40) | 2 (100) | 8/18 (44.4) | |||
| Suspension | 200 mg/5 mL | P, S, T | 7 (100)/5 (100)/A | 7 (70) | 2 (100) | 22/25 (88) | |||
| 7. | Doxycycline | Access | Capsule | 100 mg | P, S, T | 7 (100)/5 (100)/A | 8 (80) | 2 (100) | 23/25 (92) |
| 8. | Ciprofloxacin | Watch | Tablet | 250 mg, 500 mg | P, S, T | 7 (100)/5 (100)/A | 10 (100) | 2 (100) | 25/25 (100) |
| Injection | 200 mg/100 mL | P, S, T | 2 (28.6)/1 (20)/A | 7 (70) | 1 (50) | 12/25 (48) | |||
| 9. | Cotrimoxazole | Access | Tablet | 400/80, 800/160 mg | P, S, T | 6 (85.7)/4 (80)/A | 8 (80) | 1 (50) | 20/25 (80) |
| Suspension | 200 + 40 mg/5 mL | P, S, T | 1 (14.3)/2 (40)/A | 4 (40) | 1 (50) | 9/25 (36) | |||
| 10. | Metronidazole | Access | Tablet | 200 mg, 400 mg | P, S, T | 6 (85.7)/5 (100)/A | 10 (100) | 2 (100) | 24/25 (96) |
| Injection | 500 mg/100 mL | P, S, T | 3 (42.8)/4 (80)/NA | 7 (70) | 2 (100) | 16/25 (64) | |||
| Suspension | 200 mg/5 mL | P, S, T | 7 (100)/5 (100)/NA | 7 (70) | 0 | 19/25 (76) | |||
| 11. | Vancomycin # | Watch | Injection | 250 mg, 500 mg, 1 g | T | -/-/A | 6 (60) | 1 (50) | 8/13 (61.5) |
| 12. | Nitrofurantoin # | Access | Tablet | 100 mg | P, S, T | 4 (57)/4 (80)/A | 8 (80) | 2 (100) | 19/25 (76) |
| Antibiotics included in NLEM 2015 but not in the selected (secondary) list for survey | |||||||||
| 13. | Ampicillin | Access | Injection | 500 mg, 1 g | P, S, T | 3 (42.8)/4 (80)/NA | 6 (60) | 0 | 14/25 (56) |
| 14. | Benzathine benzylpenicillin | Access | Injection | 6 lac, 12 lac Units | P, S, T | 0/0/NA | 0 | 0 | 0 |
| 15. | Benzylpenicillin | Access | Injection | 10 lac Units | P, S, T | 0/0/NA | 0 | 0 | 0 |
| 16. | Cloxacillin # | Access | Capsule | 250 mg, 500 mg | P, S, T | 2 (28.6)/4 (80)/NA | 3 (30) | 0 | 9/25 (36) |
| Injection | 250 mg | P, S, T | 0/1 (20)/NA | 1 (10) | 0 | 2/25 (8) | |||
| 17. | Cefadroxil | Access | Tablet | 250 mg, 500 mg | P, S, T | 0/2 (40)/NA | 7 (70) | 0 | 9/25 (36) |
| Syrup | 125 mg/5 mL | P, S, T | 6 (85.7)/5 (100)/NA | 4 (40) | 0 | 15/25 (60) | |||
| 18. | Cefotaxime | Watch | Injection | 250 mg, 500 mg, 1 g | S, T | -/4 (100)/A | 7 (70) | 2 (100) | 14/18 (77.8) |
| 19. | Ceftazidime | Watch | Injection | 250 mg, 1 g | S, T | -/1 (20)/NA | 6 (60) | 0 | 7/18 (38.9) |
| 20. | Piperacillin + tazobactam # | Watch | Injection | 1.125 g, 2.25 g, 4.5 g | T | -/-/A | 8 (80) | 1 (50) | 10/13 (76.9) |
| 21. | Clarithromycin # | Watch | Tablet | 250 mg, 500 mg | S, T | -/0/NA | 4 (40) | 0 | 4/18 (22.2) |
| 22. | Gentamicin | Access | Injection | 10, 40 mg/mL | P, S, T | 4 (57)/5 (100)/A | 8 (80) | 1 (50) | 22/25 (88) |
| Antibiotics included in selected (secondary) list but not in NLEM 2015 | |||||||||
| 23. | Cefuroxime # | Watch | Injection | 750 mg/1.5 g | S, T | -/0/NA | 4 (40) | 0 | 4/18 (22.2) |
| 24. | Levofloxacin | Watch | Tablet | 500 mg | S, T | -/2 (40)/A | 8 (80) | 2 (100) | 13/18 (72.2) |
| 25. | Norfloxacin | Watch | Tablet | 400 mg | P, S, T | 4 (57)/3 (60)/A | 8 (80) | 2 (100) | 18/25 (72) |
| 26. | Ofloxacin | Watch | Tablet | 100, 200, 400 mg | S, T | -/4 (80)/A | 8 (80) | 1 (50) | 21/25 (84) |
| 27. | Amikacin | Access | Injection | 100, 250, 500 mg/2 mL | P, S, T | 5 (71.4)/4 (80)/A | 10 (100) | 2 (100) | 22/25 (88) |
| 28. | Linezolid # | Reserve | Tablet | 600 mg | T | -/-/A | 5 (50) | 1 (50) | 7/13 (53.8) |
| Infusion | 2 mg/mL 100, 300 mL | T | -/-/A | 4 (40) | 0 | 5/13 (38.4) | |||
| 29. | Meropenem # | Reserve | Injection | 250 mg, 500 mg, 1 g | T | -/-/A | 7 (70) | 1 (100) | 9/13 (69.2) |
| S. No. | Name of Antimicrobial | Formulation | Strength | Healthcare Facility Level | Data on Availability | |||
|---|---|---|---|---|---|---|---|---|
| Public Sector | Private Sector | Other Sector | Total | |||||
| Primary Care (N = 7); Secondary (N = 5); Tertiary (N = 1) | Private Retailers (N = 10) | (AMRIT * Pharmacy; N = 2) | ||||||
| ANTHELMINTHICS | ||||||||
| 1. | Albendazole | Tablet | 400 mg | P, S, T | 7 (100)/5 (100)/A | 10 (100) | 2 (100) | 25/25 (100) |
| Suspension | 200 mg/5 mL | P, S, T | 7 (100)/4 (80)/A | 7 (70) | 2 (100) | 21/25 (84) | ||
| 2. | Mebendazole | Tablet | 100 mg | P, S, T | 0/0/NA | 3 (30) | 1 (50) | 4/25 (16) |
| 3. | Diethylcarbamazine # | Tablet | 50 mg, 100 mg | P, S, T | 0/0/NA | 3 (30) | 0 | 3/25 (12) |
| 4. | Praziquantel # | Tablet | 600 mg | S, T | -/0/NA | 0 | 0 | 0 |
| 5. | Ivermectin #$ | Tablet | 6 mg | P, S, T | 3 (42.8)/4 (80)/A | 9 (90) | 1 (50) | 18/25 (76) |
| ANTIVIRALS | ||||||||
| 6. | Acyclovir | Tablet | 200 mg, 400 mg | P, S, T | 7 (100)/5 (100)/A | 10 (100) | 2 (100) | 25/25 (100) |
| Injection | 250 mg, 500 mg | S, T | -/5 (100)/A | 7 (70) | 2 (100) | 15/18 (83.3) | ||
| Suspension | 400 mg/5 mL | T | -/-/NA | 2 (20) | 0 | 2/13 (15.4) | ||
| 7. | Ganciclovir # | Capsule | 250 mg | S, T | -/0/NA | 1 (10) | 0 | 1/18 (5.6) |
| Injection | 500 mg | S, T | -/0/NA | 1 (10) | 0 | 1/18 (5.6) | ||
| 8. | Entecavir # | Tablet | 0.5 mg, 1 mg | S, T | -/0/NA | 1 (10) | 0 | 1/18 (5.6) |
| 9. | Pegylated IFN α 2a # | Injection | 180 µg | S, T | -/0/NA | 0 | 0 | 0 |
| 10. | Pegylated IFN α 2b # | Injection | 80, 100, 120 µg | S, T | -/0/NA | 0 | 0 | 0 |
| 11. | Ribavirin # | Capsule | 200 mg | S, T | -/4 (80)/A | 1 (10) | 0 | 6/18 (33.3) |
| 12. | Sofosbuvir # | Tablet | 400 mg | S, T | -/4 (80)/A | 1 (10) | 0 | 6/18 (33.3) |
| 13. | Tenofovir # | Tablet | 300 mg | S, T | -/3 (60)/A | 1 (10) | 0 | 5/18 (27.8) |
| 14. | Oseltamivir #$ | Tablet | 75 mg | P, S, T | 5 (71.4)/4 (80)/A | 9 (90) | 1 (50) | 20/25 (80) |
| Syrup | 6 mg/mL, 60 mL | P, S, T | 5 (71.4)/4 (80)/A | 9 (90) | 1 (50) | 20/25 (80) | ||
| ANTIFUNGALS | ||||||||
| 15. | Liposomal Amphotericin B | Injection | 50 mg/vial | S, T | -/2 (20)/NA | 2 (20) | 0 | 4/18 (22.2) |
| 16. | Clotrimazole | Pessary | 100 mg, 200 mg | P, S, T | 7 (100)/5 (100)/A | 8 (80) | 2 (100) | 23/25 (92) |
| 17. | Fluconazole | Tablet | 100, 150, 200, 400 mg | P, S, T | 6 (85.7)/5 (100)/A | 10 (100) | 2 (100) | 24/25 (96) |
| Injection | 2 mg/mL | T | -/-/A | 4 (40) | 1 (50) | 6/13 (46) | ||
| 18. | Griseofulvin | Tablet | 125, 250, 375 mg | P, S, T | 1 (14.2)/1 (20)/NA | 4 (40) | 0 | 6/25 (24) |
| 19. | Nystatin | Tablet | 5 Lac IU | P, S, T | 1 (14.2)/0/NA | 0 | 0 | 1/25 (4) |
| Pessary | 1 Lac IU | P, S, T | 1 (14.2)/0/NA | 0 | 0 | 1/25 (4) | ||
| 20. | Itraconazole #$ | Tablet | 200 mg | P, S, T | 6 (85.7)/5 (100)/A | 8 (80) | 2 (100) | 22/25 (88) |
| 21. | Voriconazole #$ | Tablet | 200 mg | T | -/-/A | 6 (60) | 1 (50) | 8/13 (61.5) |
| Injection | 200 mg | T | -/-/A | 5 (50) | 0 | 6/13 (46) | ||
| ANTIPROTOZOALS | ||||||||
| 22. | Diloxanide furoate # | Tablet | 500 mg | P, S, T | 0/0/NA | 1 (10) | 2 (100) | 3/25 (12) |
| 23. | Miltefosine # | Tablet | 10, 50 mg | P, S, T | 0/0/NA | 0 | 0 | 0 |
| 24. | Paromomycin # | Injection | 375 mg/mL | P, S, T | 0/0/NA | 0 | 0 | 0 |
| 25. | Artemether + Lumefantrine # | Tablet | 20 + 120 mg, 40 + 240 mg, 80 + 480 mg | P, S, T | 0/0/NA | 6 (60) | 0 | 6/25 (24) |
| Dry syrup | 20 + 120 mg/5 mL | P, S, T | 0/0/NA | 1 (10) | 0 | 1/25 (4) | ||
| 26. | Artesunate # | Injection | 60, 120 mg | P, S, T | 0/0/NA | 7 (70) | 1 (50) | 8/25 (32) |
| 27. | Artesunate + Sulfadoxine-Pyrimethamine # | Tablet | 25 mg + 250/12.5, 50 mg + 55/25 | P, S, T | 0/0/NA | 1 (10) | 0 | 1/25 (4) |
| 28. | Primaquine # | Tablet | 2.5, 7.5, 15 mg | P, S, T | 1 (14.2)/2 (40)/NA | 3 (30) | 0 | 6/25 (24) |
| 29. | Chloroquine # | Tablet | 150 mg | P, S, T | 3 (42.8)/2 (40)/NA | 8 (80) | 0 | 13/25 (52) |
| 30. | Clindamycin # | Capsule | 150, 300 mg | P, S, T | 1 (14.2)/1 (20)/NA | 6 (60) | 2 (100) | 10/25 (40) |
| 31. | Mefloquine # | Tablet | 250 mg | T | -/-/NA | 0 | 0 | 0 |
| 32. | Quinin e # | Tablet | 300 mg | P, S, T | 1 (14.2)/1 (20)/NA | 5 (50) | 0 | 7/25 (28) |
| Injection | 300 mg/mL | P, S, T | 0/0/NA | 3 (30) | 0 | 3/25 (12) | ||
| 33. | Pentamidine # | Injection | 200 mg | S, T | -/0/NA | 0 | 0 | 0 |
| 34. | Tinidazole $ | Tablet | 500 mg | P, S, T | 6 (85.7)/5 (100)/A | 9 (90) | 1 (50) | 22/25 (88) |
| Antibiotics | Anthelminthics | Antifungals | Antivirals | Antiprotozoals | Overall Availability in the Facility | |
|---|---|---|---|---|---|---|
| PRIMARY CARE | ||||||
| Facility 1 | 9 (60) | 1 (33.3) | 1 (20) | 1 (100) | 0 (0) | 35.3% |
| Facility 2 | 10 (66.7) | 1 (33.3) | 2 (40) | 1 (100) | 0 (0) | 41.2% |
| Facility 3 | 10 (66.7) | 1 (33.3) | 4 (80) | 1 (100) | 3 (30) | 55.9% |
| Facility 4 | 7 (46.7) | 1 (33.3) | 2 (40) | 1 (100) | 1 (10) | 35.3% |
| Facility 5 | 6 (40) | 1 (33.3) | 2 (40) | 1 (100) | 1 (10) | 32.3% |
| Facility 6 | 6 (40) | 1 (33.3) | 2 (40) | 1 (100) | 1 (10) | 32.3% |
| Facility 7 | 11 (73.3) | 1 (33.3) | 2 (40) | 1 (100) | 1 (10) | 47% |
| Overall availability in primary care | 56.2% | 33.3% | 42.8% | 100% | 10% | |
| SECONDARY CARE | ||||||
| Facility 1 | 13 (65) | 1 (25) | 2 (40) | 3 (42.8) | 0 (0) | 40.4% |
| Facility 2 | 14 (70) | 1 (25) | 3 (60) | 3 (42.8) | 3 (27.3) | 51% |
| Facility 3 | 10 (50) | 1 (25) | 2 (40) | 2 (28.6) | 1 (9) | 34% |
| Facility 4 | 15 (75) | 1 (25) | 3 (60) | 3 (42.8) | 1 (9) | 48.9% |
| Facility 5 | 13 (65) | 1 (25) | 2 (40) | 2 (28.6) | 0 (0) | 38.3% |
| Overall availability in secondary care | 65% | 25% | 48% | 37.1% | 9.1% | |
| TERTIARY CARE | ||||||
| Facility 1 | 14 (63.6) | 1 (25) | 2 (40) | 4 (57.1) | 0 (0) | 42% |
| Overall availability | 63.6% | 25% | 40% | 57.1% | 0% | |
| Total overall availability in the district | 60.8% | 28.9% | 44.6% | 48.9% | 8.7% | |
| Healthcare Level | Antibiotics | Anthelminthics | Antifungals | Antivirals | Antiprotozoals | Overall Availability in the Facility |
|---|---|---|---|---|---|---|
| Primary care | ||||||
| Facility 1 | 8 (72.7) | 1 (50) | 2 (66.7) | 2 (100) | 1 (100) | 72.2% |
| Facility 2 | 9 (81.8) | 2 (100) | 3 (100) | 2 (100) | 1 (100) | 88.9% |
| Facility 3 | 11 (100) | 2 (100) | 3 (100) | 2 (100) | 1 (100) | 100% |
| Facility 4 | 9 (81.8) | 1 (50) | 1 (33.3) | 1 (50) | 1 (100) | 61% |
| Facility 5 | 8 (72.7) | 1 (50) | 2 (66.7) | 1 (50) | 0 | 61% |
| Facility 6 | 8 (72.7) | 1 (50) | 2 (66.7) | 2 (100) | 1 (100) | 83.3% |
| Facility 7 | 11 (90.9) | 2 (100) | 3 (100) | 2 (100) | 1 (100) | 100% |
| Overall availability in primary care | 83% | 71.4% | 76.2% | 85.7% | 85.7% | |
| Secondary care | ||||||
| Facility 1 | 14 (87.5) | 2 (100) | 3 (75) | 2 (100) | 1 (100) | 87.5% |
| Facility 2 | 16 (100) | 2 (100) | 4 (100) | 2 (100) | 1 (100) | 100% |
| Facility 3 | 13 (81) | 2 (100) | 3 (75) | 1 (50) | 1 (100) | 79.2% |
| Facility 4 | 14 (87.5) | 1 (25) | 4 (100) | 2 (100) | 1 (100) | 87.5% |
| Facility 5 | 15 (93.7) | 2 (100) | 3 (75) | 2 (100) | 1 (100) | 91.7% |
| Overall availability in secondary care | 90% | 90% | 85% | 90% | 100% | |
| Tertiary care | ||||||
| Facility 1 | 17 (80) | 2 (100) | 4 (80) | 2 (100) | 1 (100) | 89.6% |
| Overall availability in tertiary care | 85% | 100% | 80% | 100% | 100% | |
| Total overall availability in the district | 86.9% | 84% | 80.4% | 92% | 92.3% | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mittal, N.; Mittal, R.; Singh, S.; Godara, S. The Availability of Essential Antimicrobials in Public and Private Sector Facilities: A Cross-Sectional Survey in a District of North India. Antibiotics 2024, 13, 131. https://doi.org/10.3390/antibiotics13020131
Mittal N, Mittal R, Singh S, Godara S. The Availability of Essential Antimicrobials in Public and Private Sector Facilities: A Cross-Sectional Survey in a District of North India. Antibiotics. 2024; 13(2):131. https://doi.org/10.3390/antibiotics13020131
Chicago/Turabian StyleMittal, Niti, Rakesh Mittal, Sukhbir Singh, and Sushila Godara. 2024. "The Availability of Essential Antimicrobials in Public and Private Sector Facilities: A Cross-Sectional Survey in a District of North India" Antibiotics 13, no. 2: 131. https://doi.org/10.3390/antibiotics13020131
APA StyleMittal, N., Mittal, R., Singh, S., & Godara, S. (2024). The Availability of Essential Antimicrobials in Public and Private Sector Facilities: A Cross-Sectional Survey in a District of North India. Antibiotics, 13(2), 131. https://doi.org/10.3390/antibiotics13020131