
Long-Term Effects of a Stepwise, Multimodal, Non-Restrictive Antimicrobial Stewardship Programme for Reducing Broad-Spectrum Antibiotic Use in the ICU

 , , ,
, , ,
Abstract
1. Introduction
2. Results
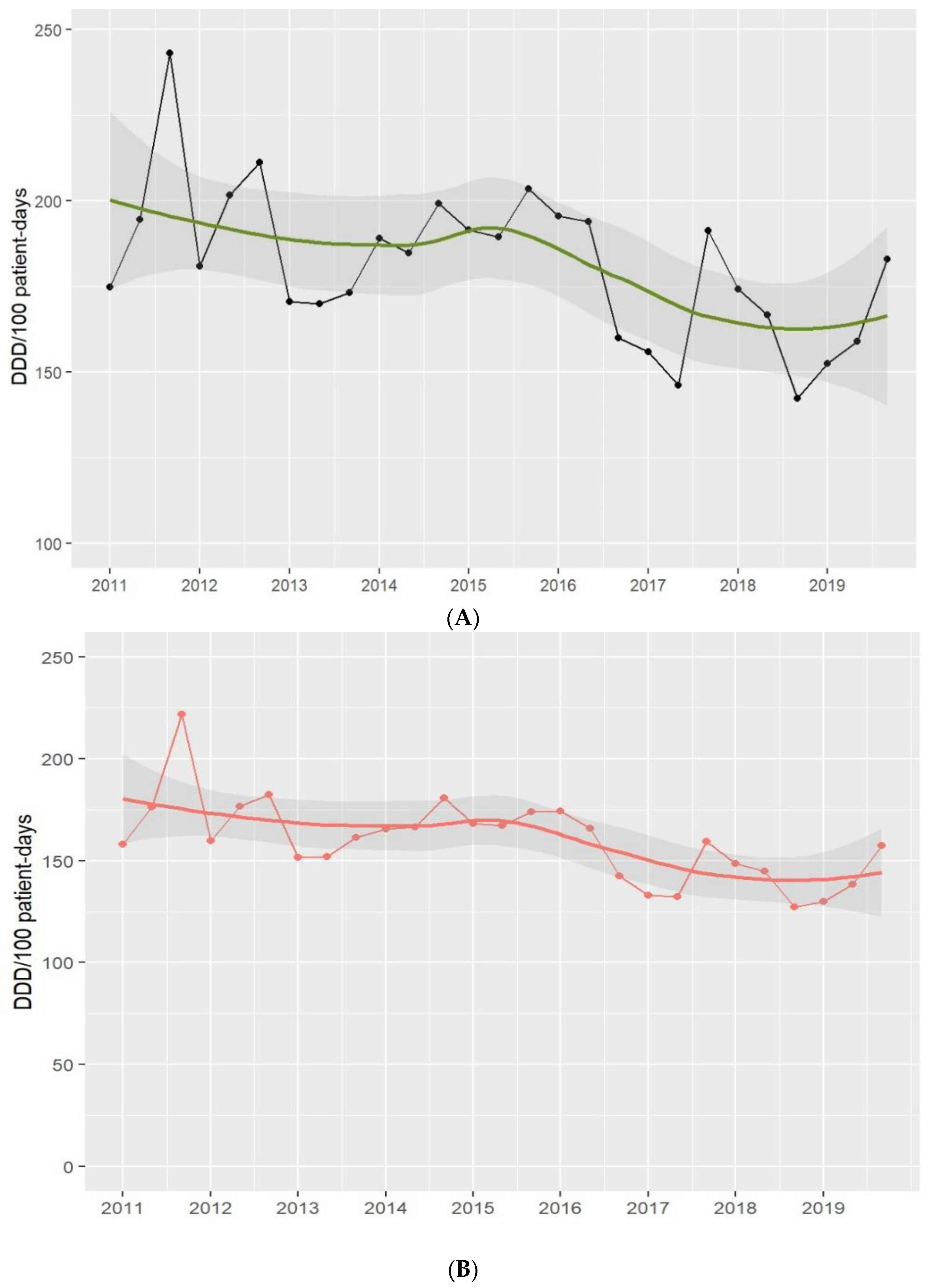
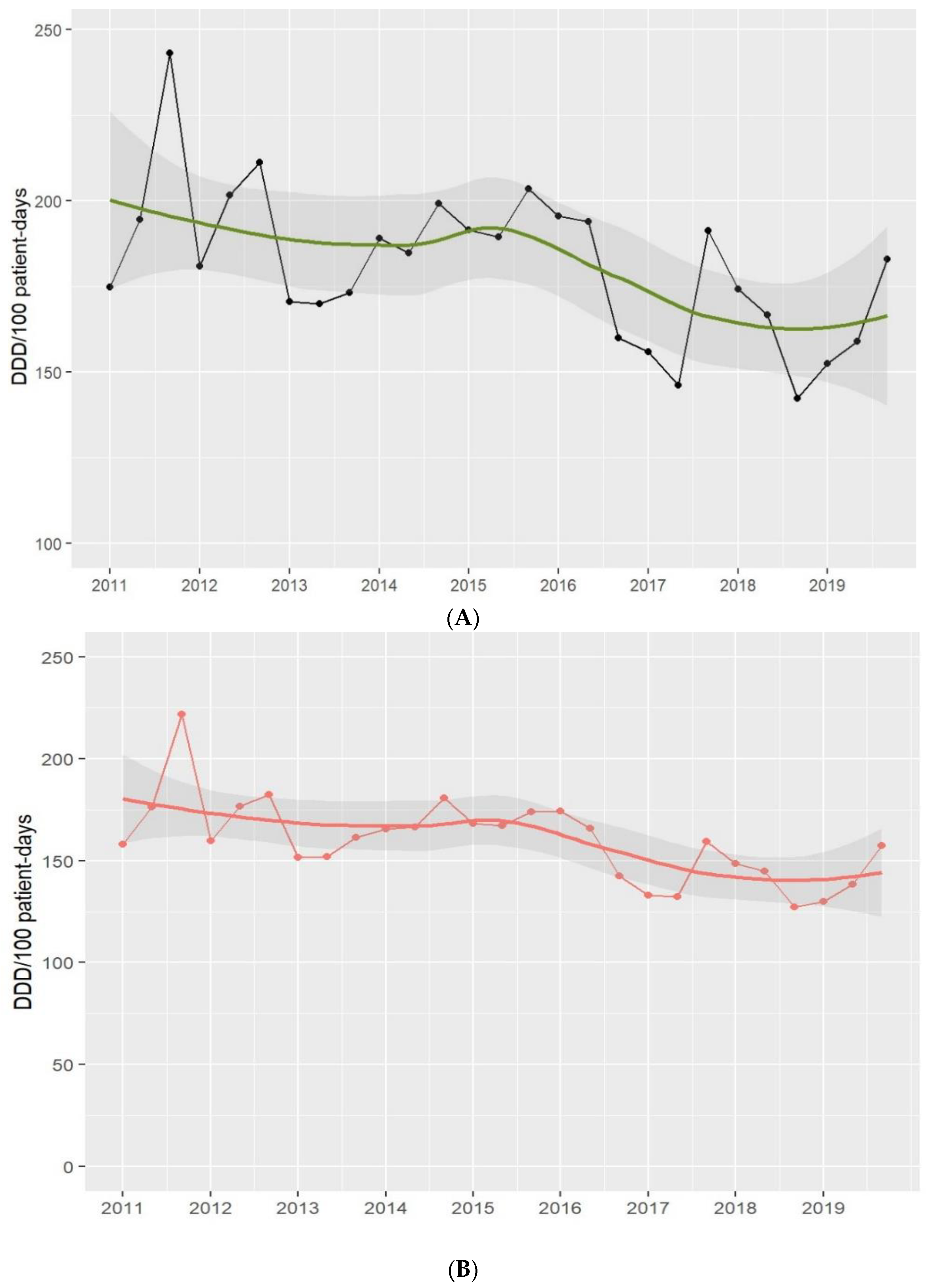
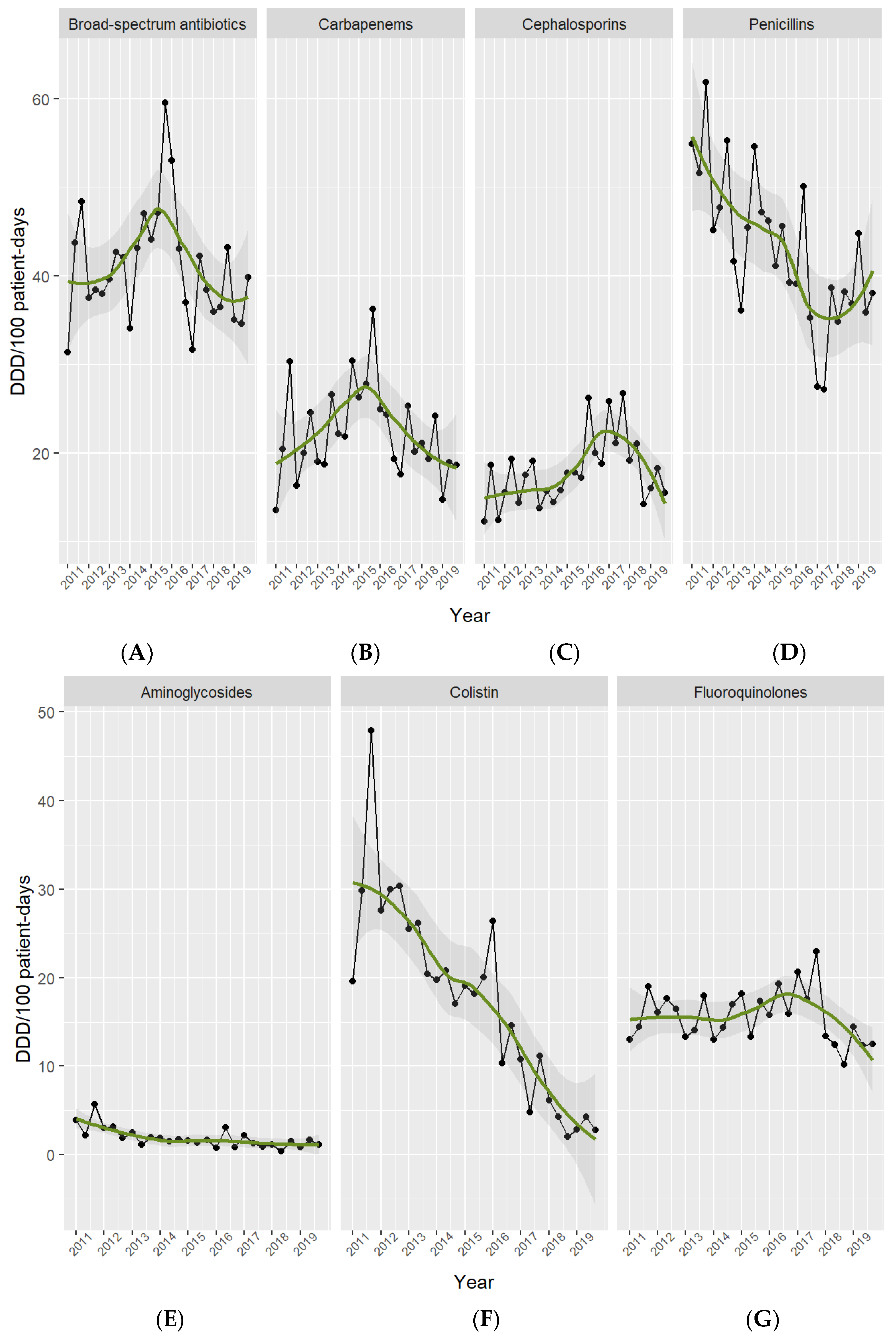
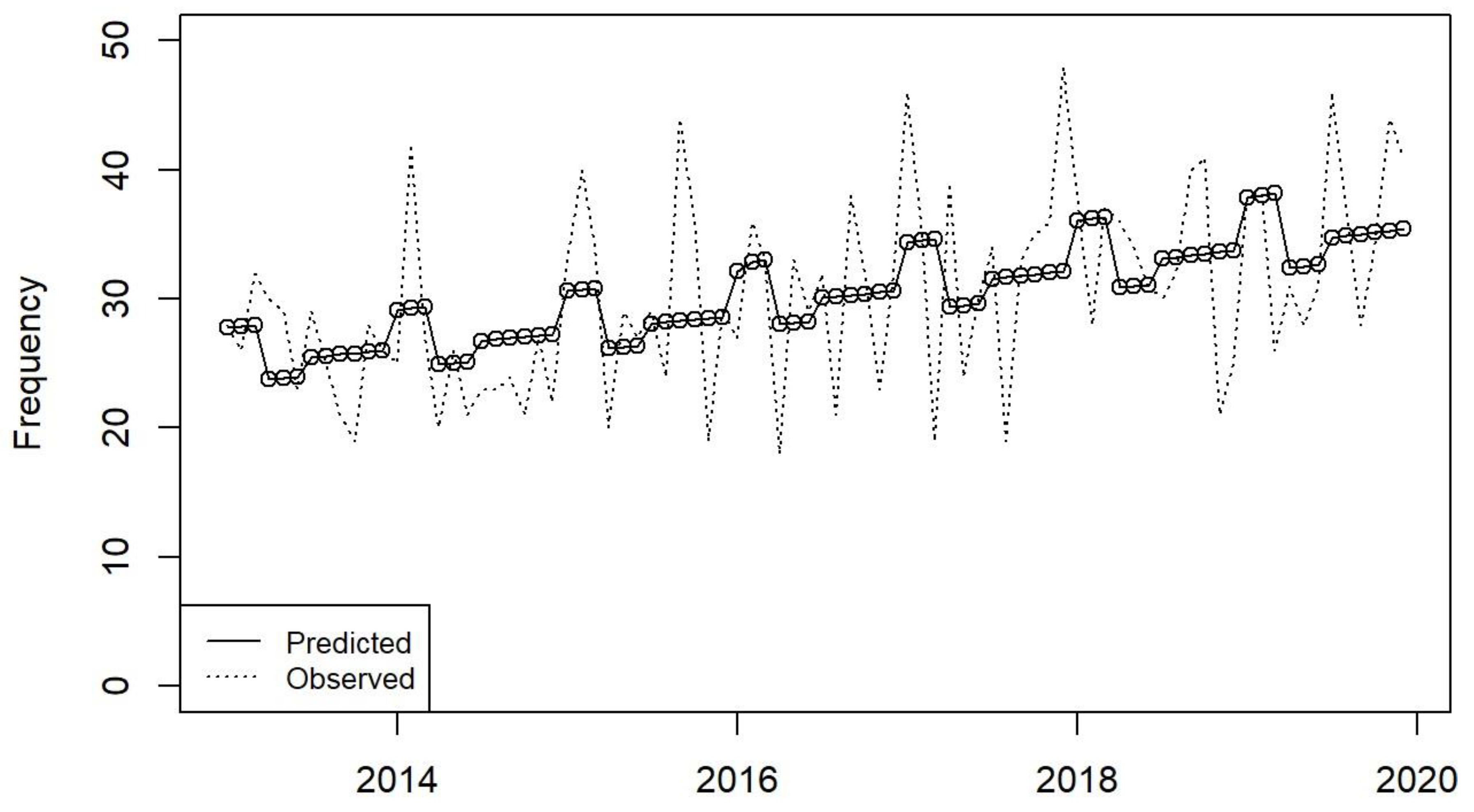
2.1. Antibiotic Use
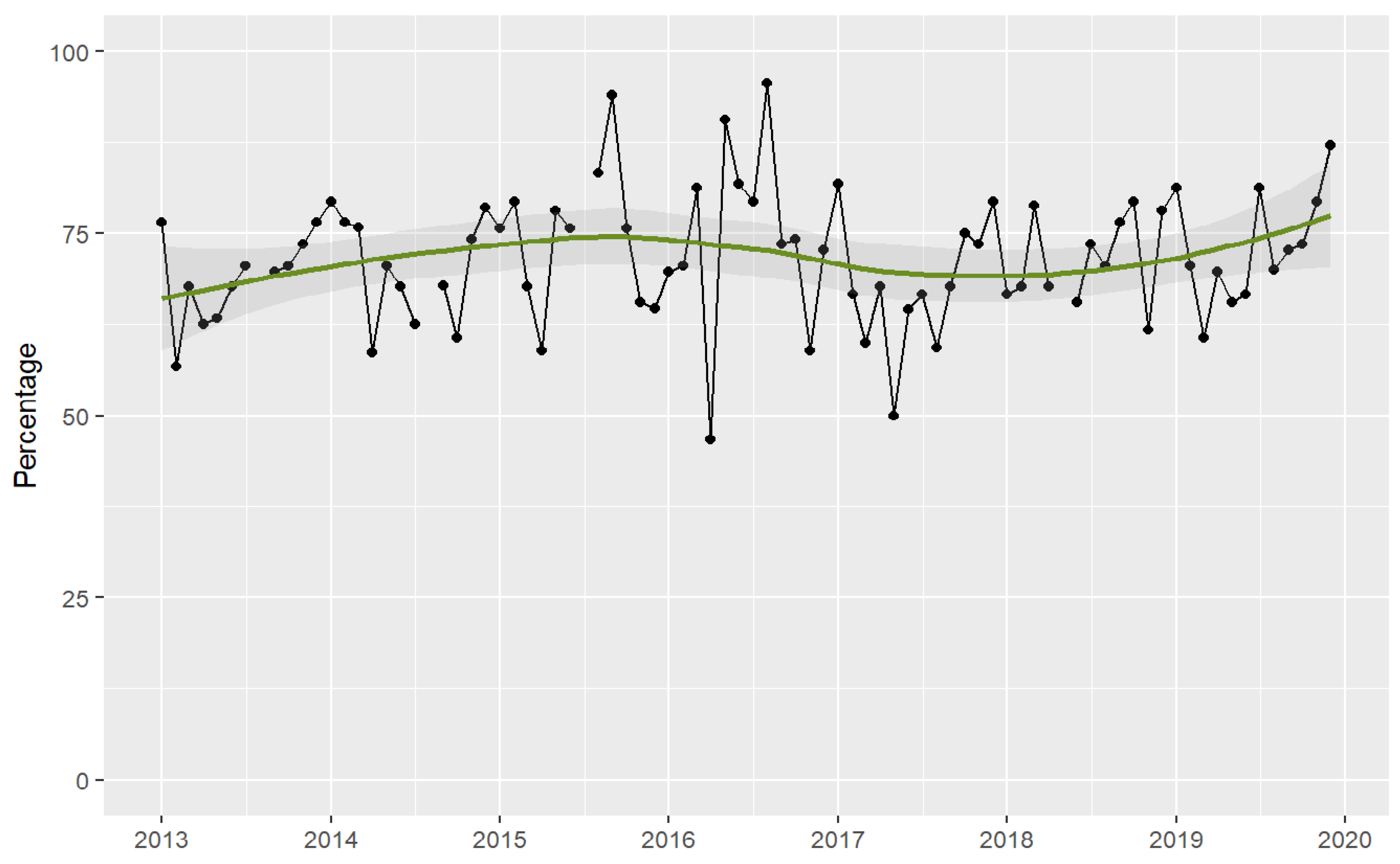
2.2. Appropriateness of Prescriptions
2.3. Outcomes
3. Discussion
4. Methods
4.1. Setting and Population
4.2. AMS Interventions
4.2.1. Guidelines for Educational Support
4.2.2. Microbiological Support
4.2.3. Optimisation of Antibiotic Dose
4.2.4. Setting up the AMS Team
4.2.5. Point-Prevalence Audit Surveys and Feedback
4.2.6. Electronic Support
4.2.7. Financial Incentives
4.3. Outcomes and Data Collection
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Action Plan on Antimicrobial Resistance; World Health Organization: Geneva, Switzerland, 2015; Available online: https://iris.who.int/bitstream/handle/10665/193736/9789241509763_eng.pdf?sequence=1 (accessed on 28 January 2024).
- World Health Organization. The Thirteenth General Programme of Work of WHO 2019–2023; World Health Organization: Geneva, Switzerland, 2019; Available online: https://iris.who.int/bitstream/handle/10665/324775/WHO-PRP-18.1-eng.pdf (accessed on 28 January 2024).
- Holmes, A.H.; Moore, L.S.; Sundsfjord, A.; Steinbakk, M.; Regmi, S.; Karkey, A.; Guerin, P.J.; Piddock, L.J. Understanding the mechanisms and drivers of antimicrobial resistance. Lancet 2016, 387, 176–187. [Google Scholar] [CrossRef]
- Dellit, T.H.; Owens, R.C.; McGowan, J.E., Jr.; Gerding, D.N.; Weinstein, R.A.; Burke, J.P.; Huskins, W.C.; Paterson, D. L; Infectious Diseases Society of America; Society for Healthcare Epidemiology of America; et al. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin Infect. Dis. 2007, 44, 159–177. [Google Scholar]
- World Health Organization. The Evolving Threat of Antimicrobial Resistance: Options for Action; World Health Organization: Geneva, Switzerland, 2012; Available online: https://www.jstor.org/stable/resrep48051 (accessed on 28 January 2024).
- Barlam, T.F.; Cosgrove, S.E.; Abbo, L.M.; MacDougall, C.; Schuetz, A.N.; Septimus, E.J.; Srinivasan, A.; Dellit, T.H.; Falck-Ytter, Y.T.; Fishman, N.O. Implementing an Antibiotic Stewardship Program: Guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin. Infect. Dis. 2016, 62, e51–e77. [Google Scholar] [CrossRef]
- Kumar, A.; Roberts, D.; Wood, K.E.; Light, B.; Parrillo, J.E.; Sharma, S.; Suppes, R.; Feinstein, D.; Zanotti, S.; Taiberg, L.; et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit. Care Med. 2006, 34, 1589–1596. [Google Scholar] [CrossRef]
- Kumar, A.; Ellis, P.; Arabi, Y.; Roberts, D.; Light, B.; Parrillo, J.E.; Dodek, P.; Wood, G.; Kumar, A.; Cooperative Antimicrobial Therapy of Septic Shock Database Research Group; et al. Initiation of inappropriate antimicrobial therapy results in a five fold reduction of survival in human septic shock. Chest 2009, 136, 1237–1248. [Google Scholar] [CrossRef]
- Fraimow, H.S. Chipping away at unnecessary antibiotic use in the ICU, one day and one study at a time. Crit. Care Med. 2013, 41, 2447–2448. [Google Scholar] [CrossRef]
- Levin, P.D.; Idrees, S.; Sprung, C.L.; Weissman, C.; Weiss, Y.; Moses, A.E.; Benenson, S. Antimicrobial use in the ICU: Indications and accuracy--an observational trial. J. Hosp. Med. 2012, 7, 672–678. [Google Scholar] [CrossRef] [PubMed]
- Kaki, R.; Elligsen, M.; Walker, S.; Simor, A.; Palmay, L.; Daneman, N. Impact of antimicrobial stewardship in critical care: A systematic review. J. Antimicrob. Chemother 2011, 66, 1223–1230. [Google Scholar] [CrossRef] [PubMed]
- Peña, C.; Pujol, M.; Ardanuy, C.; Ricart, A.; Pallares, R.; Liñares, J.; Ariza, J.; Gudiol, F. Epidemiology and successful control of a large outbreak due to Klebsiella pneumoniae producing extended-spectrum beta-lactamases. Antimicrob. Agents Chemother. 1998, 42, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Davey, P.; Marwick, C.A.; Scott, C.L.; Charani, E.; McNeil, K.; Brown, E.; Gould, I.M.; Ramsay, C.R.; Michie, S. Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane Database Syst. Rev. 2017, 2, CD003543. [Google Scholar] [CrossRef]
- Steinberg, M.; Dresser, L.D.; Daneman, N.; Smith, O.M.; Matte, A.; Marinoff, N.; Bell, C.M.; Morris, A.M. A National Survey of Critical Care Physicians’ Knowledge, Attitudes, and Perceptions of Antimicrobial Stewardship Programs. J. Intensive Care Med. 2016, 31, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Tamma, P.D.; Avdic, E.; Keenan, J.F.; Zhao, Y.; Anand, G.; Cooper, J.; Dezube, R.; Hsu, S.; Cosgrove, S.E. What Is the More Effective Antibiotic Stewardship Intervention: Preprescription Authorization or Postprescription Review with Feedback? Clin. Infect. Dis. 2017, 64, 537–543. [Google Scholar] [PubMed]
- Perozziello, A.; Lescure, F.X.; Truel, A.; Routelous, C.; Vaillant, L.; Yazdanpanah, Y.; Lucet, J.C.; Burdet, C.; Kardas, L.; Lepeule, R.; et al. Prescribers’ experience and opinions on antimicrobial stewardship programmes in hospitals: A French nationwide survey. J. Antimicrob. Chemother. 2019, 74, 2451–2458. [Google Scholar] [CrossRef] [PubMed]
- Salsgiver, E.; Bernstein, D.; Simon, M.S.; Eiras, D.P.; Greendyke, W.; Kubin, C.J.; Mehta, M.; Nelson, B.; Loo, A.; Ramos, L.G.; et al. Knowledge, Attitudes, and Practices Regarding Antimicrobial Use and Stewardship Among Prescribers at Acute-Care Hospitals. Infect. Control Hosp. Epidemiol. 2018, 39, 316–322. [Google Scholar] [CrossRef] [PubMed]
- Charani, E.; Castro-Sanchez, E.; Sevdalis, N.; Kyratsis, Y.; Drumright, L.; Shah, N.; Holmes, A. Understanding the determinants of antimicrobial prescribing within hospitals: The role of “prescribing etiquette”. Clin. Infect. Dis. 2013, 57, 188–196. [Google Scholar] [CrossRef]
- DiazGranados, C.A. Prospective audit for antimicrobial stewardship in intensive care: Impact on resistance and clinical outcomes. Am. J. Infect. Control 2012, 40, 526–529. [Google Scholar] [CrossRef]
- Elligsen, M.; Walker, S.A.N.; Pinto, R.; Simor, A.; Mubareka, S.; Rachlis, A.; Allen, V.; Daneman, N. Audit and feedback to reduce broad-spectrum antibiotic use among intensive care unit patients: A controlled interrupted time series analysis. Infect. Control Hosp. Epidemiol. 2012, 33, 354–361. [Google Scholar] [CrossRef]
- Rimawi, R.H.; Mazer, M.A.; Siraj, D.S.; Gooch, M.; Cook, P.P. Impact of regular collaboration between infectious diseases and critical care practitioners on antimicrobial utilization and patient outcome. Crit. Care Med. 2013, 41, 2099–2107. [Google Scholar] [CrossRef]
- Taggart, L.R.; Leung, E.; Muller, M.P.; Matukas, L.M.; Daneman, N. Differential outcome of an antimicrobial stewardship audit and feedback program in two intensive care units: A controlled interrupted time series study. BMC Infect. Dis. 2015, 15, 480. [Google Scholar] [CrossRef]
- Fleming, D.; Ali, K.F.; Matelski, J.; D’Sa, R.; Powis, J. When Antimicrobial Stewardship Isn’t Watching: The Educational Impact of Critical Care Prospective Audit and Feedback. Open Forum Infect. Dis. 2016, 3, ofw115. [Google Scholar] [CrossRef]
- Shaw, E.; Gavaldà, L.; Càmara, J.; Gasull, R.; Gallego, S.; Tubau, F.; Granada, R.; Ciercoles, P.; Dominguez, M.; Mañez, R.; et al. Control of endemic multidrug-resistant Gram-negative bacteria after removal of sinks and implementing a new water-safe policy in an intensive care unit. J. Hosp. Infect. 2018, 98, 275–281. [Google Scholar] [CrossRef]
- Álvarez-Lerma, F.; Grau, S.; Echeverría-Esnal, D.; Martínez-Alonso, M.; Gracia-Arnillas, M.P.; Horcajada, J.P.; Masclans, J.R. A before-and-after study of the effectiveness of antimicrobial stewardship program in critical care. Antimicrob. Agents Chemother. 2018, 62, e01825-17. [Google Scholar] [CrossRef]
- Morris, A.M.; Bai, A.; Burry, L.; Dresser, L.D.; Ferguson, N.D.; Lapinsky, S.E.; Lazar, N.M.; McIntyre, M.; Matelski, J.; Minnema, B.; et al. Long-term effect of phased implementation of antimicrobial stewardship in academic ICUs: 2007–2015. Crit. Care Med. 2019, 47, 159–166. [Google Scholar] [CrossRef]
- Adhikari, S.; Piza, M.; Taylor, P.; Deshpande, K.; Lam, D.; Konecny, P. Sustained multimodal antimicrobial stewardship in an Australian tertiary intensive care unit from 2008–2015: An interrupted time-series analysis. Int. J. Antimicrob. Agents 2018, 51, 620–628. [Google Scholar] [CrossRef]
- Onorato, L.; Macera, M.; Calò, F.; Monari, C.; Russo, F.; Iovene, M.; Signoriello, G.; Annibale, R.; Pace, M.; Aurilio, C.; et al. The effect of an antimicrobial stewardship programme in two intensive care units of a teaching hospital: An interrupted time series analysis. Clin. Microbiol. Infect. 2020, 26, e1–e782. [Google Scholar] [CrossRef] [PubMed]
- Seidelman, J.L.; Turner, N.A.; Wrenn, R.H.; Sarubbi, C.; Anderson, D.J.; Sexton, D.J.; Moehring, R.W. Impact of Antibiotic Stewardship Rounds in the Intensive Care Setting: A Prospective Cluster-Randomized Crossover Study. Clin. Infect. Dis. 2022, 74, 1986–1992. [Google Scholar] [CrossRef] [PubMed]
- Gavaldà, L.; Soriano, A.M.; Cámara, J.; Gasull, R.; Arch, O.; Ferrer, M.; Shaw, E.; Granada, R.M.; Dominguez, M.A.; Pujol, M. Control of endemic extensively drug-resistant Acinetobacter baumannii with a cohorting policy and cleaning procedures based on the 1 room, 1 wipe approach. Am. J. Infect. Control 2016, 44, 520–524. [Google Scholar] [CrossRef] [PubMed]
- Sikkens, J.J.; Van Agtmael, M.A.; Peters, E.J.; Lettinga, K.D.; Van Der Kuip, M.; Vandenbroucke-Grauls, C.M.; Wagner, C.; Kramer, M.H. Behavioral Approach to Appropriate Antimicrobial Prescribing in Hospitals: The Dutch Unique Method for Antimicrobial Stewardship (DUMAS) Participatory Intervention Study. JAMA Intern. Med. 2017, 177, 1130–1138. [Google Scholar] [CrossRef] [PubMed]
- Charani, E.; Edwards, R.; Sevdalis, N.; Alexandrou, B.; Sibley, E.; Mullett, D.; Franklin, B.D.; Holmes, A. Behavior change strategies to influence antimicrobial prescribing in acute care: A systematic review. Clin. Infect. Dis. 2011, 53, 651–662. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, P.J.; Rohailla, S.; Taggart, L.R.; Lightfoot, D.; Havey, T.; Daneman, N.; Lowe, C.; Muller, M.P. Antimicrobial stewardship and intensive care unit mortality: A systematic review. Clin. Infect. Dis. 2019, 68, 748–756. [Google Scholar] [CrossRef] [PubMed]
- Willemsen, I.; Groenhuijzen, A.; Bogaers, D.; Stuurman, A.; van Keulen, P.; Kluytmans, J. Appropriateness of antimicrobial therapy measured by repeated prevalence surveys. Antimicrob. Agents Chemother. 2007, 51, 864–867. [Google Scholar] [CrossRef] [PubMed]
- WHO Collaborating Centre for Drug Statistics Methodology. Guidelines for ATC Classification and DDD Assignment 2023; WHO Collaborating Centre for Drug Statistics Methodology: Oslo, Norway, 2022; Available online: https://www.whocc.no/filearchive/publications/2023_guidelines_web.pdf (accessed on 18 December 2023).



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | |
|---|---|---|---|---|---|---|---|---|
| Update of guidelines and education | ||||||||
| Microbiological support | ||||||||
| Setting up daily AMS team rounds | ||||||||
| Point-prevalence audit surveys and feedback | ||||||||
| ICU doctors added to the AMS team | ||||||||
| TDM and dose adjustment of ß-lactams | ||||||||
| Electronic flag reminder for prescription day | ||||||||
| Annual financial incentives |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ronda, M.; Gumucio-Sanguino, V.D.; Shaw, E.; Granada, R.; Tubau, F.; Santafosta, E.; Sabater, J.; Esteve, F.; Tebé, C.; Mañez, R.; et al. Long-Term Effects of a Stepwise, Multimodal, Non-Restrictive Antimicrobial Stewardship Programme for Reducing Broad-Spectrum Antibiotic Use in the ICU. Antibiotics 2024, 13, 132. https://doi.org/10.3390/antibiotics13020132
Ronda M, Gumucio-Sanguino VD, Shaw E, Granada R, Tubau F, Santafosta E, Sabater J, Esteve F, Tebé C, Mañez R, et al. Long-Term Effects of a Stepwise, Multimodal, Non-Restrictive Antimicrobial Stewardship Programme for Reducing Broad-Spectrum Antibiotic Use in the ICU. Antibiotics. 2024; 13(2):132. https://doi.org/10.3390/antibiotics13020132
Chicago/Turabian StyleRonda, Mar, Victor Daniel Gumucio-Sanguino, Evelyn Shaw, Rosa Granada, Fe Tubau, Eva Santafosta, Joan Sabater, Francisco Esteve, Cristian Tebé, Rafael Mañez, and et al. 2024. "Long-Term Effects of a Stepwise, Multimodal, Non-Restrictive Antimicrobial Stewardship Programme for Reducing Broad-Spectrum Antibiotic Use in the ICU" Antibiotics 13, no. 2: 132. https://doi.org/10.3390/antibiotics13020132
APA StyleRonda, M., Gumucio-Sanguino, V. D., Shaw, E., Granada, R., Tubau, F., Santafosta, E., Sabater, J., Esteve, F., Tebé, C., Mañez, R., Carratalà, J., Puig-Asensio, M., Cobo-Sacristán, S., & Padullés, A. (2024). Long-Term Effects of a Stepwise, Multimodal, Non-Restrictive Antimicrobial Stewardship Programme for Reducing Broad-Spectrum Antibiotic Use in the ICU. Antibiotics, 13(2), 132. https://doi.org/10.3390/antibiotics13020132