
Susceptibility of Actinobacillus pleuropneumoniae, Pasteurella multocida and Streptococcus suis Isolated from Pigs in Hungary between 2018 and 2021

 ,
,  ,
,
Abstract
1. Introduction
2. Results
2.1. Susceptibility of Actinobacillus pleuropneumoniae Isolates
2.2. Susceptibility of Pasteurella multocida Isolates
2.3. Susceptibility of Streptococcus suis Isolates
3. Discussion
3.1. Susceptibility of Actinobacillus pleuropneumoniae Isolates
3.2. Susceptibility of Pasteurella multocida Isolates
3.3. Susceptibility of Streptococcus suis Isolates
4. Materials and Methods
4.1. Laboratory Participants and Isolate Characterisation
4.2. Determination of Minimal Inhibitory Concentration Values
4.3. Number of Isolates Tested per Antibiotic
4.4. Data Analysis
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Petri, F.A.M.; Ferreira, G.C.; Arruda, L.P.; Malcher, C.S.; Storino, G.Y.; Almeida, H.M.d.S.; Sonalio, K.; Silva, D.G.D.; Oliveira, L.G.D. Associations between Pleurisy and the Main Bacterial Pathogens of the Porcine Respiratory Diseases Complex (PRDC). Animals 2023, 13, 1493. [Google Scholar] [CrossRef]
- Thacker, E.L. Immunology of the Porcine Respiratory Disease Complex. Vet. Clin. N. Am. Food Anim. Pract. 2001, 17, 551–565. [Google Scholar] [CrossRef] [PubMed]
- Chae, C. Porcine Respiratory Disease Complex: Interaction of Vaccination and Porcine Circovirus Type 2, Porcine Reproductive and Respiratory Syndrome Virus, and Mycoplasma hyopneumoniae. Vet. J. Lond. Engl. 1997 2016, 212, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Sargeant, J.M.; Bergevin, M.D.; Churchill, K.; Dawkins, K.; Deb, B.; Dunn, J.; Hu, D.; Moody, C.; O’Connor, A.M.; O’Sullivan, T.L.; et al. A Systematic Review of the Efficacy of Antibiotics for the Prevention of Swine Respiratory Disease. Anim. Health Res. Rev. 2019, 20, 291–304. [Google Scholar] [CrossRef]
- Saade, G.; Deblanc, C.; Bougon, J.; Marois-Créhan, C.; Fablet, C.; Auray, G.; Belloc, C.; Leblanc-Maridor, M.; Gagnon, C.A.; Zhu, J.; et al. Coinfections and Their Molecular Consequences in the Porcine Respiratory Tract. Vet. Res. 2020, 51, 80. [Google Scholar] [CrossRef]
- El Garch, F.; de Jong, A.; Simjee, S.; Moyaert, H.; Klein, U.; Ludwig, C.; Marion, H.; Haag-Diergarten, S.; Richard-Mazet, A.; Thomas, V.; et al. Monitoring of Antimicrobial Susceptibility of Respiratory Tract Pathogens Isolated from Diseased Cattle and Pigs across Europe, 2009–2012: VetPath Results. Vet. Microbiol. 2016, 194, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Antimicrobial Wild Type Distributions of Microorganisms, EUCAST. Available online: https://mic.eucast.org/search/?search%5Bmethod%5D=mic&search%5Bantibiotic%5D=-1&search%5Bspecies%5D=-1&search%5Bdisk_content%5D=-1&search%5Blimit%5D=50 (accessed on 17 April 2023).
- Holmer, I.; Salomonsen, C.M.; Jorsal, S.E.; Astrup, L.B.; Jensen, V.F.; Høg, B.B.; Pedersen, K. Antibiotic Resistance in Porcine Pathogenic Bacteria and Relation to Antibiotic Usage. BMC Vet. Res. 2019, 15, 449. [Google Scholar] [CrossRef]
- Mader, R.; Muñoz Madero, C.; Aasmäe, B.; Bourély, C.; Broens, E.M.; Busani, L.; Callens, B.; Collineau, L.; Crespo-Robledo, P.; Damborg, P.; et al. Review and Analysis of National Monitoring Systems for Antimicrobial Resistance in Animal Bacterial Pathogens in Europe: A Basis for the Development of the European Antimicrobial Resistance Surveillance Network in Veterinary Medicine (EARS-Vet). Front. Microbiol. 2022, 13, 838490. [Google Scholar] [CrossRef]
- Toutain, P.-L.; Pelligand, L.; Lees, P.; Bousquet-Mélou, A.; Ferran, A.A.; Turnidge, J.D. The Pharmacokinetic/Pharmacodynamic Paradigm for Antimicrobial Drugs in Veterinary Medicine: Recent Advances and Critical Appraisal. J. Vet. Pharmacol. Ther. 2021, 44, 172–200. [Google Scholar] [CrossRef]
- Kowalska-Krochmal, B.; Dudek-Wicher, R. The Minimum Inhibitory Concentration of Antibiotics: Methods, Interpretation, Clinical Relevance. Pathogens 2021, 10, 165. [Google Scholar] [CrossRef]
- Kardos, G.; Sárközi, R.; Laczkó, L.; Marton, S.; Makrai, L.; Bányai, K.; Fodor, L. Genetic Diversity of Actinobacillus Pleuropneumoniae Serovars in Hungary. Vet. Sci. 2022, 9, 511. [Google Scholar] [CrossRef] [PubMed]
- Burch, D.G.S.; Sperling, D. Amoxicillin—Current Use in Swine Medicine. J. Vet. Pharmacol. Ther. 2018, 41, 356–368. [Google Scholar] [CrossRef]
- European Medicines Agency Categorisation of Antibiotics in the European Union 2019. Available online: https://www.ema.europa.eu/en/documents/report/categorisation-antibiotics-european-union-answer-request-european-commission-updating-scientific_en.pdf (accessed on 17 April 2023).
- Chander, Y.; Oliveira, S.; Goyal, S.M. Characterisation of Ceftiofur Resistance in Swine Bacterial Pathogens. Vet. J. 2011, 187, 139–141. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Wu, X.; Huang, Z.; Zhang, N.; Wu, Y.; Cai, Q.; Shen, X.; Ding, H. Pharmacokinetic/Pharmacodynamic Assessment of Cefquinome against Actinobacillus Pleuropneumoniae in a Piglet Tissue Cage Infection Model. Vet. Microbiol. 2018, 219, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Xie, H.; Wang, H.; Ding, H.; Zhang, G.; Hu, J. Kill Rate and Evaluation of Ex Vivo PK/PD Integration of Cefquinome against Actinobacillus Pleuropneumoniae. Front. Vet. Sci. 2021, 8, 751957. [Google Scholar] [CrossRef]
- Tóth, A.G.; Csabai, I.; Maróti, G.; Jerzsele, Á.; Dubecz, A.; Patai, Á.V.; Judge, M.F.; Nagy, S.Á.; Makrai, L.; Bányai, K.; et al. A Glimpse of Antimicrobial Resistance Gene Diversity in Kefir and Yoghurt. Sci. Rep. 2020, 10, 22458. [Google Scholar] [CrossRef]
- Cheng, D.; Feng, Y.; Liu, Y.; Xue, J.; Li, Z. Dynamics of Oxytetracycline, Sulfamerazine, and Ciprofloxacin and Related Antibiotic Resistance Genes during Swine Manure Composting. J. Environ. Manag. 2019, 230, 102–109. [Google Scholar] [CrossRef]
- Mazurek, J.; Bok, E.; Stosik, M.; Baldy-Chudzik, K. Antimicrobial Resistance in Commensal Escherichia Coli from Pigs during Metaphylactic Trimethoprim and Sulfamethoxazole Treatment and in the Post-Exposure Period. Int. J. Environ. Res. Public Health 2015, 12, 2150–2163. [Google Scholar] [CrossRef]
- Yang, F.; Liu, H.W.; Li, M.; Ding, H.Z.; Huang, X.H.; Zeng, Z.L. Use of a Monte Carlo Analysis within a Physiologically Based Pharmacokinetic Model to Predict Doxycycline Residue Withdrawal Time in Edible Tissues in Swine. Food Addit. Contam. Part A 2012, 29, 73–84. [Google Scholar] [CrossRef]
- Dorey, L.; Pelligand, L.; Cheng, Z.; Lees, P. Pharmacokinetic/Pharmacodynamic Integration and Modelling of Florfenicol for the Pig Pneumonia Pathogens Actinobacillus Pleuropneumoniae and Pasteurella Multocida. PLoS ONE 2017, 12, e0177568. [Google Scholar] [CrossRef]
- Xiong, J.; Zhu, Q.; Yang, S.; Zhao, Y.; Cui, L.; Zhuang, F.; Qiu, Y.; Cao, J. Comparison of Pharmacokinetics of Tilmicosin in Healthy Pigs and Pigs Experimentally Infected with Actinobacillus Pleuropneumoniae. N. Z. Vet. J. 2019, 67, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Zhang, H.; Li, M.; Ahmad, I.; Wang, Y.; Yuan, Z. Pharmacokinetic-Pharmacodynamic Modeling of Tylosin against Streptococcus suis in Pigs. BMC Vet. Res. 2018, 14, 319. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Zhang, G.; Wang, Q.; Liu, W.; Huang, Y.; Yu, P.; Li, Y.; Ding, H.; Fang, B. Pharmacokinetic/Pharmacodynamic Modeling of Tulathromycin against Pasteurella Multocida in a Porcine Tissue Cage Model. Front. Pharmacol. 2017, 8, 392. [Google Scholar] [CrossRef] [PubMed]
- Bladek, T.; Posyniak, A.; Jablonski, A.; Gajda, A. Pharmacokinetics of Tulathromycin in Edible Tissues of Healthy and Experimentally Infected Pigs with Actinobacillus Pleuropneumoniae. Food Addit. Contam. Part A 2015, 32, 1823–1832. [Google Scholar] [CrossRef]
- Nielsen, P.; Gyrd-Hansen, N. Bioavailability of Spiramycin and Lincomycin after Oral Administration to Fed and Fasted Pigs. J. Vet. Pharmacol. Ther. 1998, 21, 251–256. [Google Scholar] [CrossRef]
- Pallarés, F.J.; Lasa, C.; Roozen, M.; Ramis, G. Use of Tylvalosin in the Control of Porcine Enzootic Pneumonia. Vet. Rec. Open 2015, 2, e000079. [Google Scholar] [CrossRef]
- Albert, E.; Sipos, R.; Perreten, V.; Tóth, Á.; Ungvári, E.; Papp, M.; Dán, Á.; Biksi, I. High Prevalence of Livestock-Associated Methicillin-Resistant Staphylococcus aureus in Hungarian Pig Farms and Genomic Evidence for the Spillover of the Pathogen to Humans. Transbound. Emerg. Dis. 2023, 2023, 5540019. [Google Scholar] [CrossRef]
- Somogyi, Z.; Mag, P.; Kovács, D.; Kerek, Á.; Szabó, P.; Makrai, L.; Jerzsele, Á. Synovial and Systemic Pharmacokinetics of Florfenicol and PK/PD Integration against Streptococcus suis in Pigs. Pharmaceutics 2022, 14, 109. [Google Scholar] [CrossRef]
- Somogyi, Z.; Mag, P.; Simon, R.; Kerek, Á.; Szabó, P.; Albert, E.; Biksi, I.; Jerzsele, Á. Pharmacokinetics and Pharmacodynamics of Florfenicol in Plasma and Synovial Fluid of Pigs at a Dose of 30 Mg/Kgbw Following Intramuscular Administration. Antibiotics 2023, 12, 758. [Google Scholar] [CrossRef]
- Grégoire, N.; Aranzana-Climent, V.; Magréault, S.; Marchand, S.; Couet, W. Clinical Pharmacokinetics and Pharmacodynamics of Colistin. Clin. Pharmacokinet. 2017, 56, 1441–1460. [Google Scholar] [CrossRef]
- Rhouma, M.; Beaudry, F.; Thériault, W.; Letellier, A. Colistin in Pig Production: Chemistry, Mechanism of Antibacterial Action, Microbial Resistance Emergence, and One Health Perspectives. Front. Microbiol. 2016, 7, 1789. [Google Scholar] [CrossRef]
- Rhouma, M.; Beaudry, F.; Thériault, W.; Bergeron, N.; Beauchamp, G.; Laurent-Lewandowski, S.; Fairbrother, J.M.; Letellier, A. In Vivo Therapeutic Efficacy and Pharmacokinetics of Colistin Sulfate in an Experimental Model of Enterotoxigenic Escherichia Coli Infection in Weaned Pigs. Vet. Res. 2016, 47, 58. [Google Scholar] [CrossRef]
- Chen, T.; Xie, G.; Mi, J.; Wen, X.; Cao, Z.; Ma, B.; Zou, Y.; Zhang, N.; Wang, Y.; Liao, X.; et al. Recovery of the Structure and Function of the Pig Manure Bacterial Community after Enrofloxacin Exposure. Microbiol. Spectr. 2022, 10, e02004-21. [Google Scholar] [CrossRef]
- De Smet, J.; Boyen, F.; Croubels, S.; Rasschaert, G.; Haesebrouck, F.; Temmerman, R.; Rutjens, S.; De Backer, P.; Devreese, M. The Impact of Therapeutic-Dose Induced Intestinal Enrofloxacin Concentrations in Healthy Pigs on Fecal Escherichia coli Populations. BMC Vet. Res. 2020, 16, 382. [Google Scholar] [CrossRef]
- González-Fandos, E.; Martínez-Laorden, A.; Abad-Fau, A.; Sevilla, E.; Bolea, R.; Serrano, M.J.; Mitjana, O.; Bonastre, C.; Laborda, A.; Falceto, M.V.; et al. Effect of Intramuscularly Administered Oxytetracycline or Enrofloxacin on Vancomycin-Resistant Enterococci, Extended Spectrum Beta-Lactamase- and Carbapenemase-Producing Enterobacteriaceae in Pigs. Animals 2022, 12, 622. [Google Scholar] [CrossRef]
- Kaspersen, H.; Urdahl, A.M.; Grøntvedt, C.A.; Gulliksen, S.M.; Tesfamichael, B.; Slettemeås, J.S.; Norström, M.; Sekse, C. Actinobacillus pleuropneumoniae Eradication with Enrofloxacin May Lead to Dissemination and Long-Term Persistence of Quinolone Resistant Escherichia Coli in Pig Herds. Antibiotics 2020, 9, 910. [Google Scholar] [CrossRef]
- Matamoros, V.; Casas, M.E.; Pastor, E.; Tadić, Đ.; Cañameras, N.; Carazo, N.; Bayona, J.M. Effects of Tetracycline, Sulfonamide, Fluoroquinolone, and Lincosamide Load in Pig Slurry on Lettuce: Agricultural and Human Health Implications. Environ. Res. 2022, 215, 114237. [Google Scholar] [CrossRef]
- Yang, B.; Li, X.D.; Chen, X.; Hong, J.; Liu, C.; Zheng, J.P.; Ou, Z.Y.; Yu, D.J. PK/PD Modelling of Enrofloxacin against Glaesserella parasuis Infection in Pigs. J. Vet. Pharmacol. Ther. 2022, 45, 291–300. [Google Scholar] [CrossRef]
- CLSI. Performance Standards for Antimicrobial Disk Dilution Susceptibility Tests for Bacteria Isolated from Animals, 5th ed.; CLSI Supplement VET01S; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2020. [Google Scholar]
- 128/2009. (X. 6.) FVM Rendelet az Állatgyógyászati Termékekről. Available online: https://net.jogtar.hu/jogszabaly?docid=A0900128.FVM&searchUrl=%2Fgyorskereso%3Fkeyword%3Dfvm%2520128%2F2009 (accessed on 17 April 2023).
- Committee, S. Directive 2001/82/EC of the European Parliament and of the Council of 6 November 2001 on the Community Code Relating to Veterinary Medicinal Products. Off. J. L 2001, 311, 1–66. [Google Scholar]
- European Union. Regulation (EU) 2019/6 of the European Parliament and of the Council of 11 December 2018 on Veterinary Medicinal Products and Repealing Directive 2001/82/EC (Text with EEA Relevance). Off. J. Eur. Union 2018, 4, 44. [Google Scholar]
- Portis, E. Antimicrobial Susceptibility of Porcine Pasteurella multocida, Streptococcus suis, and Actinobacillus pleuropneumoniae from the United States and Canada, 2001 to 2010. J. Swine Health Prod. 2013, 21, 30–41. [Google Scholar]
- Kucerova, Z.; Hradecka, H.; Nechvatalova, K.; Nedbalcova, K. Antimicrobial Susceptibility of Actinobacillus pleuropneumoniae Isolates from Clinical Outbreaks of Porcine Respiratory Diseases. Vet. Microbiol. 2011, 150, 203–206. [Google Scholar] [CrossRef] [PubMed]
- Sweeney, M.T. Antimicrobial Susceptibility of Actinobacillus pleuropneumoniae, Pasteurella multocida, Streptococcus suis, and Bordetella bronchiseptica Isolated from Pigs in the United States and Canada, 2011 to 2015. J. Swine Health Prod. 2017, 25, 106–120. [Google Scholar]
- Vilaró, A.; Novell, E.; Enrique-Tarancón, V.; Balielles, J.; Vilalta, C.; Martinez, S.; Fraile Sauce, L.J. Antimicrobial Susceptibility Pattern of Porcine Respiratory Bacteria in Spain. Antibiotics 2020, 9, 402. [Google Scholar] [CrossRef]
- Gutiérrez-Martín, C.B.; Blanco, N.G.D.; Blanco, M.; Navas, J.; Rodríguez-Ferri, E.F. Changes in Antimicrobial Susceptibility of Actinobacillus pleuropneumoniae Isolated from Pigs in Spain during the Last Decade. Vet. Microbiol. 2006, 115, 218–222. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Y.; An, B.; Xie, S.; Qu, W.; Hao, H.; Huang, L.; Luo, W.; Liang, J.; Peng, D. The Dose Regimen Formulation of Doxycycline Hydrochloride and Florfenicol Injection Based on Ex Vivo Pharmacokinetic-Pharmacodynamic Modeling against the Actinobacillus pleuropneumoniae in Pigs. Anim. Dis. 2023, 3, 3. [Google Scholar] [CrossRef]
- Chang, C.-F.; Chang, L.-C.; Chang, Y.-F.; Chen, M.; Chiang, T.-S. Antimicrobial Susceptibility of Actinobacillus pleuropneumoniae, Escherichia coli, and Salmonella choleraesuis Recovered from Taiwanese Swine. J. Vet. Diagn. Investig. 2002, 14, 153–157. [Google Scholar] [CrossRef]
- Matter, D.; Rossano, A.; Limat, S.; Vorlet-Fawer, L.; Brodard, I.; Perreten, V. Antimicrobial Resistance Profile of Actinobacillus pleuropneumoniae and Actinobacillus porcitonsillarum. Vet. Microbiol. 2007, 122, 146–156. [Google Scholar] [CrossRef]
- Oh, Y.-H.; Moon, D.-C.; Lee, Y.J.; Hyun, B.-H.; Lim, S.-K. Antimicrobial Resistance of Pasteurella Multocida Strains Isolated from Pigs between 2010 and 2016. Vet. Rec. Open 2018, 5, e000293. [Google Scholar] [CrossRef]
- Cuevas, I.; Carbonero, A.; Cano, D.; García-Bocanegra, I.; Amaro, M.Á.; Borge, C. Antimicrobial Resistance of Pasteurella Multocida Type B Isolates Associated with Acute Septicemia in Pigs and Cattle in Spain. BMC Vet. Res. 2020, 16, 222. [Google Scholar] [CrossRef]
- Wisselink, H.J.; Veldman, K.T.; Van den Eede, C.; Salmon, S.A.; Mevius, D.J. Quantitative Susceptibility of Streptococcus suis Strains Isolated from Diseased Pigs in Seven European Countries to Antimicrobial Agents Licenced in Veterinary Medicine. Vet. Microbiol. 2006, 113, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Garcia, J.; Wang, J.; Restif, O.; Holmes, M.A.; Mather, A.E.; Weinert, L.A.; Wileman, T.M.; Thomson, J.R.; Langford, P.R.; Wren, B.W.; et al. Patterns of Antimicrobial Resistance in Streptococcus Suis Isolates from Pigs with or without Streptococcal Disease in England between 2009 and 2014. Vet. Microbiol. 2017, 207, 117–124. [Google Scholar] [CrossRef] [PubMed]
- van Hout, J.; Heuvelink, A.; Gonggrijp, M. Monitoring of Antimicrobial Susceptibility of Streptococcus Suis in the Netherlands, 2013–2015. Vet. Microbiol. 2016, 194, 5–10. [Google Scholar] [CrossRef]
- Magiorakos, A.-P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-Resistant, Extensively Drug-Resistant and Pandrug-Resistant Bacteria: An International Expert Proposal for Interim Standard Definitions for Acquired Resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Antibacterial Agents | Isolates Tested (pcs) | Breakpoints (µg/mL) | Distribution of Bacterial Strains (pcs and %) by Dilution Series (µg/mL) | MIC50 (µg/mL) | MIC90 (µg/mL) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 128 | 64 | 32 | 16 | 8 | 4 | 2 | 1 | 0.5 | 0.25 | 0.125 | 0.06 | 0.03 | 0.015 | |||||
| Amoxicillin | 164 | ≥2 * | 36 | 18 | 1 | 3 | 1 | 8 | 9 | 48 | 13 | 13 | 14 | 0.25 | 64 | |||
| 22.0 | 11.0 | 0.6 | 1.8 | 0.6 | 4.9 | 5.5 | 29.3 | 7.9 | 7.9 | 8.5 | ||||||||
| Ceftiofur | 144 | ≥8 * | 6 | 2 | 2 | 3 | 14 | 24 | 32 | 61 | 0.03 | 0.125 | ||||||
| 4.1 | 1.4 | 1.4 | 2.1 | 9.7 | 16.7 | 22.2 | 42.4 | |||||||||||
| Cefquinome | 41 | ≥0.03 ** | 2 | 2 | 3 | 6 | 15 | 10 | 3 | 0.06 | 0.25 | |||||||
| 4.9 | 4.9 | 7.3 | 14.6 | 36.6 | 24.4 | 7.3 | ||||||||||||
| Oxytetracycline | 45 | ≥2 * | 4 | 18 | 2 | 1 | 2 | 10 | 1 | 7 | 32 | 64 | ||||||
| 8.9 | 40.0 | 4.4 | 2.2 | 4.4 | 22.2 | 2.2 | 15.6 | |||||||||||
| Doxycycline | 109 | - | 1 | 8 | 23 | 3 | 2 | 8 | 30 | 17 | 8 | 3 | 6 | 1 | 16 | |||
| 0.9 | 7.3 | 21.1 | 2.8 | 1.8 | 7.3 | 27.5 | 15.6 | 7.3 | 2.8 | 5.5 | ||||||||
| Tylosin | 78 | - | 6 | 17 | 36 | 4 | 8 | 1 | 1 | 2 | 3 | 32 | 64 | |||||
| 7.7 | 21.8 | 46.2 | 5.1 | 10.3 | 1.3 | 1.3 | 2.6 | 3.8 | ||||||||||
| Tilmicosin | 138 | ≥32 * | 2 | 3 | 1 | 3 | 43 | 20 | 19 | 29 | 2 | 2 | 2 | 12 | 4 | 8 | ||
| 1.4 | 2.2 | 0.7 | 2.2 | 31.2 | 14.5 | 13.8 | 21.0 | 1.4 | 1.4 | 1.4 | 8.7 | |||||||
| Tylvalosin | 58 | - | 1 | 37 | 7 | 1 | 1 | 2 | 4 | 64 | 64 | |||||||
| 1.8 | 63.8 | 12.1 | 1.7 | 1.7 | 3.4 | 6.9 | ||||||||||||
| Tulathromycin | 139 | ≥128 * | 1 | 1 | 23 | 18 | 8 | 4 | 8 | 23 | 27 | 2 | 24 | 0.5 | 16 | |||
| 0.7 | 0.7 | 16.5 | 12.9 | 5.8 | 2.9 | 5.8 | 16.5 | 19.4 | 1.4 | 17.3 | ||||||||
| Lincomycin | 70 | - | 5 | 27 | 13 | 15 | 4 | 6 | 32 | 64 | ||||||||
| 7.1 | 38.6 | 18.6 | 21.4 | 5.7 | 8.6 | |||||||||||||
| Tiamulin | 112 | ≥32 * | 9 | 6 | 18 | 23 | 14 | 14 | 10 | 9 | 1 | 2 | 6 | 8 | 64 | |||
| 8.0 | 5.4 | 16.1 | 20.5 | 12.5 | 12.5 | 8.9 | 8.0 | 0.9 | 0.0 | 1.8 | 5.4 | |||||||
| Florfenicol | 164 | ≥8 * | 1 | 1 | 19 | 21 | 54 | 52 | 1 | 3 | 6 | 6 | 1 | 4 | ||||
| 0.6 | 0.6 | 11.6 | 12.8 | 32.9 | 31.7 | 0.6 | 1.8 | 3.7 | 3.7 | |||||||||
| Colistin | 88 | - | 3 | 8 | 3 | 23 | 51 | 0.015 | 1 | |||||||||
| 3.4 | 9.1 | 3.4 | 26.1 | 58.0 | ||||||||||||||
| Enrofloxacin | 141 | ≥1 * | 3 | 1 | 2 | 7 | 11 | 25 | 25 | 2 | 2 | 12 | 2 | 9 | 40 | 1 | 4 | |
| 2.1 | 0.7 | 1.4 | 5.0 | 7.8 | 17.7 | 17.7 | 1.4 | 1.4 | 8.5 | 1.4 | 6.4 | 28.4 | ||||||
| Sulfamethoxazole/ Trimethoprim+ | 61 | ≥0.125 ** | 5 | 3 | 2 | 7 | 12 | 13 | 5 | 3 | 1 | 4 | 6 | 2 | 64 | |||
| 8.2 | 4.9 | 3.3 | 11.5 | 19.7 | 21.3 | 8.2 | 4.9 | 1.6 | 6.6 | 9.8 | ||||||||
| Antimicrobial Agents | Strains Tested (pcs) | Breakpoints (µg/mL) | Sensitive (%) | Resistant (%) |
|---|---|---|---|---|
| Amoxicillin | 164 | ≥2 * | 64.0 | 36.0 |
| Ceftiofur | 144 | ≥8 * | 100.0 | 0.0 |
| Cefquinome | 41 | ≥0.03 ** | 7.3 | 92.7 |
| Oxytetracycline | 45 | ≥2 * | 44.4 | 55.6 |
| Tilmicosin | 138 | ≥32 * | 95.7 | 4.3 |
| Tulathromycin | 139 | ≥128 * | 100.0 | 0.0 |
| Tiamulin | 112 | ≥32 * | 70.5 | 29.5 |
| Florfenicol | 164 | ≥8 * | 98.8 | 1.2 |
| Enrofloxacin | 141 | ≥1 * | 47.5 | 52.5 |
| Sulfamethoxazole/Trimethoprim+ | 61 | ≥0.125 ** | 9.8 | 90.8 |
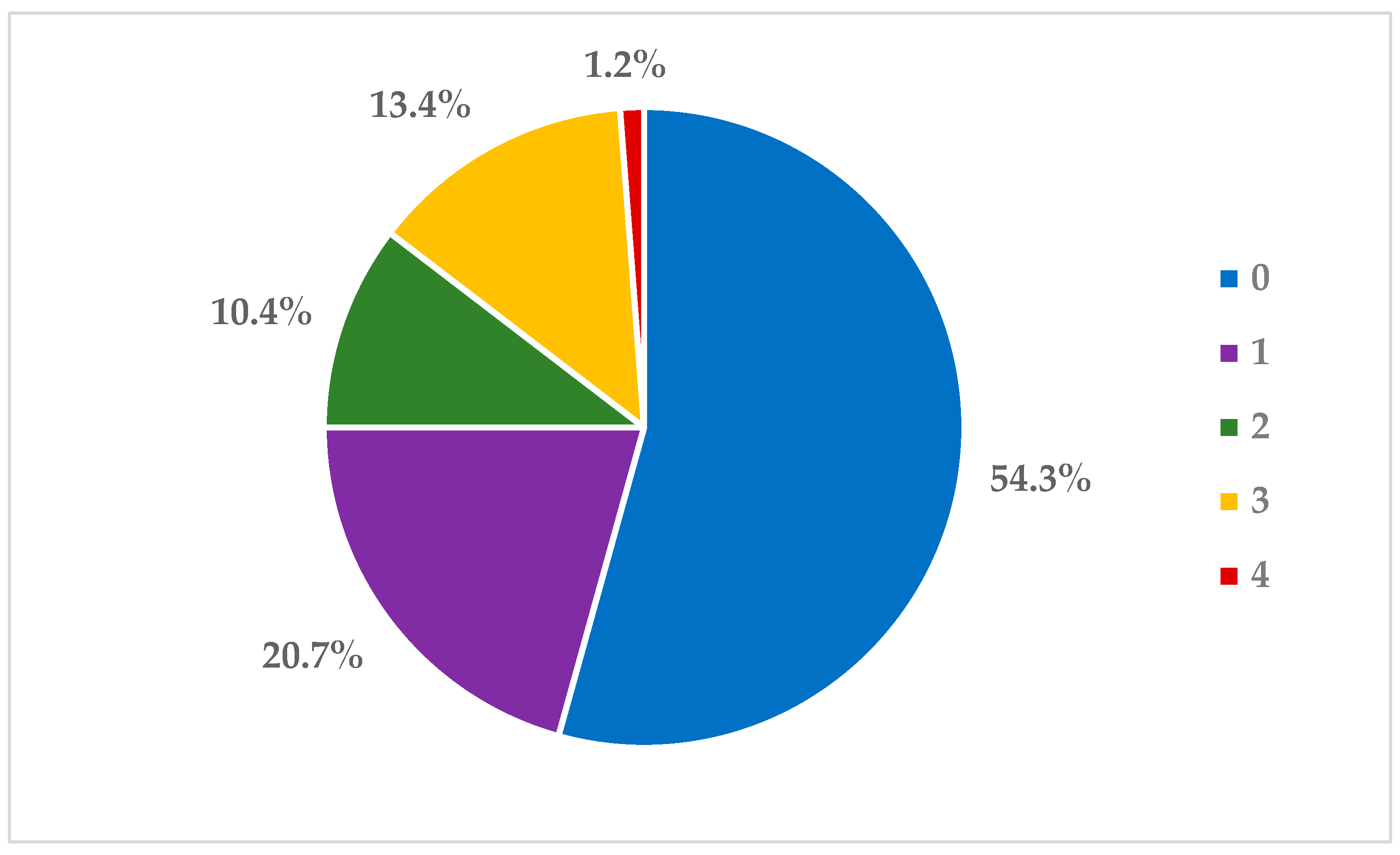
| Profile Number | Number of Isolates | MDR Profile * |
|---|---|---|
| 1 | 12 | AM, TIA, ENR |
| 2 | 8 | AM, OTC, TIA |
| 3 | 2 | AM, OTC, TIA, FLO |
| 4 | 1 | AM, OTC, TILM |
| 5 | 1 | OTC, TILM, TIA |
| Antibacterial Agents | Isolates Tested (pcs) | Breakpoints (µg/mL) | Distribution of Bacterial Strains (pcs and %) by Dilution Series (µg/mL) | MIC50 (µg/mL) | MIC90 (µg/mL) | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 256 | 128 | 64 | 32 | 16 | 8 | 4 | 2 | 1 | 0.5 | 0.25 | 0.125 | 0.06 | 0.03 | 0.015 | |||||
| Amoxicillin | 65 | ≥2 * | 13 | 15 | 21 | 4 | 10 | 2 | 0.25 | 1 | |||||||||
| 20.0 | 23.1 | 32.3 | 6.2 | 15.4 | 3.1 | ||||||||||||||
| Ceftiofur | 63 | ≥8 * | 1 | 2 | 1 | 2 | 4 | 7 | 14 | 32 | 0.015 | 0.125 | |||||||
| 1.6 | 3.2 | 1.6 | 3.2 | 6.3 | 11.1 | 22.2 | 50.8 | ||||||||||||
| Doxycycline | 65 | ≥1 ** | 2 | 1 | 3 | 5 | 9 | 19 | 7 | 6 | 13 | 0.5 | 2 | ||||||
| 3.1 | 1.5 | 4.6 | 7.7 | 13.8 | 29.2 | 10.8 | 9.2 | 20.0 | |||||||||||
| Tylosin | 29 | - | 2 | 11 | 13 | 3 | 16 | 32 | |||||||||||
| 6.9 | 37.9 | 44.8 | 10.3 | ||||||||||||||||
| Tilmicosin | 42 | ≥32 * | 2 | 1 | 2 | 2 | 11 | 8 | 12 | 4 | 1 | 8 | |||||||
| 4.8 | 2.4 | 4.8 | 4.8 | 26.2 | 19.0 | 28.6 | 9.5 | ||||||||||||
| Tulathromycin | 59 | ≥64 * | 1 | 1 | 1 | 5 | 9 | 17 | 23 | 2 | 0.125 | 0.5 | |||||||
| 1.7 | 1.7 | 1.7 | 8.5 | 15.3 | 28.8 | 39.0 | 3.4 | ||||||||||||
| Lincomycin | 19 | - | 2 | 6 | 6 | 1 | 2 | 2 | 16 | 32 | |||||||||
| 10.5 | 31.6 | 31.6 | 5.3 | 10.5 | 10.5 | ||||||||||||||
| Tiamulin | 44 | ≥64 ** | 1 | 2 | 13 | 22 | 5 | 1 | 8 | 16 | |||||||||
| 2.3 | 4.5 | 29.5 | 50.0 | 11.4 | 2.3 | ||||||||||||||
| Florfenicol | 65 | ≥8 * | 2 | 2 | 11 | 30 | 16 | 1 | 3 | 0.5 | 1 | ||||||||
| 3.1 | 3.1 | 16.9 | 46.2 | 24.6 | 1.5 | 4.6 | |||||||||||||
| Colistin | 25 | - | 1 | 8 | 10 | 6 | 0.03 | 0.06 | |||||||||||
| 4 | 32 | 40 | 24 | ||||||||||||||||
| Enrofloxacin | 41 | ≥1 * | 9 | 12 | 20 | 0.03 | 0.06 | ||||||||||||
| 22.0 | 29.3 | 48.8 | |||||||||||||||||
| Sulfamethoxazole/ Trimethoprim+ | 54 | ≥0.125 ** | 3 | 2 | 9 | 5 | 4 | 10 | 19 | 2 | 4 | 32 | |||||||
| 5.6 | 3.7 | 16.7 | 9.3 | 7.4 | 18.5 | 35.2 | 3.7 | ||||||||||||
| Antimicrobial Agents | Strains Tested (pcs) | Breakpoints (µg/mL) | Sensitive (%) | Resistant (%) |
|---|---|---|---|---|
| Amoxicillin | 65 | ≥2 * | 100.0 | 0.0 |
| Ceftiofur | 63 | ≥8 * | 98.4 | 1.6 |
| Doxycycline | 65 | ≥1 ** | 69.2 | 30.8 |
| Tilmicosin | 42 | ≥32 * | 95.2 | 4.8 |
| Tulathromycin | 59 | ≥64 * | 100.0 | 0.0 |
| Tiamulin | 44 | ≥64 ** | 97.7 | 2.3 |
| Florfenicol | 65 | ≥8 * | 100.0 | 0.0 |
| Enrofloxacin | 41 | ≥1 * | 100.0 | 0.0 |
| Sulfamethoxazole/Trimethoprim+ | 54 | ≥0.125 ** | 0.0 | 100.0 |
| Antibacterial Agents | Isolates Tested (pcs) | Breakpoints (µg/mL) | Distribution of Bacterial Strains (pcs and %) by Dilution Series (µg/mL) | MIC50 (µg/mL) | MIC90 (µg/mL) | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 256 | 128 | 64 | 32 | 16 | 8 | 4 | 2 | 1 | 0.5 | 0.25 | 0.125 | 0.06 | 0.03 | 0.015 | |||||
| Amoxicillin | 116 | - | 4 | 2 | 4 | 1 | 2 | 4 | 3 | 4 | 12 | 37 | 43 | 0.06 | 4 | ||||
| 3.4 | 1.7 | 3.4 | 0.9 | 1.7 | 3.4 | 2.6 | 3.4 | 10.3 | 31.9 | 37.1 | |||||||||
| Ceftiofur | 117 | ≥8 * | 2 | 3 | 8 | 4 | 10 | 3 | 13 | 17 | 57 | 0.03 | 1 | ||||||
| 1.7 | 2.6 | 6.8 | 3.4 | 8.5 | 2.6 | 11.1 | 14.5 | 48.7 | |||||||||||
| Doxycycline | 100 | - | 3 | 24 | 18 | 6 | 8 | 7 | 2 | 5 | 4 | 8 | 15 | 8 | 32 | ||||
| 3 | 24 | 18 | 6 | 8 | 7 | 2 | 5 | 4 | 8 | 15 | |||||||||
| Tylosin | 41 | - | 15.0 | 12.0 | 2.0 | 3.0 | 2.0 | 1.0 | 6.0 | 32 | 128 | ||||||||
| 36.6 | 29.3 | 4.9 | 7.3 | 4.9 | 2.4 | 14.6 | |||||||||||||
| Tilmicosin | 86 | - | 21 | 2 | 11 | 7 | 3 | 1 | 4 | 16 | 3 | 7 | 4 | 7 | 8 | 128 | |||
| 24.4 | 2.3 | 12.8 | 8.1 | 3.5 | 1.2 | 4.7 | 18.6 | 3.5 | 8.1 | 4.7 | 8.1 | ||||||||
| Tylvalosin | 89 | - | 17 | 1 | 14 | 6 | 4 | 7 | 3 | 5 | 8 | 4 | 16 | 2 | 2 | 2 | 128 | ||
| 19.1 | 1.1 | 15.7 | 6.7 | 4.5 | 7.9 | 3.4 | 5.6 | 9.0 | 4.5 | 18.0 | 2.2 | 2.2 | |||||||
| Lincomycin | 40 | - | 17 | 3 | 4 | 2 | 2 | 4 | 8 | 32 | 128 | ||||||||
| 42.5 | 7.5 | 10.0 | 5.0 | 5.0 | 10.0 | 20.0 | |||||||||||||
| Tiamulin | 33 | - | 8 | 7 | 1 | 1 | 6 | 1 | 1 | 4 | 1 | 1 | 2 | 16 | 128 | ||||
| 24.2 | 21.2 | 3.0 | 3.0 | 18.2 | 3.0 | 3.0 | 12.1 | 3.0 | 3.0 | 6.1 | |||||||||
| Florfenicol | 118 | ≥8 * | 8 | 4 | 17 | 24 | 38 | 9 | 5 | 3 | 5 | 5 | 2 | 8 | |||||
| 6.8 | 3.4 | 14.4 | 20.3 | 32.2 | 7.6 | 4.2 | 2.5 | 4.2 | 4.2 | ||||||||||
| Enrofloxacin | 70 | ≥2 * | 4 | 5 | 1 | 2 | 12 | 12 | 7 | 11 | 6 | 4 | 6 | 0.5 | 8 | ||||
| 5.7 | 7.1 | 1.4 | 2.9 | 17.1 | 17.1 | 10.0 | 15.7 | 8.6 | 5.7 | 8.6 | |||||||||
| Sulfamethoxazole/ Trimethoprim + | 105 | ≥0.25 ** | 15 | 17 | 2 | 9 | 10 | 13 | 18 | 3 | 2 | 9 | 1 | 6 | 16 | 256 | |||
| 14.3 | 16.2 | 1.9 | 8.6 | 9.5 | 12.4 | 17.1 | 2.9 | 1.9 | 8.6 | 1.0 | 5.7 | ||||||||
| Antimicrobial Agents | Strains Tested (pcs) | Breakpoints (µg/mL) | Sensitive (%) | Resistant (%) |
|---|---|---|---|---|
| Ceftiofur | 117 | ≥8 * | 100.0 | 0.0 |
| Florfenicol | 118 | ≥8 * | 75.4 | 24.6 |
| Enrofloxacin | 105 | ≥2 * | 82.9 | 17.1 |
| Sulfamethoxazole/Trimethoprim+ | 116 | ≥0.25 ** | 5.7 | 94.3 |
| Antibacterial Agent | A. pleuropneumoniae (pcs) | P. multocida (pcs) | S. suis (pcs) |
|---|---|---|---|
| Amoxicillin | 164 | 65 | 116 |
| Ceftiofur | 144 | 63 | 117 |
| Cefquinome | 41 | - | - |
| Oxytetracycline | 45 | - | - |
| Doxycycline | 109 | 65 | 100 |
| Tylosin | 78 | 29 | 41 |
| Tilmicosin | 138 | 42 | 86 |
| Tylvalosin | 58 | - | - |
| Tulathromycin | 139 | 59 | 89 |
| Lincomycin | 70 | 19 | 40 |
| Tiamulin | 112 | 44 | 33 |
| Florfenicol | 164 | 65 | 118 |
| Colistin | 88 | 25 | - |
| Enrofloxacin | 141 | 41 | 70 |
| Sulfamethoxazole: Trimethoprim (20:1) | 61 | 54 | 105 |
| Total (pcs) | 164 | 65 | 118 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Somogyi, Z.; Mag, P.; Simon, R.; Kerek, Á.; Makrai, L.; Biksi, I.; Jerzsele, Á. Susceptibility of Actinobacillus pleuropneumoniae, Pasteurella multocida and Streptococcus suis Isolated from Pigs in Hungary between 2018 and 2021. Antibiotics 2023, 12, 1298. https://doi.org/10.3390/antibiotics12081298
Somogyi Z, Mag P, Simon R, Kerek Á, Makrai L, Biksi I, Jerzsele Á. Susceptibility of Actinobacillus pleuropneumoniae, Pasteurella multocida and Streptococcus suis Isolated from Pigs in Hungary between 2018 and 2021. Antibiotics. 2023; 12(8):1298. https://doi.org/10.3390/antibiotics12081298
Chicago/Turabian StyleSomogyi, Zoltán, Patrik Mag, Réka Simon, Ádám Kerek, László Makrai, Imre Biksi, and Ákos Jerzsele. 2023. "Susceptibility of Actinobacillus pleuropneumoniae, Pasteurella multocida and Streptococcus suis Isolated from Pigs in Hungary between 2018 and 2021" Antibiotics 12, no. 8: 1298. https://doi.org/10.3390/antibiotics12081298
APA StyleSomogyi, Z., Mag, P., Simon, R., Kerek, Á., Makrai, L., Biksi, I., & Jerzsele, Á. (2023). Susceptibility of Actinobacillus pleuropneumoniae, Pasteurella multocida and Streptococcus suis Isolated from Pigs in Hungary between 2018 and 2021. Antibiotics, 12(8), 1298. https://doi.org/10.3390/antibiotics12081298