
Two-Stage Revision Arthroplasty for Resistant Gram-Positive Periprosthetic Joint Infections Using an Oral Linezolid-Based Antibiotic Regime

 , ,
, ,
Abstract
1. Introduction
2. Results
2.1. Patient Details
2.2. Subsequent PJI
2.3. Microbiological Failure
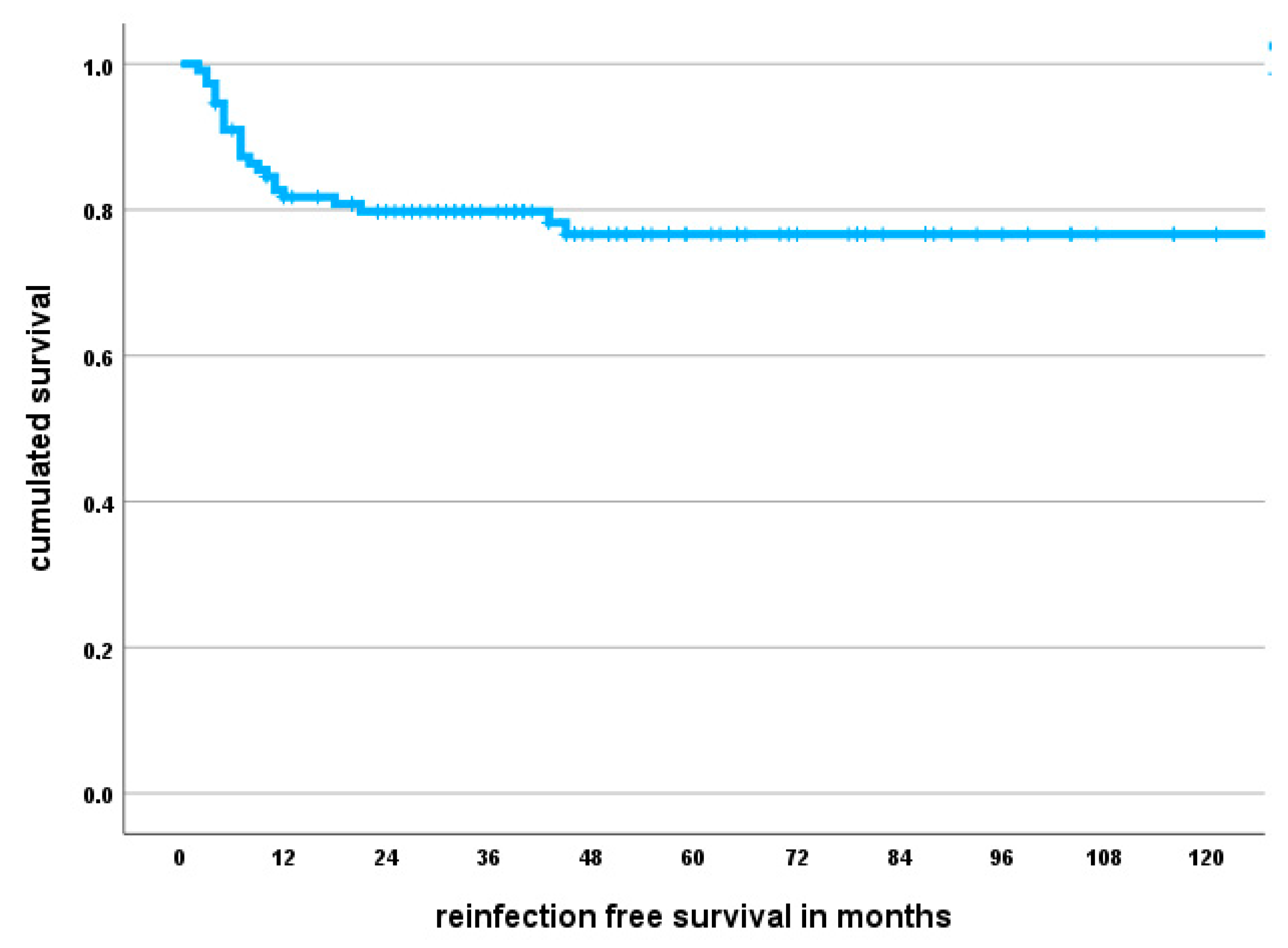
2.4. Infection-Free Survival
2.5. Factors Associated with Subsequent PJI
2.6. Adverse Events and Treatment Discontinuation
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Osmon, D.R.; Berbari, E.F.; Berendt, A.R.; Lew, D.; Zimmerli, W.; Steckelberg, J.M.; Rao, N.; Hanssen, A.; Wilson, W.R.; Infectious Diseases Society of America. Executive summary: Diagnosis and management of prosthetic joint infection: Clinical practice guidelines by the Infectious Diseases Society of America. Clin. Infect. Dis. 2013, 56, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Anemuller, R.; Belden, K.; Brause, B.; Citak, M.; Del Pozo, J.L.; Frommelt, L.; Gehrke, T.; Hewlett, A.; Higuera, C.A.; Hughes, H.; et al. Hip and Knee Section, Treatment, Antimicrobials: Proceedings of International Consensus on Orthopedic Infections. J. Arthroplast. 2019, 34, S463–S475. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, S.M.; Lau, E.C.; Son, M.S.; Chang, E.T.; Zimmerli, W.; Parvizi, J. Are We Winning or Losing the Battle With Periprosthetic Joint Infection: Trends in Periprosthetic Joint Infection and Mortality Risk for the Medicare Population. J. Arthroplast. 2018, 33, 3238–3245. [Google Scholar] [CrossRef] [PubMed]
- Leitner, L.; Posch, F.; Amerstorfer, F.; Sadoghi, P.; Leithner, A.; Glehr, M. The Dark Side of Arthroplasty: Competing Risk Analysis of Failed Hip and Knee Arthroplasty With Periprosthetic Joint Infection. J. Arthroplast. 2020, 35, 2601–2606. [Google Scholar] [CrossRef]
- Osmon, D.R.; Berbari, E.F.; Berendt, A.R.; Lew, D.; Zimmerli, W.; Steckelberg, J.M.; Rao, N.; Hanssen, A.; Wilson, W.R. Infectious Diseases Society of America. Diagnosis and management of prosthetic joint infection: Clinical practice guidelines by the Infectious Diseases Society of America. Clin. Infect. Dis. 2013, 56, e1–e25. [Google Scholar] [CrossRef]
- de Beaubien, B.; Belden, K.; Bell, K.; Boyle, K.; Cordero-Ampuero, J.; Della Valle, C.J.; Eijer, H.; Ferry, C.; Janz, V.; Kessler, B.; et al. Hip and Knee Section, Treatment, Antimicrobials: Proceedings of International Consensus on Orthopedic Infections. J. Arthroplast. 2018, 34, S477–S482. [Google Scholar] [CrossRef]
- Sendi, P.; Zimmerli, W. Antimicrobial treatment concepts for orthopaedic device-related infection. Clin. Microbiol. Infect. 2012, 18, 1176–1184. [Google Scholar] [CrossRef]
- Zimmerli, W.; Sendi, P. Role of Rifampin against Staphylococcal Biofilm Infections In Vitro, in Animal Models, and in Orthopedic-Device-Related Infections. Antimicrob. Agents Chemother. 2019, 63, 10–1128. [Google Scholar] [CrossRef]
- Hipfl, C.; Winkler, T.; Janz, V.; Perka, C.; Muller, M. Management of Chronically Infected Total Knee Arthroplasty With Severe Bone Loss Using Static Spacers With Intramedullary Rods. J. Arthroplast. 2019, 34, 1462–1469. [Google Scholar] [CrossRef]
- Lourtet-Hascoet, J.; Felice, M.P.; Bicart-See, A.; Bouige, A.; Giordano, G.; Bonnet, E. Species and antimicrobial susceptibility testing of coagulase-negative staphylococci in periprosthetic joint infections. Epidemiol. Infect. 2018, 146, 1771–1776. [Google Scholar] [CrossRef]
- De Vecchi, E.; George, D.A.; Romano, C.L.; Pregliasco, F.E.; Mattina, R.; Drago, L. Antibiotic sensitivities of coagulase-negative staphylococci and Staphylococcus aureus in hip and knee periprosthetic joint infections: Does this differ if patients meet the International Consensus Meeting Criteria? Infect. Drug. Resist. 2018, 11, 539–546. [Google Scholar] [CrossRef] [PubMed]
- Drago, L.; De Vecchi, E.; Bortolin, M.; Zagra, L.; Romano, C.L.; Cappelletti, L. Epidemiology and Antibiotic Resistance of Late Prosthetic Knee and Hip Infections. J. Arthroplast. 2017, 32, 2496–2500. [Google Scholar] [CrossRef] [PubMed]
- Moise, P.A.; Forrest, A.; Birmingham, M.C.; Schentag, J.J. The efficacy and safety of linezolid as treatment for Staphylococcus aureus infections in compassionate use patients who are intolerant of, or who have failed to respond to, vancomycin. J. Antimicrob. Chemother. 2002, 50, 1017–1026. [Google Scholar] [CrossRef] [PubMed]
- Deroche, L.; Plouzeau, C.; Bemer, P.; Tande, D.; Valentin, A.S.; Jolivet-Gougeon, A.; Lemarie, C.; Bret, L.; Kempf, M.; Hery-Arnaud, G.; et al. Probabilistic chemotherapy in knee and hip replacement infection: The place of linezolid. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 1659–1663. [Google Scholar] [CrossRef] [PubMed]
- McGregor, J.C.; Hartung, D.M.; Allen, G.P.; Taplitz, R.A.; Traver, R.; Tong, T.; Bearden, D.T. Risk factors associated with linezolid-nonsusceptible enterococcal infections. Am. J. Infect. Control. 2012, 40, 886–887. [Google Scholar] [CrossRef]
- Theil, C.; Schmidt-Braekling, T.; Gosheger, G.; Schwarze, J.; Dieckmann, R.; Schneider, K.N.; Mollenbeck, B. Clinical use of linezolid in periprosthetic joint infections—a systematic review. J. Bone Jt. Infect. 2020, 6, 7–16. [Google Scholar] [CrossRef]
- Bassetti, M.; Vitale, F.; Melica, G.; Righi, E.; Di Biagio, A.; Molfetta, L.; Pipino, F.; Cruciani, M.; Bassetti, D. Linezolid in the treatment of Gram-positive prosthetic joint infections. J. Antimicrob. Chemother. 2005, 55, 387–390. [Google Scholar] [CrossRef]
- Eriksson, H.K.; Ahadpour, D.; Hailer, N.P.; Lazarinis, S.; Jarhult, J.D. Linezolid in the treatment of periprosthetic joint infection caused by coagulase-negative staphylococci. Infect. Dis. 2019, 51, 683–690. [Google Scholar] [CrossRef]
- Morata, L.; Senneville, E.; Bernard, L.; Nguyen, S.; Buzele, R.; Druon, J.; Tornero, E.; Mensa, J.; Soriano, A. A Retrospective Review of the Clinical Experience of Linezolid with or Without Rifampicin in Prosthetic Joint Infections Treated with Debridement and Implant Retention. Infect. Dis. Ther. 2014, 3, 235–243. [Google Scholar] [CrossRef]
- Morata, L.; Tornero, E.; Martinez-Pastor, J.C.; Garcia-Ramiro, S.; Mensa, J.; Soriano, A. Clinical experience with linezolid for the treatment of orthopaedic implant infections. J. Antimicrob. Chemother. 2014, 69 (Suppl. S1), i47–i52. [Google Scholar] [CrossRef][Green Version]
- Soriano, A.; Gomez, J.; Gomez, L.; Azanza, J.R.; Perez, R.; Romero, F.; Pons, M.; Bella, F.; Velasco, M.; Mensa, J. Efficacy and tolerability of prolonged linezolid therapy in the treatment of orthopedic implant infections. Eur. J. Clin. Microbiol. Infect. Dis. 2007, 26, 353–356. [Google Scholar] [CrossRef] [PubMed]
- Gomez, J.; Canovas, E.; Banos, V.; Martinez, L.; Garcia, E.; Hernandez-Torres, A.; Canteras, M.; Ruiz, J.; Medina, M.; Martinez, P.; et al. Linezolid plus rifampin as a salvage therapy in prosthetic joint infections treated without removing the implant. Antimicrob. Agents Chemother. 2011, 55, 4308–4310. [Google Scholar] [CrossRef] [PubMed]
- McPherson, E.J.; Tontz, W., Jr.; Patzakis, M.; Woodsome, C.; Holtom, P.; Norris, L.; Shufelt, C. Outcome of infected total knee utilizing a staging system for prosthetic joint infection. Am. J. Orthop. 1999, 28, 161–165. [Google Scholar]
- McPherson, E.J.; Woodson, C.; Holtom, P.; Roidis, N.; Shufelt, C.; Patzakis, M. Periprosthetic total hip infection: Outcomes using a staging system. Clin. Orthop. Relat. Res. 2002, 403, 8–15. [Google Scholar] [CrossRef]
- Oussedik, S.I.; Haddad, F.S. The use of linezolid in the treatment of infected total joint arthroplasty. J. Arthroplast. 2008, 23, 273–278. [Google Scholar] [CrossRef]
- Rao, N.; Ziran, B.H.; Hall, R.A.; Santa, E.R. Successful treatment of chronic bone and joint infections with oral linezolid. Clin. Orthop. Relat. Res. 2004, 427, 67–71. [Google Scholar] [CrossRef]
- Petis, S.M.; Perry, K.I.; Mabry, T.M.; Hanssen, A.D.; Berry, D.J.; Abdel, M.P. Two-Stage Exchange Protocol for Periprosthetic Joint Infection Following Total Knee Arthroplasty in 245 Knees without Prior Treatment for Infection. J. Bone Joint Surg. Am. 2019, 101, 239–249. [Google Scholar] [CrossRef]
- Chalmers, B.P.; Mabry, T.M.; Abdel, M.P.; Berry, D.J.; Hanssen, A.D.; Perry, K.I. Two-Stage Revision Total Hip Arthroplasty With a Specific Articulating Antibiotic Spacer Design: Reliable Periprosthetic Joint Infection Eradication and Functional Improvement. J. Arthroplast. 2018, 33, 3746–3753. [Google Scholar] [CrossRef] [PubMed]
- Stevoska, S.; Himmelbauer, F.; Stiftinger, J.; Stadler, C.; Gotterbarm, T.; Heyse, T.J.; Klasan, A. Significant Difference in Antimicrobial Resistance of Coagulase Negative Periprosthetic Joint Infection in Septic Revision Total Knee Arthroplasty Between Two Major Orthopedic Centers. J. Arthroplast. 2022, 37, S306–S312. [Google Scholar] [CrossRef]
- Charalambous, L.T.; Kim, B.I.; Schwartz, A.M.; Case, A.; Seidelman, J.L.; Hendershot, E.F.; Bolognesi, M.P.; Seyler, T.M.; Jiranek, W.A. Prosthetic Knee Infection With Coagulase-Negative Staphylococcus: A Harbinger of Poor Outcomes. J. Arthroplast. 2022, 37, S313–S320. [Google Scholar] [CrossRef]
- Ahmad, S.S.; Orlik, L.; Ahmad, S.J.S.; Albers, C.E.; Siebenrock, K.A.; Klenke, F.M. Obesity and smoking predict the results of two-stage exchange in septic revision hip arthroplasty: A cohort study. Orthop. Traumatol. Surg. Res. 2019, 105, 467–471. [Google Scholar] [CrossRef]
- Bernard, L.; Legout, L.; Zurcher-Pfund, L.; Stern, R.; Rohner, P.; Peter, R.; Assal, M.; Lew, D.; Hoffmeyer, P.; Uckay, I. Six weeks of antibiotic treatment is sufficient following surgery for septic arthroplasty. J. Infect. 2010, 61, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Legout, L.; Valette, M.; Dezeque, H.; Nguyen, S.; Lemaire, X.; Loiez, C.; Caillaux, M.; Beltrand, E.; Dubreuil, L.; Yazdanpanah, Y.; et al. Tolerability of prolonged linezolid therapy in bone and joint infection: Protective effect of rifampicin on the occurrence of anaemia? J. Antimicrob. Chemother. 2010, 65, 2224–2230. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, S.; Pasquet, A.; Legout, L.; Beltrand, E.; Dubreuil, L.; Migaud, H.; Yazdanpanah, Y.; Senneville, E. Efficacy and tolerance of rifampicin-linezolid compared with rifampicin-cotrimoxazole combinations in prolonged oral therapy for bone and joint infections. Clin. Microbiol. Infect. 2009, 15, 1163–1169. [Google Scholar] [CrossRef]
- Chaussade, H.; Uckay, I.; Vuagnat, A.; Druon, J.; Gras, G.; Rosset, P.; Lipsky, B.A.; Bernard, L. Antibiotic therapy duration for prosthetic joint infections treated by Debridement and Implant Retention (DAIR): Similar long-term remission for 6 weeks as compared to 12 weeks. Int. J. Infect. Dis. 2017, 63, 37–42. [Google Scholar] [CrossRef]
- Bernard, L.; Arvieux, C.; Brunschweiler, B.; Touchais, S.; Ansart, S.; Bru, J.P.; Oziol, E.; Boeri, C.; Gras, G.; Druon, J.; et al. Antibiotic Therapy for 6 or 12 Weeks for Prosthetic Joint Infection. N. Engl. J. Med. 2021, 384, 1991–2001. [Google Scholar] [CrossRef] [PubMed]
- Vazquez, J.A.; Arnold, A.C.; Swanson, R.N.; Biswas, P.; Bassetti, M. Safety of long-term use of linezolid: Results of an open-label study. Ther. Clin. Risk Manag. 2016, 12, 1347–1354. [Google Scholar] [CrossRef] [PubMed]
- Tornero, E.; Morata, L.; Martinez-Pastor, J.C.; Angulo, S.; Combalia, A.; Bori, G.; Garcia-Ramiro, S.; Bosch, J.; Mensa, J.; Soriano, A. Importance of selection and duration of antibiotic regimen in prosthetic joint infections treated with debridement and implant retention. J. Antimicrob. Chemother. 2016, 71, 1395–1401. [Google Scholar] [CrossRef]
- Gandelman, K.; Zhu, T.; Fahmi, O.A.; Glue, P.; Lian, K.; Obach, R.S.; Damle, B. Unexpected effect of rifampin on the pharmacokinetics of linezolid: In silico and in vitro approaches to explain its mechanism. J. Clin. Pharmacol. 2011, 51, 229–236. [Google Scholar] [CrossRef]
- Parvizi, J.; Zmistowski, B.; Berbari, E.F.; Bauer, T.W.; Springer, B.D.; Della Valle, C.J.; Garvin, K.L.; Mont, M.A.; Wongworawat, M.D.; Zalavras, C.G. New definition for periprosthetic joint infection: From the Workgroup of the Musculoskeletal Infection Society. Clin. Orthop. Relat. Res. 2011, 469, 2992–2994. [Google Scholar] [CrossRef]
- Horan, T.C.; Andrus, M.; Dudeck, M.A. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am. J. Infect. Control 2008, 36, 309–332. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Ledezma, C.; Higuera, C.A.; Parvizi, J. Success after treatment of periprosthetic joint infection: A Delphi-based international multidisciplinary consensus. Clin. Orthop. Relat. Res. 2013, 471, 2374–2382. [Google Scholar] [CrossRef] [PubMed]
- Pea, F.; Cojutti, P.G.; Baraldo, M. A 10-Year Experience of Therapeutic Drug Monitoring (TDM) of Linezolid in a Hospital-wide Population of Patients Receiving Conventional Dosing: Is there Enough Evidence for Suggesting TDM in the Majority of Patients? Basic. Clin. Pharmacol. Toxicol. 2017, 121, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Pea, F.; Furlanut, M.; Cojutti, P.; Cristini, F.; Zamparini, E.; Franceschi, L.; Viale, P. Therapeutic drug monitoring of linezolid: A retrospective monocentric analysis. Antimicrob. Agents Chemother. 2010, 54, 4605–4610. [Google Scholar] [CrossRef] [PubMed]
- Pea, F.; Viale, P.; Cojutti, P.; Del Pin, B.; Zamparini, E.; Furlanut, M. Therapeutic drug monitoring may improve safety outcomes of long-term treatment with linezolid in adult patients. J. Antimicrob. Chemother. 2012, 67, 2034–2042. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Median (25–75% IQR) | Reinfection Group (24/111) | Infection Control Group (87/111) | p-Value |
|---|---|---|---|---|
| Age | 72 (63–78) | 76 | 71 | 0.08 |
| CCI | 3 (1–4) | 4 | 3 | 0.68 |
| BMI | 29 (26–34) | 32 | 28 | 0.002 |
| Number of previous revision arthroplasties | 3 (1–5) | 2 | 3 | 0.38 |
| Days until second-stage reimplantation | 67 (52–82) | 75 | 64 | 0.13 |
| Variable | % (n/111) | Reinfection Group % (n/24) | Infection Control Group % (n/87) | p-Value |
|---|---|---|---|---|
| Female | 56 (62) | 46 (11) | 59 (51) | 0.33 |
| Diabetic | 24 (27) | 8 (33) | 22 (19) | 0.24 |
| Implant location | 0.82 | |||
| THA | 48 (53) | 50 (12) | 47 (41) | |
| TKA | 52 (58) | 50 (12) | 53 (46) | |
| Currently smoking | 3 (3) | n/a | 3 (3) | n/a |
| Obesity (BMI > 30) | 46 (51) | 63 (15) | 41 (36) | 0.05 |
| Previous revision arthroplasty | 87 (96) | 75 (18) | 90 (78) | 0.13 |
| Previous revision for PJI | 53 (59) | 50 (12) | 54 (47) | 0.82 |
| Fistulating infection | 22 (24) | 17 (4) | 23 (20) | 0.64 |
| Systemic host grade | 0.58 | |||
| A | 50 (56) | 46 (11) | 52 (45) | |
| B | 47 (52) | 50 (12) | 46 (40) | |
| C | 3 (3) | 4 (1) | 2 (2) | |
| Extremity grade | 0.29 | |||
| 1 | 8 (9) | n/a | 10 (9) | |
| 2 | 72 (80) | 83 (20) | 69 (60) | |
| 3 | 20 (22) | 17 (4) | 21 (18) |
| Microbiology at First-Stage Surgery * | % (n/111) |
|---|---|
| MR-ConS | 64 (71) |
| MRSA | 11 (10) |
| MSSA | 8 (9) |
| Enterococcus | 7 (6) |
| Polymicrobial | 33 (37) |
| Others ** | 13 (15) |
| Microbiology at Reinfection | % (n/24) |
|---|---|
| Polymicrobial | 42 (10) |
| MR-coagulase negative staphylococci (CoNS) | 21 (5) |
| Gram-negative microorganisms | 17 (4) |
| Others * | 21 (5) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gründer, L.; Bockholt, S.; Gosheger, G.; Schulze, M.; Schwarze, J.; Pützler, J.; Moellenbeck, B.; Theil, C. Two-Stage Revision Arthroplasty for Resistant Gram-Positive Periprosthetic Joint Infections Using an Oral Linezolid-Based Antibiotic Regime. Antibiotics 2023, 12, 1235. https://doi.org/10.3390/antibiotics12081235
Gründer L, Bockholt S, Gosheger G, Schulze M, Schwarze J, Pützler J, Moellenbeck B, Theil C. Two-Stage Revision Arthroplasty for Resistant Gram-Positive Periprosthetic Joint Infections Using an Oral Linezolid-Based Antibiotic Regime. Antibiotics. 2023; 12(8):1235. https://doi.org/10.3390/antibiotics12081235
Chicago/Turabian StyleGründer, Lars, Sebastian Bockholt, Georg Gosheger, Martin Schulze, Jan Schwarze, Jan Pützler, Burkhard Moellenbeck, and Christoph Theil. 2023. "Two-Stage Revision Arthroplasty for Resistant Gram-Positive Periprosthetic Joint Infections Using an Oral Linezolid-Based Antibiotic Regime" Antibiotics 12, no. 8: 1235. https://doi.org/10.3390/antibiotics12081235
APA StyleGründer, L., Bockholt, S., Gosheger, G., Schulze, M., Schwarze, J., Pützler, J., Moellenbeck, B., & Theil, C. (2023). Two-Stage Revision Arthroplasty for Resistant Gram-Positive Periprosthetic Joint Infections Using an Oral Linezolid-Based Antibiotic Regime. Antibiotics, 12(8), 1235. https://doi.org/10.3390/antibiotics12081235