
Cemented versus Cementless Stem Fixation in Revision Total Knee Arthroplasty: A Systematic Review and Meta-Analysis

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
- “Total Knee Replacement*” OR “Total Knee Arthroplasty*”
- AND
- “Reoperation” OR “Revision” OR “Reimplantation”
- AND
- “stem*” OR “cement*” OR “hybrid”.
2.2. Study Selection and Eligibility Criteria
2.3. Data Collection Process
2.4. Study Risk of Bias Assessment
2.5. Effect Measures
2.6. Synthesis Methods and Statistical Analysis
3. Results
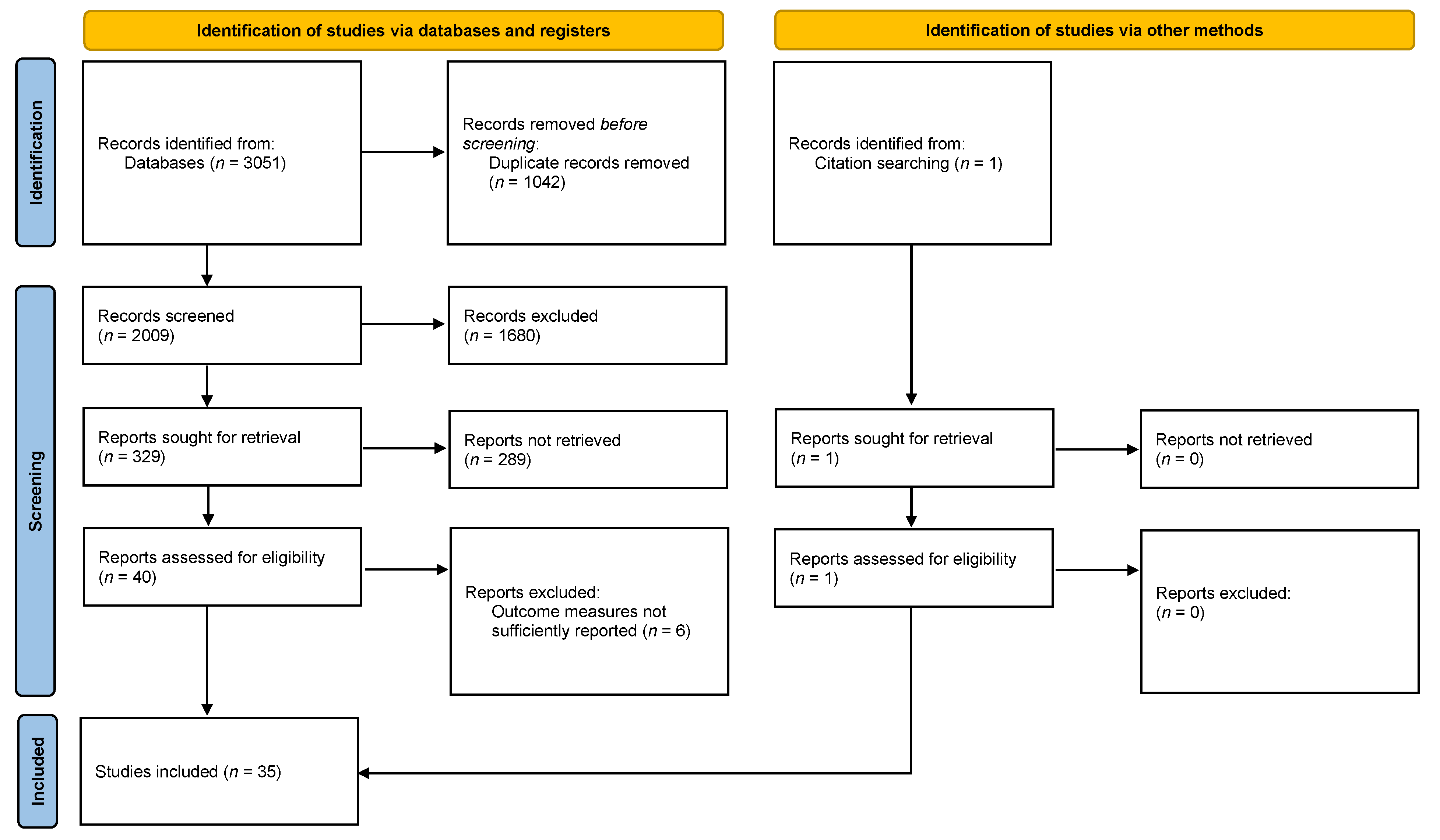
3.1. Search Results
3.2. Study Characteristics
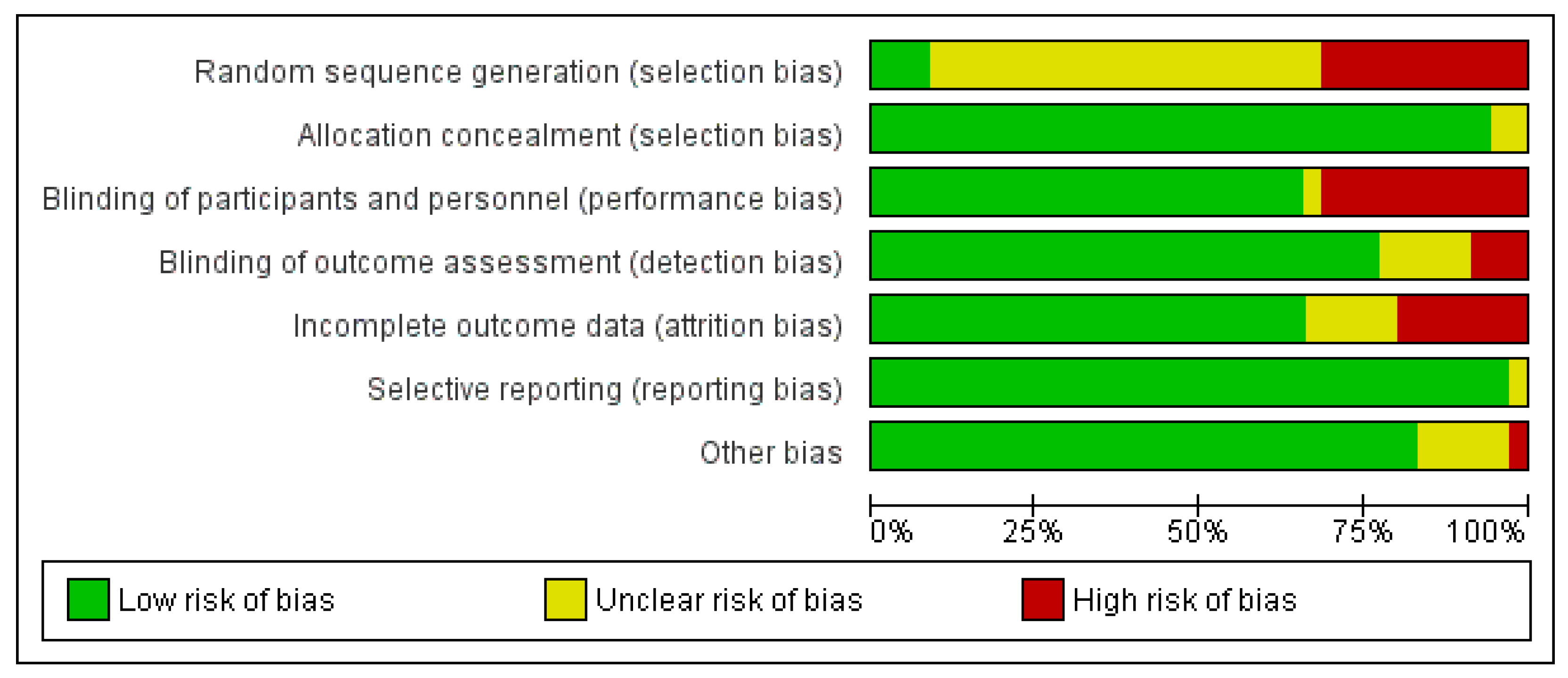
3.3. Risk of Bias in the Included Studies
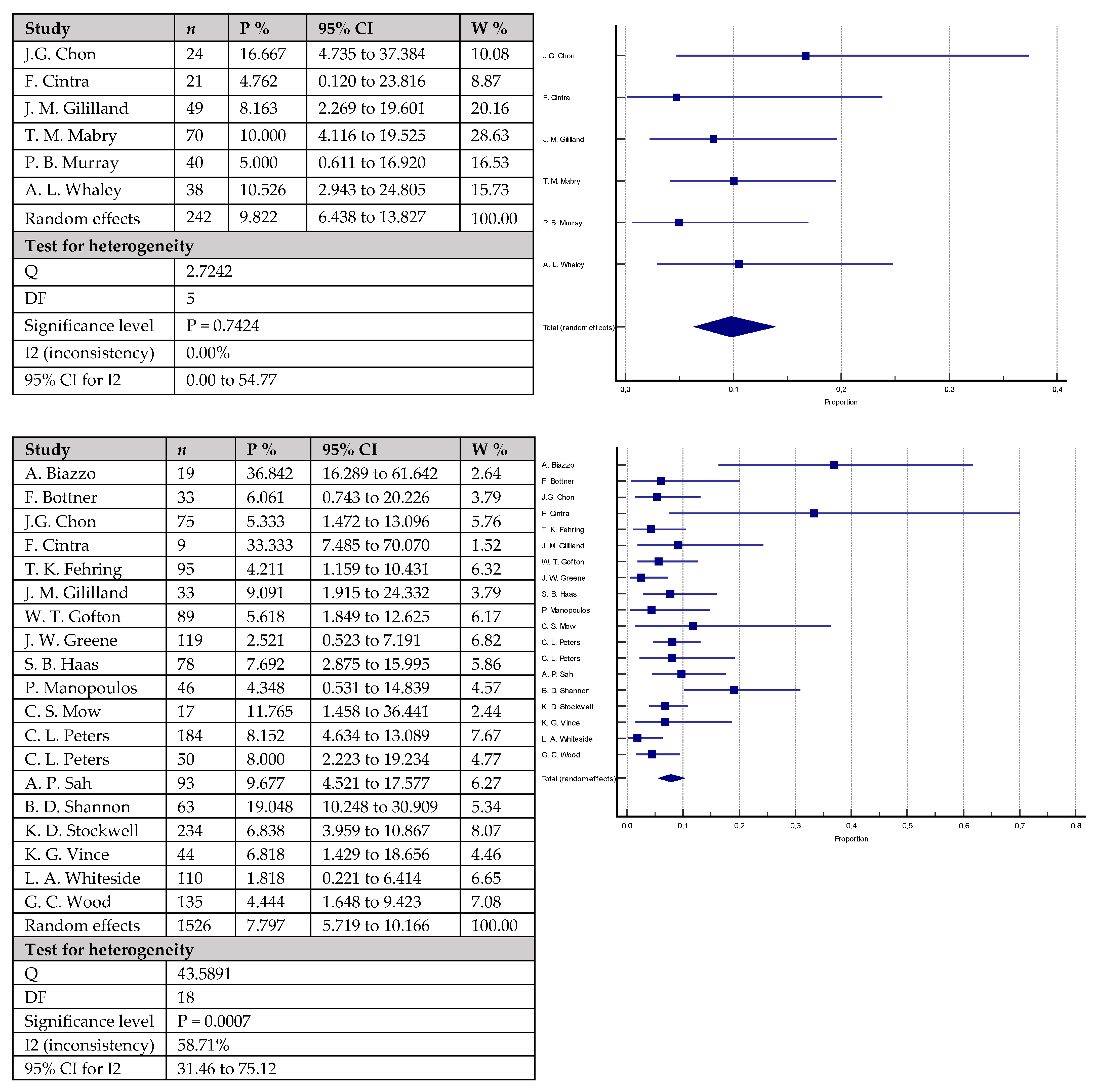
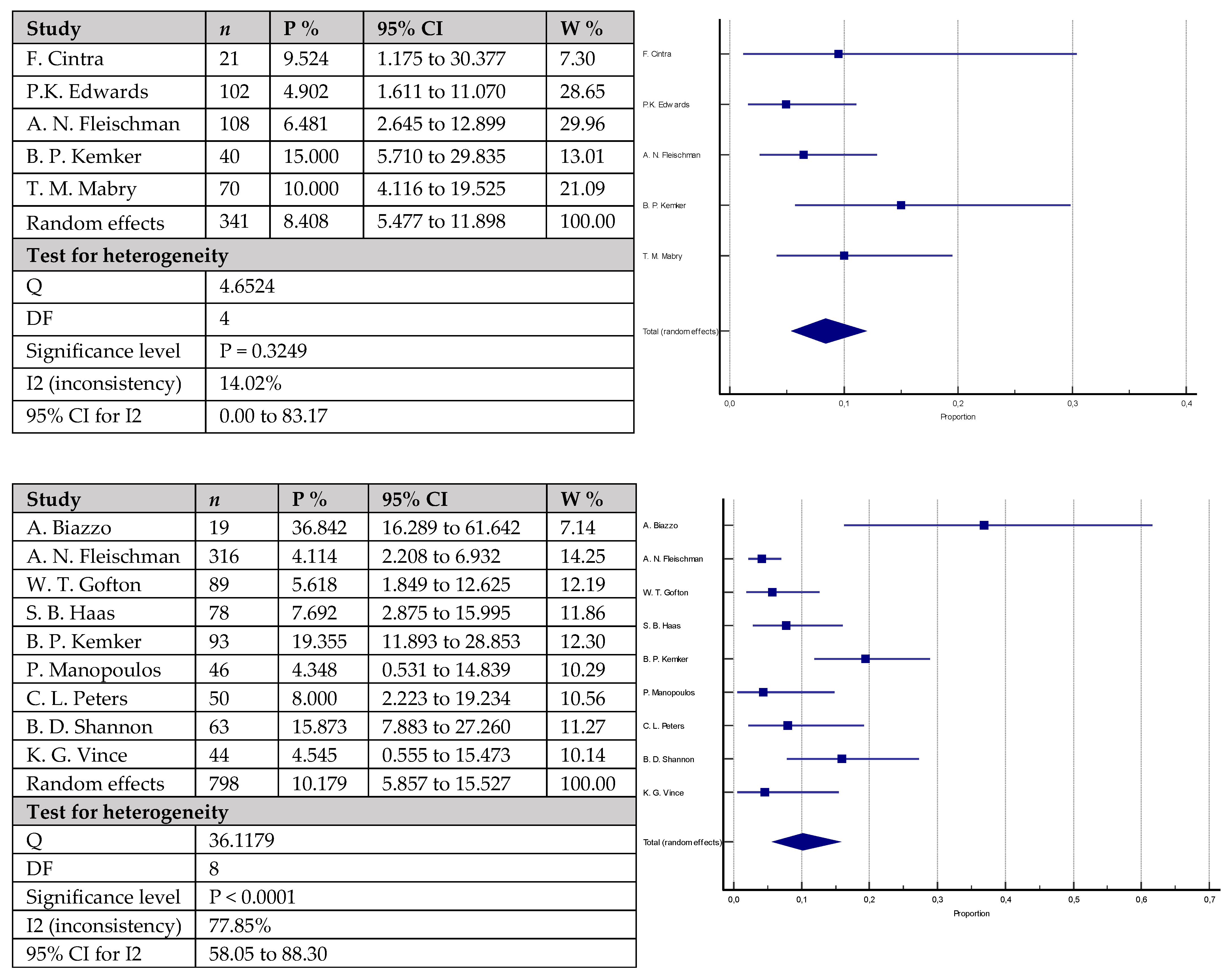
3.4. Results of Individual Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kurtz, S.M.; Lau, E.; Ong, K.; Zhao, K.; Kelly, M.; Bozic, K.J. Future young patient demand for primary and revision joint replacement: National projections from 2010 to 2030. Clin. Orthop. Relat. Res.® 2009, 467, 2606–2612. [Google Scholar] [CrossRef]
- Ravi, B.; Croxford, R.; Reichmann, W.M.; Losina, E.; Katz, J.N.; Hawker, G.A. The changing demographics of total joint arthroplasty recipients in the United States and Ontario from 2001 to 2007. Best Pract. Res. Clin. Rheumatol. 2012, 26, 637–647. [Google Scholar] [CrossRef]
- Wang, C.; Pfitzner, T.; von Roth, P.; Mayr, H.O.; Sostheim, M.; Hube, R. Fixation of stem in revision of total knee arthroplasty: Cemented versus cementless-a meta-analysis. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 3200–3211. [Google Scholar] [CrossRef]
- Figueroa, D.; Calvo, R.; Figueroa, F.; Avilés, C.; Garín, A.; Cancino, J. Clinical and functional outcomes of primary total knee arthroplasty: A South American perspective. Arthroplast. Today 2019, 5, 358–361. [Google Scholar] [CrossRef]
- Barrack, R.L.; McClure, J.T.; Burak, C.F.; Clohisy, J.C.; Parvizi, J.; Sharkey, P. Revision total knee arthroplasty: The patient’s perspective. Clin. Orthop. Relat. Res.® 2007, 464, 146–150. [Google Scholar] [CrossRef]
- Geary, M.B.; Macknet, D.M.; Ransone, M.P.; Odum, S.D.; Springer, B.D. Why Do Revision Total Knee Arthroplasties Fail? A Single-Center Review of 1632 Revision Total Knees Comparing Historic and Modern Cohorts. J. Arthroplast. 2020, 35, 2938–2943. [Google Scholar] [CrossRef]
- Murray, P.B.; Rand, J.A.; Hanssen, A.D. Cemented long-stem revision total knee arthroplasty. Clin. Orthop. Relat. Res.® 1994, 116–123. [Google Scholar]
- Completo, A.; Fonseca, F.; Simões, J.A. Strain shielding in proximal tibia of stemmed knee prosthesis: Experimental study. J. Biomech. 2008, 41, 560–566. [Google Scholar] [CrossRef]
- Jazrawi, L.M.; Bai, B.; Kummer, F.J.; Hiebert, R.; Stuchin, S.A. The effect of stem modularity and mode of fixation on tibial component stability in revision total knee arthroplasty. J. Arthroplast. 2001, 16, 759–767. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Santos, C.M.d.C.; Pimenta, C.A.d.M.; Nobre, M.R.C. The PICO strategy for the research question construction and evidence search. Rev. Lat.-Am. Enferm. 2007, 15, 508–511. [Google Scholar] [CrossRef]
- Freeman, M.F.; Tukey, J.W. Transformations Related to the Angular and the Square Root. Ann. Math. Stat. 1950, 21, 607–611. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Baggio, L.; Gil-González, S.; Barra-González, X.; Collado-Saenz, F.; Cruz-Olive, E. Cemented stems in revision total knee arthroplasty on patients older than 75 y/o. Clinical and radiological analysis. Acta Ortop. Mex. 2016, 30, 85–90. [Google Scholar]
- Bertin, K.C.; Freeman, M.A.; Samuelson, K.M.; Ratcliffe, S.S.; Todd, R.C. Stemmed revision arthroplasty for aseptic loosening of total knee replacement. J. Bone Jt. Surg. Br. 1985, 67, 242–248. [Google Scholar] [CrossRef]
- Biazzo, A.; D’Ambrosi, R.; Staals, E.; Masia, F.; Verde, F. Hybrid Cementation Technique Using the New Modular System for Aseptic Knee Arthroplasty Revision Surgery. Arch. Bone Jt. Surg. 2022, 10, 432–438. [Google Scholar] [CrossRef]
- Bottner, F.; Laskin, R.; Windsor, R.E.; Haas, S.B. Hybrid component fixation in revision total knee arthroplasty. Clin. Orthop. Relat. Res.® 2006, 446, 127–131. [Google Scholar] [CrossRef]
- Chon, J.G.; Lombardi, A.V., Jr.; Berend, K.R. Hybrid stem fixation in revision total knee arthroplasty (TKA). Surg. Technol. Int. 2004, 12, 214–220. [Google Scholar]
- Cintra, F.F.; Yepéz, A.K.; Rasga, M.G.; Abagge, M.; Alencar, P.G. Tibial component in revision of total knee arthroplasty: Comparison between cemented and hybrid fixation. Rev. Bras. Ortop. 2011, 46, 585–590. [Google Scholar] [CrossRef] [PubMed]
- Edwards, P.K.; Fehring, T.K.; Hamilton, W.G.; Perricelli, B.; Beaver, W.B.; Odum, S.M. Are cementless stems more durable than cemented stems in two-stage revisions of infected total knee arthroplasties? Clin. Orthop. Relat. Res.® 2014, 472, 206–211. [Google Scholar] [CrossRef]
- Fehring, T.K.; Odum, S.; Olekson, C.; Griffin, W.L.; Mason, J.B.; McCoy, T.H. Stem fixation in revision total knee arthroplasty: A comparative analysis. Clin. Orthop. Relat. Res.® 2003, 416, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Fleischman, A.N.; Azboy, I.; Fuery, M.; Restrepo, C.; Shao, H.; Parvizi, J. Effect of Stem Size and Fixation Method on Mechanical Failure after Revision Total Knee Arthroplasty. J. Arthroplast. 2017, 32, S202–S208. [Google Scholar] [CrossRef] [PubMed]
- Gililland, J.M.; Gaffney, C.J.; Odum, S.M.; Fehring, T.K.; Peters, C.L.; Beaver, W.B. Clinical & radiographic outcomes of cemented vs. diaphyseal engaging cementless stems in aseptic revision TKA. J. Arthroplast. 2014, 29, 224–228. [Google Scholar] [CrossRef]
- Gofton, W.T.; Tsigaras, H.; Butler, R.A.; Patterson, J.J.; Barrack, R.L.; Rorabeck, C.H. Revision total knee arthroplasty: Fixation with modular stems. Clin. Orthop. Relat. Res.® 2002, 404, 158–168. [Google Scholar] [CrossRef]
- Gómez-Vallejo, J.; Albareda-Albareda, J.; Seral-García, B.; Blanco-Rubio, N.; Ezquerra-Herrando, L. Revision total knee arthroplasty: Hybrid vs standard cemented fixation. J. Orthop. Traumatol. 2018, 19, 9. [Google Scholar] [CrossRef]
- Greene, J.W.; Reynolds, S.M.; Stimac, J.D.; Malkani, A.L.; Massini, M.A. Midterm results of hybrid cement technique in revision total knee arthroplasty. J. Arthroplast. 2013, 28, 570–574. [Google Scholar] [CrossRef]
- Haas, S.B.; Insall, J.N.; Montgomery, W., 3rd; Windsor, R.E. Revision total knee arthroplasty with use of modular components with stems inserted without cement. J. Bone Jt. Surg. Am. 1995, 77, 1700–1707. [Google Scholar] [CrossRef]
- Heesterbeek, P.J.; Wymenga, A.B.; van Hellemondt, G.G. No Difference in Implant Micromotion Between Hybrid Fixation and Fully Cemented Revision Total Knee Arthroplasty: A Randomized Controlled Trial with Radiostereometric Analysis of Patients with Mild-to-Moderate Bone Loss. J. Bone Jt. Surg. Am. 2016, 98, 1359–1369. [Google Scholar] [CrossRef]
- Iamaguchi, M.M.; de Castro, F.B.; Gobbi, R.G.; Tirico, L.E.; Pécora, J.R.; Camanho, G.L. Results of revision total knee arthroplasty using press-fit cementless stem. Acta Ortop. Bras. 2013, 21, 23–26. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kemker, B.P.; Sowers, C.B.; Seedat, R.; Satpathy, J.; Patel, N.K.; Lombardo, D.J.; Golladay, G.J. Comparing Revision Total Knee Arthroplasty Stems at a High-Volume Revision Center. Front. Surg. 2022, 9, 716510. [Google Scholar] [CrossRef] [PubMed]
- Kosse, N.M.; van Hellemondt, G.G.; Wymenga, A.B.; Heesterbeek, P.J. Comparable Stability of Cemented vs Press-Fit Placed Stems in Revision Total Knee Arthroplasty With Mild to Moderate Bone Loss: 6.5-Year Results From a Randomized Controlled Trial With Radiostereometric Analysis. J. Arthroplast. 2017, 32, 197–201. [Google Scholar] [CrossRef] [PubMed]
- Lachiewicz, P.F.; O’Dell, J.A. Is There a Difference between Cemented and Uncemented Femoral Stem Extensions in Revision Knee Arthroplasty? J. Knee Surg. 2020, 33, 84–88. [Google Scholar] [CrossRef]
- Larson, D.J.; Rosenberg, J.H.; Lawlor, M.A.; Garvin, K.L.; Hartman, C.W.; Lyden, E.; Konigsberg, B.S. Pain associated with cemented and uncemented long-stemmed tibial components in revision total knee arthroplasty. Bone Jt. J. 2021, 103B, 165–170. [Google Scholar] [CrossRef]
- Mabry, T.M.; Vessely, M.B.; Schleck, C.D.; Harmsen, W.S.; Berry, D.J. Revision total knee arthroplasty with modular cemented stems: Long-term follow-up. J. Arthroplast. 2007, 22, 100–105. [Google Scholar] [CrossRef]
- Manopoulos, P.; Havet, E.; Pearce, O.; Lardanchet, J.F.; Mertl, P. Mid- to long-term results of revision total knee replacement using press-fit intramedullary stems with cemented femoral and tibial components. J. Bone Jt. Surg. Br. 2012, 94, 937–940. [Google Scholar] [CrossRef]
- Miralles-Muñoz, F.A.; Ruiz-Lozano, M.; Perez-Aznar, A.; Sebastia-Forcada, E.; Lizaur-Utrilla, A.; Vizcaya-Moreno, M.F. Similar patient-reported outcomes for hybrid and cemented stem fixation for aseptic tibial revision total knee arthroplasty: A comparison of sequential prospective cohorts. Knee Surg. Sports Traumatol. Arthrosc. 2022, 30, 3992–3997. [Google Scholar] [CrossRef]
- Mow, C.S.; Wiedel, J.D. Noncemented revision total knee arthroplasty. Clin. Orthop. Relat. Res.® 1994, 309, 110–115. [Google Scholar]
- Peters, C.L.; Erickson, J.A.; Gililland, J.M. Clinical and radiographic results of 184 consecutive revision total knee arthroplasties placed with modular cementless stems. J. Arthroplast. 2009, 24, 48–53. [Google Scholar] [CrossRef]
- Peters, C.L.; Erickson, J.; Kloepper, R.G.; Mohr, R.A. Revision total knee arthroplasty with modular components inserted with metaphyseal cement and stems without cement. J. Arthroplast. 2005, 20, 302–308. [Google Scholar] [CrossRef] [PubMed]
- Sah, A.P.; Shukla, S.; Della Valle, C.J.; Rosenberg, A.G.; Paprosky, W.G. Modified hybrid stem fixation in revision TKA is durable at 2 to 10 years. Clin. Orthop. Relat. Res.® 2011, 469, 839–846. [Google Scholar] [CrossRef] [PubMed]
- Shannon, B.D.; Klassen, J.F.; Rand, J.A.; Berry, D.J.; Trousdale, R.T. Revision total knee arthroplasty with cemented components and uncemented intramedullary stems. J. Arthroplast. 2003, 18, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Stockwell, K.D.; Malleck, S.; Gascoyne, T.C.; Turgeon, T.R. Clinical and radiographic outcomes of a hybrid fixation revision total knee arthroplasty system at short to mid-term follow-up. Knee 2019, 26, 240–249. [Google Scholar] [CrossRef] [PubMed]
- Vince, K.G.; Long, W. Revision knee arthroplasty: The limits of press fit medullary fixation. Clin. Orthop. Relat. Res.® 1995, 317, 172–177. [Google Scholar]
- Whaley, A.L.; Trousdale, R.T.; Rand, J.A.; Hanssen, A.D. Cemented long-stem revision total knee arthroplasty. J. Arthroplast. 2003, 18, 592–599. [Google Scholar] [CrossRef]
- Whiteside, L.A. Cementless fixation in revision total knee arthroplasty. Clin. Orthop. Relat. Res.® 2006, 446, 140–148. [Google Scholar] [CrossRef]
- Winemaker, M.J.; Beingessner, D.M.; Rorabeck, C.H. Revision total knee arthroplasty: Should tibial stems be cemented or uncemented? Knee 1998, 5, 175–181. [Google Scholar] [CrossRef]
- Wood, G.C.; Naudie, D.D.; MacDonald, S.J.; McCalden, R.W.; Bourne, R.B. Results of press-fit stems in revision knee arthroplasties. Clin. Orthop. Relat. Res.® 2009, 467, 810–817. [Google Scholar] [CrossRef]
- Clatworthy, M.G.; Ballance, J.; Brick, G.W.; Chandler, H.P.; Gross, A.E. The use of structural allograft for uncontained defects in revision total knee arthroplasty. A minimum five-year review. J. Bone Jt. Surg. Am. 2001, 83, 404–411. [Google Scholar] [CrossRef]
- Nelson, C.L.; Vanushkina, M.; Irgit, K.; Strohecker, K.; Bowen, T.R. Stemmed femoral implants show lower failure rates in revision total knee arthroplasty. Knee 2015, 22, 429–434. [Google Scholar] [CrossRef] [PubMed]
- Meijer, M.F.; Reininga, I.H.F.; Boerboom, A.L.; Stevens, M.; Bulstra, S.K. Poorer survival after a primary implant during revision total knee arthroplasty. Int. Orthop. 2013, 37, 415–419. [Google Scholar] [CrossRef] [PubMed]
- Mullaji, A.; Shetty, G.M. Cemented stems: A requisite in revision total knee replacement. Bone Jt. J. 2014, 96B, 115–117. [Google Scholar] [CrossRef] [PubMed]
- Lachiewicz, P.F.; Soileau, E.S. A 30-mm cemented stem extension provides adequate fixation of the tibial component in revision knee arthroplasty. Clin. Orthop. Relat. Res.® 2015, 473, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Hernigou, P.; Dupuys, N.; Delambre, J.; Guissou, I.; Poignard, A.; Allain, J.; Flouzat Lachaniette, C.H. Long, titanium, cemented stems decreased late periprosthetic fractures and revisions in patients with severe bone loss and previous revision. Int. Orthop. 2015, 39, 639–644. [Google Scholar] [CrossRef]
- Whiteside, L.A. Cementless fixation issues in revision total knee arthroplasty. Instr. Course Lect. 1999, 48, 177–182. [Google Scholar] [PubMed]
- Dunne, N.; Tzagiollari, A.; Sahebalzamani, M.; Dunne, T.J. 8—Acrylic cements for bone fixation in joint replacement. In Joint Replacement Technology, 3rd ed.; Revell, P., Ed.; Woodhead Publishing: Sawston, UK, 2021; pp. 213–262. [Google Scholar] [CrossRef]
- Hines, C.B. Understanding Bone Cement Implantation Syndrome. AANA J. 2018, 86, 433–441. [Google Scholar]
- Rassir, R.; Schuiling, M.; Sierevelt, I.N.; van der Hoeven, C.W.P.; Nolte, P.A. What Are the Frequency, Related Mortality, and Factors Associated with Bone Cement Implantation Syndrome in Arthroplasty Surgery? Clin. Orthop. Relat. Res.® 2021, 479, 755–763. [Google Scholar] [CrossRef]
- Donaldson, A.J.; Thomson, H.E.; Harper, N.J.; Kenny, N.W. Bone cement implantation syndrome. Br. J. Anaesth. 2009, 102, 12–22. [Google Scholar] [CrossRef]
- Moldovan, F. Bone Cement Implantation Syndrome: A Rare Disaster Following Cemented Hip Arthroplasties-Clinical Considerations Supported by Case Studies. J. Pers. Med. 2023, 13, 1381. [Google Scholar] [CrossRef]
- Rothberg, D.L.; Kubiak, E.N.; Peters, C.L.; Randall, R.L.; Aoki, S.K. Reducing the risk of bone cement implantation syndrome during femoral arthroplasty. Orthopedics 2013, 36, e463–e467. [Google Scholar] [CrossRef]
- Hoskins, W.; van Bavel, D.; Lorimer, M.; de Steiger, R.N. Polished Cemented Femoral Stems Have a Lower Rate of Revision Than Matt Finished Cemented Stems in Total Hip Arthroplasty: An Analysis of 96,315 Cemented Femoral Stems. J. Arthroplast. 2018, 33, 1472–1476. [Google Scholar] [CrossRef] [PubMed]
- Mikolajczyk, T.; Moldovan, F.; Ciobanu, I.; Chalupczak, A.; Marin, A.G. Brain Research Using Computer Test. Procedia Technol. 2016, 22, 1113–1120. [Google Scholar] [CrossRef]
- O’dowd-Booth, C.J.; White, J.; Smitham, P.; Khan, W.; Marsh, D.R. Bone Cement: Perioperative Issues, Orthopaedic Applications and Future Developments. J. Perioper. Pract. 2011, 21, 304–308. [Google Scholar] [CrossRef] [PubMed]
- Yoshii, I.; Whiteside, L.A.; Milliano, M.T.; White, S.E. The effect of central stem and stem length on micromovement of the tibial tray. J. Arthroplast. 1992, 7, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Mihalko, W.M.; Whiteside, L.A. Stem pain after cementless revision total knee arthroplasty. J. Surg. Orthop. Adv. 2015, 24, 137–139. [Google Scholar]
- Barrack, R.L.; Rorabeck, C.; Burt, M.; Sawhney, J. Pain at the end of the stem after revision total knee arthroplasty. Clin. Orthop. Relat. Res.® 1999, 367, 216–225. [Google Scholar] [CrossRef]
- Kimpton, C.I.; Crocombe, A.D.; Bradley, W.N.; Gavin Huw Owen, B. Analysis of stem tip pain in revision total knee arthroplasty. J. Arthroplast. 2013, 28, 971–977. [Google Scholar] [CrossRef]
- Cipriano, C.A.; Brown, N.M.; Della Valle, C.J.; Moric, M.; Sporer, S.M. Intra-operative periprosthetic fractures associated with press fit stems in revision total knee arthroplasty: Incidence, management, and outcomes. J. Arthroplast. 2013, 28, 1310–1313. [Google Scholar] [CrossRef]
- Mills, K.; Wymenga, A.B.; van Hellemondt, G.G.; Heesterbeek, P.J.C. No difference in long-term micromotion between fully cemented and hybrid fixation in revision total knee arthroplasty: A randomized controlled trial. Bone Jt. J. 2022, 104B, 875–883. [Google Scholar] [CrossRef]
- Nelson, C.L.; Lonner, J.H.; Rand, J.A.; Lotke, P.A. Strategies of stem fixation and the role of supplemental bone graft in revision total knee arthroplasty. J. Bone Jt. Surg. Am. 2003, 85 (Suppl. S1), S52–S57. [Google Scholar] [CrossRef] [PubMed]
- Leta, T.H.; Lygre, S.H.; Skredderstuen, A.; Hallan, G.; Furnes, O. Failure of aseptic revision total knee arthroplasties. Acta Orthop. 2015, 86, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Ng, H.J.H.; Tan, G.K.Y.; Tan, R.G.; Kau, C.Y. Incidence of Radiolucent Lines after Cemented Total Knee Arthroplasty. Arch. Bone Jt. Surg. 2022, 10, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Whiteside, L.A. Cementless revision total knee arthroplasty. Clin. Orthop. Relat. Res.® 1993, 286, 160–167. [Google Scholar] [CrossRef]
- Mulpur, P.; Jayakumar, T.; Masilamani, A.B.S.; Hippalgaonkar, K.; Reddy, A.V.G. Unusual Failure of Modular TKA Prosthesis and Screw Migration following Revision Total Knee Arthroplasty. J. Orthop. Case Rep. 2022, 12, 25–29. [Google Scholar] [CrossRef]
- Scully, W.F.; Deren, M.E.; Bloomfield, M.R. Catastrophic tibial baseplate failure of a modern cementless total knee arthroplasty implant. Arthroplast. Today 2019, 5, 446–452. [Google Scholar] [CrossRef]
- Fokter, S.K.; Gubeljak, N.; Punzón-Quijorna, E.; Pelicon, P.; Kelemen, M.; Vavpetič, P.; Predan, J.; Ferlič, L.; Novak, I. Total Knee Replacement with an Uncemented Porous Tantalum Tibia Component: A Failure Analysis. Materials 2022, 15, 2575. [Google Scholar] [CrossRef]
- Gibon, E.; Vasilopoulos, T.; Sipavicius, E.; Deen, J.T.; Prieto, H.A.; Gray, C.F.; Parvataneni, H.K.; Pulido, L. Surgical Management of Tibial Bone Loss in Revision Total Knee Arthroplasty: Clinical Outcomes and Radiographic Analysis of Tantalum Cones, Titanium Cones and Titanium Sleeves. Iowa Orthop. J. 2022, 42, 145–153. [Google Scholar]
- Bobyn, J.D.; Poggie, R.A.; Krygier, J.J.; Lewallen, D.G.; Hanssen, A.D.; Lewis, R.J.; Unger, A.S.; O’Keefe, T.J.; Christie, M.J.; Nasser, S.; et al. Clinical validation of a structural porous tantalum biomaterial for adult reconstruction. J. Bone Jt. Surg. Am. 2004, 86 (Suppl. S2), 123–129. [Google Scholar] [CrossRef]
- Meneghini, R.M.; Lewallen, D.G.; Hanssen, A.D. Use of porous tantalum metaphyseal cones for severe tibial bone loss during revision total knee replacement. J. Bone Jt. Surg. Am. 2008, 90, 78–84. [Google Scholar] [CrossRef]
- Kamath, A.F.; Lewallen, D.G.; Hanssen, A.D. Porous tantalum metaphyseal cones for severe tibial bone loss in revision knee arthroplasty: A five to nine-year follow-up. J. Bone Jt. Surg. Am. 2015, 97, 216–223. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Year | Fixation | Antibiotic-Impregnated Cement? | No of Knees | Mean Age (Years) | Male % | Female % | Follow-up (Months) | |
|---|---|---|---|---|---|---|---|---|---|
| L. Baggio [16] | 2016 | c | Yes | Gentamicin | 27 | 82.6 | 33.3 | 66.7 | 43 |
| K.C. Bertin [17] | 1985 | u | - | - | 53 | - | 32.1 | 67.9 | 18 |
| A. Biazzo [18] | 2022 | u | - | - | 19 | 69.9 | 21.1 | 78.9 | 33.6 |
| F. Bottner [19] | 2006 | u | - | - | 33 | 68 | 36.4 | 63.6 | 38 |
| J.G. Chon [20] | 2004 | c | n/a | n/a | 24 | 65 | - | - | 44 |
| u | - | - | 75 | 65 | - | - | 44 | ||
| F. Cintra [21] | 2011 | c | Yes | Gentamicin (1 g per dose) | 21 | 62.8 | 46.2 | 53.8 | 62 |
| u | - | - | 9 | 42 | |||||
| P.K. Edwards [22] | 2014 | c | Yes | Not recorded | 102 | 65 | 38.5 | 61.5 | 45 |
| u | - | - | 126 | 65 | 49.2 | 50.8 | 52 | ||
| T. K. Fehring [23] | 2003 | c | Yes | Not recorded | 107 | 67.5 | 38.5 | 61.5 | 53 |
| u | - | - | 95 | 61 | |||||
| A. N. Fleischman [24] | 2017 | c | Yes | Not recorded | 108 | 65.8 | 30.6 | 69.4 | 64.3 |
| u | - | - | 316 | 63.9 | 42.7 | 57.3 | 59.6 | ||
| J. M. Gililland [25] | 2014 | c | Yes | Not recorded | 49 | 65 | 49 | 51 | 76 |
| u | - | - | 33 | 64 | 33.3 | 66.7 | 121 | ||
| W. T. Gofton [26] | 2002 | u | - | - | 89 | 69.1 | 36 | 64 | 70.8 |
| J. Gómez-Vallejo [27] | 2018 | c | No | - | 29 | 79.7 | - | - | 84 |
| u | - | - | 38 | 78.4 | - | - | |||
| J. W. Greene [28] | 2013 | u | - | - | 119 | 67 | 53.8 | 46.2 | 62 |
| S. B. Haas [29] | 1995 | u | - | - | 78 | 61 | 35.9 | 64.1 | 42 |
| P. J. Heesterbeek [30] | 2016 | c | Yes | Gentamicin Gentamicin/Clindamycin Gentamicin/Vancomycin | 15 | 67 | 37.5 | 62.5 | 24 |
| u | - | - | 15 | 64.5 | 18.7 | 81.3 | |||
| M. M. Iamaguchi [31] | 2013 | u | - | - | 35 | 68.5 | 40 | 60 | 26.4 |
| B. P. Kemker [32] | 2022 | c | n/a | n/a | 40 | 63.8 | 32.5 | 67.5 | 24.6 |
| u | - | - | 93 | 63.8 | 36.6 | 63.4 | 24.6 | ||
| N. M. Kosse [33] | 2017 | c | Yes | Gentamicin Gentamicin/Clindamycin Gentamicin/Vancomycin | 12 | 73 | 33.3 | 66.7 | 78 |
| u | - | - | 11 | 67 | 20 | 80 | |||
| P. F. Lachiewicz [34] | 2020 | c | Yes | Gentamicin/Tobramycin | 34 | 68 | 38.2 | 61.8 | 72 |
| u | - | - | 50 | 68 | 38 | 62 | |||
| D. J. Larson [35] | 2021 | c | n/a | n/a | 63 | 65.9 | 47.6 | 52.4 | 60 |
| u | - | - | 47 | 66 | 57.4 | 42.6 | |||
| T. M. Mabry [36] | 2007 | c | Yes | Not recorded | 70 | 73 | 55.7 | 44.3 | 122.4 |
| P. Manopoulos [37] | 2012 | u | - | - | 46 | 69 | 37 | 63 | 102 |
| F. A. Miralles-Muñoz [38] | 2022 | c | Yes | Not recorded | 31 | 67.8 | 38.7 | 61.3 | 75.6 |
| u | - | - | 42 | 65.3 | 40.5 | 59.5 | 75.6 | ||
| C. S. Mow [39] | 1994 | u | - | - | 17 | 65 | 58.8 | 41.2 | 72 |
| P. B. Murray [7] | 1994 | c | n/a | n/a | 40 | 67.2 | 47.5 | 52.5 | 58.2 |
| C. L. Peters [40] | 2009 | u | - | - | 184 | 63 | 32.6 | 67.4 | 48 |
| C. L. Peters [41] | 2005 | u | - | - | 50 | 68 | 32 | 68 | 36 |
| A. P. Sah [42] | 2011 | u | - | - | 93 | 68.8 | 33.3 | 66.7 | 65 |
| B. D. Shannon [43] | 2003 | u | - | - | 63 | 66 | 52.4 | 47.6 | 69 |
| K. D. Stockwell [44] | 2019 | u | - | - | 234 | 68 | 43.2 | 56.8 | 58.8 |
| K. G. Vince [45] | 1995 | u | - | - | 44 | - | - | - | 24–72 |
| A. L. Whaley [46] | 2003 | c | n/a | n/a | 38 | 67 | 42.1 | 57.9 | 121.2 |
| L. A. Whiteside [47] | 2006 | u | - | - | 110 | 73 | 40 | 60 | 60–127 |
| M. J. Winemaker [48] | 1998 | c | n/a | n/a | 17 | 71.9 | 33.3 | 66.7 | 28 |
| u | - | - | 15 | 69.8 | 28 | ||||
| G. C. Wood [49] | 2009 | u | - | - | 135 | 71 | 41.5 | 58.5 | 60 |
| Parameter/Rate | Cementless Fixation | Cemented Fixation | p-Value | ||
|---|---|---|---|---|---|
| Value | 95% CI | Value | 95% CI | ||
| Revision | 7.797% | 5.719–10.166 | 9.822% | 6.428–13.827 | 0.2613 |
| Failure | 10.179% | 5.857–15.527 | 8.408% | 5.477–11.898 | 0.3559 |
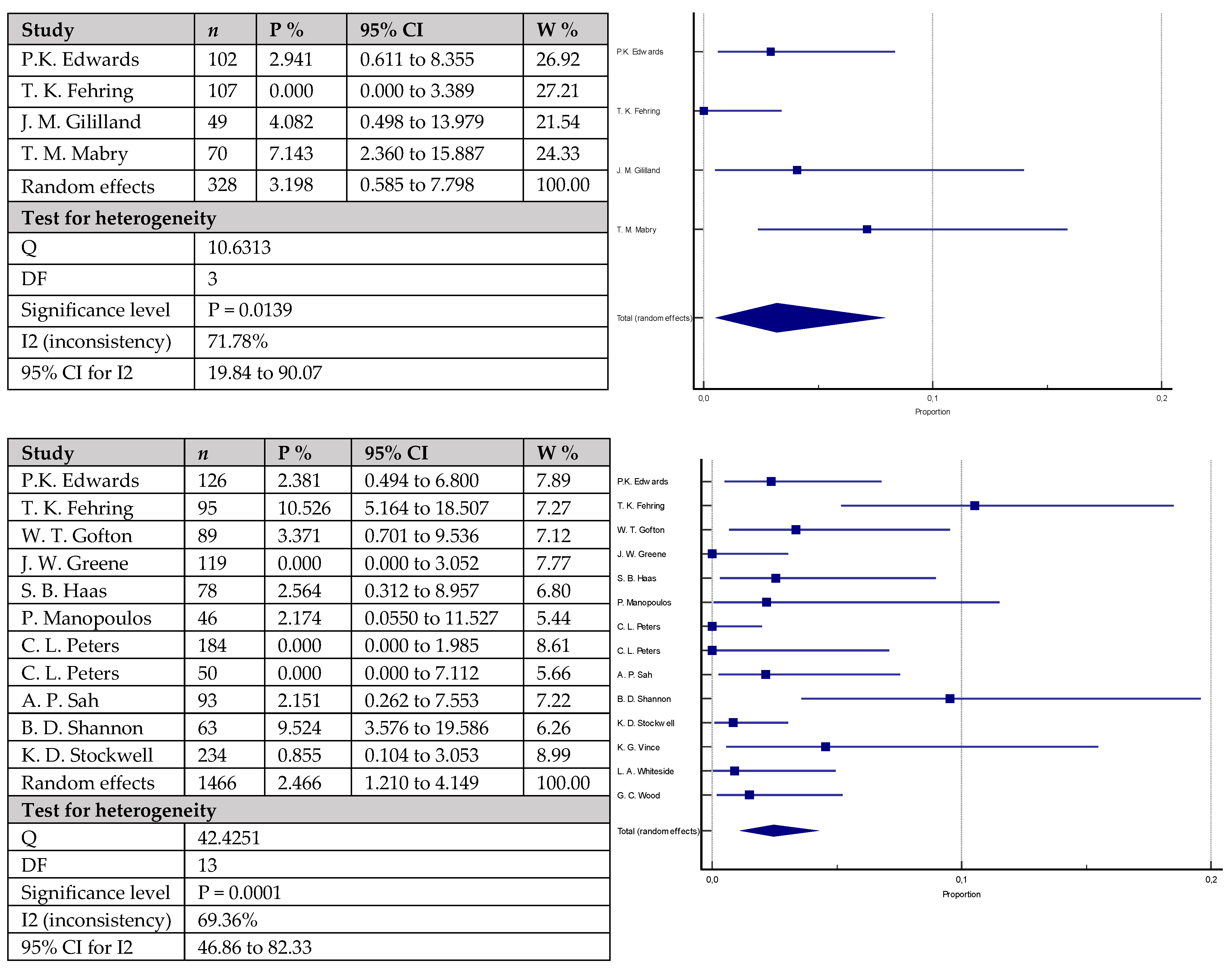
| Asepticloosening | 2.466% | 1.210–4.149 | 3.198% | 0.585–7.798 | 0.3999 |
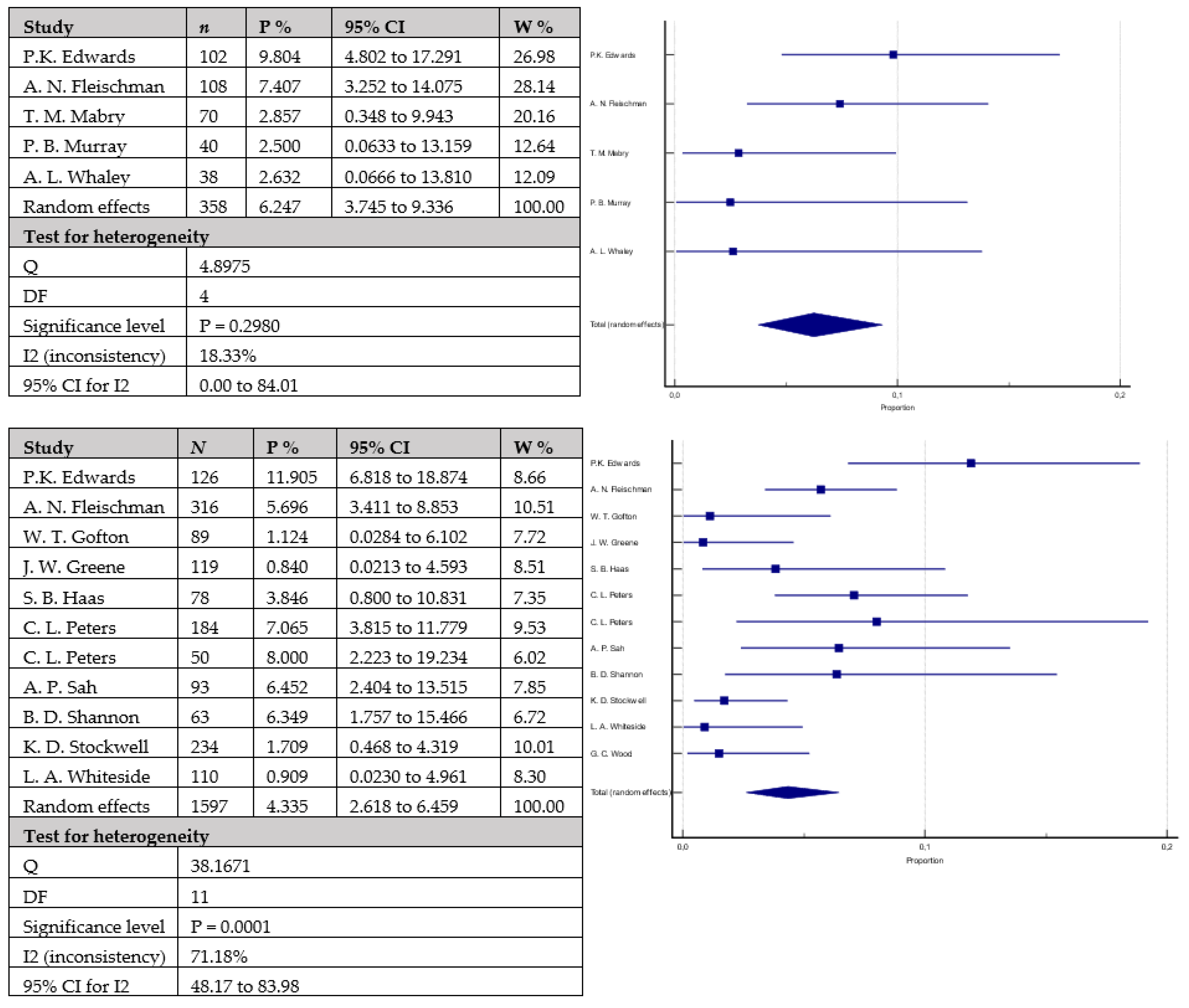
| Periprosthetic infection | 4.335% | 2.618–6.459 | 6.247% | 3.745–9.336 | 0.1010 |
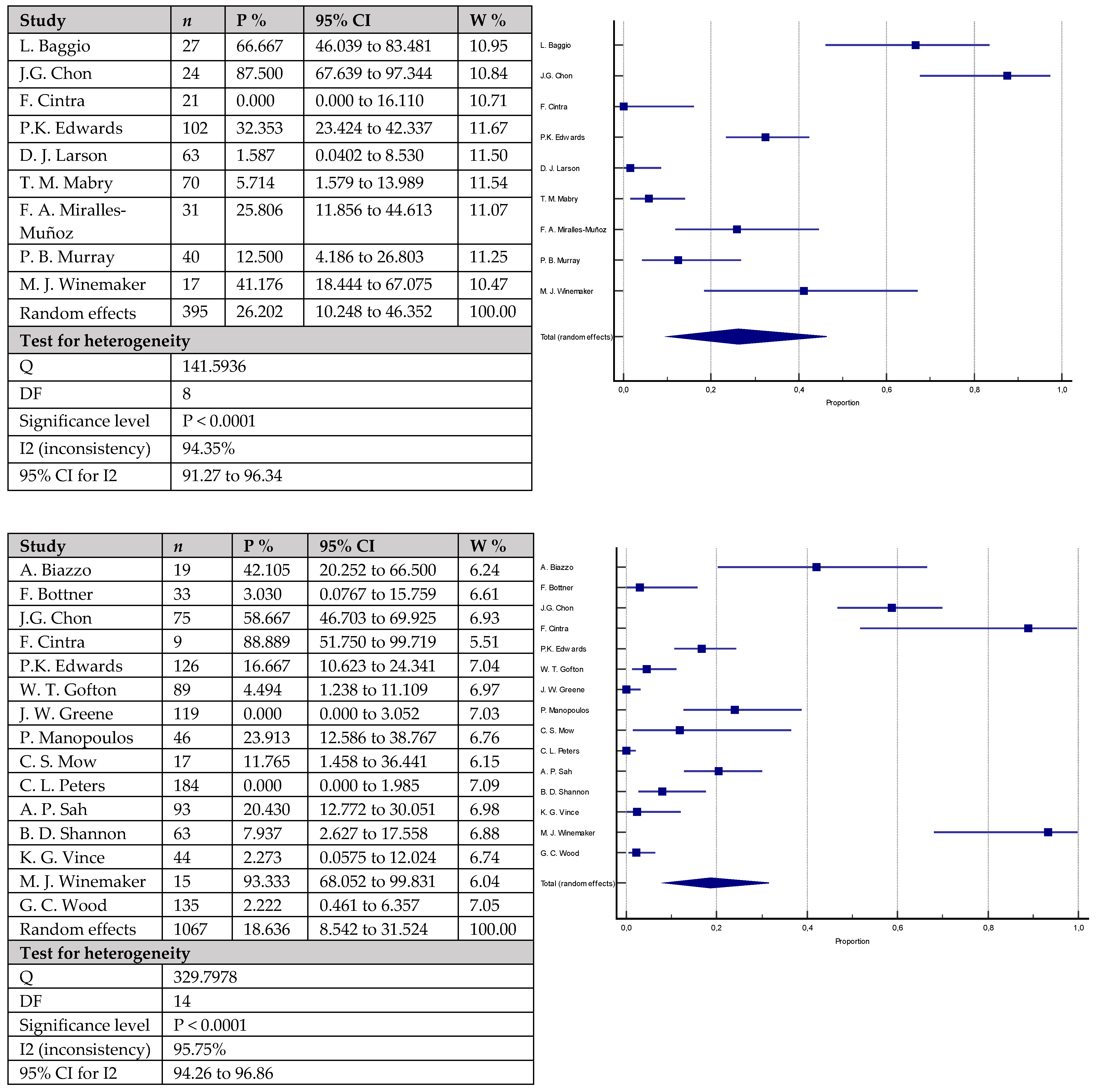
| Radiolucent lines | 18.636% | 8.542–31.524 | 26.202% | 10.248–46.352 | <0.0001 * |
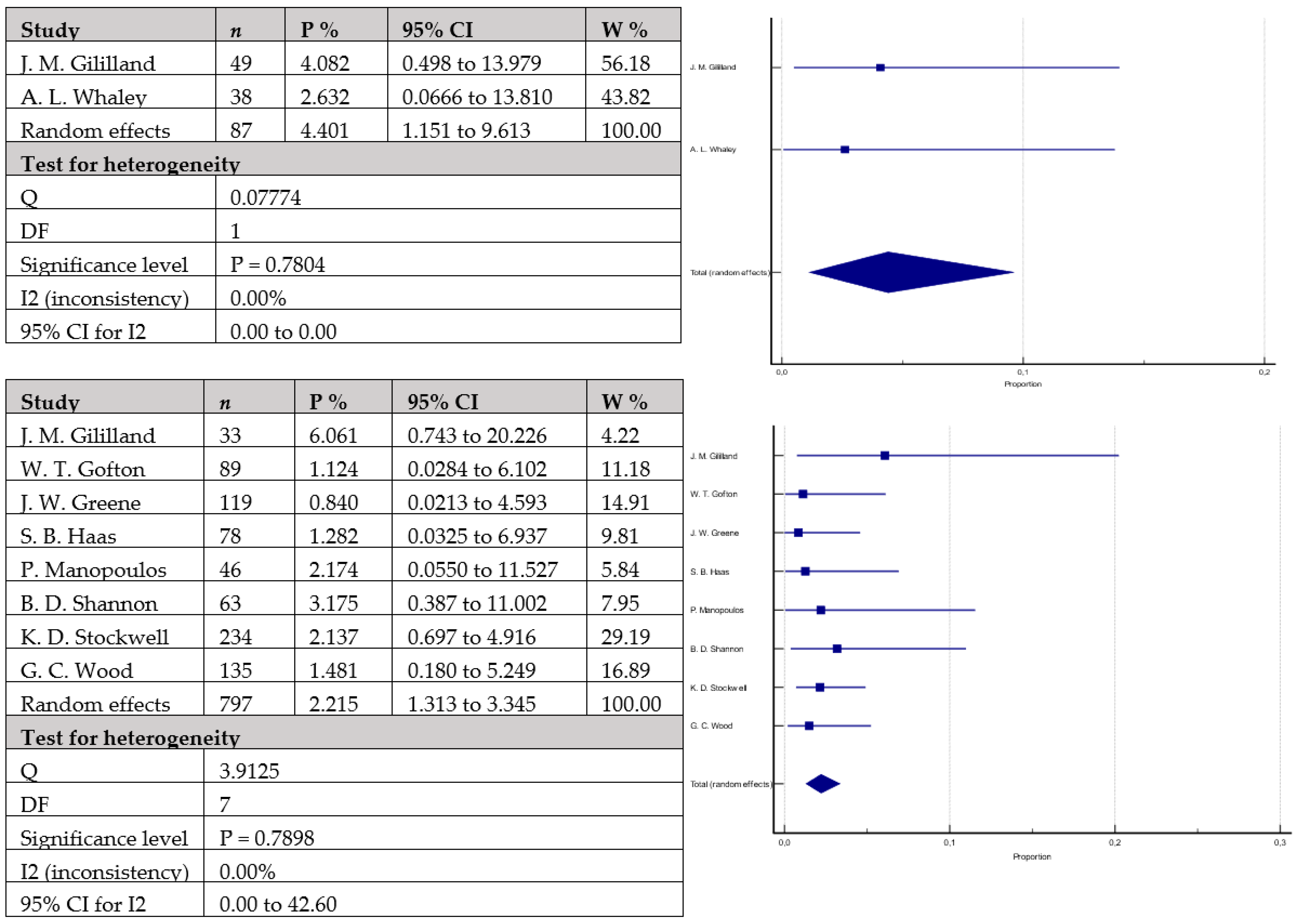
| Instability | 2.215% | 1.313–3.345 | 4.401% | 1.151–9.613 | 0.2621 |
| KSS total | 149.47 ± 16.22 points | 138.15 ± 12.89 points | 0.3780 | ||
| KSS functional | 58.81 ± 12.40 points | 65.51 ± 12.03 points | 0.2678 | ||
| KSS clinical | 81.81 ± 5.06 points | 76.20 ± 12.37 points | 0.0841 | ||
| WOMAC | 82.36 ± 3.01 points | 75.65 ± 8.03 points | 0.3235 | ||
| Range of motion | 101.75 ± 5.32 degrees | 96.09 ± 8.32 degrees | 0.1036 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Darwich, A.; Jovanovic, A.; Dally, F.-J.; Abd El Hai, A.; Baumgärtner, T.; Assaf, E.; Gravius, S.; Hetjens, S.; Bdeir, M. Cemented versus Cementless Stem Fixation in Revision Total Knee Arthroplasty: A Systematic Review and Meta-Analysis. Antibiotics 2023, 12, 1633. https://doi.org/10.3390/antibiotics12111633
Darwich A, Jovanovic A, Dally F-J, Abd El Hai A, Baumgärtner T, Assaf E, Gravius S, Hetjens S, Bdeir M. Cemented versus Cementless Stem Fixation in Revision Total Knee Arthroplasty: A Systematic Review and Meta-Analysis. Antibiotics. 2023; 12(11):1633. https://doi.org/10.3390/antibiotics12111633
Chicago/Turabian StyleDarwich, Ali, Andrea Jovanovic, Franz-Joseph Dally, Asseel Abd El Hai, Tobias Baumgärtner, Elio Assaf, Sascha Gravius, Svetlana Hetjens, and Mohamad Bdeir. 2023. "Cemented versus Cementless Stem Fixation in Revision Total Knee Arthroplasty: A Systematic Review and Meta-Analysis" Antibiotics 12, no. 11: 1633. https://doi.org/10.3390/antibiotics12111633
APA StyleDarwich, A., Jovanovic, A., Dally, F.-J., Abd El Hai, A., Baumgärtner, T., Assaf, E., Gravius, S., Hetjens, S., & Bdeir, M. (2023). Cemented versus Cementless Stem Fixation in Revision Total Knee Arthroplasty: A Systematic Review and Meta-Analysis. Antibiotics, 12(11), 1633. https://doi.org/10.3390/antibiotics12111633