
Recent Advances in Pharmaceutical Approaches of Antimicrobial Agents for Selective Delivery in Various Administration Routes

 ,
,
Abstract
1. Introduction
2. Sites of Infection
2.1. Skin and Soft Tissue Infections
2.2. Mucosal Layer Infections
2.3. Respiratory Tract Infections
2.4. Gastrointestinal Infections
2.5. Urinary Tract Infections (UTI)
2.6. Lymphatic Infections
2.7. Central Nervous System (CNS) Infections
3. Commonly Used Antimicrobials for the Treatment of Infectious Diseases Caused by Microorganisms
3.1. Skin Infection
3.1.1. Bacterial
3.1.2. Fungi
3.1.3. Viral
3.2. Mucosal Infection
3.2.1. Bacterial
3.2.2. Fungi
3.3. Pulmonary Infection
3.3.1. Bacterial
3.3.2. Viral
- A.
- Ribavirin
- B.
- Cidofovir
- Inhibitors of proteases
- b.
- siRNA
3.4. CNS Infection
3.4.1. Bacterial
3.4.2. Viral
3.4.3. Fungi
3.5. Gastrointestinal Infection
3.5.1. Bacterial
3.5.2. Viral
3.5.3. Protozoa
3.6. Lymphatic Infection
3.6.1. Bacterial
3.6.2. Viral
3.6.3. Parasites
4. A New Approach of Antimicrobials Drug Delivery Systems for the Treatment of Infectious Diseases through Stimuli-Responsive Development
4.1. Skin and Soft Tissue Infection
4.1.1. pH-Responsive Delivery System
4.1.2. Enzyme-Responsive Delivery System
4.1.3. Redox-Responsive Delivery System
4.1.4. Temperature-Responsive Delivery System
4.1.5. Magnetic-Responsive Delivery System
4.1.6. Light-Responsive Delivery System
4.2. Mucosal Layer Infection
4.2.1. Vaginal Infection
pH-Responsive Delivery System
Enzyme-Responsive Delivery System
Temperature-Responsive Delivery System
4.2.2. Ocular/Eye Infection
pH-Responsive Delivery System
Enzyme-Responsive Delivery System
Temperature-Responsive Delivery System
4.3. Respiratory Tract Infections
4.3.1. Tuberculosis
pH-Responsive Delivery System
Enzyme-Responsive Delivery System
Temperature-Responsive Delivery System
Light-Responsive Delivery System
4.3.2. Cystic Fibrosis
pH-Responsive Delivery System
Enzyme-Responsive Delivery System
Temperature-Responsive Delivery System

Redox-Responsive Delivery System
Light-Responsive Delivery System
4.4. Gastrointestinal Infection
4.4.1. pH-Responsive Delivery System
4.4.2. Enzyme-Responsive Delivery System
4.4.3. Temperature-Responsive Delivery System
4.4.4. Light-Responsive Delivery System
4.5. Urinary Tract Infection (UTI)
4.5.1. pH-Responsive Delivery System
4.5.2. Enzyme-Responsive Delivery System
4.6. Lymphatic Infections
4.6.1. pH-Responsive Delivery System
4.6.2. Enzyme-Responsive Delivery System
4.7. CNS Infections
4.7.1. pH-Responsive Delivery System
4.7.2. Temperature-Responsive Delivery System
4.7.3. Redox-Responsive Delivery System
5. Conclusions and Future Perspective
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yeh, Y.C.; Huang, T.H.; Yang, S.C.; Chen, C.C.; Fang, J.Y. Nano-Based Drug Delivery or Targeting to Eradicate Bacteria for Infection Mitigation: A Review of Recent Advances. Front. Chem. 2020, 8, 286. [Google Scholar] [CrossRef] [PubMed]
- Zhong, C.; Wu, Y.; Lin, H.; Liu, R. Advances in the antimicrobial treatment of osteomyelitis. Compos. Part B Eng. 2023, 249, 110428. [Google Scholar] [CrossRef]
- Theuretzbacher, U.; Outterson, K.; Engel, A.; Karlén, A. The global preclinical antibacterial pipeline. Nat. Rev. Microbiol. 2020, 18, 275–285. [Google Scholar] [CrossRef] [PubMed]
- Gigante, V.; Sati, H.; Beyer, P. Recent advances and challenges in antibacterial drug development. ADMET DMPK 2022, 10, 147–151. [Google Scholar] [CrossRef]
- Maxson, T.; Mitchell, D.A. Targeted treatment for bacterial infections: Prospects for pathogen-specific antibiotics coupled with rapid diagnostics. Tetrahedron 2016, 72, 3609–3624. [Google Scholar] [CrossRef]
- Gao, W.; Thamphiwatana, S.; Angsantikul, P.; Zhang, L. Nanoparticle approaches against bacterial infections. Wiley Interdiscip. Rev. Nanomed. Nanobiotechnol. 2014, 6, 532–547. [Google Scholar] [CrossRef]
- Devarajan, P.V.; Dawre, S.M.; Dutta, R. Infectious Diseases: Need for Targeted Drug Delivery. In Targeted Drug Delivery: Concepts and Design; Springer: Berlin/Heidelberg, Germany, 2015; pp. 113–148. [Google Scholar] [CrossRef]
- Chen, H.; Jin, Y.; Wang, J.; Wang, Y.; Jiang, W.; Dai, H.; Pang, S.; Lei, L.; Ji, J.; Wang, B. Design of smart targeted and responsive drug delivery systems with enhanced antibacterial properties. Nanoscale 2018, 10, 20946–20962. [Google Scholar] [CrossRef]
- Liu, M.; Du, H.; Zhang, W.; Zhai, G. Internal stimuli-responsive nanocarriers for drug delivery: Design strategies and applications. Mater. Sci. Eng. C 2017, 71, 1267–1280. [Google Scholar] [CrossRef]
- Llor, C.; Bjerrum, L. Antimicrobial resistance: Risk associated with antibiotic overuse and initiatives to reduce the problem. Ther. Adv. Drug Saf. 2014, 5, 229–241. [Google Scholar] [CrossRef]
- Prestinaci, F.; Pezzotti, P.; Pantosti, A. Antimicrobial resistance: A global multifaceted phenomenon. Pathog. Glob. Health 2015, 109, 309–318. [Google Scholar] [CrossRef]
- Sikder, A.; Chaudhuri, A.; Mondal, S.; Singh, N.D.P. Recent Advances on Stimuli-Responsive Combination Therapy against Multidrug-Resistant Bacteria and Biofilm. ACS Appl. Bio Mater. 2021, 4, 4667–4683. [Google Scholar] [CrossRef] [PubMed]
- Radovic-Moreno, A.F.; Lu, T.K.; Puscasu, V.A.; Yoon, C.J.; Langer, R.; Farokhzad, O.C. Surface charge-switching polymeric nanoparticles for bacterial cell wall-targeted delivery of antibiotics. ACS Nano 2012, 6, 4279–4287. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Ding, C.; Wang, Y.; Tan, H.; Li, J. PH-Responsive polymeric nanocarriers for efficient killing of cariogenic bacteria in biofilms. Biomater. Sci. 2019, 7, 1643–1651. [Google Scholar] [CrossRef] [PubMed]
- Du, X.; Li, X.; Xiong, L.; Zhang, X.; Kleitz, F.; Qiao, S.Z. Mesoporous silica nanoparticles with organo-bridged silsesquioxane framework as innovative platforms for bioimaging and therapeutic agent delivery. Biomaterials 2016, 91, 90–127. [Google Scholar] [CrossRef]
- Shao, D.; Li, M.; Wang, Z.; Zheng, X.; Lao, Y.H.; Chang, Z.; Zhang, F.; Lu, M.; Yue, J.; Hu, H.; et al. Bioinspired Diselenide-Bridged Mesoporous Silica Nanoparticles for Dual-Responsive Protein Delivery. Adv. Mater. 2018, 30, 1801198. [Google Scholar] [CrossRef]
- Nurul Fitri Marzaman, A.; Sartini Mudjahid, M.; Puspita Roska, T.; Sam, A.; Permana, A.D. Development of chloramphenicol whey protein-based microparticles incorporated into thermoresponsive in situ hydrogels for improved wound healing treatment. Int. J. Pharm. 2022, 628, 122323. [Google Scholar] [CrossRef]
- Yao, Q.; Ye, Z.; Sun, L.; Jin, Y.; Xu, Q.; Yang, M.; Wang, Y.; Zhou, Y.; Ji, J.; Chen, H.; et al. Bacterial infection microenvironment-responsive enzymatically degradable multilayer films for multifunctional antibacterial properties. J. Mater. Chem. B 2017, 5, 8532–8541. [Google Scholar] [CrossRef]
- Gebreyohannes, G.; Nyerere, A.; Bii, C.; Sbhatu, D.B. Challenges of intervention, treatment, and antibiotic resistance of biofilm-forming microorganisms. Heliyon 2019, 5, e02192. [Google Scholar] [CrossRef]
- Vestby, L.K.; Grønseth, T.; Simm, R.; Nesse, L.L. Bacterial biofilm and its role in the pathogenesis of disease. Antibiotics 2020, 9, 59. [Google Scholar] [CrossRef]
- Wu, H.; Moser, C.; Wang, H.Z.; Høiby, N.; Song, Z.J. Strategies for combating bacterial biofilm infections. Int. J. Oral Sci. 2015, 7, 1–7. [Google Scholar] [CrossRef]
- Park, W.; Bae, B.-C.; Na, K. A highly tumor-specific light-triggerable drug carrier responds to hypoxic tumor conditions for effective tumor treatment. Biomaterials 2016, 77, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Higuchi, A.; Ling, Q.-D.; Kumar, S.S.; Chang, Y.; Kao, T.-C.; Munusamy, M.A.; Alarfaj, A.A.; Hsu, S.-T.; Umezawa, A. External stimulus-responsive biomaterials designed for the culture and differentiation of ES, iPS, and adult stem cells. Prog. Polym. Sci. 2014, 39, 1585–1613. [Google Scholar] [CrossRef]
- Laurent, S.; Dutz, S.; Häfeli, U.O.; Mahmoudi, M. Magnetic fluid hyperthermia: Focus on superparamagnetic iron oxide nanoparticles. Adv. Colloid Interface Sci. 2011, 166, 8–23. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.; Yang, F.; Xiong, F.; Gu, N. The smart drug delivery system and its clinical potential. Theranostics 2016, 6, 1306–1323. [Google Scholar] [CrossRef]
- Patel, U.; Rathnayake, K.; Jani, H.; Jayawardana, K.W.; Dhakal, R.; Duan, L.; Jayawardena, S.N. Near-infrared responsive targeted drug delivery system that offer chemo-photothermal therapy against bacterial infection. Nano Sel. 2021, 2, 1750–1769. [Google Scholar] [CrossRef]
- Wu, G.; Mikhailovsky, A.; Khant, H.A.; Fu, C.; Chiu, W.; Zasadzinski, J.A. Remotely Triggered Liposome Release by Near-Infrared Light Absorption via Hollow Gold Nanoshells. J. Am. Chem. Soc. 2008, 130, 8175–8177. [Google Scholar] [CrossRef]
- Geilich, B.M.; Gelfat, I.; Sridhar, S.; van de Ven, A.L.; Webster, T.J. Superparamagnetic iron oxide-encapsulating polymersome nanocarriers for biofilm eradication. Biomaterials 2017, 119, 78–85. [Google Scholar] [CrossRef]
- Grice, E.A.; Segre, J.A. The skin microbiome. Nat. Rev. Microbiol. 2011, 9, 244–253. [Google Scholar] [CrossRef]
- Leong, H.N.; Kurup, A.; Tan, M.Y.; Kwa, A.L.H.; Liau, K.H.; Wilcox, M.H. Management of complicated skin and soft tissue infections with a special focus on the role of newer antibiotics. Infect. Drug Resist. 2018, 11, 1959–1974. [Google Scholar] [CrossRef]
- Ramsay, I.D.; Török, M.E. Skin and soft tissue infections. Medicine 2017, 45, 699–706. [Google Scholar] [CrossRef]
- Ramakrishnan, K.; Salinas, R.C.; Ivan, N.; Higuita, A. Skin and Soft Tissue Infections. Am. Fam. Physician 2015, 92, 474–483. [Google Scholar] [PubMed]
- Ki, V.; Rotstein, C. Bacterial skin and soft tissue infections in adults: A review of their epidemiology, pathogenesis, diagnosis, treatment and site of care. Can. J. Infect. Dis. Med. Microbiol. 2018, 19, 173–184. [Google Scholar] [CrossRef] [PubMed]
- Dryden, M.S. Complicated skin and soft tissue infection. J. Antimicrob. Chemother. 2010, 65, iii35–iii44. [Google Scholar] [CrossRef] [PubMed]
- Watson, S.; Cabrera-Aguas, M.; Khoo, P. Common eye infections. Aust. Prescr. 2018, 41, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Teweldemedhin, M.; Gebreyesus, H.; Atsbaha, A.H.; Asgedom, S.W.; Saravanan, M. Bacterial profile of ocular infections: A systematic review. BMC Ophthalmol. 2017, 17, 212. [Google Scholar] [CrossRef]
- Deepthi, K.N.G.; Prabagaran, S.R. Ocular bacterial infections: Pathogenesis and diagnosis. Microb. Pathog. 2020, 145, 104206. [Google Scholar] [CrossRef]
- Austin, A.; Lietman, T.; Rose-Nussbaumer, J. Update on the Management of Infectious Keratitis. Ophthalmology 2017, 124, 1678–1689. [Google Scholar] [CrossRef]
- Relhan, N.; Flynn, H.W. Endophthalmitis Caused by Gram-Negative Bacteria. In Endophthalmitis; Springer Singapore: Singapore, 2018; pp. 185–198. [Google Scholar] [CrossRef]
- Paladine, H.L.; Desai, U.A. Vaginitis: Diagnosis and Treatment. Am. Fam. Physician 2018, 97, 321–329. Available online: www.aafp.org/afphttp://www.aafp.org/afp/2018/0301/p321-s1.html (accessed on 23 April 2023).
- Palmeira-de-Oliveira, R.; Palmeira-de-Oliveira, A.; Martinez-de-Oliveira, J. New strategies for local treatment of vaginal infections. Adv. Drug Deliv. Rev. 2015, 92, 105–122. [Google Scholar] [CrossRef]
- Ding, C.; Yu, Y.; Zhou, Q. Bacterial Vaginosis: Effects on reproduction and its therapeutics. J. Gynecol. Obstet. Hum. Reprod. 2021, 50, 102174. [Google Scholar] [CrossRef]
- Rodríguez-Cerdeira, C.; Gregorio, M.C.; Molares-Vila, A.; López-Barcenas, A.; Fabbrocini, G.; Bardhi, B.; Sinani, A.; Sánchez-Blanco, E.; Arenas-Guzmán, R.; Hernandez-Castro, R. Biofilms and vulvovaginal candidiasis. Colloids Surf. B Biointerfaces 2019, 174, 110–125. [Google Scholar] [CrossRef]
- Denning, D.W.; Kneale, M.; Sobel, J.D.; Rautemaa-Richardson, R. Global burden of recurrent vulvovaginal candidiasis: A systematic review. Lancet Infect. Dis. 2018, 18, e339–e347. [Google Scholar] [CrossRef] [PubMed]
- Nice. Respiratory Tract Infections-Antibiotic Prescribing Prescribing of Antibiotics for Self-Limiting Respiratory Tract Infections in Adults and Children in Primary Care. 2008. Available online: www.nic.org.uk (accessed on 28 March 2023).
- Thomas, M.; Bomar, P.A. Upper Respiratory Tract Infection. Indian J. Pediatr. 2001, 68, 1135–1138. [Google Scholar]
- Barrett, B. Viral Upper Respiratory Infection. In Integrative Medicine, 4th ed.; Elsevier: Amsterdam, The Netherlands, 2018; pp. 170–179.e7. [Google Scholar] [CrossRef]
- MacIntyre, C.R.; Chughtai, A.A.; Zhang, Y.; Seale, H.; Yang, P.; Chen, J.; Pan, Y.; Zhang, D.; Wang, Q. Viral and bacterial upper respiratory tract infection in hospital health care workers over time and association with symptoms. BMC Infect. Dis. 2017, 17, 553. [Google Scholar] [CrossRef]
- Noviello, S.; Huang, D.B. The basics and the advancements in diagnosis of bacterial lower respiratory tract infections. Diagnostics 2019, 9, 37. [Google Scholar] [CrossRef] [PubMed]
- Musher, D.M.; Abers, M.S.; Bartlett, J.G. Evolving Understanding of the Causes of Pneumonia in Adults, with Special Attention to the Role of Pneumococcus. Clin. Infect. Dis. 2017, 65, 1736–1744. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.; Self, W.H.; Wunderink, R.G.; Fakhran, S.; Balk, R.; Bramley, A.M.; Chappell, J.D. Community-Acquired Pneumonia Requiring Hospitalization among U.S. Adults. N. Engl. J. Med. 2015, 373, 415–427. [Google Scholar] [CrossRef] [PubMed]
- Burk, M.; El-Kersh, K.; Saad, M.; Wiemken, T.; Ramirez, J.; Cavallazzi, R. Viral infection in community-acquired pneumonia: A systematic review and meta-analysis. Eur. Respir. Rev. 2016, 25, 178–188. [Google Scholar] [CrossRef]
- Kalil, A.C.; Metersky, M.L.; Klompas, M.; Muscedere, J.; Sweeney, D.A.; Palmer, L.B.; Napolitano, L.M.; O’Grady, N.P.; Bartlett, J.G.; Carratala, J.; et al. Management of Adults with Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin. Infect. Dis. 2016, 63, e61–e111. [Google Scholar] [CrossRef]
- Furin, J.; Cox, H.; Pai, M. Tuberculosis. Lancet 2019, 393, 1642–1656. [Google Scholar] [CrossRef]
- Esmail, H.; Barry, C.E.; Young, D.B.; Wilkinson, R.J. The ongoing challenge of latent tuberculosis. Philos. Trans. R. Soc. B Biol. Sci. 2014, 369, 20130437. [Google Scholar] [CrossRef]
- Pai, M.; Behr, M.A.; Dowdy, D.; Dheda, K.; Divangahi, M.; Boehme, C.C.; Ginsberg, A.; Swaminathan, S.; Spigelman, M.; Getahun, H.; et al. Tuberculosis. Nat. Rev. Dis. Prim. 2016, 2, 16076. [Google Scholar] [CrossRef] [PubMed]
- Sinha, R.; Rajesh, A.; Rawat, S.; Rajiah, P.; Ramachandran, I. Infections and infestations of the gastrointestinal tract. Part 1: Bacterial, viral and fungal infections. Clin. Radiol. 2012, 67, 484–494. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Sell, J.; Dolan, B. Common Gastrointestinal Infections. Prim Care 2018, 45, 519–532. [Google Scholar] [CrossRef] [PubMed]
- Malik, T.F.; Gnanapandithan, K.; Singh, K. Peptic Ulcer Disease. Lancet 2009, 374, 1449–1461. [Google Scholar]
- Majumdar, D.; Bebb, J. Helicobacter pylori infection and peptic ulcers. Medicine 2019, 47, 292–300. [Google Scholar] [CrossRef]
- Lamps, L.W. Infectious Disorders of the GI Tract. In Surgical Pathology of the GI Tract, Liver, Biliary Tract, and Pancreas; Elsevier: Amsterdam, The Netherlands, 2009; pp. 51–79. [Google Scholar] [CrossRef]
- Ferrah, N.; Leder, K.; Gibney, K. Review of the causes and management of chronic gastrointestinal symptoms in returned travellers referred to an Australian infectious diseases service. Aust. Fam. Physician 2016, 45, 333–339. [Google Scholar]
- Stamm, W.E.; Norrby, S.R. Urinary Tract Infections: Disease Panorama and Challenges. J. Infect. Dis. 2001, 183, S1–S4. [Google Scholar] [CrossRef]
- Murray, B.O.; Flores, C.; Williams, C.; Flusberg, D.A.; Marr, E.E.; Kwiatkowska, K.M.; Charest, J.L.; Isenberg, B.C.; Rohn, J.L. Recurrent Urinary Tract Infection: A Mystery in Search of Better Model Systems. Front. Cell. Infect. Microbiol. 2021, 11, 691210. [Google Scholar] [CrossRef]
- Flores-Mireles, A.L.; Walker, J.N.; Caparon, M.; Hultgren, S.J. Urinary tract infections: Epidemiology, mechanisms of infection and treatment options. Nat. Rev. Microbiol. 2015, 13, 269–284. [Google Scholar] [CrossRef]
- Sabih, A.; Leslie, S.W. Complicated Urinary Tract Infections. In StatPearls; StatPearls Publishing: Tampa, FL, USA, 2022. [Google Scholar]
- Cueni, L.N.; Detmar, M. The lymphatic system in health and disease. Lymphat. Res. Biol. 2008, 6, 109–122. [Google Scholar] [CrossRef]
- Maini, R.; Nagalli, S. Lymphadenopathy. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar] [PubMed]
- Myers, A.L. Localized Lymphadenitis, Lymphadenopathy, and Lymphangitis. In Principles and Practice of Pediatric Infectious Diseases; Elsevier Inc.: Amsterdam, The Netherlands, 2018; pp. 158–163.e1. [Google Scholar] [CrossRef]
- Swartz, M.A. The physiology of the lymphatic system. Adv. Drug Deliv. Rev. 2001, 50, 3–20. [Google Scholar] [CrossRef] [PubMed]
- Chandy, A.; Thakur, A.S.; Singh, M.P.; Manigauha, A. A review of neglected tropical diseases: Filariasis. Asian Pac. J. Trop. Med. 2011, 4, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Permana, A.D.; Tekko, I.A.; McCrudden, M.T.C.; Anjani, Q.K.; Ramadon, D.; McCarthy, H.O.; Donnelly, R.F. Solid lipid nanoparticle-based dissolving microneedles: A promising intradermal lymph targeting drug delivery system with potential for enhanced treatment of lymphatic filariasis. J. Control. Release 2019, 316, 34–52. [Google Scholar] [CrossRef] [PubMed]
- Nathan, C.L.; Emmert, B.E.; Nelson, E.; Berger, J.R. CNS fungal infections: A review. J. Neurol. Sci. 2021, 422, 117325. [Google Scholar] [CrossRef]
- Robertson, F.C.; Lepard, J.R.; Mekary, R.A.; Davis, M.C.; Yunusa, I.; Gormley, W.B.; Baticulon, R.E.; Mahmud, M.R.; Misra, B.K.; Rattani, A.; et al. Epidemiology of central nervous system infectious diseases: A meta-analysis and systematic review with implications for neurosurgeons worldwide. J. Neurosurg. 2019, 130, 1107–1126. [Google Scholar] [CrossRef]
- van de Beek, D.; Brouwer, M.; Hasbun, R.; Koedel, U.; Whitney, C.G.; Wijdicks, E. Community-acquired bacterial meningitis. Nat. Rev. Dis. Prim. 2016, 2, 809–820. [Google Scholar] [CrossRef]
- Griffiths, M.J.; McGill, F.; Solomon, T. Management of acute meningitis. Clin. Med. 2018, 18, 164–169. [Google Scholar] [CrossRef]
- Archibald, L.K.; Quisling, R.G. Central Nervous System Infections. In Textbook of Neurointensive Care; Springer London: London, UK, 2013; pp. 427–517. [Google Scholar] [CrossRef]
- Parikh, V.; Tucci, V.; Galwankar, S. Infections of the nervous system. Int. J. Crit. Illn. Inj. Sci. 2012, 2, 82. [Google Scholar] [CrossRef]
- Nguyen, I.; Urbanczyk, K.; Mtui, E.; Li, S. Intracranial CNS Infections: A Literature Review and Radiology Case Studies. Semin. Ultrasound CT MRI 2020, 41, 106–120. [Google Scholar] [CrossRef]
- Gabillot-Carré, M.; Roujeau, J.C. Acute bacterial skin infections and cellulitis. Curr. Opin. Infect. Dis. 2007, 20, 118–123. [Google Scholar] [CrossRef]
- Gibbons, J.A.; Smith, H.L.; Kumar, S.C.; Duggins, K.J.; Bushman, A.M.; Danielson, J.M.; Yost, W.J.; Wadle, J.J. Antimicrobial stewardship in the treatment of skin and soft tissue infections. Am. J. Infect. Control 2017, 45, 1203–1207. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Peghin, M.; Castaldo, N.; Giacobbe, D.R. The safety of treatment options for acute bacterial skin and skin structure infections. Expert Opin. Drug Saf. 2019, 18, 635–650. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.C.; Chan, W.W.; Metelitsa, A.I.; Fiorillo, L.; Lin, A.N. Pseudomonas skin infection: Clinical features, epidemiology, and management. Am. J. Clin. Dermatol. 2011, 12, 157–169. [Google Scholar] [CrossRef] [PubMed]
- Hodille, E.; Rose, W.; Diep, B.A.; Goutelle, S.; Lina, G.; Dumitrescu, O. The Role of Antibiotics in Modulating Virulence in Staphylococcus aureus. Clin. Microbiol. Rev. 2017, 30, 887–917. [Google Scholar] [CrossRef]
- Luther, M.K.; Timbrook, T.T.; Caffrey, A.R.; Dosa, D.; Lodise, T.P.; LaPlante, K.L. Vancomycin plus piperacillin-tazobactam and acute kidney injury in adults: A systematic review and meta-analysis. Crit. Care Med. 2018, 46, 12–20. [Google Scholar] [CrossRef]
- Pulido-Cejudo, A.; Guzmán-Gutierrez, M.; Jalife-Montaño, A.; Ortiz-Covarrubias, A.; Martínez-Ordaz, J.L.; Noyola-Villalobos, H.F.; Hurtado-Lopez, L.-M. Management of acute bacterial skin and skin structure infections with a focus on patients at high risk of treatment failure. Ther. Adv. Infect. Dis. 2017, 4, 143–161. [Google Scholar] [CrossRef]
- Golan, Y. Current treatment options for acute skin and skin-structure infections. Clin. Infect. Dis. 2019, 68, S206–S212. [Google Scholar] [CrossRef]
- Stevens, D.L.; Bisno, A.L.; Chambers, H.F.; Everett, E.D.; Dellinger, P.; Goldstein, E.J.C.; Gorbach, S.L.; Hirschmann, J.V.; Kaplan, E.L.; Montoya, J.G.; et al. Practice guidelines for the diagnosis and management of skin and soft-tissue infections. Clin. Infect. Dis. 2005, 41, 1373–1406. [Google Scholar] [CrossRef]
- Eckmann, C.; Dryden, M. Treatment of complicated skin and soft-tissue infections caused by resistant bacteria: Value of linezolid, tigecycline, daptomycin and vancomycin. Eur. J. Med. Res. 2010, 15, 554–563. [Google Scholar] [CrossRef]
- Bernard, P. Management of common bacterial infections of the skin. Curr. Opin. Infect. Dis. 2008, 21, 122–128. [Google Scholar] [CrossRef]
- Yun, H.-J.; Lee, S.W.; Yoon, G.M.; Kim, S.Y.; Choi, S.; Lee, Y.S.; Choi, E.-C.; Kim, S. Prevalence and mechanisms of low- and high-level mupirocin resistance in staphylococci isolated from a Korean hospital. J. Antimicrob. Chemother. 2003, 51, 619–623. [Google Scholar] [CrossRef] [PubMed]
- McCurdy, S.; Lawrence, L.; Quintas, M.; Woosley, L.; Flamm, R.; Tseng, C.; Cammarata, S. In vitro activity of delafloxacin and microbiological response against fluoroquinolone-susceptible and nonsusceptible Staphylococcus aureus isolates from two phase 3 studies of acute bacterial skin and skin structure infections. Antimicrob. Agents Chemother. 2017, 61, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Borgers, M.; Degreef, H.; Cauwenbergh, G. Fungal Infections of the Skin: Infection Process and Antimycotic Therapy. Curr. Drug Targets 2005, 6, 849–862. [Google Scholar] [CrossRef] [PubMed]
- Kyle, A.A.; Dahl, M.V. Topical therapy for fungal infections. Am. J. Clin. Dermatol. 2004, 5, 443–451. [Google Scholar] [CrossRef]
- Rotta, I.; Sanchez, A.; Gonçalves, P.R.; Otuki, M.F.; Correr, C.J. Efficacy and safety of topical antifungals in the treatment of dermatomycosis: A systematic review. Br. J. Dermatol. 2012, 166, 927–933. [Google Scholar] [CrossRef]
- Hay, R. Therapy of skin, hair and nail fungal infections. J. Fungi 2018, 4, 99. [Google Scholar] [CrossRef]
- Crawford, F.; Hollis, S. Topical treatments for fungal infections of the skin and nails of the foot. Cochrane Database Syst. Rev. 2007, 2007, CD001434. [Google Scholar] [CrossRef]
- Budimulja, U.; Bramono, K.; Urip, K.S.; Basuki, S.; Widodo, G.; Rapatz, G.; Paul, C. Once daily treatment with terbinafine 1% cream (Lamisil®) for one week is effective in the treatment of tinea corporis and cruris. A placebo-controlled study. Mycoses 2001, 44, 300–306. [Google Scholar] [CrossRef]
- Auvinen, T.; Tiihonen, R.; Soini, M.; Wangel, M.; Sipponen, A.; Jokinen, J. Efficacy of topical resin lacquer, amorolfine and oral terbinafine for treating toenail onychomycosis: A prospective, randomized, controlled, investigator-blinded, parallel-group clinical trial. Br. J. Dermatol. 2015, 173, 940–948. [Google Scholar] [CrossRef]
- Keyser, P.D.; Backer, M.D.; Massart, D.L.; Westelinck, K.J. Two-week oral treatment of tinea pedis, comparing terbinafine (250 mg/day) with itraconazole (100 mg/day): A double-blind, multicentre study. Br. J. Dermatol. 1994, 130, 22–25. [Google Scholar] [CrossRef]
- Frieden, I.J. Diagnosis and management of tinea capitis. Pediatr. Ann. 1987, 16, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Moriarty, B.; Hay, R.; Morris-Jones, R. The diagnosis and management of tinea. BMJ 2012, 345, E4380. [Google Scholar] [CrossRef] [PubMed]
- Sahoo, A.; Mahajan, R. Management of tinea corporis, tinea cruris, and tinea pedis: A comprehensive review. Indian Derm. Online J. 2018, 7, 77. [Google Scholar]
- Handa, S.; Villasis-Keever, A.; Shenoy, M.; Anandan, S.; Bhrushundi, M.; Garodia, N.; Fife, D.; De Doncker, P.; Shalayda, K.; Hu, P.; et al. No evidence of resistance to itraconazole in a prospective real-world trial of dermatomycosis in India. PLoS ONE 2023, 18, e0281514. [Google Scholar] [CrossRef]
- Wingfield, A.B.; Fernandez-Obregon, A.C.; Wignall, F.S.; Greer, D.L. Treatment of tinea imbricata: A randomized clinical trial using griseofulvin, terbinafine, itraconazole and fluconazole. Br. J. Dermatol. 2004, 150, 119–126. [Google Scholar] [CrossRef]
- Gupta, A.K.; Sauder, D.N.; Shear, N.H. Antifungal agents: An overview. Part I. J. Am. Acad. Dermatol. 1994, 30, 677–698. [Google Scholar] [CrossRef]
- De Clercq, E. Antiviral drugs: Current state of the art. J. Clin. Virol. 2001, 22, 73–89. [Google Scholar] [CrossRef]
- Park, K.C.; Han, W.S. Diagnosis and Treatment Considerations. Drugs 2002, 62, 479–490. [Google Scholar] [CrossRef]
- Newton, H. Viral infections of the skin: Clinical features and treatment options. Nurs. Stand. 2013, 27, 43–47. [Google Scholar] [CrossRef]
- Donders, G. Diagnosis and management of bacterial vaginosis and other types of abnormal vaginal bacterial flora: A review. Obstet. Gynecol. Surv. 2010, 65, 462–473. [Google Scholar] [CrossRef]
- De Backer, E.; Verhelst, R.; Verstraelen, H.; Claeys, G.; Verschraegen, G.; Temmerman, M.; Vaneechoutte, M. Antibiotic susceptibility of Atopobium vaginae. BMC Infect. Dis. 2006, 6, 51. [Google Scholar] [CrossRef] [PubMed]
- Sheikh, A.; Hurwitz, B. Antibiotics versus placebo for acute bacterial conjunctivitis. Cochrane Database Syst. Rev. 2006, 2, CD001211. [Google Scholar] [CrossRef]
- Care, S. Antibiotic Guidelines for Ophthalmological Indications in Adults in Secondary Care; NHS: Barnstaple, UK, 2019. [Google Scholar]
- Katusic, D.; Petricek, I.; Mandic, Z.; Petric, I.; Salopek-Rabatic, J.; Kruzic, V.; Oreskovic, K.; Sikic, J.; Petricek, G. Azithromycin vs doxycycline in the treatment of inclusion conjunctivitis. Am. J. Ophthalmol. 2003, 135, 447–451. [Google Scholar] [CrossRef] [PubMed]
- Spinillo, A.; Capuzzo, E.; Acciano, S.; De Santolo, A.; Zara, F. Effect of antibiotic use on the prevalence of symptomatic vulvovaginal candidiasis. Am. J. Obstet. Gynecol. 1999, 180, 14–17. [Google Scholar] [CrossRef] [PubMed]
- Thompson, G.R., III; Patel, P.K.; Kirkpatrick, W.R.; Westbrook, S.D.; Berg, D.; Erlandsen, J.; Redding, S.W.; Patterson, T.F. Oropharyngeal candidiasis in the era of antiretroviral therapy. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2010, 109, 488–495. [Google Scholar] [CrossRef]
- Williams, D.; Lewis, M. Pathogenesis and treatment of oral candidosis. J. Oral Microbiol. 2011, 3, 5771. [Google Scholar] [CrossRef]
- Laílla Vicens, J.M. Candidiasis vulvovaginal. Med. Clin. 1990, 94, 337–338. [Google Scholar]
- Dovnik, A.; Golle, A.; Novak, D.; Arko, D.; Takač, I. Treatment of vulvovaginal candidiasis: A review of the literature. Acta Dermatovenerol. Alp. Pannonica Et Adriat. 2015, 24, 5–7. [Google Scholar] [CrossRef]
- Zhou, X.; Li, T.; Fan, S.; Zhu, Y.; Liu, X.; Guo, X.; Liang, Y. The efficacy and safety of clotrimazole vaginal tablet vs. oral fluconazole in treating severe vulvovaginal candidiasis. Mycoses 2016, 59, 419–428. [Google Scholar] [CrossRef]
- Metlay, J.P.; Waterer, G.W.; Long, A.C.; Anzueto, A.; Brozek, J.; Crothers, K.; Cooley, L.A.; Dean, N.C.; Fine, M.J.; Flanders, S.A.; et al. Diagnosis and treatment of adults with community-acquired pneumonia. Am. J. Respir. Crit. Care Med. 2019, 200, E45–E67. [Google Scholar] [CrossRef]
- Mandell, L.A.; Wunderink, R.G.; Anzueto, A. Infectious Diseases Society of America. American Thoracic Society et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin. Infect. Dis. 2007, 44 (Suppl. 2), S27–S72. [Google Scholar] [CrossRef] [PubMed]
- Hammerschlag, M.R. Mycoplasma pneumoniae infections. Curr. Opin. Infect. Dis. 2001, 14, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Paulman, P.M.; Taylor, R.B.; Paulman, A.A.; Nasir, L.S. Family Medicine: Principles and Practice; Springer International Publishing: Berlin/Heidelberg, Germany, 2016; pp. 1–1863. [Google Scholar] [CrossRef]
- Sethi, S.; Murphy, T.F. Bacterial infection in chronic obstructive pulmonary disease in 2000: A state-of-the-art review. Clin. Microbiol. Rev. 2001, 14, 336–363. [Google Scholar] [CrossRef] [PubMed]
- Woodhead, M.; Blasi, F.; Ewig, S.; Garau, J.; Huchon, G.; Ieven, M.; Ortqvist, A.; Schaberg, T.; Torres, A.; van der Heijden, G.; et al. Guidelines for the management of adult lower respiratory tract infections. Eur. Respir. J. 2005, 26, 1138–1180. [Google Scholar] [CrossRef]
- Brailsford, J.F.; Crawford, J.H. Treatment of Tuberculosis. Lancet 1947, 249, 232. [Google Scholar] [CrossRef]
- Nahid, P.; Dorman, S.E.; Alipanah, N.; Barry, P.M.; Brozek, J.L.; Cattamanchi, A.; Chaisson, L.H.; Chaisson, R.E.; Daley, C.L.; Grzemska, M.; et al. Official American Thoracic Society/Centers for Disease Control and Prevention/Infectious Diseases Society of America Clinical Practice Guidelines: Treatment of Drug-Susceptible Tuberculosis. Clin. Infect. Dis. 2016, 63, e147–e195. [Google Scholar] [CrossRef]
- Foweraker, J. Recent advances in the microbiology of respiratory tract infection in cystic fibrosis. Br. Med. Bull. 2009, 89, 93–110. [Google Scholar] [CrossRef]
- Alipour, M.; Suntres, Z.E. Liposomal antibiotic formulations for targeting the lungs in the treatment of Pseudomonas aeruginosa. Ther. Deliv. 2014, 5, 409–427. [Google Scholar] [CrossRef]
- Hamed, K.; Debonnett, L. Tobramycin inhalation powder for the treatment of pulmonary Pseudomonas aeruginosa infection in patients with cystic fibrosis: A review based on clinical evidence. Ther. Advanve Respir. Dis. 2017, 11, 193–209. [Google Scholar] [CrossRef]
- Cipolla, D.; Chan, H.K. Inhaled antibiotics to treat lung infection. Pharm. Pat. Anal. 2013, 2, 647–663. [Google Scholar] [CrossRef]
- Hoppentocht, M.; Hagedoorn, P.; Frijlink, H.W.; de Boer, A.H. Developments and strategies for inhaled antibiotic drugs in tuberculosis therapy: A critical evaluation. Eur. J. Pharm. Biopharm. 2014, 86, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Alastruey-Izquierdo, A.; Cadranel, J.; Flick, H.; Godet, C.; Hennequin, C.; Hoenigl, M.; Kosmidis, C.; Lange, C.; Munteanu, O.; Page, I.; et al. Treatment of Chronic Pulmonary Aspergillosis: Current Standards and Future Perspectives. Respiration 2018, 96, 159–170. [Google Scholar] [CrossRef] [PubMed]
- Patterson, T.F.; Thompson, G.R., III; Denning, D.W.; Fishman, J.A.; Hadley, S.; Herbrecht, R.; Kontoyiannis, D.P.; Marr, K.A.; Morrison, V.A.; Nguyen, M.H.; et al. Practice guidelines for the diagnosis and management of aspergillosis: 2016 update by the infectious diseases society of America. Clin. Infect. Dis. 2016, 63, e1–e60. [Google Scholar] [CrossRef] [PubMed]
- Denning, D.W.; Cadranel, J.; Beigelman-Aubry, C.; Ader, F.; Chakrabarti, A.; Blot, S.; Ullmann, A.J.; Dimopoulos, G.; Lange, C.; Lange, D.C. on behalf of the European Society for Clinical Microbiology and Infectious Diseases and European Respiratory Society. Chronic pulmonary aspergillosis: Rationale and clinical guidelines for diagnosis and management. Eur. Respir. J. 2016, 47, 45–68. [Google Scholar] [CrossRef] [PubMed]
- Abed, Y.; Boivin, G. Treatment of respiratory virus infections. Antivir. Res. 2006, 70, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Howard, D.S.; Phillips, I.G.L.; Reece, D.E.; Munn, R.K.; Henslee-Downey, J.; Pittard, M.; Barker, M.; Pomeroy, C. Adenovirus Infections in Hematopoietic Stem Cell Transplant Recipients. Clin. Infect. Dis. 1999, 29, 1494–1501. [Google Scholar] [CrossRef] [PubMed]
- Kapelushnik, J.; Or, R.; Delukina, M.; Nagler, A.; Livni, N.; Engelhard, D. Intravenous Ribavirin Therapy for Adenovirus Gastroenteritis After Bone Marrow Transplantation. J. Craniofacial Surg. 1995, 21, 110–112. [Google Scholar] [CrossRef]
- Me Carthy, A.J.; Bergin, M.; De Silva, L.M.; Stevens, M. Intravenous ribavirin therapy for disseminated adenovirus infection. Pediatr. Infect. Dis. J. 1995, 14, 1003. [Google Scholar] [CrossRef]
- Ribaud, P.; Scieux, C.; Freymuth, F.; Morinet, F.; Gluckman, E. Successful Treatment of Adenovirus Disease with Intravenous Cidofovir in an Unrelated Stem-Cell Transplant Recipient. Clin. Infect. Dis. 1999, 28, 690–691. [Google Scholar] [CrossRef]
- Bordigoni, P.; Carret, A.-S.; Venard, V.; Witz, F.; Le Faou, A. Treatment of Adenovirus Infections in Patients Undergoing Allogeneic Hematopoietic Stem Cell Transplantation. Clin. Infect. Dis. 2001, 32, 1290–1297. [Google Scholar] [CrossRef]
- Brooks, M.J.; Sasadeusz, J.J.; Tannock, G.A. Antiviral chemotherapeutic agents against respiratory viruses. Curr. Opin. Pulm. Med. 2004, 10, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Balfour, H.H. Antiviral Drugs. N. Engl. J. Med. 1999, 340, 1255–1268. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Singh, M.; Malashkevich, V.N.; Kim, P.S. Structural characterization of the human respiratory syncytial virus fusion protein core. Proc. Natl. Acad. Sci. USA 2000, 97, 14172–14177. [Google Scholar] [CrossRef] [PubMed]
- Crooke, S.T. Therapeutic applications of oligonucleotides. Annu. Rev. Pharmacol. Toxicol. 1992, 32, 329–376. [Google Scholar] [CrossRef]
- Maggon, K.; Barik, S. New drugs and treatment for respiratory syncytial virus. Rev. Med. Virol. 2004, 14, 149–168. [Google Scholar] [CrossRef] [PubMed]
- Vujovic, O. Preventive and therapeutic strategies for respiratory syncytial virus infection. Curr. Opin. Pharmacol. 2001, 1, 497–503. [Google Scholar] [CrossRef]
- Tyrrell, D.A.J.; Bynoe, M.L. Cultivation of a Novel Type of Common-cold Virus in Organ Cultures. BMJ 1965, 1, 1467–1470. [Google Scholar] [CrossRef]
- Thiel, V.; Herold, J.; Schelle, B.; Siddell, S.G. Infectious RNA transcribed in vitro from a cDNA copy of the human coronavirus genome cloned in vaccinia virus. J. Gen. Virol. 2001, 82, 1273–1281. [Google Scholar] [CrossRef]
- Peiris, J.S.; Yuen, K.Y.; Osterhaus, A.D.; Stöhr, K. The Severe Acute Respiratory Syndrome. N. Engl. J. Med. 2003, 349, 2431–2441. [Google Scholar] [CrossRef]
- Ksiazek, T.G.; Erdman, D.; Goldsmith, C.S.; Zaki, S.R.; Peret, T.; Emery, S.; Tong, S.; Urbani, C.; Comer, J.A.; Lim, W.; et al. A Novel Coronavirus Associated with Severe Acute Respiratory Syndrome. N. Engl. J. Med. 2003, 348, 1953–1966. [Google Scholar] [CrossRef]
- Chan, J.F.W.; Yao, Y.; Yeung, M.L.; Deng, W.; Bao, L.; Jia, L.; Li, F.; Xiao, C.; Gao, H.; Yu, P.; et al. Treatment with Lopinavir/Ritonavir or Interferon-beta1b Improves Outcome of MERS-CoV Infection in a Nonhuman Primate Model of Common Marmoset. J. Infect. Dis. 2015, 212, 1904–1913. [Google Scholar] [CrossRef] [PubMed]
- Chu, C.M.; Cheng, V.C.C.; Hung, I.F.N.; Wong, M.M.L.; Chan, K.H.; Chan, K.S.; Kao, R.Y.T.; Poon, L.L.M.; Wong, C.L.P.; Guan, Y.; et al. Role of lopinavir/ritonavir in the treatment of SARS: Initial virological and clinical findings. Thorax 2004, 59, 252–256. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, N.; Yang, R.; Yoshinaka, Y.; Amari, S.; Nakano, T.; Cinatl, J.; Rabenau, H.; Doerr, H.W.; Hunsmann, G.; Otaka, A.; et al. HIV protease inhibitor nelfinavir inhibits replication of SARS-associated coronavirus. Biochem. Biophys. Res. Commun. 2004, 318, 719–725. [Google Scholar] [CrossRef] [PubMed]
- He, M.; Zheng, B.; Peng, Y.; Peiris, J.S.M.; Poon, L.; Yuen, K.-Y.; Lin, M.C.M.; Kung, H.-F.; Guan, Y. Inhibition of SARS-Associated Coronavirus Infection and Replication by RNA Interference. JAMA 2003, 290, 2665–2666. [Google Scholar] [CrossRef] [PubMed]
- Ziai, W.C.; Iii, J.J.L. Update in the Diagnosis and Management of Central Nervous System Infections. Neurol. Clin. 2008, 22, 427–468. [Google Scholar] [CrossRef]
- Tan, Y.C.; Gill, A.K.; Kim, K.S.; Gill, A.K.; Kim, K.S. Treatment strategies for central nervous system infections: An update. Expert Opin. Pharmacother. 2015, 16, 187–203. [Google Scholar] [CrossRef]
- Nau, R.; So, F. Penetration of Drugs through the Blood-Cerebrospinal Fluid/Blood-Brain Barrier for Treatment of Central Nervous System Infections † physiology of the exchange of drugs between blood and the different. Clin. Microbiol. Rev. 2010, 23, 858–883. [Google Scholar] [CrossRef]
- Tunkel, A.R.; Hasbun, R.; Bhimraj, A.; Byers, K.; Kaplan, S.L.; Scheld, W.M.; van de Beek, D.; Bleck, T.P.; Garton, H.J.; Zunt, J.R. 2017 Infectious Diseases Society of America’s Clinical Practice Guidelines for Healthcare-Associated Ventriculitis and Meningitis. Clin. Infect. Diseases 2017, 64, e34–e65. [Google Scholar] [CrossRef]
- Archibald, L.K.; Quisling, R.G. Textbook of Neurointensive Care. Textbook of Neurointensive Care; Saunders: Philadelphi, PA, USA, 2013. [Google Scholar] [CrossRef]
- Sarrazin, J.; Bonneville, F.; Martin-blondel, G. Brain infections Neural way. Diagn. Interv. Imaging 2012, 93, 473–490. [Google Scholar] [CrossRef]
- Silvestro, E.M.; Nakano, V.; Arana-Chavez, V.E.; Marques, M.V.; Avila-Campos, M.J. Effects of subinhibitory concentrations of clindamycin on the morphological, biochemical and genetic characteristics of Bacteroides fragilis. FEMS Microbiol. Lett. 2006, 257, 189–194. [Google Scholar] [CrossRef][Green Version]
- Brook, I. Microbiology and treatment of brain abscess. J. Clin. Neurosci. 2017, 371, 6–10. [Google Scholar] [CrossRef] [PubMed]
- Brouwer, M.C.; Tunkel, A.R. Brain Abscess. N. Engl. J. Med. 2014, 371, 447–456. [Google Scholar] [CrossRef] [PubMed]
- Grandgirard, D.; Oberson, K.; Buhlmann, A.; Gaumann, R.; Leib, S.L. Attenuation of cerebrospinal fluid inflammation by the nonbacteriolytic antibiotic daptomycin versus that by ceftriaxone in experimental pneumococcal meningitis. Antimicrob. Agents Chemother. 2010, 54, 1323–1326. [Google Scholar] [CrossRef] [PubMed]
- Black, K.E.; Baden, L.R. Fungal Infections of the CNS. CNS Drugs 2007, 21, 293–318. [Google Scholar] [CrossRef] [PubMed]
- Martino, R.; Cortès, M.; Subirá, M.; Parody, R.; Moreno, E.; Sierra, J. Efficacy and toxicity of intermediate-dose amphotericin B lipid complex as a primary or salvage treatment of fungal infections in patients with hematological malignancies. Leuk. Lymphoma 2005, 46, 1429–1435. [Google Scholar] [CrossRef] [PubMed]
- Saag, M.S.; Graybill, R.J.; Larsen, R.A.; Pappas, P.G.; Perfect, J.R.; Powderly, W.G.; Sobel, J.D.; Dismukes, W.E. Mycoses Study Group Cryptococcal Subproject Practice Guidelines for the Management of Cryptococcal Disease. Clin. Infect. Dis. 2000, 30, 710–718. [Google Scholar] [CrossRef] [PubMed]
- Kontoyiannis, D.P.; Boktour, M.; Hanna, H.; Torres, H.A.; Hachem, R.; Raad, I.I. Itraconazole added to a lipid formulation of amphotericin B does not improve outcome of primary treatment of invasive aspergillosis. Cancer 2005, 103, 2334–2337. [Google Scholar] [CrossRef]
- Denning, D.W.; Stevens, D.A. Antifungal and surgical treatment of invasive aspergillosis: Review of 2121 published cases. Rev. Infect. Dis. 1990, 12, 1147–1201. [Google Scholar] [CrossRef]
- Mukherjee, P.K.; Sheehan, D.J.; Hitchcock, C.A.; Ghannoum, M.A. Combination treatment of invasive fungal infections. Clin. Microbiol. Rev. 2005, 18, 163–194. [Google Scholar] [CrossRef]
- Vertzoni, M.; Augustijns, P.; Grimm, M.; Koziolek, M.; Lemmens, G.; Parrott, N.; Pentafragka, C.; Reppas, C.; Rubbens, J.; Van Den Abeele, J.; et al. Impact of regional differences along the gastrointestinal tract of healthy adults on oral drug absorption: An UNGAP review. Eur. J. Pharm. Sci. 2019, 134, 153–175. [Google Scholar] [CrossRef]
- Hodges, K.; Gill, R. Infectious diarrhea Cellular and molecular mechanisms. Gut Microbes 2010, 1, 4–21. [Google Scholar] [CrossRef] [PubMed]
- Britton, R.A.; Versalovic, J. Probiotics and Gastrointestinal Infections. Interdiscip. Perspect. Infect. Dis. 2008, 2008, 290769. [Google Scholar] [CrossRef] [PubMed]
- Graves, N.S. Acute Gastroenteritis. Prim. Care Clin. Off. Pract. 2013, 40, 727–741. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M.; D’Anci, K.E.; Rosenberg, I.H. Water, hydration, and health. Nutr. Rev. 2010, 68, 439–458. [Google Scholar] [CrossRef]
- Gopalakrishnakone, P.; Balali-Mood, M.; Llewellyn, L.; Ram Singh, B. Biological Toxins and Bioterrorism; Springer Netherlands: Berlin/Heidelberg, Germany, 2015. [Google Scholar]
- Parker, N.; Schneegurt, M.; Tu, A.-H.T.; Lister, P.; Forster, B.M. Microbiology; OpenStax: Houston, TX, USA, 2016. [Google Scholar]
- Julio-Pieper, M.; Alejandra, L.; Eyzaguirre-vel, J.; Olavarr, L. Gut Susceptibility to Viral Invasion: Contributing Roles of Diet, Microbiota and Enteric Nervous System to Mucosal Barrier Preservation. Int. J. Mol. Sci. 2021, 22, 4734. [Google Scholar] [CrossRef] [PubMed]
- Berhe, B.; Bugssa, G.; Bayisa, S.; Alemu, M. Foodborne intestinal protozoan infection and associated factors among patients with watery diarrhea in Northern Ethiopia; A cross-sectional study. J. Health Popul. Nutr. 2018, 37, 5. [Google Scholar] [CrossRef]
- Abdullah, I.; Tak, H.; Ahmad, F.; Gul, N.; Nabi, S.; Sofi, A.T. Predominance of Gastrointestinal Protozoan Parasites in Children: A Brief Review. J. Health Educ. Res. Dev. 2016, 4, 1000194. [Google Scholar] [CrossRef]
- Born, B.A. The Essential Massage Companion; Concepts Born, LLC: Sioux Falls, SD, USA, 2005. [Google Scholar]
- McCue, J.D.; Kahan, S. Infectious Disease; Lippincott Williams & Wilkins: Philadelphi, PA, USA, 2007. [Google Scholar]
- Moini, J. Introduction to Pathology for the Physical Therapist Assistant; Jones & Bartlett Learning: Burlington, MA, USA, 2013. [Google Scholar]
- Leung AK, C. Childhood Cervical Lymphadenopathy. J. Pediatr. Health Care 2004, 18, 3–7. [Google Scholar] [CrossRef]
- Pecora, F.; Abate, L.; Scavone, S.; Petrucci, I.; Costa, F.; Caminiti, C.; Argentiero, A.; Esposito, S. Management of Infectious Lymphadenitis in Children. Children 2021, 8, 860. [Google Scholar] [CrossRef]
- Borton, D.; Brinsko, V.; Gilmor, G.K.; Hendler, G.B.; Kenneley, I.L.; Lopez, C.; McBride, P.J.; Walker, B.W. Lippincott’s Guide to Infectious Diseases; Lippincott Williams & Wilkins: Philadelphi, PA, USA, 2011; Available online: https://www.wolterskluwer.com/en/solutions/ovid/lippincotts-guide-to-infectious-diseases-8850 (accessed on 15 April 2023).
- Ferri, F.F. Ferri’s Clinical Advisor 2016; Elsevier, Inc.: Amsterdam, The Netherlands, 2016. [Google Scholar]
- Mohseni, S.; Shojaiefard, A.; Khorgami, Z.; Alinejad, S.; Ghorbani, A.; Ghafouri, A. Peripheral Lymphadenopathy: Approach and Diagnostic Tools. Iran. J. Med Sci. 2014, 39, 158–170. [Google Scholar]
- Leung, A.K.C.; Dele Davies, H. Cervical lymphadenitis: Etiology, diagnosis, and management. Curr. Infect. Dis. Rep. 2009, 11, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Gaddey, H.L.; Riegel, A.M. Unexplained Lymphadenopathy: Evaluation and Differential Diagnosis. Am. Fam. Physician 2016, 94, 896–903. [Google Scholar] [PubMed]
- Supali, T.; Ismid, I.S.; Rückert, P.; Fischer, P. Treatment of Brugia timori and Wuchereria bancrofti infections in Indonesia using DEC or a combination of DEC and albendazole: Adverse reactions and short-term effects on microfilariae. Trop. Med. Int. Health 2002, 7, 894–901. [Google Scholar] [CrossRef] [PubMed]
- Ismail, M.; Jayakody, R.; Weil, G.; Nirmalan, N.; Jayasinghe, K.; Abeyewickrema, W.; Sheriff, M.; Rajaratnam, H.; Amarasekera, N.; De Silva, D.; et al. Efficacy of single dose combinations of albendazole, ivermectin and diethylcarbamazine for the treatment of bancroftian filariasis. Trans. R. Soc. Trop. Med. Hyg. 1998, 92, 94–97. [Google Scholar] [CrossRef] [PubMed]
- Addiss, D.G.; Eberhard, M.L.; Lammie, P.J.; McNeeley, M.B.; Lee, S.H.; Spencer, H.C. Comparative Efficacy of Clearing-Dose and Single High-Dose Ivermectin and Diethylcarbamazine against Wuchereria bancrofti Microfilaremia. Am. J. Trop. Med. Hyg. 1993, 48, 178–185. [Google Scholar] [CrossRef]
- Lu, Y.; Aimetti, A.A.; Langer, R.; Gu, Z. Bioresponsive materials. Nat. Rev. Mater. 2016, 2, 16075. [Google Scholar] [CrossRef]
- Sonawane, S.J.; Kalhapure, R.S.; Rambharose, S.; Mocktar, C.; Vepuri, S.B.; Soliman, M.; Govender, T. Ultra-small lipid-dendrimer hybrid nanoparticles as a promising strategy for antibiotic delivery: In vitro and in silico studies. Int. J. Pharm. 2016, 504, 1–10. [Google Scholar] [CrossRef]
- Gao, W.; Chen, Y.; Zhang, Y.; Zhang, Q.; Zhang, L. Nanoparticle-based local antimicrobial drug delivery. Adv. Drug Deliv. Rev. 2018, 127, 46–57. [Google Scholar] [CrossRef]
- Gandhi, K.; Maganti, R.S.; Kaur, H.; Vinod, K.S.; Verma, P. Formulation and evaluation of Sol-Gel drug delivery system for intracanal pH sensitive controlled delivery of chlorhexidine. J. Clin. Diagn. Res. 2017, 11, ZC68–ZC72. [Google Scholar] [CrossRef]
- Liu, P.; Xu, G.; Pranantyo, D.; Xu, L.Q.; Neoh, K.-G.; Kang, E.-T. PH-Sensitive Zwitterionic Polymer as an Antimicrobial Agent with Effective Bacterial Targeting. ACS Biomater. Sci. Eng. 2018, 4, 40–46. [Google Scholar] [CrossRef]
- Tate, S.; MacGregor, G.; Davis, M.; Innes, J.A.; Greening, A.P. Airways in cystic fibrosis are acidified: Detection by exhaled breath condensate. Thorax 2002, 57, 926–929. [Google Scholar] [CrossRef] [PubMed]
- Kalhapure, R.S.; Sikwal, D.R.; Rambharose, S.; Mocktar, C.; Singh, S.; Bester, L.A.; Oh, J.K.; Renukuntla, J.; Govender, T. Enhancing targeted antibiotic therapy via pH responsive solid lipid nanoparticles from an acid cleavable lipid. Nanomed. Nanotechnol. Biol. Med. 2017, 13, 2067–2077. [Google Scholar] [CrossRef] [PubMed]
- Mhule, D.; Kalhapure, R.S.; Jadhav, M.; Omolo, C.A.; Rambharose, S.; Mocktar, C.; Singh, S.; Waddad, A.Y.; Ndesendo, V.M.; Govender, T. Synthesis of an oleic acid based pH-responsive lipid and its application in nanodelivery of vancomycin. Int. J. Pharm. 2018, 550, 149–159. [Google Scholar] [CrossRef] [PubMed]
- Makhathini, S.S.; Kalhapure, R.S.; Jadhav, M.; Waddad, A.Y.; Gannimani, R.; Omolo, C.A.; Rambharose, S.; Mocktar, C.; Govender, T. Novel two-chain fatty acid-based lipids for development of vancomycin pH-responsive liposomes against Staphylococcus aureus and methicillin-resistant Staphylococcus aureus (MRSA). J. Drug Target 2019, 27, 1094–1107. [Google Scholar] [CrossRef]
- Osman, N.; Omolo, C.A.; Gannimani, R.; Waddad, A.Y.; Rambharose, S.; Mocktar, C.; Singh, S.; Parboosing, R.; Govender, T. Novel fatty acid-based pH-responsive nanostructured lipid carriers for enhancing antibacterial delivery. J. Drug Deliv. Sci. Technol. 2019, 53, 101125. [Google Scholar] [CrossRef]
- Singh, N.; Romero, M.; Travanut, A.; Monteiro, P.F.; Jordana-Lluch, E.; Hardie, K.R.; Williams, P.; Alexander, M.R.; Alexander, C. Dual bioresponsive antibiotic and quorum sensing inhibitor combination nanoparticles for treatment of Pseudomonas aeruginosa biofilms in vitro and ex vivo. Biomater. Sci. 2019, 7, 4099–4111. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, M.M.; Carlini, A.S.; Chien, M.-P.; Sonnenberg, S.; Luo, C.; Braden, R.L.; Osborn, K.G.; Li, Y.; Gianneschi, N.C.; Christman, K.L. Enzyme-Responsive Nanoparticles for Targeted Accumulation and Prolonged Retention in Heart Tissue after Myocardial Infarction. Adv. Mater. 2015, 27, 5547–5552. [Google Scholar] [CrossRef] [PubMed]
- Callmann, C.E.; Barback, C.V.; Thompson, M.P.; Hall, D.J.; Mattrey, R.F.; Gianneschi, N.C. Therapeutic Enzyme-Responsive Nanoparticles for Targeted Delivery and Accumulation in Tumors. Adv. Mater. 2015, 27, 4611–4615. [Google Scholar] [CrossRef]
- de la Rica, R.; Aili, D.; Stevens, M.M. Enzyme-responsive nanoparticles for drug release and diagnostics. Adv. Drug Deliv. Rev. 2012, 64, 967–978. [Google Scholar] [CrossRef]
- Lock, L.L.; Tang, Z.; Keith, D.; Reyes, C.; Cui, H. Enzyme-specific doxorubicin drug beacon as drug-resistant theranostic molecular probes. ACS Macro. Lett. 2015, 4, 552–555. [Google Scholar] [CrossRef]
- Grützner, V.; Unger, R.E.; Baier, G.; Choritz, L.; Freese, C.; Böse, T.; Landfester, K.; Kirkpatrick, C.J. Enzyme-responsive nanocomposites for wound infection prophylaxis in burn management: In vitro evaluation of their compatibility with healing processes. Int. J. Nanomed. 2015, 10, 4111–4124. [Google Scholar] [CrossRef] [PubMed]
- Garzoni, C.; Kelley, W.L. Staphylococcus aureus: New evidence for intracellular persistence. Trends Microbiol. 2009, 17, 59–65. [Google Scholar] [CrossRef]
- Irache, J.M.; Salman, H.H.; Gamazo, C.; Espuelas, S. Mannose-targeted systems for the delivery of therapeutics. Expert Opin. Drug Deliv. 2008, 5, 703–724. [Google Scholar] [CrossRef] [PubMed]
- Wijagkanalan, W.; Kawakami, S.; Higuchi, Y.; Yamashita, F.; Hashida, M. Intratracheally instilled mannosylated cationic liposome/NFκB decoy complexes for effective prevention of LPS-induced lung inflammation. J. Control Release 2011, 149, 42–50. [Google Scholar] [CrossRef]
- Xiong, M.-H.; Li, Y.-J.; Bao, Y.; Yang, X.-Z.; Hu, B.; Wang, J. Bacteria-responsive multifunctional nanogel for targeted antibiotic delivery. Adv. Mater. 2012, 24, 6175–6180. [Google Scholar] [CrossRef]
- Xiong, M.H.; Bao, Y.; Yang, X.Z.; Wang, Y.C.; Sun, B.; Wang, J. Lipase-Sensitive Polymeric Triple-Layered Nanogel for “On-Demand” Drug Delivery. J. Am. Chem. Soc. 2012, 134, 4355–4362. [Google Scholar] [CrossRef]
- Li, Y.; Liu, G.; Wang, X.; Hu, J.; Liu, S. Enzyme-Responsive Polymeric Vesicles for Bacterial-Strain-Selective Delivery of Antimicrobial Agents. Angew. Chem. Int. Ed. 2016, 55, 1760–1764. [Google Scholar] [CrossRef]
- Baier, G.; Cavallaro, A.; Vasilev, K.; Mailänder, V.; Musyanovych, A.; Landfester, K. Enzyme responsive hyaluronic acid nanocapsules containing polyhexanide and their exposure to bacteria to prevent infection. Biomacromolecules 2013, 14, 1103–1112. [Google Scholar] [CrossRef]
- Mu, S.; Liu, W.; Zhao, L.; Long, Y.; Gu, H. Antimicrobial AgNPs composites of gelatin hydrogels crosslinked by ferrocene-containing tetrablock terpolymer. Polymer 2019, 169, 80–94. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhang, J.; Chen, W.; Angsantikul, P.; Spiekermann, A.K.; Fang, R.H.; Gao, W.; Zhang, L. Erythrocyte membrane-coated nanogel for combinatorial antivirulence and responsive antimicrobial delivery against Staphylococcus aureus infection. J. Control. Release 2017, 263, 185–191. [Google Scholar] [CrossRef]
- Amoli-Diva, M.; Sadighi-Bonabi, R.; Pourghazi, K. Laser-assisted triggered-drug release from silver nanoparticles-grafted dual-responsive polymer. Mater. Sci. Eng. C 2017, 76, 536–542. [Google Scholar] [CrossRef] [PubMed]
- Maleki, A.; He, J.; Bochani, S.; Nosrati, V.; Shahbazi, M.-A.; Guo, B. Multifunctional Photoactive Hydrogels for Wound Healing Acceleration. ACS Nano 2021, 15, 18895–18930. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Yang, Y.; Shi, Y.; Song, H.; Yu, C. Antibiotic-Free Antibacterial Strategies Enabled by Nanomaterials: Progress and Perspectives. Adv. Mater. 2020, 32, 1904106. [Google Scholar] [CrossRef]
- Ballesteros CA, S.; Correa, D.S.; Zucolotto, V. Polycaprolactone nanofiber mats decorated with photoresponsive nanogels and silver nanoparticles: Slow release for antibacterial control. Mater. Sci. Eng. C 2020, 107, 110334. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Li, H.; Tao, X.; Xie, Y.; Yang, L.; Mao, Z.; Xia, W. Light-Triggered Nitric Oxide Release by a Photosensitizer to Combat Bacterial Biofilm Infections. Chem. A Eur. J. 2020, 27, 5453–5460. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.; Gan, G.; Shen, Z.; Gao, L.; Zhang, G.; Hu, J. Red Light-Triggered Intracellular Carbon Monoxide Release Enables Selective Eradication of MRSA Infection. Angew. Chem. 2021, 133, 13625–13632. [Google Scholar] [CrossRef]
- Pang, Q.; Jiang, Z.; Wu, K.; Hou, R.; Zhu, Y. Nanomaterials-Based Wound Dressing for Advanced Management of Infected Wound. Antibiotics 2023, 12, 351. [Google Scholar] [CrossRef]
- Wang, J.; Zhang, C.; Yang, Y.; Fan, A.; Chi, R.; Shi, J.; Zhang, X. Poly (vinyl alcohol) (PVA) hydrogel incorporated with Ag/TiO2 for rapid sterilization by photoinspired radical oxygen species and promotion of wound healing. Appl. Surf. Sci. 2019, 494, 708–720. [Google Scholar] [CrossRef]
- Owen, D.H.; Katz, D.F. A vaginal fluid simulant. Contraception 1999, 59, 91–95. [Google Scholar] [CrossRef]
- Pandey, M.; Choudhury, H.; Abdul-Aziz, A.; Bhattamisra, S.K.; Gorain, B.; Carine, T.; Wee Toong, T.; Yi, N.J.; Win Yi, L. Promising drug delivery approaches to treat microbial infections in the vagina: A recent update. Polymers 2021, 23, 26. [Google Scholar] [CrossRef]
- Martín-Illana, A.; Notario-Pérez, F.; Cazorla-Luna, R.; Ruiz-Caro, R.; Veiga, M.D. Smart Freeze-Dried Bigels for the Prevention of the Sexual Transmission of HIV by Accelerating the Vaginal Release of Tenofovir during Intercourse. Pharmaceutics 2019, 11, 232. [Google Scholar] [CrossRef] [PubMed]
- Cazorla-Luna, R.; Martín-Illana, A.; Notario-Pérez, F.; Bedoya, L.M.; Tamayo, A.; Ruiz-Caro, R.; Rubio, J.; Veiga, M.-D. Vaginal polyelectrolyte layer-by-layer films based on chitosan derivatives and Eudragit® S100 for pH responsive release of tenofovir. Mar. Drugs 2020, 18, 44. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Traore, Y.L.; Chen, Y.; Ho, E.A.; Liu, S. Switchable On-Demand Release of a Nanocarrier from a Segmented Reservoir Type Intravaginal Ring Filled with a pH-Responsive Supramolecular Polyurethane Hydrogel. ACS Appl. Bio Mater. 2018, 1, 652–662. [Google Scholar] [CrossRef] [PubMed]
- Ilomuanya, M.O.; Elesho, R.F.; Amenaghawon, A.N.; Adetuyi, A.O.; Velusamy, V.; Akanmu, A.S. Development of trigger sensitive hyaluronic acid/palm oil-based organogel for in vitro release of HIV/AIDS microbicides using artificial neural networks. Future J. Pharm. Sci. 2020, 6, 1. [Google Scholar] [CrossRef]
- Valcarcel, J.; García, M.R.; Varela, U.R.; Vázquez, J.A. Hyaluronic acid of tailored molecular weight by enzymatic and acid depolymerization. Int. J. Biol. Macromol. 2020, 145, 788–794. [Google Scholar] [CrossRef]
- Buhren, B.A.; Schrumpf, H.; Hoff, N.-P.; Bölke, E.; Hilton, S.; Gerber, P.A. Hyaluronidase: From clinical applications to molecular and cellular mechanisms. Eur. J. Med. Res. 2016, 21, 5. [Google Scholar] [CrossRef]
- Mei, L.; Chen, J.; Yu, S.; Huang, Y.; Xie, Y.; Wang, H.; Pan, X.; Wu, C. Expansible thermal gelling foam aerosol for vaginal drug delivery. Drug Deliv. 2017, 24, 1325–1337. [Google Scholar] [CrossRef]
- Tuğcu-Demiröz, F. Development of in situ poloxamer-chitosan hydrogels for vaginal drug delivery of benzydamine hydrochloride: Textural, mucoadhesive and in vitro release properties. Marmara Pharm. J. 2017, 21, 762–770. [Google Scholar] [CrossRef]
- Jelvehgari, M.; Montazam, H. Evaluation of mechanical and rheological properties of metronidazole gel as local delivery system. Arch. Pharm. Res. 2011, 34, 931–940. [Google Scholar] [CrossRef]
- Cevher, E.; Taha MA, M.; Orlu, M.; Araman, A. Evaluation of mechanical and mucoadhesive properties of clomiphene citrate gel formulations containing carbomers and their thiolated derivatives. Drug Deliv. 2008, 15, 57–67. [Google Scholar] [CrossRef]
- Gupta, H.; Sharma, A. Ion activated bioadhesive in situ gel of clindamycin for vaginal application. Int. J. Drug Deliv. 2011, 1, 32–40. [Google Scholar] [CrossRef]
- Patel, P.; Patel, P. Formulation and evaluation of clindamycin HCL in situ gel for vaginal application. Int. J. Pharm. Investig. 2015, 5, 50. [Google Scholar] [CrossRef]
- Yenkar, P.; Mayee, R.; Nawale, R.; Chavan, R.; Salunke, T.; Bhoyar, V. Bio responsive in situ gel of clindamycin for vaginal application. Res. Rev. J. Pharm. Pharm. Sci. 2013, 2, 26–32. Available online: https://www.semanticscholar.org/paper/Bio-Responsive-In-Situ-Gel-of-Clindamycin-for-Yenkar-Mayee/a30d3d99c2e0ab536fc5c739f6c84906600b8a98 (accessed on 15 April 2023).
- Faria, M.J.; Machado, R.; Ribeiro, A.; Gonçalves, H.; Oliveira, M.E.C.D.R.; Viseu, T.; das Neves, J.; Lúcio, M. Rational development of liposomal hydrogels: A strategy for topical vaginal antiretroviral drug delivery in the context of HIV prevention. Pharmaceutics 2019, 11, 485. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Kaushal, J.C. Thermosensitive in situ gel of tinidazole in treatment of bacterial vaginosis: Formulation and evaluation. Int. J. Ayu. Alt. Med. 2014, 2, 1610. [Google Scholar]
- Agrawal, A.K.; Das, M.; Jain, S. In situ gel systems as ‘smart’ carriers for sustained ocular drug delivery. Expert Opin. Drug Deliv. 2012, 9, 383–402. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Haglund, B.O.; Himmelstein, K.J. In Situ-Forming Gels for Ophthalmic Drug Delivery. J. Ocul. Pharmacol. 1994, 10, 47–56. [Google Scholar] [CrossRef]
- Kumar, S.; Himmelstein, K.J. Modification of in situ gelling behavior of carbopol solutions by hydroxypropyl methylcellulose. J. Pharm. Sci. 1995, 84, 344–348. [Google Scholar] [CrossRef]
- Srividya, B.; Cardoza, R.M.; Amin, P.D. Sustained ophthalmic delivery of ofloxacin from a pH triggered in situ gelling system. J. Control. Release 2001, 73, 205–211. [Google Scholar] [CrossRef]
- Jain, S.P.; Shah, S.P.; Rajadhyaksha, N.S.; Pirthi, P.S.; Amin, P.D. In situ ophthalmic gel of ciprofloxacin hydrochloride for once a day sustained delivery. Drug Dev. Ind. Pharm. 2008, 34, 445–452. [Google Scholar] [CrossRef]
- Varshosaz, J.; Tabbakhian, M.; Salmani, Z. Designing of a Thermosensitive Chitosan/Poloxamer In Situ Gel for Ocular Delivery of Ciprofloxacin. Open Drug Deliv. J. 2008, 2, 61–70. [Google Scholar] [CrossRef]
- Obuobi, S.; Mayandi, V.; Nor, N.A.M.; Lee, B.J.; Lakshminarayanan, R.; Ee, P.L.R. Nucleic acid peptide nanogels for the treatment of bacterial keratitis. Nanoscale 2020, 12, 17411–17425. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Tao, Q.; Xie, J.; Lu, L.; Xie, X.; Zhang, Y.; Jin, Y. Advances in Nanogels for Topical Drug Delivery in Ocular Diseases. Gels 2023, 9, 292. [Google Scholar] [CrossRef]
- Lin, X.; Ma, Q.; Su, J.; Wang, C.; Kankala, R.K.; Zeng, M.; Lin, H.; Zhou, S.-F. Dual-Responsive Alginate Hydrogels for Controlled Release of Therapeutics. Molecules 2019, 24, 2089. [Google Scholar] [CrossRef] [PubMed]
- Yin, M.-J.; Yao, M.; Gao, S.; Zhang, A.P.; Tam, H.-Y.; Wai, P.-K.A. Rapid 3D Patterning of Poly(acrylic acid) Ionic Hydrogel for Miniature pH Sensors. Adv. Mater. 2015, 28, 1394–1399. [Google Scholar] [CrossRef] [PubMed]
- Davaran, S.; Lotfipour, F.; Sedghipour, N.; Sedghipour, M.R.; Alimohammadi, S.; Salehi, R. Preparation and in vivo evaluation of in situ gel system as dual thermo-/pH-responsive nanocarriers for sustained ocular drug delivery. J. Microencapsul. 2015, 32, 511–519. [Google Scholar]
- Permana, A.D.; Utami, R.N.; Layadi, P.; Himawan, A.; Juniarti, N.; Anjani, Q.K.; Utomo, E.; Mardikasari, S.A.; Arjuna, A.; Donnelly, R.F. Thermosensitive and mucoadhesive in situ ocular gel for effective local delivery and antifungal activity of itraconazole nanocrystal in the treatment of fungal keratitis. Int. J. Pharm. 2021, 602, 120623. [Google Scholar] [CrossRef]
- Scherließ, R.; Etschmann, C. DPI formulations for high dose applications—Challenges and opportunities. Int. J. Pharm. 2018, 548, 49–53. [Google Scholar] [CrossRef]
- Scherließ, R. Future of nanomedicines for treating respiratory diseases. Expert Opin. Drug Deliv. 2019, 16, 59–68. [Google Scholar] [CrossRef]
- Hwang, A.A.; Lee, B.Y.; Clemens, D.L.; Dillon, B.J.; Zink, J.I.; Horwitz, M.A. pH-Responsive Isoniazid-Loaded Nanoparticles Markedly Improve Tuberculosis Treatment in Mice. Small 2015, 11, 5066–5078. [Google Scholar] [CrossRef]
- Davaran, S.; Lotfipour, F.; Sedghipour, N.; Sedghipour, M.R.; Alimohammadi, S.; Salehi, R. Montmorillonite–Rifampicin Nanohybrid for pH-Responsive Release of the Tuberculostatic. Pharmaceutics 2023, 15, 512. [Google Scholar]
- Secret, E.; Kelly, S.J.; Crannell, K.E.; Andrew, J.S. Enzyme-Responsive Hydrogel Microparticles for Pulmonary Drug Delivery. ACS Appl. Mater. Interfaces 2014, 6, 10313–10321. [Google Scholar] [CrossRef] [PubMed]
- Maretti, E.; Costantino, L.; Rustichelli, C.; Leo, E.; Croce, M.A.; Buttini, F.; Truzzi, E.; Iannuccelli, V. Surface engineering of Solid Lipid Nanoparticle assemblies by methyl α- d -mannopyranoside for the active targeting to macrophages in anti-tuberculosis inhalation therapy. Int. J. Pharm. 2017, 528, 440–451. [Google Scholar] [CrossRef] [PubMed]
- Alves, A.D.; Cavaco, J.S.; Guerreiro, F.; Lourenço, J.P.; Da Costa, A.M.R.; Grenha, A.; Da Costa, A.M.R. Inhalable Antitubercular Therapy Mediated by Locust Bean Gum Microparticles. Molecules 2016, 21, 702. [Google Scholar] [CrossRef] [PubMed]
- Guerreiro, F.; Pontes, J.F.; Rosa da Costa, A.M.; Grenha, A. Spray-drying of konjac glucomannan to produce microparticles for an application as antitubercular drug carriers. Powder Technol. 2019, 342, 246–252. [Google Scholar] [CrossRef]
- Maretti, E.; Costantino, L.; Buttini, F.; Rustichelli, C.; Leo, E.; Truzzi, E.; Iannuccelli, V. Newly synthesized surfactants for surface mannosylation of respirable SLN assemblies to target macrophages in tuberculosis therapy. Drug Deliv. Transl. Res. 2018, 9, 298–310. [Google Scholar] [CrossRef]
- Gaspar, D.P.; Gaspar, M.M.; Eleutério, C.V.; Grenha, A.; Blanco, M.; Gonçalves, L.M.D.; Taboada, P.; Almeida, A.J.; Remuñán-López, C. Microencapsulated Solid Lipid Nanoparticles as a Hybrid Platform for Pulmonary Antibiotic Delivery. Mol. Pharm. 2017, 14, 2977–2990. [Google Scholar] [CrossRef]
- Melis, V.; Manca, M.L.; Bullita, E.; Tamburini, E.; Castangia, I.; Cardia, M.C.; Valenti, D.; Fadda, A.M.; Peris, J.E.; Manconi, M. Inhalable polymer-glycerosomes as safe and effective carriers for rifampicin delivery to the lungs. Colloids Surf. B Biointerfaces 2016, 143, 301–308. [Google Scholar] [CrossRef]
- Shah, K.; Chan, L.W.; Wong, T.W. Critical physicochemical and biological attributes of nanoemulsions for pulmonary delivery of rifampicin by nebulization technique in tuberculosis treatment. Drug Deliv. 2017, 24, 1631–1647. [Google Scholar] [CrossRef]
- Manca, M.L.; Castangia, I.; Caddeo, C.; Pando, D.; Escribano, E.; Valenti, D.; Lampis, S.; Zaru, M.; Fadda, A.M.; Manconi, M. Improvement of quercetin protective effect against oxidative stress skin damages by incorporation in nanovesicles. Colloids Surf. B Biointerfaces 2014, 123, 566–574. [Google Scholar] [CrossRef]
- Dicker, K.T.; Gurski, L.A.; Pradhan-Bhatt, S.; Witt, R.L.; Farach-Carson, M.C.; Jia, X. Hyaluronan: A simple polysaccharide with diverse biological functions. Acta Biomater. 2013, 10, 1558–1570. [Google Scholar] [CrossRef] [PubMed]
- Kwon, M.Y.; Wang, C.; Galarraga, J.H.; Puré, E.; Han, L.; Burdick, J.A. Influence of hyaluronic acid modification on CD44 binding towards the design of hydrogel biomaterials. Biomaterials 2019, 222, 119451. [Google Scholar] [CrossRef] [PubMed]
- East, L.; Isacke, C.M. The mannose receptor family. Biochim. Biophys. Acta Gen. Subj. 2002, 1572, 364–386. [Google Scholar] [CrossRef]
- Pourshahab, P.S.; Gilani, K.; Moazeni, E.; Eslahi, H.; Fazeli, M.R.; Jamalifar, H. Preparation and characterization of spray dried inhalable powders containing chitosan nanoparticles for pulmonary delivery of isoniazid. J. Microencapsul. 2011, 28, 605–613. [Google Scholar] [CrossRef]
- Rawal, T.; Patel, S.; Butani, S. Chitosan nanoparticles as a promising approach for pulmonary delivery of bedaquiline. Eur. J. Pharm. Sci. 2018, 124, 273–287. [Google Scholar] [CrossRef]
- Cunha, L.; Rodrigues, S.; da Costa, A.M.R.; Faleiro, M.L.; Buttini, F.; Grenha, A. Inhalable chitosan microparticles for simultaneous delivery of isoniazid and rifabutin in lung tuberculosis treatment. Drug Dev. Ind. Pharm. 2019, 45, 1313–1320. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Liao, W.; Wang, W.; Zhou, J.; Tan, W.; Xiang, W.; Zhang, J.; Guo, L.; Chen, T.; Ma, D.; et al. Genipin-crosslinked carboxymethyl chitosan nanogel for lung-targeted delivery of isoniazid and rifampin. Carbohydr. Polym. 2018, 197, 403–413. [Google Scholar] [CrossRef]
- Ong, V.; Mei, V.; Cao, L.; Lee, K.; Chung, E.J. Nanomedicine for Cystic Fibrosis. SLAS Technol. 2019, 24, 169–180. [Google Scholar] [CrossRef]
- Kozáková, J.; Altay, A.; Ždímal, V.; Mašková, L.; Sonvico, F.; Quarta, E.; Rossi, A.; Buttini, F.; Colombo, G. Dry powder inhaler of colistimethate sodium for lung infections in cystic fibrosis: Optimization of powder construction. Drug Dev. Ind. Pharm. 2019, 45, 1664–1673. [Google Scholar] [CrossRef]
- Cayli, Y.A.; Sahin, S.; Buttini, F.; Balducci, A.G.; Montanari, S.; Vural, I.; Oner, L. Dry powders for the inhalation of ciprofloxacin or levofloxacin combined with a mucolytic agent for cystic fibrosis patients. Drug Dev. Ind. Pharm. 2017, 43, 1378–1389. [Google Scholar] [CrossRef]
- Chance, D.L.; Mawhinney, T.P. Observations of, and Insights into, Cystic Fibrosis Mucus Heterogeneity in the Pre-Modulator Era: Sputum Characteristics, DNA and Glycoprotein Content, and Solubilization Time. J. Respir. 2020, 1, 8–29. [Google Scholar] [CrossRef]
- Prasher, P.; Sharma, M.; Singh, S.K.; Gulati, M.; Jha, N.K.; Gupta, P.K.; Gupta, G.; Chellappan, D.K.; Zacconi, F.; Pinto, T.D.J.A.; et al. Targeting mucus barrier in respiratory diseases by chemically modified advanced delivery systems. Chem. -Biol. Interact. 2022, 365, 110048. [Google Scholar] [CrossRef] [PubMed]
- Bahamondez-Canas, T.F.; Zhang, H.; Tewes, F.; Leal, J.; Smyth, H.D.C. PEGylation of Tobramycin Improves Mucus Penetration and Antimicrobial Activity against Pseudomonas aeruginosa Biofilms in Vitro. Mol. Pharmacol. 2018, 15, 1643–1652. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Sastre, M.; Pastor, M.; Esquisabel, A.; Sans, E.; Viñas, M.; Fleischer, A.; Palomino, E.; Bachiller, D.; Pedraz, J.L. Pulmonary delivery of tobramycin-loaded nanostructured lipid carriers for Pseudomonas aeruginosa infections associated with cystic fibrosis. Int. J. Pharm. 2016, 498, 263–273. [Google Scholar] [CrossRef]
- Schneider, C.S.; Xu, Q.; Boylan, N.J.; Chisholm, J.; Tang, B.C.; Schuster, B.S.; Henning, A.; Ensign, L.M.; Lee, E.; Adstamongkonkul, P.; et al. Nanoparticles that do not adhere to mucus provide uniform and long-lasting drug delivery to airways following inhalation. Sci. Adv. 2017, 3, e1601556. [Google Scholar] [CrossRef]
- D’angelo, I.; Casciaro, B.; Miro, A.; Quaglia, F.; Mangoni, M.L.; Ungaro, F. Overcoming barriers in Pseudomonas aeruginosa lung infections: Engineered nanoparticles for local delivery of a cationic antimicrobial peptide. Colloids Surf. B Biointerfaces 2015, 135, 717–725. [Google Scholar] [CrossRef]
- Ungaro, F.; D’Angelo, I.; Coletta, C.; Bianca, R.D.D.V.; Sorrentino, R.; Perfetto, B.; Tufano, M.A.; Miro, A.; La Rotonda, M.I.; Quaglia, F. Dry powders based on PLGA nanoparticles for pulmonary delivery of antibiotics: Modulation of encapsulation efficiency, release rate and lung deposition pattern by hydrophilic polymers. J. Control. Release 2012, 157, 149–159. [Google Scholar] [CrossRef]
- Du, J.; El-Sherbiny, I.M.; Smyth, H.D. Swellable Ciprofloxacin-Loaded Nano-in-Micro Hydrogel Particles for Local Lung Drug Delivery. Ageing Int. 2014, 15, 1535–1544. [Google Scholar] [CrossRef]
- Rathnayake, K.; Patel, U.; Pham, C.; McAlpin, A.; Budisalich, T.; Jayawardena, S.N. Targeted Delivery of Antibiotic Therapy to Inhibit Pseudomonas aeruginosa Using Lipid-Coated Mesoporous Silica Core–Shell Nanoassembly. ACS Appl. Biol. Mater. 2020, 3, 6708–6721. [Google Scholar] [CrossRef]
- Mizoguchi, R.; Waraya, H.; Hirakura, Y. Application of Co-Amorphous Technology for Improving the Physicochemical Properties of Amorphous Formulations. Mol. Pharm. 2019, 16, 2142–2152. [Google Scholar] [CrossRef]
- Karagianni, A.; Kachrimanis, K.; Nikolakakis, I. Co-amorphous solid dispersions for solubility and absorption improvement of drugs: Composition, preparation, characterization and formulations for oral delivery. Pharmaceutics 2018, 10, 98. [Google Scholar] [CrossRef] [PubMed]
- Momin, M.A.M.; Sinha, S.; Tucker, I.G.; Doyle, C.; Das, S.C. Dry powder formulation of kanamycin with enhanced aerosolization efficiency for drug-resistant tuberculosis. Int. J. Pharm. 2017, 528, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Lababidi, N.; Kissi, E.O.; Elgaher, W.A.; Sigal, V.; Haupenthal, J.; Schwarz, B.C.; Hirsch, A.K.; Rades, T.; Schneider, M. Spray-drying of inhalable, multifunctional formulations for the treatment of biofilms formed in cystic fibrosis. J. Control. Release 2019, 314, 62–71. [Google Scholar] [CrossRef]
- Salvati, A.; Aberg, C.; dos Santos, T.; Varela, J.; Pinto, P.; Lynch, I.; Dawson, K.A. Experimental and theoretical comparison of intracellular import of polymeric nanoparticles and small molecules: Toward models of uptake kinetics. Nanomedicine 2011, 7, 818–826. [Google Scholar] [CrossRef]
- Mangal, S.; Nie, H.; Xu, R.; Guo, R.; Cavallaro, A.; Zemlyanov, D.; Zhou, Q. Physico-Chemical Properties, Aerosolization and Dissolution of Co-Spray Dried Azithromycin Particles with L-Leucine for Inhalation. Pharm. Res. 2018, 35, 28. [Google Scholar] [CrossRef]
- Lamy, B.; Tewes, F.; Serrano, D.R.; Lamarche, I.; Gobin, P.; Couet, W.; Healy, A.M.; Marchand, S. New aerosol formulation to control ciprofloxacin pulmonary concentration. J. Control. Release 2018, 271, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Tewes, F.; Brillault, J.; Lamy, B.; O’connell, P.; Olivier, J.-C.; Couet, W.; Healy, A.M. Ciprofloxacin-Loaded Inorganic–Organic Composite Microparticles To Treat Bacterial Lung Infection. Mol. Pharm. 2015, 13, 100–112. [Google Scholar] [CrossRef]
- Nafee, N.; Forier, K.; Braeckmans, K.; Schneider, M. Mucus-penetrating solid lipid nanoparticles for the treatment of cystic fibrosis: Proof of concept, challenges and pitfalls. Eur. J. Pharm. Biopharm. 2018, 124, 125–137. [Google Scholar] [CrossRef]
- Alp, G.; Aydogan, N. Lipid-based mucus penetrating nanoparticles and their biophysical interactions with pulmonary mucus layer. Eur. J. Pharm. Biopharm. 2020, 149, 45–57. [Google Scholar] [CrossRef]
- Wu, X.; Zhang, W.; Hayes, D.; Mansour, H.M. Physicochemical characterization and aerosol dispersion performance of organic solution advanced spray-dried cyclosporine A multifunctional particles for dry powder inhalation aerosol delivery. Int. J. Nanomed. 2013, 8, 1269–1283. [Google Scholar]
- Sanders, N.; Rudolph, C.; Braeckmans, K.; De Smedt, S.C.; Demeester, J. Extracellular barriers in respiratory gene therapy. Adv. Drug Deliv. Rev. 2009, 61, 115–127. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.C.; Li, R.Y.; Chen, J.Y.; Chen, J.K. Biphasic release of gentamicin from chitosan/fucoidan nanoparticles for pulmonary delivery. Carbohydrat Polym. 2016, 138, 114–122. [Google Scholar] [CrossRef] [PubMed]
- Torge, A.; Wagner, S.; Chaves, P.S.; Oliveira, E.G.; Guterres, S.S.; Pohlmann, A.R.; Titz, A.; Schneider, M.; Beck, R.C. Ciprofloxacin-loaded lipid-core nanocapsules as mucus penetrating drug delivery system intended for the treatment of bacterial infections in cystic fibrosis. Int. J. Pharm. 2017, 527, 92–102. [Google Scholar] [CrossRef] [PubMed]
- Al-Bakri, A.G.; Mahmoud, N.N. Photothermal-Induced Antibacterial Activity of Gold Nanorods Loaded into Polymeric Hydrogel against Pseudomonas aeruginosa Biofilm. Molecules 2019, 24, 2661. [Google Scholar] [CrossRef]
- Wan, F.; Nylander, T.; Klodzinska, S.N.; Foged, C.; Yang, M.; Baldursdóttir, S.G.; Nielsen, H.M. Lipid Shell-Enveloped Polymeric Nanoparticles with High Integrity of Lipid Shells Improve Mucus Penetration and Interaction with Cystic Fibrosis-Related Bacterial Biofilms. ACS Appl. Mater. Interfaces 2018, 10, 10678–10687. [Google Scholar] [CrossRef]
- Luo, M.; Jia, Y.-Y.; Jing, Z.-W.; Li, C.; Zhou, S.-Y.; Mei, Q.-B.; Zhang, B.-L. Construction and optimization of pH-sensitive nanoparticle delivery system containing PLGA and UCCs-2 for targeted treatment of Helicobacter pylori. Colloids Surf. B Biointerfaces 2018, 164, 11–19. [Google Scholar] [CrossRef]
- Chahardahmasoumi, S.; Sarvi, M.N.; Jalali, S.A.H. Modified montmorillonite nanosheets as a nanocarrier with smart pH-responsive control on the antimicrobial activity of tetracycline upon release. Appl. Clay Sci. 2019, 178, 105135. [Google Scholar] [CrossRef]
- Thamphiwatana, S.; Gao, W.; Pornpattananangkul, D.; Zhang, Q.; Fu, V.; Li, J.; Li, J.; Obonyo, M.; Zhang, L. Phospholipase A2-responsive antibiotic delivery via nanoparticle-stabilized liposomes for the treatment of bacterial infection. J. Mater. Chem. B 2014, 2, 8201–8207. [Google Scholar] [CrossRef]
- Zhang, S.; Sunami, Y.; Hashimoto, H. Mini review: Nanosheet technology towards biomedical application. Nanomaterials 2017, 7, 246. [Google Scholar] [CrossRef]
- Ofokansi, K.C.; Adikwu, M.U. Formulation and Evaluation of Microspheres Based on Gelatin-Mucin Admixtures for the Rectal Delivery of Cefuroxime Sodium. Trop. J. Pharm. Res. 2007, 6, 825–832. [Google Scholar] [CrossRef][Green Version]
- Heffernan, J.M.; McLaren, A.C.; Overstreet, D.J. Local antimicrobial delivery from temperature-responsive hydrogels reduces incidence of intra-abdominal infection in rats. Comp. Immunol. Microbiol. Infect. Dis. 2022, 86, 101823. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Chaves, C.; Soto-Alvaredo, J.; Montes-Bayon, M.; Bettmer, J.; Llopis, J.; Sanchez-Gonzalez, C. Gold nanoparticles: Distribution, bioaccumulation and toxicity. In vitro and in vivo studies. Nanomed. Nanotechnol. Biol. Med. 2018, 14, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Zhi, X.; Liu, Y.; Lin, L.; Yang, M.; Zhang, L.; Zhang, L.; Liu, Y.; Alfranca, G.; Ma, L.; Zhang, Q.; et al. Oral pH sensitive GNS@ab nanoprobes for targeted therapy of Helicobacter pylori without disturbance gut microbiome. Nanomedicine 2019, 20, 102019. [Google Scholar] [CrossRef] [PubMed]
- Cui, D.; Ma, L.; Zhi, X.; Zhang, C. Advance and Prospects of Nanotheranostic Technology for Gastric Cancer. Nano Biomed. Eng. 2016, 8, 219–239. [Google Scholar] [CrossRef]
- Milo, S.; Thet, N.T.; Liu, D.; Nzakizwanayo, J.; Jones, B.V.; Jenkins, A.T.A. An in-situ infection detection sensor coating for urinary catheters. Biosens. Bioelectron. 2016, 81, 166–172. [Google Scholar] [CrossRef]
- Chen, W.; Hazoor, S.; Madigan, R.; Adones, A.A.; Chintapula, U.K.; Nguyen, K.T.; Tang, L.; Foss, F.W.; Dong, H. Alkaline-responsive polydiacetylene-peptide hydrogel for pH-sensing and on-demand antimicrobial release. Mater. Today Adv. 2022, 16, 100288. [Google Scholar] [CrossRef]
- Mitragotri, S.; Stayton, P. Organic nanoparticles for drug delivery and imaging. MRS Bull 2014, 39, 219–223. [Google Scholar] [CrossRef]
- Mittal, R.; Pan, D.R.; Parrish, J.M.; Huang, E.H.; Yang, Y.; Patel, A.P.; Malhotra, A.K.; Mittal, J.; Chhibber, S.; Harjai, K. Local drug delivery in the urinary tract: Current challenges and opportunities. J. Drug Target 2018, 26, 658–669. [Google Scholar] [CrossRef]
- Fernandes, M.M.; Ivanova, K.; Francesko, A.; Mendoza, E.; Tzanov, T. Immobilization of antimicrobial core-shell nanospheres onto silicone for prevention of Escherichia coli biofilm formation. Process Biochem. 2017, 59, 116–122. [Google Scholar] [CrossRef]
- Francesko, A.; Fernandes, M.; Ivanova, K.; Amorim, S.; Reis, R.L.; Pashkuleva, I.; Mendoza, E.; Pfeifer, A.; Heinze, T.; Tzanov, T. Bacteria-responsive multilayer coatings comprising polycationic nanospheres for bacteria biofilm prevention on urinary catheters. Acta Biomater. 2016, 33, 203–212. [Google Scholar] [CrossRef]
- Lopes, L.Q.S.; de Almeida Vaucher, R.; Giongo, J.L.; Gündel, A.; Santos RC, V. Characterisation and anti-biofilm activity of glycerol monolaurate nanocapsules against Pseudomonas aeruginosa. Microbiol. Pathog. 2019, 130, 178–185. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; Khan, A.K.; Anwar, A.; Ali, S.A.; Shah, M.R. Biofilm inhibitory effect of chlorhexidine conjugated gold nanoparticles against Klebsiella pneumoniae. Microbiol. Pathog. 2016, 98, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Singh, I.; Swami, R.; Khan, W.; Sistla, R. Focal Controlled Drug Delivery; Delivery Systems for Lymphatic Targeting; Springer: Boston, MA, USA, 2013; pp. 429–458. [Google Scholar] [CrossRef] [PubMed]
- Cavalli, R.; Zara, G.P.; Caputo, O.; Bargoni, A.; Fundarò, A.; Gasco, M.R. Transmucosal transport of tobramycin incorporated in SLN after duodenal administration to rats. Part I—A pharmacokinetic study. Pharmacol. Res. 2000, 42, 541–545. [Google Scholar] [CrossRef] [PubMed]
- Bargoni, A.; Cavalli, R.; Caputo, O.; Fundarò, A.; Gasco, M.R.; Zara, G.P. Solid Lipid Nanoparticles in Lymph and Plasma After Duodenal Administration to Rats. Pharm. Res. 1998, 15, 745–750. [Google Scholar] [CrossRef]
- Zara, G.P.; Bargoni, A.; Cavalli, R.; Fundarò, A.; Vighetto, D.; Gasco, M.R. Pharmacokinetics and Tissue Distribution of Idarubicin-Loaded Solid Lipid Nanoparticles After Duodenal Administration to Rats. J. Pharm. Sci. 2002, 91, 1324–1333. [Google Scholar] [CrossRef]
- Kumanohoso, T.; Natsugoe, S.; Shimada, M.; Aikou, T. Enhancement of therapeutic efficacy of bleomycin by incorporation into biodegradable poly-d,l-lactic acid. Cancer Chemother. Pharmacol. 1997, 40, 112–116. [Google Scholar] [CrossRef]
- Liu, J.; Wong, H.-L.; Moselhy, J.; Bowen, B.; Wu, X.Y.; Johnston, M.R. Targeting colloidal particulates to thoracic lymph nodes. Lung Cancer 2006, 51, 377–386. [Google Scholar] [CrossRef]
- Kaur, C.D.; Nahar, M.; Jain, N.K. Lymphatic targeting of zidovudine using surface-engineered liposomes. J. Drug Target 2008, 16, 798–805. [Google Scholar] [CrossRef]
- Sheue Nee Ling, S.; Magosso, E.; Abdul Karim Khan, N.; Hay Yuen, K.; Anne Barker, S. Enhanced Oral Bioavailability and Intestinal Lymphatic Transport of a Hydrophilic Drug Using Liposomes. Drug Dev. Ind. Pharm. 2006, 32, 335–345. [Google Scholar] [CrossRef]
- Lockman, P.R.; Mumper, R.J.; Khan, M.A.; Allen, D.D. Nanoparticle technology for drug delivery across the blood-brain barrier. Drug Dev. Ind. Pharm. 2002, 28, 1–13. [Google Scholar] [CrossRef]
- Barbu, E.; Molnàr, É.; Tsibouklis, J.; Górecki, D.C. The potential for nanoparticle-based drug delivery to the brain: Overcoming the blood-brain barrier. Expert Opin. Drug Deliv. 2009, 6, 553–565. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Zhang, H.; Wu, Y. Dendrimer advances for the central nervous system delivery of therapeutics. ACS Chem. Neurosci. 2014, 5, 2–13. [Google Scholar] [CrossRef]
- Hwang, S.R.; Kim, K. Nano-enabled delivery systems across the blood-brain barrier. Arch. Pharm. Res. 2014, 37, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Biddlestone-Thorpe, L.; Marchi, N.; Guo, K.; Ghosh, C.; Janigro, D.; Valerie, K.; Yang, H. Nanomaterial-mediated CNS delivery of diagnostic and therapeutic agents. Adv Drug Deliv. Rev. 2012, 64, 605–613. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Li, X.; Zhang, L.-Y.; Song, Q.-R.; Zhang, M.; Zhao, C.-X.; Wang, J.; Sun, G.-T.; Liu, Z.-H. Stimuli-Responsive Nanocarriers for Drug Delivery to the Central Nervous System. Curr. Nanosci. 2015, 12, 4–17. [Google Scholar] [CrossRef]
- Perche, F.; Torchilin, V.P. Recent Trends in Multifunctional Liposomal Nanocarriers for Enhanced Tumor Targeting. J. Drug Deliv. 2013, 2013, 705265. [Google Scholar] [CrossRef]
- Ye, M.; Han, Q.-L.; Ding, L.; Xu, S. Fully distributed Nash equilibrium seeking for high-order players with actuator limitations. IEEE/CAA J. Autom. Sin. 2022, 1–11. [Google Scholar] [CrossRef]
- Torchilin, V.P. Tat peptide-mediated intracellular delivery of pharmaceutical nanocarriers. Adv. Drug Deliv. Rev. 2008, 60, 548–558. [Google Scholar] [CrossRef]
- Bartomeu Garcia, C.; Shi, D.; Webster, T.J. Tat-functionalized liposomes for the treatment of meningitis: An in vitro study. Int. J. Nanomed. Vol. 2017, 12, 3009–3021. [Google Scholar] [CrossRef]
- Hong, W.; Zhang, Z.; Liu, L.; Zhao, Y.; Zhang, D.; Liu, M. Brain-targeted delivery of PEGylated nano-bacitracin A against Penicillin-sensitive and -resistant Pneumococcal meningitis: Formulated with RVG29 and Pluronic® P85 unimers. Drug Deliv. 2018, 25, 1886–1897. [Google Scholar] [CrossRef]
- Shao, K.; Zhang, Y.; Ding, N.; Huang, S.; Wu, J.; Li, J.; Yang, C.; Leng, Q.; Ye, L.; Lou, J.; et al. Functionalized nanoscale micelles with brain targeting ability and intercellular microenvironment biosensitivity for anti-intracranial infection applications. Adv. Healthc. Mater. 2015, 4, 291–300. [Google Scholar] [CrossRef] [PubMed]
- Xu, K.; Wang, H.; Liu, L.; Xu, W.; Sheng, J.; Fan, W.; Yang, Y.-Y.; Li, L. Efficacy of CG3R6TAT nanoparticles self-assembled from a novel antimicrobial peptide for the treatment of candida albicans meningitis in rabbits. Chemotherapy 2012, 57, 417–425. [Google Scholar] [CrossRef] [PubMed]












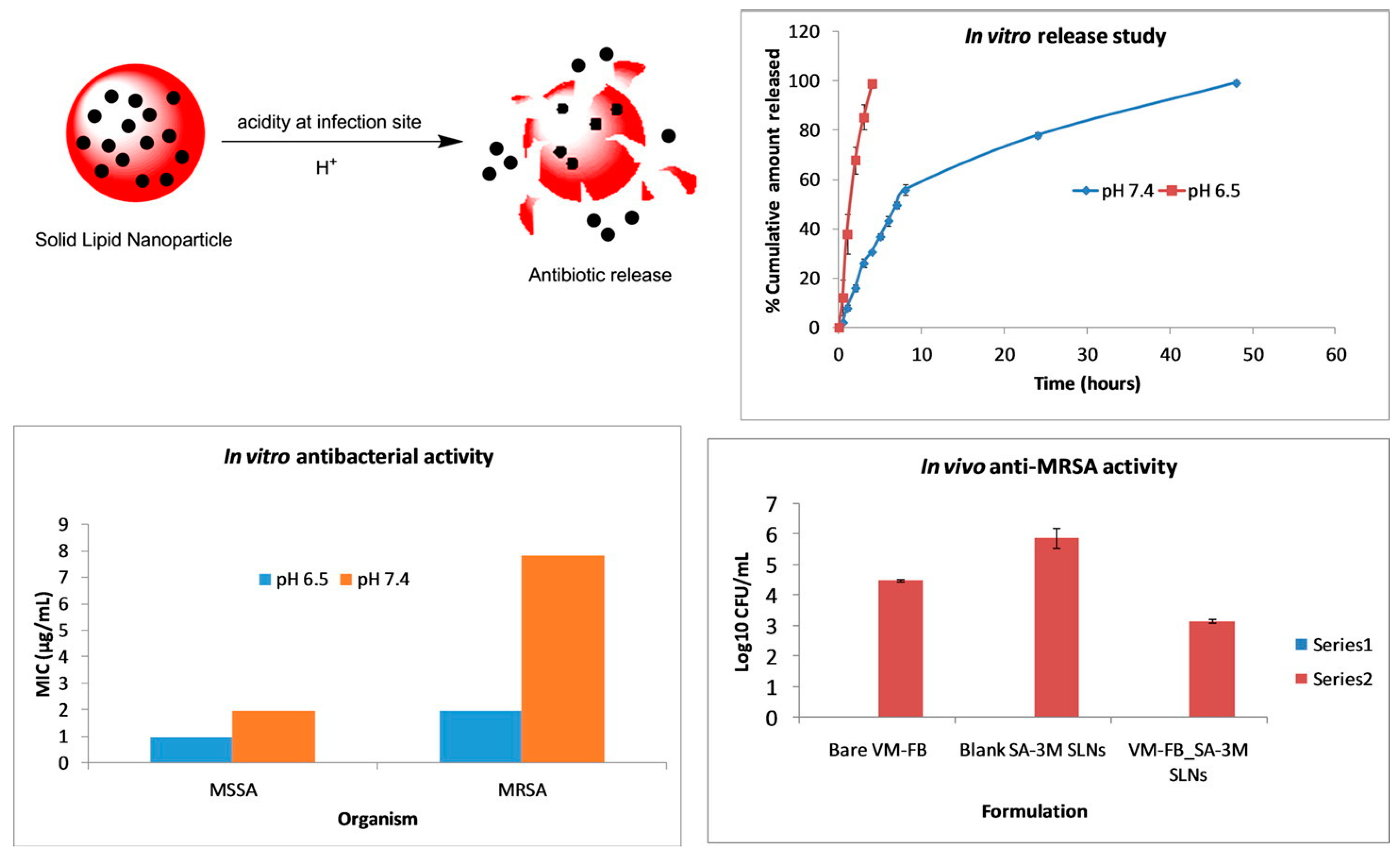{kind=link}
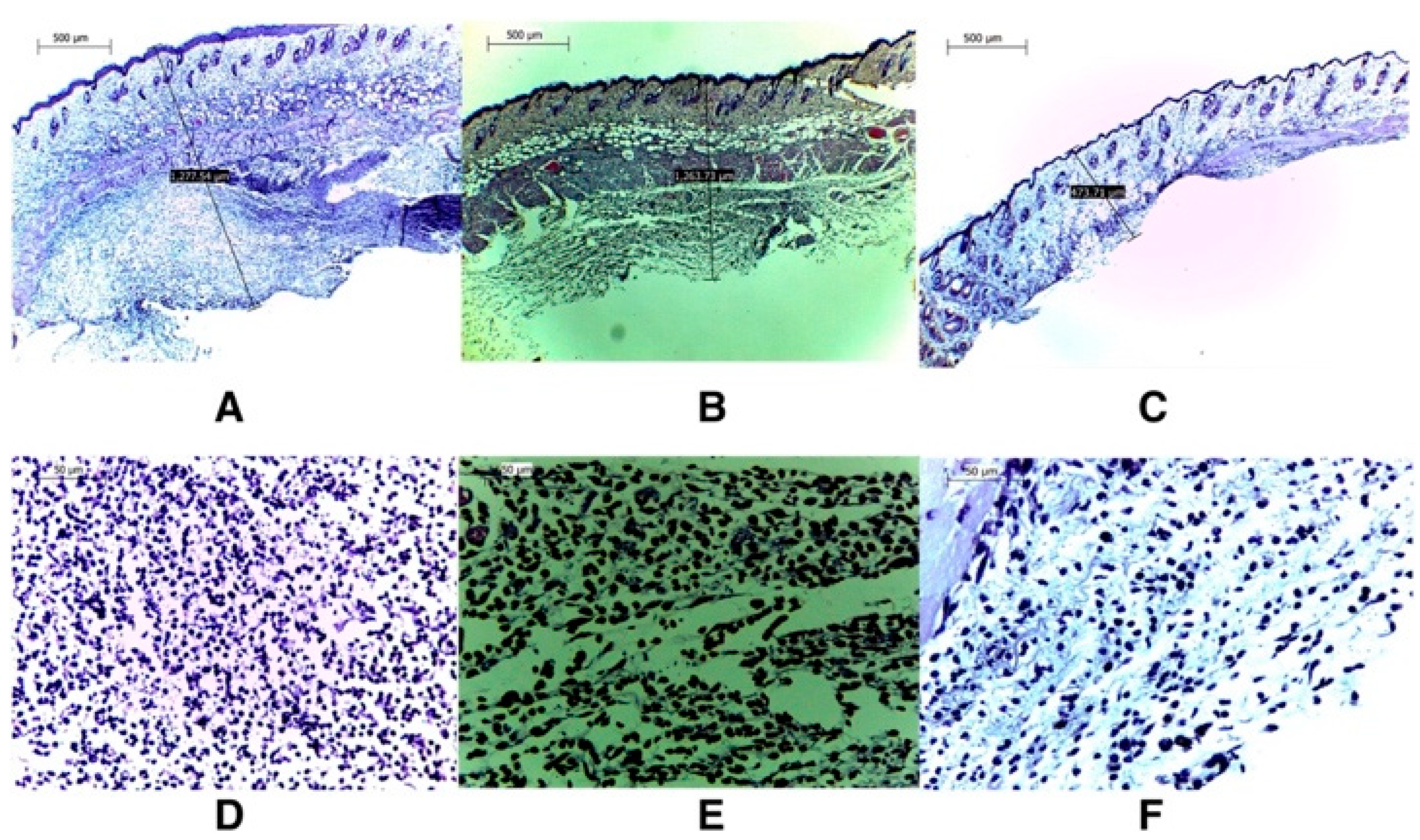{kind=link}
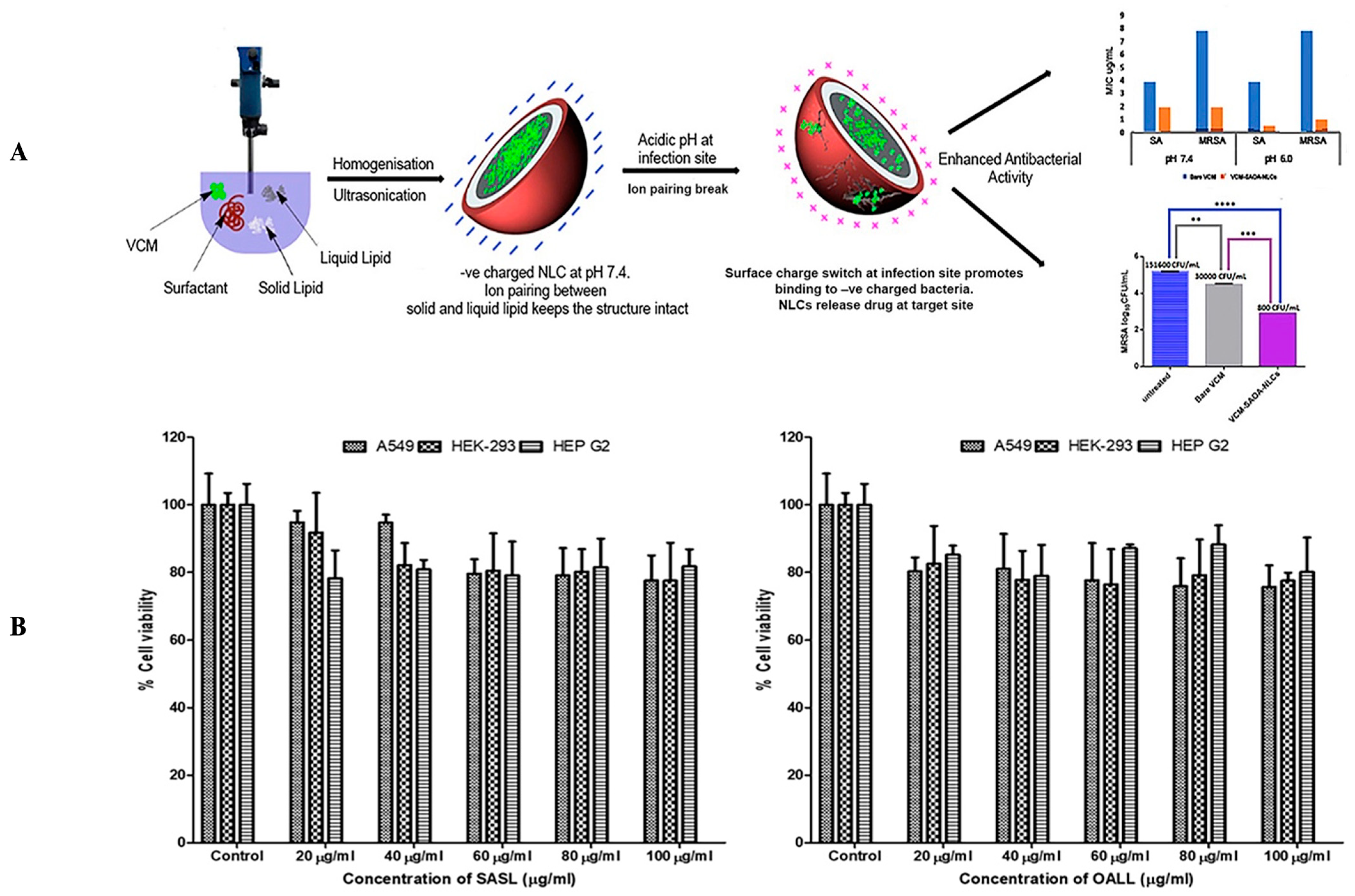{kind=link}
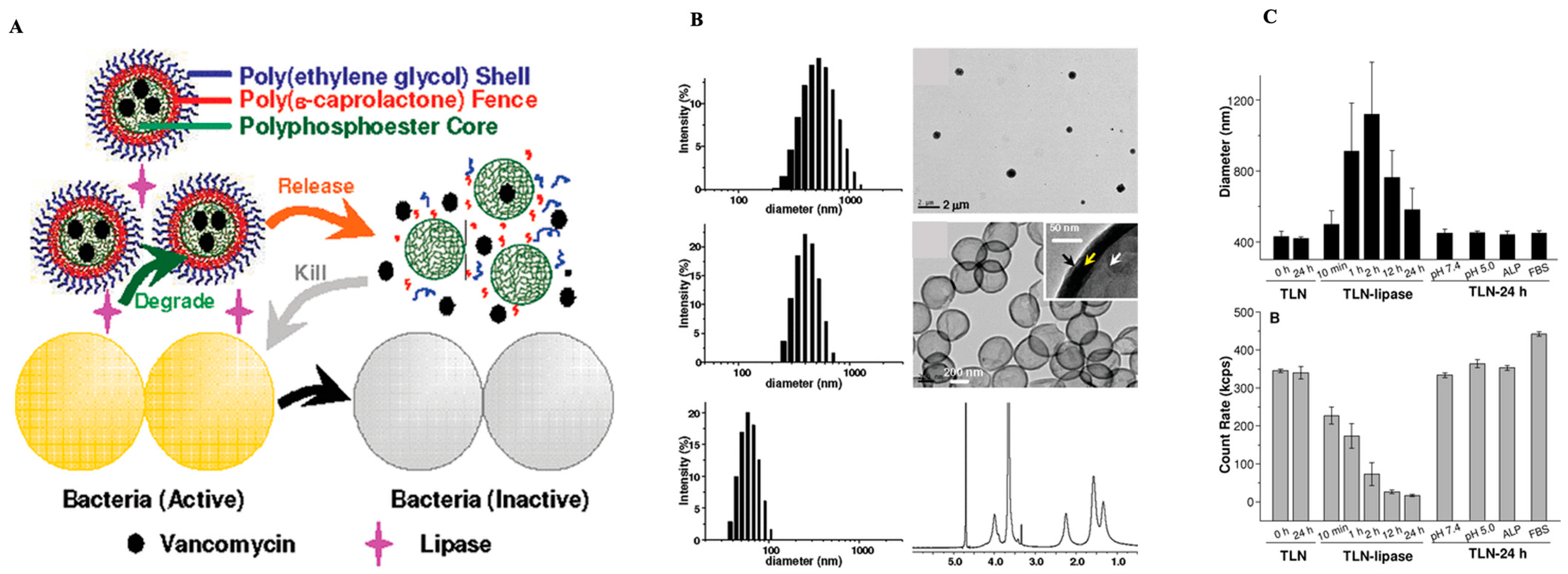{kind=link}
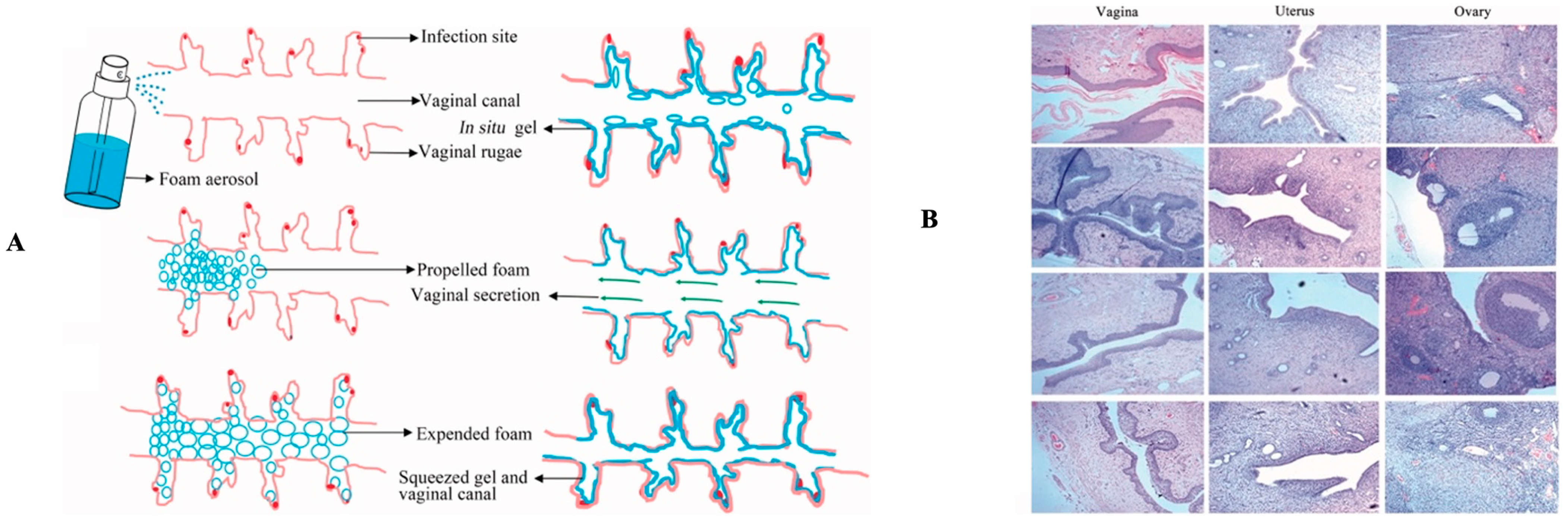{kind=link}
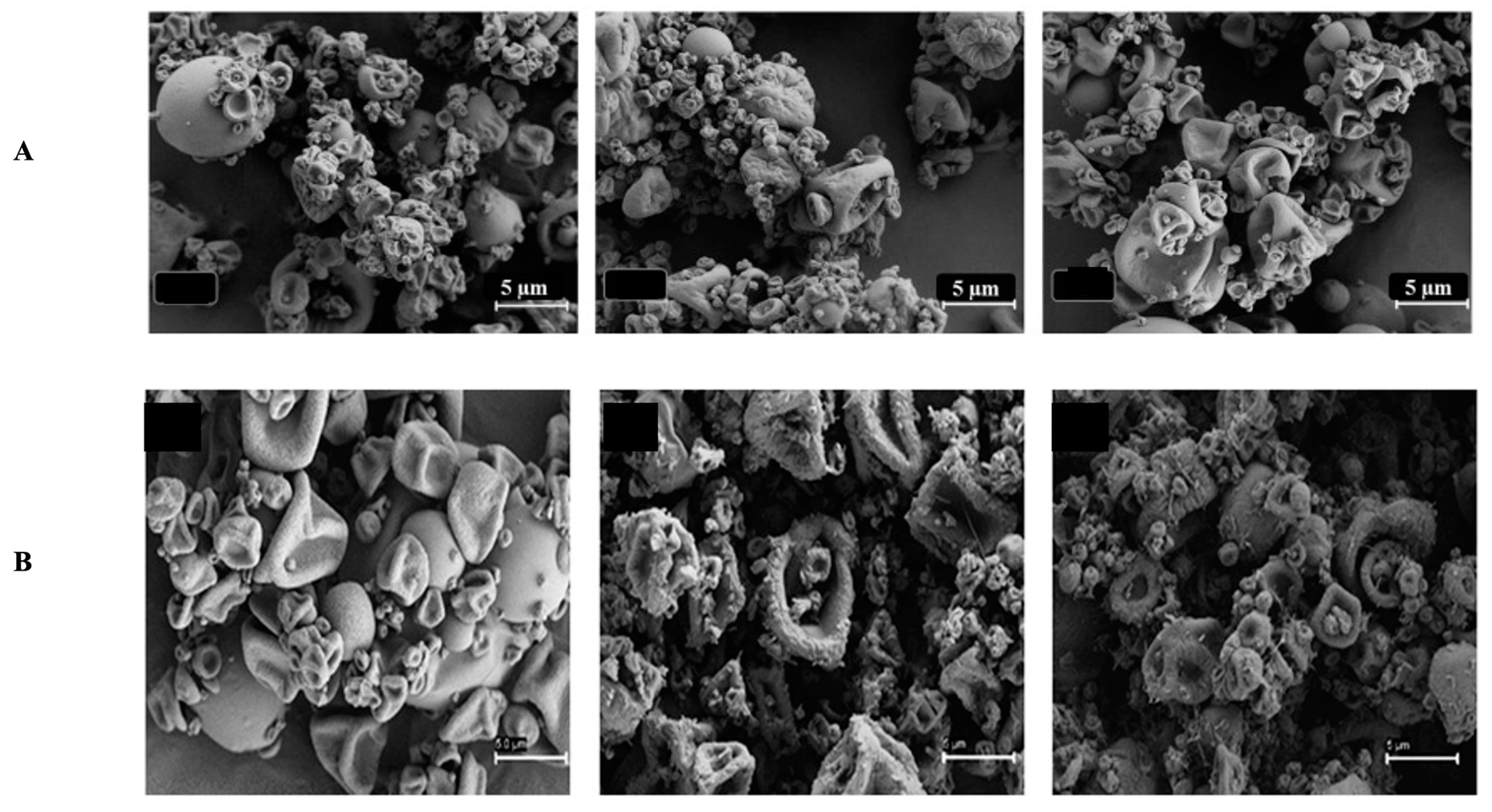{kind=link}
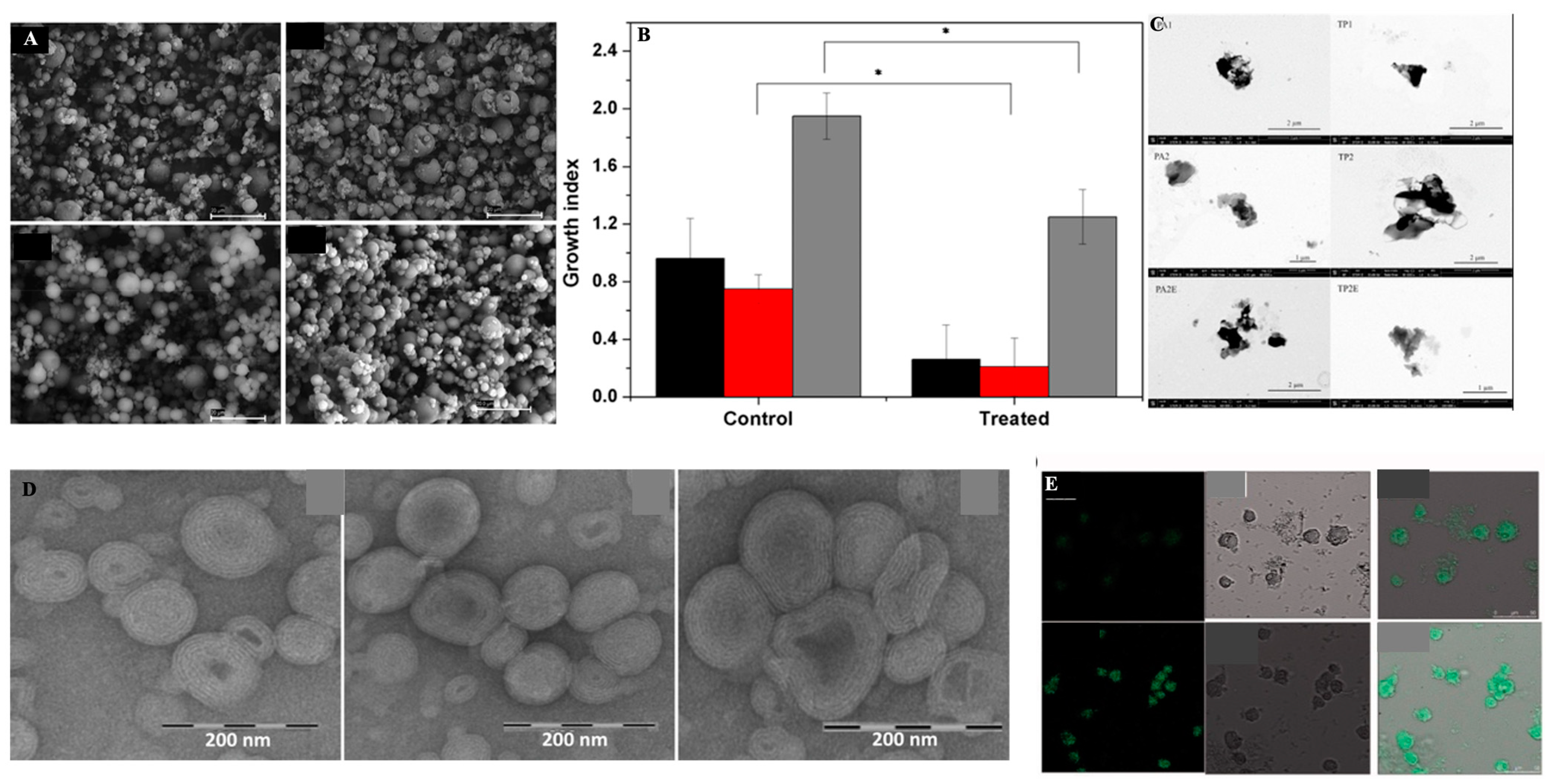{kind=link}
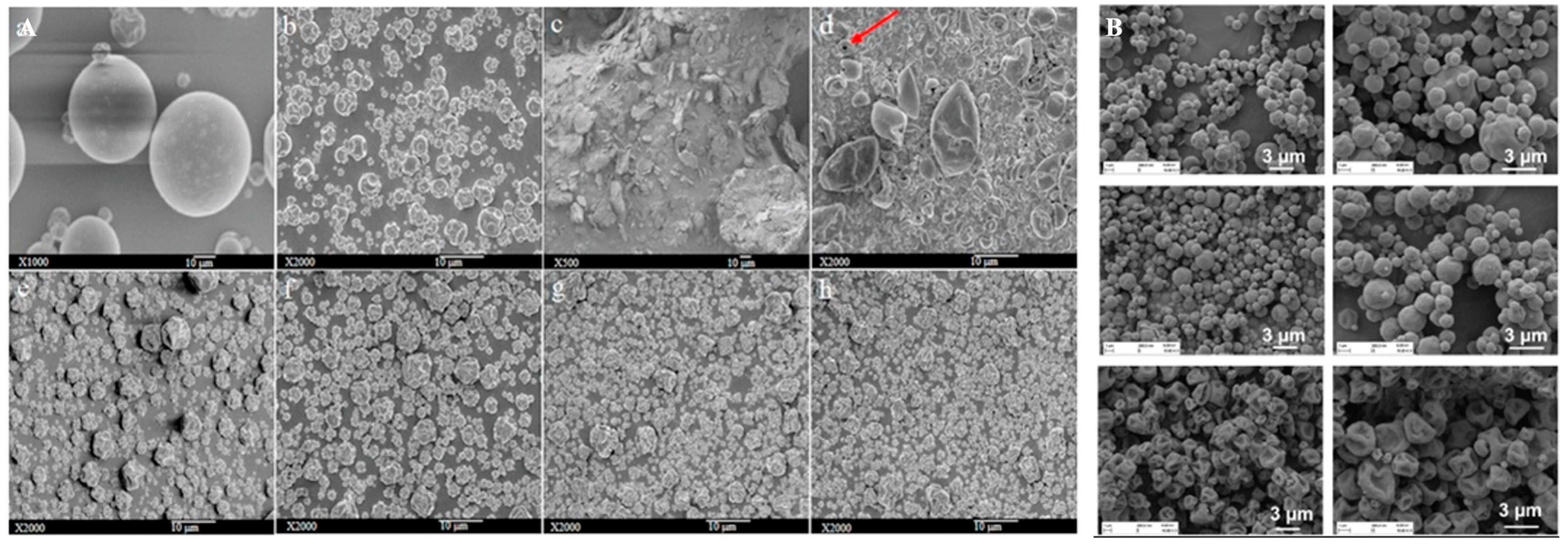{kind=link}
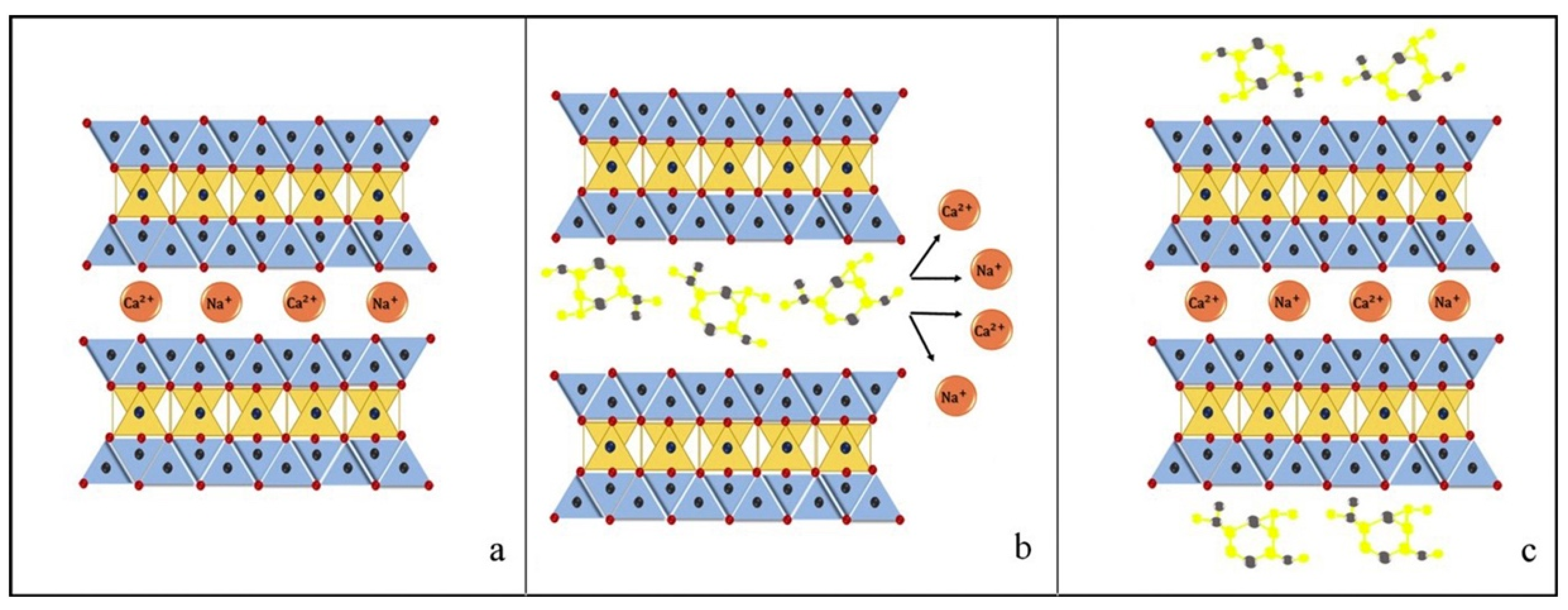{kind=link}
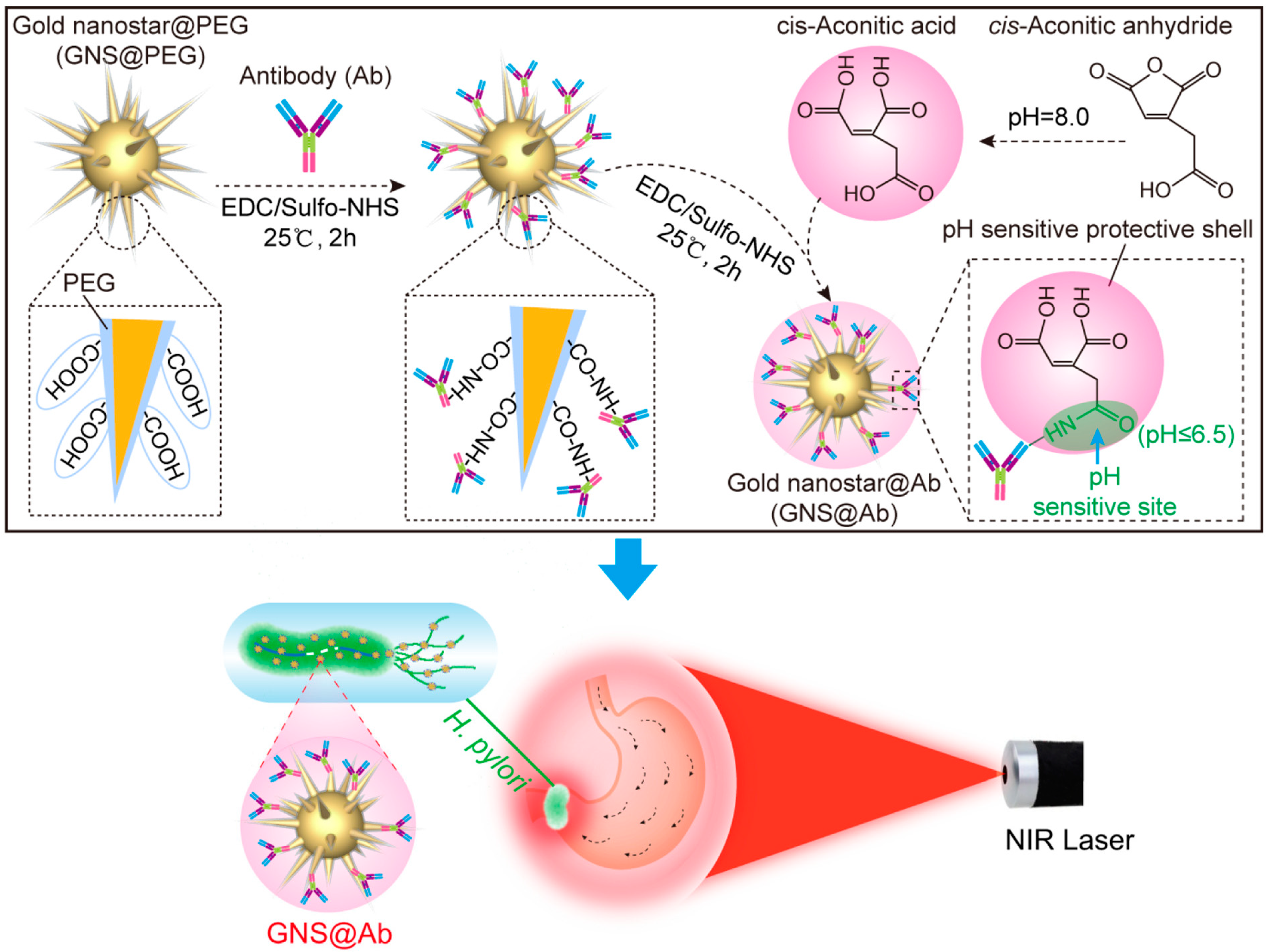{kind=link}
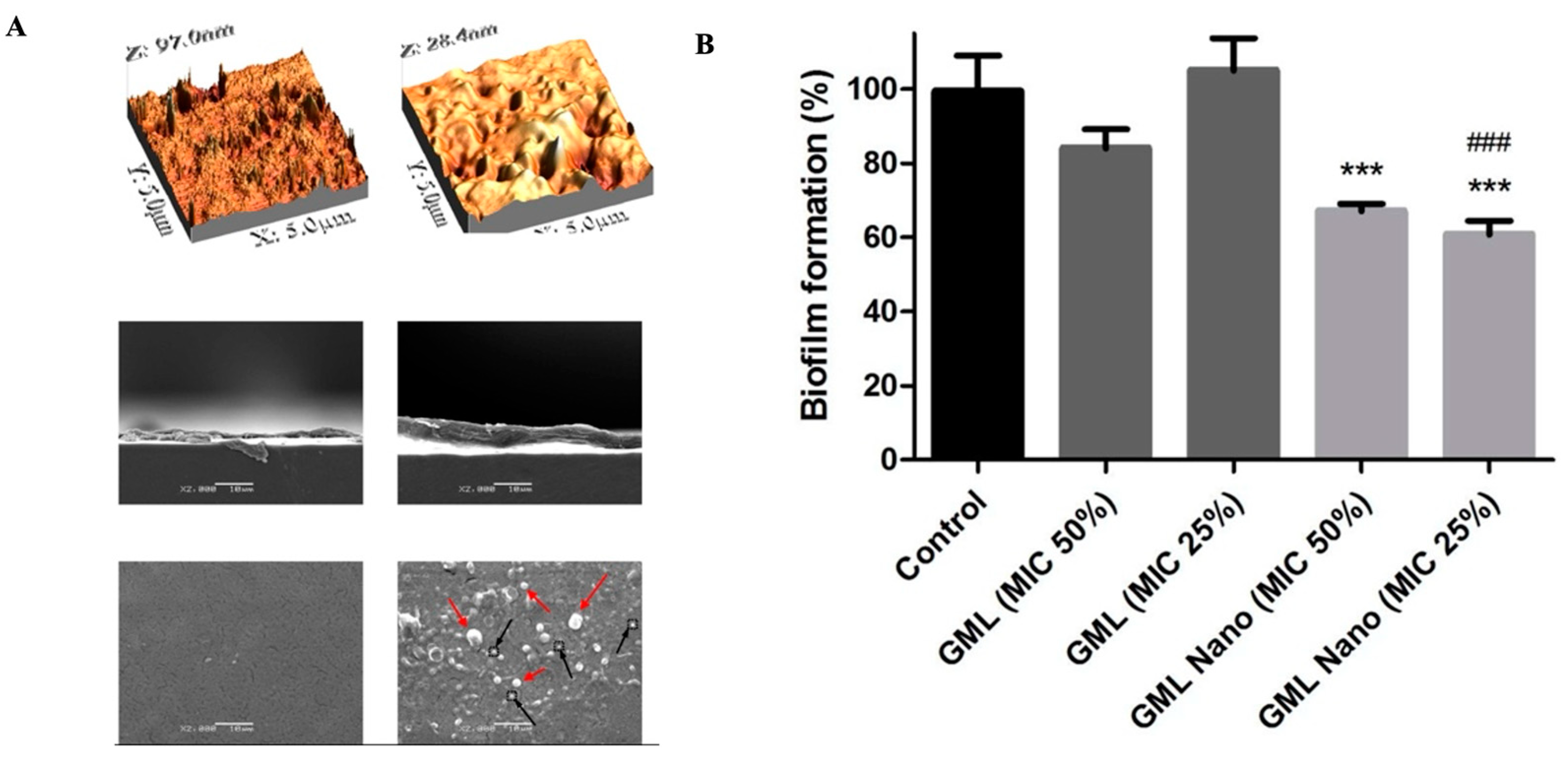{kind=link}
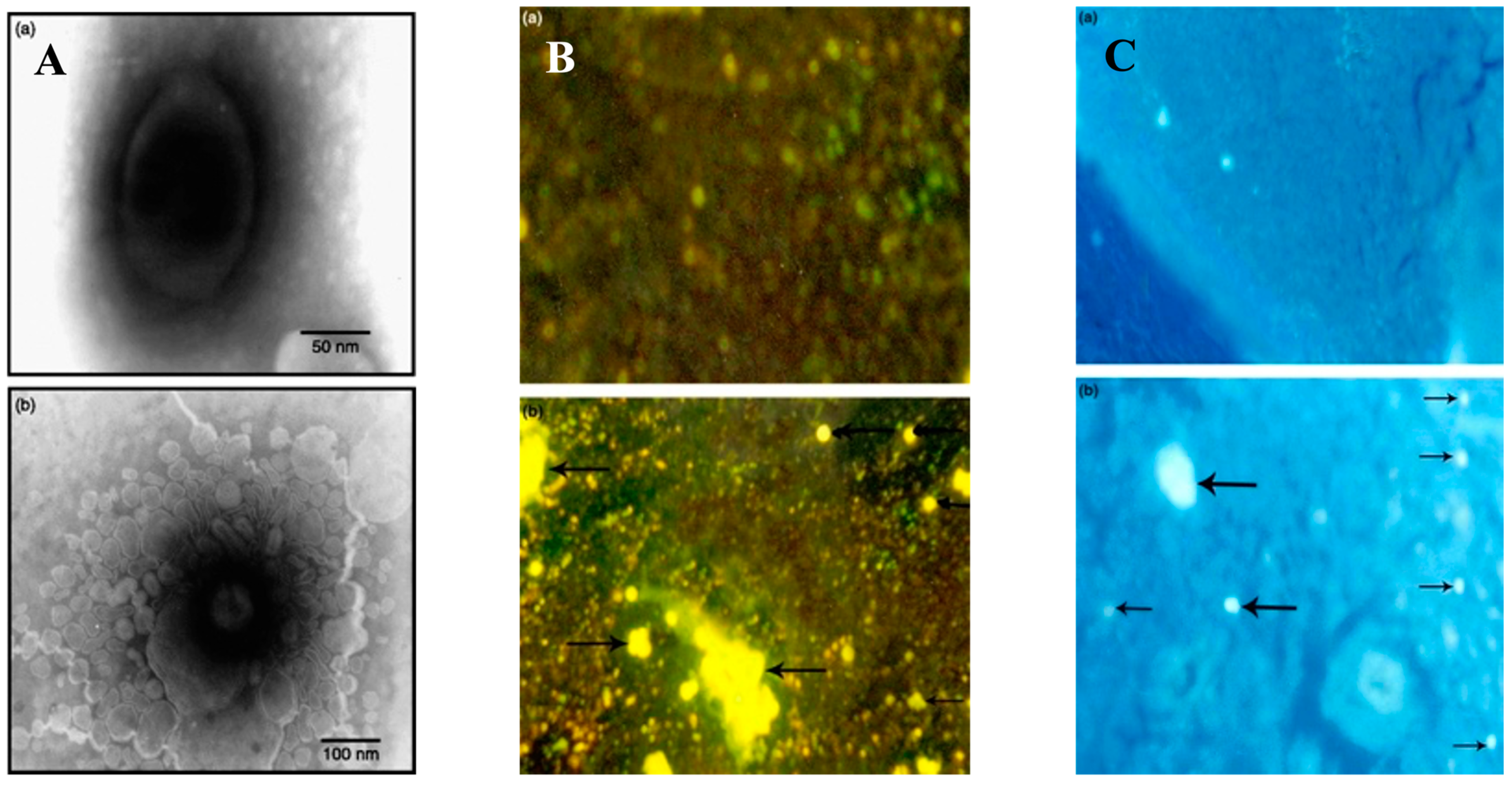{kind=link}
| The Location of Treatment | Causes of Infection | Treatment Options |
|---|---|---|
| Inpatient, Non-ICU | H. influenzae S. aureus S. pneumoniae | β-lactam plus macrolide: Cefotaxime IV/IM + Azithromycin oral Ceftriaxone IV/IM + Azithromycin oral Ampicillin IV/IM + Azithromycin oral Alternative to macrolide: Doxycycline oral Respiratory fluoroquinolone: Levofloxacin, Moxifloxacin, or Gemifloxacin |
| Inpatient, ICU | Legionella H. influenzae Gram-negative enteric organisms S. pneumoniae (including drug resistant) | β-lactam plus macrolide: Cefotaxime, Ceftriaxone, or Ampicillin-sulbactam IV/IM. Plus: Azithromycin or Levofloxacin IV Penicillin allergy: levofloxacin + aztreonam IV |
| Inpatient, ICU | Methicillin resistant S. aureus (MRSA) | β-lactam plus macrolide: Cefotaxime, Ceftriaxone, or Ampicillin-sulbactam IV/IM. Plus: Azithromycin or Levofloxacin IV Penicillin allergy: levofloxacin + aztreonam IV Plus: Vancomycin IV or Linezolid IV or oral |
| Inpatient/ICU | Pseudomonas aeruginosa, suspected | Anti-pseudomonal β-lactam: Piperacillin-tazobactam IV, Cefepime IV, Imipenem IV Plus, either: Ciprofloxacin IV, Levofloxacin IV Penicillin allergy: Aztreonam IV can be substituted for β-lactam |
| Cause of Infection | Antibiotic Treatment | Duration of Therapy |
|---|---|---|
| Streptococcus pneumoniae Penicillin-susceptible isolate | Adults: penicillin G or ampicillin IV. Children: penicillin G or ampicillin. Severe penicillin allergy: substitute cephalosporin agent with chloramphenicol. | 10–14 days |
| Neisseria meningitidis | Adults: penicillin G IV or ampicillin IV or ceftriaxone IV or cefotaxime IV. Penicillin allergy: substitute cephalosporin agent with chloramphenicol. Children: penicillin G IV. Penicillin allergy: substitute with chloramphenicol. | 7 days |
| Haemophilus influenza | Betalactamase positive: ceftriaxone IV or cefotaxime IV Betalactamase negative: Ampicillin IV | 7 days |
| Pseudomonas aeruginosa | Ceftazidime IV or cefepime IV plus gentamicin IV | 21 days |
| Group B Streptococcus Suspected/empiric | Preterm: ampicillin IV plus cefotaxime. Infants ≤7 days: ampicillin IV plus aminoglycoside Infants >7 days: ampicillin IV plus an aminoglycoside, Intraventricular treatment not recommended. | 14–21 days |
| Enterobacteriaceae | Ceftriaxone IV or cefotaxime IV plus gentamicin IV | 21 days |
| Listeria monocytogenes | Infants ≤7 days: ampicillin IV plus aminoglycoside, Infants >7 days: ampicillin IV plus aminoglycoside. Adults >50, alcoholism, or other risk factors: ampicillin IV plus ceftriaxone IV or cefotaxime IV plus gentamicin IV loading dose, then plus dexamethasone IV Penicillin allergy: trimethoprim/sulfamethoxazole | 21 days |
| Disease | Pathogen | Treatment |
|---|---|---|
| Bacillus cereus infection | Bacillus cereus | Rehydration and supportive therapy. Antibiotics are usually not needed. |
| Campylobacter jejuni gastroenteritis | Campylobacter jejuni | Antibiotics are usually not required, but erythromycin or ciprofloxacin may be used. |
| Cholera | Vibrio cholera | Antibiotics are usually not required, but tetracycline, azithromycin, and others may be used. |
| Clostridium difficile infection | Clostridium difficile | First, stop the use of antibiotics and provide supportive therapy with electrolyte and fluid replacement. Metronidazole or vancomycin may also be used. |
| Clostridium perfringens gastroenteritis | Clostridium perfringens (especially type A) | Rehydration therapy, electrolyte replacement, and intravenous fluids. Antibiotics are not recommended. |
| Escherichia coli (E. coli) infection | Enterotoxigenic E. coli (ETEC) | Self-limiting; if needed, fluoroquinolones, doxycycline, rifaximin, TMP/SMZ; antibiotic resistance is a problem. |
| Enteroinvasive E. coli (EIEC) | Supportive therapy only; antibiotics not recommended. | |
| Enteropathogenic E. coli (EPEC) | Self-limiting; if needed, fluoroquinolones, doxycycline, rifaximin (TMP/SMZ); antibiotic resistance is a problem. | |
| Enterohemorrhagic E. coli (EHEC) | Antibiotics are not recommended due to the risk of HUS. | |
| Peptic ulcers | Helicobacter pylori | Amoxicillin, clarithromycin, metronidazole, tetracycline, and lansoprazole. Antacids may also be given in combination with antibiotics. |
| Salmonellosis | Salmonella enterica, serotype Enteritides | Oral rehydration therapy. Antibiotics are only recommended for serious cases such as in immunocompromised patients; fluoroquinolones, third-generation cephalosporins, and ampicillin are recommended. |
| Shigella dysentry | Shigella dysenteriae, S. flexneri, S. boydii, and S. sonnei | Ciprofloxacin and azithromycin. |
| Staphylococcal food poisoning | Staphylococcus aureus | Without treatment this condition usually heals relatively quickly, within 24 h. |
| Typhoid fever | S. enterica, serotype Typhi or Paratyhphi | Fluoroquinolones, ceftriaxone, and azithromycin. Preventive vaccine available. |
| Yersinia infection | Y. enterocolitica and Y. pseudotuberculosis. | Supportive therapy such as rehydration without antibiotics. Fluoroquinolones, aminoglycosides, doxycycline, and trimethoprim-sulfamethoxazole may be used for systemic infections. |
| Disease | Pathogen | Treatment |
|---|---|---|
| Astrovirus gastroenteritis | Astrovirus | Supportive therapy such as rehydration and electrolyte replacement. |
| Norovirus gastroenteritis | Norovirus | Supportive therapy. |
| Rotavirus gastroenteritis | Rotavirus | Supportive therapy and vaccinations for babies. |
| Disease | Pathogen | Treatment |
|---|---|---|
| Amoebiasis (amoebic dysentery) | Entamoeba histolytica | Metronidazole, tinidazole, diloxanide furoate, iodoquinol, and paromomycin. |
| Cryptosporidiosis | Cryptosporidium parvum, Cryptosporidium hominis | Oral rehydration therapy and anti-parasitic drugs (nitazoxanide, azithromycin, and paromomycin). |
| Cyclosporiasis | Cyclospora cayetanensis | Trimethoprim-sulfamethoxazole. |
| Giardiasis | Giardia lamblia | Metronidazole and tinidazole. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marzaman, A.N.F.; Roska, T.P.; Sartini, S.; Utami, R.N.; Sulistiawati, S.; Enggi, C.K.; Manggau, M.A.; Rahman, L.; Shastri, V.P.; Permana, A.D. Recent Advances in Pharmaceutical Approaches of Antimicrobial Agents for Selective Delivery in Various Administration Routes. Antibiotics 2023, 12, 822. https://doi.org/10.3390/antibiotics12050822
Marzaman ANF, Roska TP, Sartini S, Utami RN, Sulistiawati S, Enggi CK, Manggau MA, Rahman L, Shastri VP, Permana AD. Recent Advances in Pharmaceutical Approaches of Antimicrobial Agents for Selective Delivery in Various Administration Routes. Antibiotics. 2023; 12(5):822. https://doi.org/10.3390/antibiotics12050822
Chicago/Turabian StyleMarzaman, Ardiyah Nurul Fitri, Tri Puspita Roska, Sartini Sartini, Rifka Nurul Utami, Sulistiawati Sulistiawati, Cindy Kristina Enggi, Marianti A. Manggau, Latifah Rahman, Venkatram Prasad Shastri, and Andi Dian Permana. 2023. "Recent Advances in Pharmaceutical Approaches of Antimicrobial Agents for Selective Delivery in Various Administration Routes" Antibiotics 12, no. 5: 822. https://doi.org/10.3390/antibiotics12050822
APA StyleMarzaman, A. N. F., Roska, T. P., Sartini, S., Utami, R. N., Sulistiawati, S., Enggi, C. K., Manggau, M. A., Rahman, L., Shastri, V. P., & Permana, A. D. (2023). Recent Advances in Pharmaceutical Approaches of Antimicrobial Agents for Selective Delivery in Various Administration Routes. Antibiotics, 12(5), 822. https://doi.org/10.3390/antibiotics12050822