


Antibiotic Misuse Behaviours of Older People: Confirmation of the Factor Structure of the Antibiotic Use Questionnaire

Abstract
1. Introduction
1.1. Driving Factors of Antibiotic Resistance
1.2. Public Health Literacy of AR and Prevalence of Antibiotic Use in Older Adults
1.3. Antibiotic Misuse and Stewardship in Older Adults
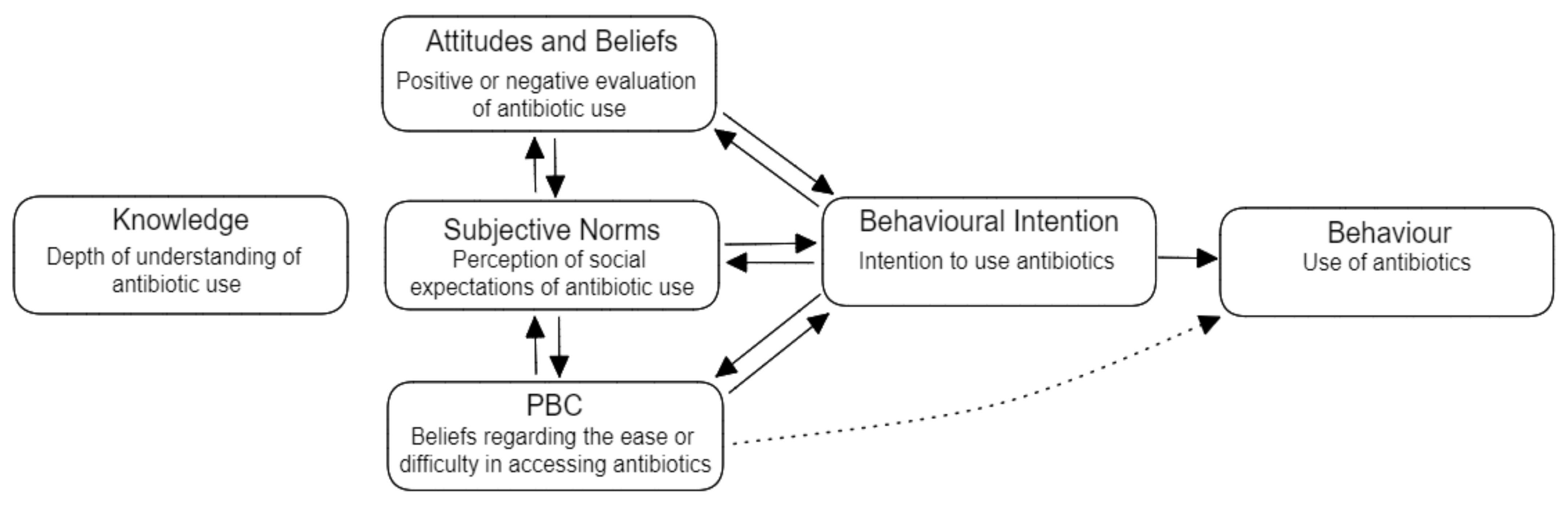
1.4. Theory of Planned Behaviour
1.5. Aim
2. Materials and Methods
2.1. Participants and Procedure
2.2. Measures
2.3. Statistical Analysis
3. Results
3.1. Initial Findings
3.2. CFA of the AUQ
3.3. Regression Analyses for the SDS, AUQ Factors and Behaviour
4. Discussion
4.1. Predictors of Antibiotic Misuse Behaviours
4.2. Comparison with Previous Research
4.3. Older Adults and TPB Factors
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Australian Commission on Safety and Quality in Health Care. Aura: Fourth Australian Report on Antimicrobial Use and Resistance in Human Health; Australian Government: Sydney, NSW, Australia, 2021.
- World Health Organisation. Antimocrobial Resistance Fact Sheet; World Health Organisation: Geneva, Switzerland, 2021. [Google Scholar]
- World Health Organisation. Tracss Country Report on the Implementation of National Action Plan on Antimicrobial Resistance (AMR): Australia; World Health Organisation: Geneva, Switzerland, 2021. [Google Scholar]
- Byrne, M.K.; Miellet, S.; McGlinn, A.; Fish, J.; Meedya, S.; Reynolds, N.; van Oijen, A.M. The drivers of antibiotic use and misuse: The development and investigation of a theory driven community measure. BMC Public Health 2019, 19, 1425. [Google Scholar] [CrossRef]
- Van-Driel, M.; Gregory, M.; Emma, B.; Jonathan, D.; Lisa, H.; Clare, H. Preserving antibiotics for the future. Aust. J. Gen. Pract. 2022, 51, 10–13. [Google Scholar] [CrossRef] [PubMed]
- Kong, L.S.; Islahudin, F.; Muthupalaniappen, L.; Chong, W.W. Knowledge and expectations on antibiotic use among older adults in Malaysia: A cross-sectional survey. Geriatrics 2019, 4, 61. [Google Scholar] [CrossRef] [PubMed]
- Guo, H.; Hildon, Z.J.-L.; Lye, D.C.B.; Straughan, P.T.; Chow, A. The associations between poor antibiotic and antimicrobial resistance knowledge and inappropriate antibiotic use in the general population are modified by age. Antibiotics 2022, 11, 47. [Google Scholar] [CrossRef] [PubMed]
- Department of Health and Agriculture. Australia’s national antimicrobial resistance strategy—2020 and beyond. In Agriculture DoHa; Commonwealth of Australia: Canberra, ACT, Australia, 2019. [Google Scholar]
- Anderson, R.; Rhodes, A.; Cranswick, N.; Downes, M.; O’Hara, J.; Measey, M.-A.; Gwee, A. A nationwide parent survey of antibiotic use in Australian children. J. Antimicrob. Chemother. 2020, 75, 1347–1351. [Google Scholar] [CrossRef]
- Hawkins, O.; Scott, A.M.; Montgomery, A.; Nicholas, B.; Mullan, J.; van Oijen, A.; Degeling, C. Comparing public attitudes, knowledge, beliefs and behaviours towards antibiotics and antimicrobial resistance in Australia, United Kingdom, and Sweden (2010-2021): A systematic review, meta-analysis, and comparative policy analysis. PLoS ONE 2022, 17, 110–123. [Google Scholar] [CrossRef]
- World Health Organisation. WHO Essential Medicines List Antibiotic Book—Infographics—Version 1.1; World Health Organisation: Geneva, Switzerland, 2021; pp. 1–141. [Google Scholar]
- Liu, C.; Wang, D.; Liu, C.; Jiang, J.; Wang, X.; Chen, H.; Ju, X.; Zhang, X. What is the meaning of health literacy? A systematic review and qualitative synthesis. Fam. Med. Community Health 2020, 8, 251–264. [Google Scholar] [CrossRef]
- Grigoryan, L.; Germanos, G.; Zoorob, R.; Juneja, S.; Raphael, J.; Paasche-Orlow, M.; Trautner, B. Use of antibiotics without a prescription in the U.S. population. Ann. Intern. Med. 2019, 171, 257–263. [Google Scholar] [CrossRef]
- Smith, C.A.; Chang, E.; Gallego, G.; Khan, A.; Armour, M.; Balneaves, L.G. An education intervention to improve decision making and health literacy among older Australians: A randomised controlled trial. BMC Geriatr. 2019, 19, 129–140. [Google Scholar] [CrossRef]
- Machowska, A.; Stålsby-Lundborg, C. Drivers of Irrational Use of Antibiotics in Europe. Int. J. Environ. Res. Public Health 2019, 16, 27. [Google Scholar] [CrossRef]
- Cattaneo, D.; Falcone, M.; Gervasoni, C.; Marriott, D.J.E. Therapeutic drug monitoring of antibiotics in the elderly: A narrative review. Ther. Drug Monit. 2022, 44, 75–85. [Google Scholar] [CrossRef]
- Dylis, A.; Boureau, A.S.; Coutant, A.; Batard, E.; Javaudin, F.; Berrut, G.; de Decker, L.; Chapelet, G. Antibiotics prescription and guidelines adherence in elderly: Impact of the comorbidities. BMC Geriatr. 2019, 19, 291. [Google Scholar] [CrossRef]
- Cox, S.; Lo-A-Foe, K.; van Hoof, M.; Dinant, G.-J.; Oudhuis, G.; Savelkoul, P.; Cals, J.; de Bont, E. Physician-targeted interventions in antibiotic prescribing for urinary tract infections in general practice: A systematic review. Antibiotics 2022, 11, 1560. [Google Scholar] [CrossRef]
- Gajdács, M.; Ábrók, M.; Lázár, A.; Burián, K. Urinary tract infections in elderly patients: A 10-year study on their epidemiology and antibiotic resistance based on the WHO Access, Watch and Reserve (AWaRe) classification. Antibiotics 2021, 10, 1098. [Google Scholar] [CrossRef] [PubMed]
- Malani, P.; Solway, E.; Kirch, M.; Singer, D.C.; Kullgren, J.T. Use and perceptions of antibiotics among US adults aged 50–80 years. Infect. Control Hosp. Epidemiol. 2021, 42, 628–629. [Google Scholar] [CrossRef] [PubMed]
- Manafo, E.; Wong, S. Health literacy programs for older adults: A systematic literature review. Health Educ. Res. 2012, 27, 947–960. [Google Scholar] [CrossRef] [PubMed]
- Beckett, C.L.; Harbarth, S.; Huttner, B. Special considerations of antibiotic prescription in the geriatric population. Clin. Microbiol. Infect. 2015, 21, 3–9. [Google Scholar] [CrossRef]
- Raban, M.Z.; Gates, P.J.; Gasparini, C.; Westbrook, J.I. Temporal and regional trends of antibiotic use in long-term aged care facilities across 39 countries, 1985-2019: Systematic review and meta-analysis. PLoS ONE 2021, 16, 225–234. [Google Scholar] [CrossRef]
- O’Neill, J. Tackling Drug-Resistant Infections Globally: Final Report and Recommendations; Government of the United Kingdom: London, UK, 2016.
- Merlino, J.; Siarakas, S. Antibiotic prescribing and antimicrobial resistance from an Australian perspective. Microb. Drug Resist. 2022, 1, 10–22. [Google Scholar] [CrossRef]
- Morgan, D.J.; Okeke, I.N.; Laxminarayan, R.; Perencevich, E.N.; Weisenberg, S. Non-prescription antimicrobial use worldwide: A systematic review. Lancet Infect. Dis. 2011, 11, 692–701. [Google Scholar] [CrossRef]
- Sun, R.; Yao, T.; Zhou, X.; Harbarth, S.; Lin, L. Non-biomedical factors affecting antibiotic use in the community: A mixed-methods systematic review and meta-analysis. Clin. Microbiol. Infect. 2022, 28, 345–354. [Google Scholar] [CrossRef] [PubMed]
- Peters, L.; Greenfield, G.; Majeed, A.; Hayhoe, B. The impact of private online video consulting in primary care. J. R. Soc. Med. 2018, 111, 162–166. [Google Scholar] [CrossRef]
- Han, S.M.; Greenfield, G.; Majeed, A.; Hayhoe, B. Impact of remote consultations on antibiotic prescribing in primary health care: Systematic review. J. Med. Internet Res. 2020, 22, 234–352. [Google Scholar] [CrossRef] [PubMed]
- Hensey, C.C.; Gwee, A. Counterfeit drugs: An Australian perspective. Med. J. Aust. 2016, 204, 344–353. [Google Scholar] [CrossRef] [PubMed]
- Hope, D.L.; Woods, P.; Mey, A.; Kelly, F.S.; Townshend, J.; Baumann-Birkbeck, L.M.; King, M.A. Australian pharmacists: Ready for increased non-prescription medicines reclassification. Int. J. Pharm. Pract. 2020, 28, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Mortazavi, S.S.; Shati, M.; Khankeh, H.R.; Ahmadi, F.; Mehravaran, S.; Malakouti, S.K. Self-medication among the elderly in Iran: A content analysis study. BMC Geriatr. 2017, 17, 198. [Google Scholar] [CrossRef]
- Ajzen, I. The theory of planned behaviour: Frequently asked questions. Hum. Behav. Emerg. Technol. 2020, 2, 314–324. [Google Scholar] [CrossRef]
- Ajzen, I. The theory of planned behaviour: Reactions and reflections. Psychol. Health 2011, 26, 1113–1127. [Google Scholar] [CrossRef]
- Ajzen, I. The theory of planned behaviour. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- La Barbera, F.; Ajzen, I. Control interactions in the theory of planned behavior: Rethinking the role of subjective norm. Eur. J. Psychol. 2020, 16, 401–417. [Google Scholar] [CrossRef]
- Evans, I.E.M.; Martyr, A.; Collins, R.; Brayne, C.; Clare, L. Social isolation and cognitive function in later life: A systematic review and meta-analysis. J. Alzheimer’s Dis. 2019, 70, 119–144. [Google Scholar] [CrossRef] [PubMed]
- Gillis, C.; Mirzaei, F.; Potashman, M.; Ikram, M.A.; Maserejian, N. The incidence of mild cognitive impairment: A systematic review and data synthesis. Alzheimer’s Dement. Diagn. Assess. Dis. Monit. 2019, 11, 248–256. [Google Scholar] [CrossRef] [PubMed]
- John, A.; Patel, U.; Rusted, J.; Richards, M.; Gaysina, D. Affective problems and decline in cognitive state in older adults: A systematic review and meta-analysis. Psychol. Med. 2019, 49, 353–365. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022; Available online: https://www.R-project.org/ (accessed on 19 January 2023).
- Project, T.J. Jamovi (Version 2.3.9.0) 2022. Available online: https://www.jamovi.org (accessed on 19 January 2023).
- Reynolds, W.M. Development of reliable and valid short forms of the Marlowe-Crowne social desirability scale. J. Clin. Psychol. 1982, 38, 119–125. [Google Scholar] [CrossRef]
- Kline, R.; Williams, M.; Vogt, W. Convergence of structural equation modeling and multilevel modeling. In The SAGE Handbook of Innovation in Social Research Methods; Sage Publications Ltd.: London, UK, 2011; pp. 562–603. [Google Scholar]
- Palin, V.; Mölter, A.; Belmonte, M.; Ashcroft, D.M.; White, A.; Welfare, W.; van Staa, T. Antibiotic prescribing for common infections in UK general practice: Variability and drivers. J. Antimicrob. Chemother. 2019, 74, 2440–2450. [Google Scholar] [CrossRef]
- Schröder, W.; Sommer, H.; Gladstone, B.P.; Foschi, F.; Hellman, J.; Evengard, B.; Tacconelli, E. Gender differences in antibiotic prescribing in the community: A systematic review and meta-analysis. J. Antimicrob. Chemother. 2016, 71, 1800–1806. [Google Scholar] [CrossRef] [PubMed]
- Scaioli, G.; Gualano, M.R.; Gili, R.; Masucci, S.; Bert, F.; Siliquini, R. Antibiotic use: A cross-sectional survey assessing the knowledge, attitudes and practices amongst students of a school of medicine in Italy. PLoS ONE 2015, 10, 122–139. [Google Scholar] [CrossRef]
- Fine, L.; Weinborn, M.; Ng, A.; Loft, S.; Li, Y.R.; Hodgson, E.; Parker, D.; Smith, S.R.; Sohrabi, H.R.; Brown, B.; et al. Sleep disruption explains age-related prospective memory deficits: Implications for cognitive aging and intervention. Aging Neuropsychol. Cogn. 2019, 26, 621–636. [Google Scholar] [CrossRef]
- Lawrence, B.J.; Jayakody, D.M.P.; Bennett, R.J.; Eikelboom, R.H.; Gasson, N.; Friedland, P.L. Hearing loss and depression in older adults: A systematic review and meta-analysis. Gerontologist 2019, 60, 137–154. [Google Scholar] [CrossRef]
- Scholes, G. Protein-energy malnutrition in older Australians: A narrative review of the prevalence, causes and consequences of malnutrition, and strategies for prevention. Health Promot. J. Aust. 2022, 33, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Lau, E.T.L.; Steadman, K.J.; Cichero, J.A.Y.; Nissen, L.M. Dosage form modification and oral drug delivery in older people. Adv. Drug Deliv. Rev. 2018, 135, 75–84. [Google Scholar] [CrossRef]
- Hu, T.; Zhao, X.; Wu, M.; Li, Z.; Luo, L.; Yang, C.; Yang, F. Prevalence of depression in older adults: A systematic review and meta-analysis. Psychiatry Res. 2022, 311, 114–125. [Google Scholar] [CrossRef]
- Lyons, A.; Alba, B.; Heywood, W.; Fileborn, B.; Minichiello, V.; Barrett, C.; Hinchliff, S.; Malta, S.; Dow, B. Experiences of ageism and the mental health of older adults. Aging Ment. Health 2018, 22, 1456–1464. [Google Scholar] [CrossRef]
- Sussman, R.; Gifford, R. Causality in the theory of planned behavior. Personal. Soc. Psychol. Bull. 2019, 45, 920–933. [Google Scholar] [CrossRef]
- Castanier, C.; Deroche, T.; Woodman, T. Theory of planned behaviour and road violations: The moderating influence of perceived behavioural control. Transp. Res. Part F Traffic Psychol. Behav. 2013, 18, 148–158. [Google Scholar] [CrossRef]
- Poirier, G.; Ohayon, A.; Juranville, A.; Mourey, F.; Gaveau, J. Deterioration, compensation and motor control processes in healthy aging, mild cognitive impairment and Alzheimer’s disease. Geriatrics 2021, 6, 33. [Google Scholar] [CrossRef] [PubMed]
- Wildenbos, G.A.; Peute, L.; Jaspers, M. Aging barriers influencing mobile health usability for older adults: A literature based framework (MOLD-US). Int. J. Med. Inform. 2018, 114, 66–75. [Google Scholar] [CrossRef] [PubMed]
- Lanz, L.; Thielmann, I.; Gerpott, F.H. Are social desirability scales desirable? A meta-analytic test of the validity of social desirability scales in the context of prosocial behavior. J. Personal. 2022, 90, 203–221. [Google Scholar] [CrossRef] [PubMed]
- Chou, M.-Y.; Nishita, Y.; Nakagawa, T.; Tange, C.; Tomida, M.; Shimokata, H.; Otsuka, R.; Chen, L.-K.; Arai, H. Role of gait speed and grip strength in predicting 10-year cognitive decline among community-dwelling older people. BMC Geriatr. 2019, 19, 186. [Google Scholar] [CrossRef] [PubMed]
- Holcombe, A.O.; Kovacs, M.; Aust, F.; Aczel, B. Documenting contributions to scholarly articles using CRediT and tenzing. PLoS ONE 2020, 15, e0244611. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Survey Platform | N | Mean | SD | T-Statistic | p-Value | |
|---|---|---|---|---|---|---|
| Education | In-Person | 79 | 3.49 | 1.395 | −9.69 | <0.001 |
| M-Turk | 85 | 5.19 | 0.779 | |||
| Healthcare Training | In-Person | 79 | 1.80 | 0.404 | 10.09 | <0.001 |
| M-Turk | 85 | 1.18 | 0.383 | |||
| Healthcare Worker in Family | In-Person | 79 | 1.47 | 0.502 | 5.61 | <0.001 |
| M-Turk | 85 | 1.11 | 0.310 | |||
| Age | In-Person | 79 | 76.65 | 4.139 | 8.90 | <0.001 |
| M-Turk | 85 | 72.09 | 2.175 |
| Statistic | p | ||
|---|---|---|---|
| Q1. Abs Reduce Cold Symptoms | Mann-Whitney U | 3275 | 0.760 |
| Q2. Friends & Family Follow AB Recommendations | Mann-Whitney U | 824 | <0.001 |
| Q3. Abs Are Needed for Colds | Mann-Whitney U | 3350 | 0.978 |
| Q4. Abs Can Have Negative Side Effects | Mann-Whitney U | 855 | <0.001 |
| Q5. I Use Abs Without Dr. Consultation | Mann-Whitney U | 3162 | 0.490 |
| Q6. I Use Leftover Abs | Mann-Whitney U | 3217 | 0.619 |
| Q7. It’s My Right to Ask for ABs | Mann-Whitney U | 819 | <0.001 |
| Q8. Friends & Family | Mann-Whitney U | 1037 | <0.001 |
| Q.9 Know When I Need AB’s | Mann-Whitney U | 2158 | <0.001 |
| Q10. Use of ABs Without Prescription is Common | Mann-Whitney U | 1952 | <0.001 |
| Q11. Confident to Ask for AB’s | Mann-Whitney U | 995 | <0.001 |
| Q12. Abs Will be Less Effective in Future | Mann-Whitney U | 970 | <0.001 |
| Q13. I Consult Dr. Prior to Taking ABs | Mann-Whitney U | 417 | <0.001 |
| Q14. I Keep Leftover ABs | Mann-Whitney U | 2878 | 0.090 |
| Q15. Easily Get Abs from Dr. | Mann-Whitney U | 1465 | <0.001 |
| Q16. Easily Get Abs Online | Mann-Whitney U | 2717 | 0.018 |
| Q17. Easily Get Abs Family | Mann-Whitney U | 3147 | 0.438 |
| Q18. Expect Abs from Dr. | Mann-Whitney U | 2553 | 0.004 |
| Self-Completed or Had Help | Mean | SD | |
|---|---|---|---|
| Gender | Self-Completed | 1.67 | 0.482 |
| Had Help | 1.57 | 0.535 | |
| Education | Self-Completed | 3.71 | 1.654 |
| Had Help | 2.57 | 0.976 | |
| Age | Self-Completed | 78.17 | 3.435 |
| Had Help | 80.43 | 5.593 | |
| Health Training | Self-Completed | 1.83 | 0.387 |
| Had Help | 1.86 | 0.378 | |
| Health Worker in Family | Self-Completed | 1.50 | 0.511 |
| Had Help | 1.71 | 0.488 | |
| Behaviour | Self-Completed | 2.14 | 0.410 |
| Had Help | 2.54 | 0.419 | |
| Social Desirability Scale | Self-Completed | 5.13 | 0.338 |
| Had Help | 5.00 | 0.000 | |
| Knowledge | Self-Completed | 2.58 | 0.319 |
| Had Help | 2.64 | 0.378 | |
| Attitudes and Beliefs | Self-Completed | 2.54 | 0.588 |
| Had Help | 2.79 | 0.585 | |
| Subjective Norms | Self-Completed | 2.98 | 0.454 |
| Had Help | 2.86 | 0.244 | |
| Perceived Behavioural Control | Self-Completed | 1.82 | 0.486 |
| Had Help | 2.04 | 0.304 |
| Attitudes & Beliefs | Subjective Norms | Perceived Behavioural Control | Knowledge | Behaviour | |
|---|---|---|---|---|---|
| Q7. It’s My Right to Ask for ABs | 0.508 | 0.227 | 2.207 | 0.048 | |
| Q9. Know When I Need ABs | 1.209 | 3.894 | 0.301 | 1.371 | |
| Q11. Confident to Ask for ABs | 5.325 | 7.097 | 0.817 | 4.715 | |
| Q18. Expect Abs form Dr. | 5.955 | 20.565 | 5.336 | 10.053 | |
| Q2. Friends & Family Follow AB Recommendations | 4.164 | 1.178 | 1.368 | 3.140 | |
| Q8. Friends & Family Only Use Prescribed ABs | 4.164 | 1.178 | 1.368 | 3.140 | |
| Q10. Use of Abs Without Prescription is Common | 0.798 | 3.309 | 1.885 | 3.664 | |
| Q15. Easily Get Abs from Dr. | 6.717 | 0.014 | 0.001 | 9.237 | |
| Q16. Easily Get Abs Online | 10.109 | 5.341 | 5.631 | 3.962 | |
| Q17. Easily Get Abs Family | 0.087 | 3.224 | 0.581 | 7.848 | |
| Q1. Abs Reduce Cold Symptoms | 0.002 | 2.682 | 0.664 | 2.476 | |
| Q3. Abs Are Needed for Colds | 0.907 | 0.174 | 0.180 | 0.375 | |
| Q4. Abs Can Have Negative Side Effects | 3.221 | 0.007 | 0.002 | 0.025 | |
| Q12. Abs Will be Less Effective in Future | 0.235 | 2.674 | 3.329 | 7.758 | |
| Q5. I Use Abs Without Dr. Consultation | 0.018 | 0.006 | 1.675 | 5.455 | |
| Q6. I Use Leftover ABs | 1.386 | 0.452 | 0.064 | 1.434 | |
| Q13. I Consult Dr. Prior to Taking ABs | 0.059 | 0.233 | 0.609 | 0.048 | |
| Q14. I Keep Leftover ABs | 1.693 | 0.109 | 1.179 | 1.893 |
| Survey Platform | Mean | SD | Cronbach’s α | |
|---|---|---|---|---|
| Behaviour | In-Person | 2.76 | 0.56 | 0.68 |
| M-Turk | 2.32 | 0.69 | 0.77 | |
| Knowledge | In-Person | 3.03 | 0.53 | 0.70 |
| M-Turk | 2.73 | 0.54 | 0.53 | |
| Perceived Behavioural Control | In-Person | 2.02 | 0.40 | 0.48 |
| M-Turk | 2.03 | 0.53 | 0.59 | |
| Subjective Norms | In-Person | 2.83 | 0.55 | 0.59 |
| M-Turk | 2.86 | 0.76 | 0.75 | |
| Attitudes & Beliefs | In-Person | 2.76 | 0.56 | 0.68 |
| M-Turk | 2.32 | 0.69 | 0.77 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schramm, L.; Byrne, M.K.; Sweetnam, T. Antibiotic Misuse Behaviours of Older People: Confirmation of the Factor Structure of the Antibiotic Use Questionnaire. Antibiotics 2023, 12, 718. https://doi.org/10.3390/antibiotics12040718
Schramm L, Byrne MK, Sweetnam T. Antibiotic Misuse Behaviours of Older People: Confirmation of the Factor Structure of the Antibiotic Use Questionnaire. Antibiotics. 2023; 12(4):718. https://doi.org/10.3390/antibiotics12040718
Chicago/Turabian StyleSchramm, Loni, Mitchell K. Byrne, and Taylor Sweetnam. 2023. "Antibiotic Misuse Behaviours of Older People: Confirmation of the Factor Structure of the Antibiotic Use Questionnaire" Antibiotics 12, no. 4: 718. https://doi.org/10.3390/antibiotics12040718
APA StyleSchramm, L., Byrne, M. K., & Sweetnam, T. (2023). Antibiotic Misuse Behaviours of Older People: Confirmation of the Factor Structure of the Antibiotic Use Questionnaire. Antibiotics, 12(4), 718. https://doi.org/10.3390/antibiotics12040718