

Amelioration Strategies for Silver Diamine Fluoride: Moving from Black to White



 ,
, 

Abstract
1. Introduction
2. Early Childhood Caries: The Ripple Effect
3. Silver Diamine Fluoride SDF: Sharpening an Anticaries Agent
4. Silver: The Old New
5. SDF Re-Composition: Nanometals vs. Ionic Silver
6. Selenium: A Plausible Substitute
6.1. Selenium and Human Health
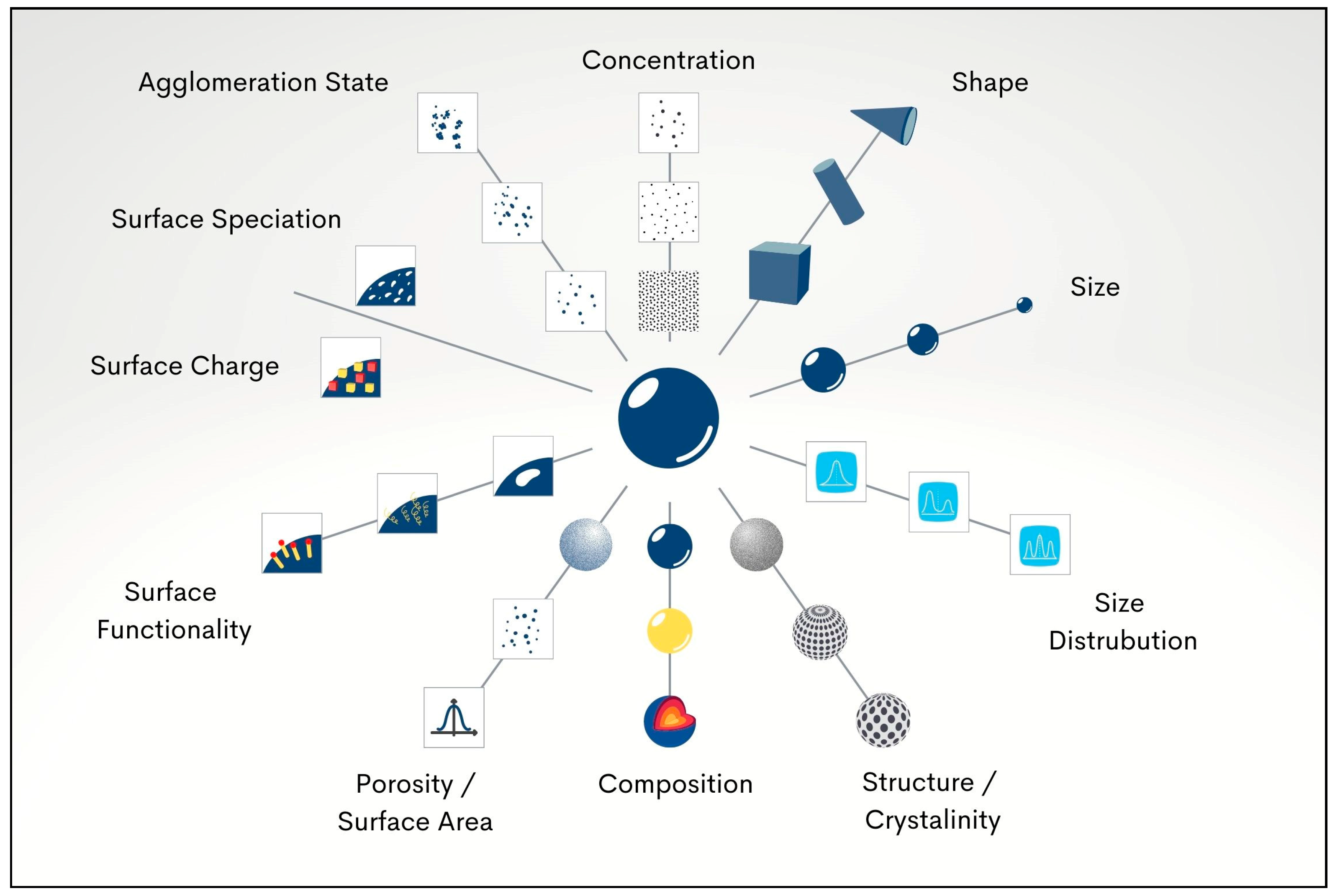
6.2. Selenium Nanoparticle Properties: Size, Shape, and Synthesis
6.3. Selenium Nanoparticles and Toxicity Concerns
6.4. SeNPs and the Role of Capping Agents

{kind=link}
{kind=link}
| STUDY | METHODS | KEY FINDINGS |
|---|---|---|
| [103] | Synthesis: chemically—Na2SeO3 reduction; Stabiliser: BSA Characterisation: TEM and DLS Tested microbes: S. aureus SeNPs tested concentrations: 7.8, 15.5, 31 μg/mL | -SeNPs shape/size: spherical/40–60 nm -SeNPs inhibited S. aureus growth compared with no treatment. -SeNPs killed approx. 40% of S. aureus after 3, 4, and 5 h |
| [129] | Synthesis: chemically—chitosan dissolution Characterisation: DLS Sample: skin infection swabs (n = 25) Tested microbes: 49 various bacterial strains Antibacterial tests: agar diffusion assay, growth curves SeNPs tested concentrations: up to 100 μg/mL | * Size and shape of SeNPs: not revealed -Bacterial growth curves were inhibited by low concentration (1 μg/mL) in all tested bacterial isolates -64 μg/mL of SeNPs shows complete inhibition when applied on E. fergusonii, P. aeruginosa, and S. agalactiae assays |
| [130] | Synthesis: biosynthesis—R. Alstonia eutropha bacterium-based Na2SeO3 reduction Characterisation: TEM, SEM, XRD, and SAED Tested microbes: E. coli, P. aeruginosa, S. aureus, S. pyogenes, and A. clavatus | -SeNPs shape/size: spherical 40–120 nm hexagonal crystalline -MIC: E. coli 125 μg/mL, P. aeruginosa 100 μg/mL, S. aureus 100 μg/mL, S. pyogenes 250 μg/mL and A. clavatus 500 μg/mL |
| [131] | Synthesis: chemically—Na2SeO3 reduction using glutathione Stabiliser: BSA Characterisation: FTIR, UV–Vis, DLS, SEM, and TEM Tested microbes: E. coli, S. aureus, Salmonella, and Listeria | -SeNPs shape/size: spherical ~79 nm -SeNPs show dose-dependent antimicrobial action against S. aureus but not the other three pathogens -SeNPs exerts cytotoxicity on cancer cells Caco-2 after 24 h exposure |
| [132] | Synthesis: (1) biosynthesised SeNPs (B. mycoides); (2) chemically synthesised SeNPs Characterisation: TEM, EDX, and DLS Tested microbes: P. aeruginosa and S. aureus Antibacterial tests: biofilms on hydroxyapatite discs | -SeNPs shape: spherical -Biosynthesized SeNPs had greater antibacterial action than chemically synthesized SeNPs |
| [133] | Synthesis: chemical method (using SeO2 as a precursor) Stabiliser: polyvinyl alcohol Characterisation: TEM, EDS, and FTIR Tested microbes: S. aureus Cytotoxicity: human dermal fibroblasts | -SeNPs shape/size: amorphous and spherical 43–205 nm -SeNPs antimicrobial; action is size dependent -greatest antibacterial action was observed in 81 nm SeNPs |
| [134] | Synthesis: chemical method (using SeO2 and ascorbic acid) Stabiliser: egg white lysozyme (EWL) Characterisation: UV–Vis, FTIR, TEM, and XRD Tested microbes: E. coli, S. pneumoniae, B. cereus, K. pneumoniae, P. mirabilis, and B. subtilis | -SeNPs shape/size: spherical (crystalline structure)/40–60 nm -MIC: 10.0 μg mL−1 -ZOI: 19 mm (B. subtilis), 15 mm (E. coli), 14 mm (B. cereus), and 13 mm (K. pneumoniae) -SeNPs exhibits prolonged stability (minimum of 12 months) |
| [135] | Synthesis: chemical method (using dissolution of Na2SeO3, L-ascorbic acid, and polyvinyl alcohol PVA in purified water) Characterisation: TEM, XPS, and SEM (Ti implants coated with SeNPs 30–70 nm) Tested microbes: S. aureus | -SeNPs shape/size: spherical (crystalline structure)/50–200 nm -Oxidation state: zero -SeNPs showed great antibacterial activity even at 0.5 ppm |
| [136] | Synthesis: chemical method (using Na2SeO3 as a precursor) Stabiliser: BSA, D-glucose, and soluble starch Characterisation: UV–Vis, FTIR, SEM, and EDXTested microbes: B. subtilis (mid-log) Antimicrobial test: SEM | -SeNPs shape/size: (BSA): rod shaped/200–250 nm (D-Glucose): spherical/200 nm (starch): cubes/250–300 nm -Antioxidation capacity: starch > D-Glucose > BSA -Antibacterial effect seen in all samples but not quantified |
| [137] | Synthesis: green synthesis—ascorbic acid as reductant Stabiliser: BSA Tested microbes: S. aureus and E. coli | -SeNPs shape/size: spherical/10–100 nm Proliferation of fibroblasts was promoted by SeNPs, whereas growth of S. aureus was suppressed |
| [138] | Synthesis: green method (Na2SeO3 as a precursor, using bovine urine) Characterisation: UV–Vis, SEM, TEM, DLS, AFM, and EDX Tested microbes: E. coli, K. pneumoniae, P. aeruginosa, Serratia, Proteus, and S. aureus | -SeNPs shape/size: spherical/110 nm -SeNPs effective against all species especially against Klebsiella species. |
| [139] | Synthesis: chemically—using Na2SeO3 Characterisation: UV–Vis Tested microbes: P. aeruginosa, Salmonella typhimurium, E.coli, S. sanguinis, S. aureus, and E. faecalis | MIC: S. sanguinis, 68 μg/mL S. aureus, 137 μg/mL E. faecalis 274 μg/mL |
| [140] | Synthesis: chemically—Na2SeO3 as a precursor Stabiliser: (i) BSA + ascorbic acid, (ii) Chitosan + ascorbic acid, and (iii) glucose Characterisation: FTIR, XRD, DLS, TEM, DLS, and UV–Vis Tested microbes: mixed biofilm S. aureus and C. albicans Cytotoxicity: human dermal fibroblasts | -SeNPs shape/size: spherical/70–300 nm -MIC: The lowest MIC was against C. albicans (25 μg/mL) -Zeta potential: SeNPs-Chit < SeNPs-BSA < SeNPs-Gluc * SeNPs-BSA was less cytotoxic than the other two formulations |
| [141] | Synthesis: chemical method (using Na2SeO3 as a precursor) Characterisation: UV–Vis, XRD, and SEM Tested microbes: S. aureus isolated from public water Antibacterial tests: disk diffusion assay, microdilution assay | -SeNPs shape/size: rod/85–275 nm -MIC: 50 μg/mL -synthetic SeNPs contributed to the breakdown of S. aureus biofilms |
| [109] | Synthesis: chemically—reduction of Na2SeO3 Characterisation: TEM, DLS, and XRD Tested microbes: E. faecalis Cytotoxicity: human fibroblasts | -SeNPs shape/size: spherical/77 + 27 nm -CFU: significantly reduced compared with control -Methylene Blue-induced Photodynamic Antimicrobial Chemotherapy SeNPs-MB-PACT showed the greatest antibiofilm impact -At 128 μg/mL SeNPs, 50% of human fibroblasts survived |
| [142] | Synthesis: biosynthesis—guava leaves (Psidium guajava) Characterisation: UV–Vis, DLS, TEM, and XRD Tested microbes: E. faecalis Group I: Distilled water (control), Group II: SeNPs (1 mg/mL), Group III: Calcium hydroxide (1 mg/mL), Group IV: 2% CHX, and Group V: 5.25% NaOCl Antibacterial tests: agar diffusion method, microdilution, viable cell count, antibiofilm assay, and Anthrone and Bradford’s tests | -SeNPs shape/size: spherical/30–50 nm -Zeta potential: −60 mV. -MIC: 25 mg/mL -ZOI: SeNPs 11.33–28.50 mm (based on the concentration) -SeNPs are the most active against E. faecalis biofilm, followed by NaOCl, CHX and Ca(OH)2 |
| [19] | Synthesis: green method (using Brassica Oleracea (Broccoli)) Characterisation: UV–Vis, TEM, FTIR, and EDX Tested microbes: S. mutans, S. aureus, E. faecalis, Lactobacillus, and C. albicans | -SeNPs shape/size: spherical/10–25 nm -greatest ZOI reported against S. mutans |
| [143] | Synthesis: biosynthesis—Na2SeO3 with citrus fruit extracts (lemons and grapefruits) Characterisation: UV–Vis, TEM, FTIR, and DLS Tested microbes: E. coli, M. luteus, K. pneumoniae, and B. subtilis Antimicrobial tests: agar diffusion assay | -SeNPs shape/size: not determined -SeNPs ZOI: 20 ± 1.646 mm against K. pneumoniae -A noticeable antimicrobial effect was detected after testing Citrus SeNPs -SeNPs could replace traditional antibiotics |
| [144] | Synthesis: biosynthesis—Na2SeO3 using Rosmarinus officinalis extract Characterisation: UV–Vis, DLS, TEM, XRD, and FTIR Tested microbes: M. tuberculosis, S. aureus, S. mutans, E. coli, and P. aeruginosa | -SeNPs shape/size: Spherical 20 to 40 nm -MIC in µg/mL: (M. tuberculosis), 256; (S. aureus), 16; (S. mutans), 32; (E. coli), 128; and (P. aeruginosa), 64 |
| [145] | Synthesis: chemical reduction Bacterial tests: MHB microdilution to assess MIC and MBC | SeNPs size: 81.4 nm MIC in µg/mL: S. mutans 68, L. acidophilus 137 and C. albicans 274 MBC in µg/mL: S. mutans 274 after 1–2 h and 137 after 6–24 h |
| [120] | Synthesis: biosynthesis—Na2SeO3 (precursor) using Calendula officinalis L. flowers as a (capping agent) Characterisation: SEM, TEM, FTIR, and EDX Tested microbes: Serratia marcescens, Enterobacter cloacae, and Alcaligenes faecalis bacteria Antimicrobial tests: disc diffusion | -SeNPs shape/size: spherical/40–60 nm -SeNPs demonstrated superior antibacterial effect, at various incubation times compared with the antibiotic ciprofloxacin CIP -SeNPs had greater antioxidant activity than methanolic extracts of flowers Cof-Met extract and Na2SeO3 |
| [146] | Synthesis: chemically—concentration was 128 and 64 μg/mL Characterisation: chemical reduction method Cytotoxicity: MTT test on human gingival fibroblast Tested Microbes: S. mutans | SeNPs enhanced photodynamic therapy (PDT) activity and exhibited significant antibiofilm action against S. mutans |
| [15] | Tested Microbes: S. salivarius, S. mutans, and S. sanguinis Control: untreated sealant Analysis: SEM, CLSM | Organo-selenium dental sealant was able to inhibit the growth of all species individually and in a mixed biofilm. |
7. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nguyen, T.M.; Tonmukayakul, U.; Hall, M.; Calache, H. Cost-effectiveness analysis of silver diamine fluoride to divert dental general anaesthesia compared to standard care. Aust. Dent. J. 2022, 67, 352–361. [Google Scholar] [CrossRef] [PubMed]
- Burgess, J.O.; Vaghela, P.M. Silver diamine fluoride: A successful anticarious solution with limits. Adv. Dent. Res. 2018, 29, 131–134. [Google Scholar] [CrossRef] [PubMed]
- Rosenblatt, A.; Stamford, T.C.; Niederman, R. Silver diamine fluoride: A caries “silver-fluoride bullet”. J. Dent. Res. 2009, 88, 116–125. [Google Scholar] [CrossRef] [PubMed]
- Gao, S.S.; Zhao, I.S.; Hiraishi, N.; Duangthip, D.; Mei, M.L.; Lo, E.C.M.; Chu, C.H. Clinical trials of silver diamine fluoride in arresting caries among children: A systematic review. JDR Clin. Transl. Res. 2016, 1, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Fung, M.H.T.; Duangthip, D.; Wong, M.C.M.; Lo, E.C.M.; Chu, C.H. Arresting dentine caries with different concentration and periodicity of silver diamine fluoride. JDR Clin. Transl. Res. 2016, 1, 143–152. [Google Scholar] [CrossRef] [PubMed]
- Duangthip, D.; Fung, M.H.T.; Wong, M.C.M.; Chu, C.H.; Lo, E.C.M. Adverse effects of silver diamine fluoride treatment among preschool children. J. Dent. Res. 2018, 97, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Crystal, Y.O.; Niederman, R. Evidence-based dentistry update on silver diamine fluoride. Dent. Clin. North Am. 2019, 63, 45–68. [Google Scholar] [CrossRef] [PubMed]
- Nelson, T.; Scott, J.M.; Crystal, Y.O.; Berg, J.H.; Milgrom, P. Silver diamine fluoride in pediatric dentistry training programs: Survey of graduate program directors. Pediatr. Dent. 2016, 38, 212–217. [Google Scholar]
- Sabbagh, H.; Othman, M.; Khogeer, L.; Al-Harbi, H.; Al Harthi, A.; Abdulgader Yaseen Abdulgader, A. Parental acceptance of silver diamine fluoride application on primary dentition: A systematic review and meta-analysis. BMC Oral Health 2020, 20, 227. [Google Scholar] [CrossRef]
- Duangthip, D.; Gao, S.S.; Chen, K.J.; Lo, E.C.M.; Chu, C.H. Oral health-related quality of life of preschool children receiving silver diamine fluoride therapy: A prospective 6-month study. J. Dent. 2019, 81, 27–32. [Google Scholar] [CrossRef]
- Gomes, M.C.; Perazzo, M.F.; Neves, E.T.; Martins, C.C.; Paiva, S.M.; Granville-Garcia, A.F. Oral problems and self-confidence in preschool children. Braz. Dent. J. 2017, 28, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Seifo, N.; Cassie, H.; Radford, J.R.; Innes, N.P.T. “I guess it looks worse to me, it doesn’t look like there’s been a problem solved but obviously there is”: A qualitative exploration of children’s and their parents’ views of silver diamine fluoride for the management of carious lesions in children. BMC Oral Health 2021, 21, 367. [Google Scholar] [CrossRef]
- Al-Bitar, Z.B.; Al-Omari, I.K.; Sonbol, H.N.; Al-Ahmad, H.T.; Cunningham, S.J. Bullying among Jordanian schoolchildren, its effects on school performance, and the contribution of general physical and dentofacial features. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 872–878. [Google Scholar] [CrossRef] [PubMed]
- Saafan, A.; Zaazou, M.H.; Sallam, M.K.; Mosallam, O.; El Danaf, H.A. Assessment of photodynamic therapy and nanoparticles effects on caries models. Open Access Maced. J. Med. Sci. 2018, 6, 1289–1295. [Google Scholar] [CrossRef] [PubMed]
- Tran, P.; Kopel, J.; Ray, C.; Reed, J.; Reid, T.W. Organo-selenium containing dental sealant inhibits biofilm formation by oral bacteria. Dent. Mater. 2022, 38, 848–857. [Google Scholar] [CrossRef]
- Bisht, N.; Phalswal, P.; Khanna, P.K. Selenium nanoparticles: A review on synthesis and biomedical applications. Mater. Adv. 2022, 3, 1415–1431. [Google Scholar] [CrossRef]
- Handy, R.D.; Owen, R.; Valsami-Jones, E. The ecotoxicology of nanoparticles and nanomaterials: Current status, knowledge gaps, challenges, and future needs. Ecotoxicology 2008, 17, 315–325. [Google Scholar] [CrossRef]
- Jolly, J.; Mohd Ahmar, R.; Zeeshan, A. Selenium nanoparticles: Small is the new big: Mini review. Open J. Chem. 2020, 6, 13–16. [Google Scholar] [CrossRef]
- Dhanraj, G.; Rajeshkumar, S. Anticariogenic effect of selenium nanoparticles synthesized using Brassica oleracea. J. Nanomater. 2021, 2021, 8115585. [Google Scholar] [CrossRef]
- Kassebaum, N.J.; Bernabe, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.; Marcenes, W. Global burden of untreated caries: A systematic review and metaregression. J. Dent. Res. 2015, 94, 650–658. [Google Scholar] [CrossRef]
- AAPD. Policy on Early Childhood Caries (ECC): Classifications, Consequences, and Preventive Strategies. The Reference Manual of Pediatric Dentistry; American Academy of Pediatric Dentistry: Chicago, IL, USA, 2022; pp. 90–93. [Google Scholar]
- Paolone, G.; Mazzitelli, C.; Formiga, S.; Kaitsas, F.; Breschi, L.; Mazzoni, A.; Tete, G.; Polizzi, E.; Gherlone, E.; Cantatore, G. One-year impact of COVID-19 pandemic on Italian dental professionals: A cross-sectional survey. Minerva Dent. Oral Sci. 2022, 71, 212–222. [Google Scholar] [CrossRef] [PubMed]
- Chu, C.H.; Ho, P.-L.; Lo, E.C. Oral health status and behaviours of preschool children in Hong Kong. BMC Public Health 2012, 12, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Duangthip, D.; Gao, S.S.; Lo, E.C.; Chu, C.H. Early childhood caries among 5- to 6-year-old children in Southeast Asia. Int. Dent. J. 2017, 67, 98–106. [Google Scholar] [CrossRef]
- Casamassimo, P.S.; Thikkurissy, S.; Edelstein, B.L.; Maiorini, E. Beyond the dmft: The human and economic cost of early childhood caries. J. Am. Dent. Assoc. 2009, 140, 650–657. [Google Scholar] [CrossRef] [PubMed]
- Ladewig, N.M.; Camargo, L.B.; Tedesco, T.K.; Floriano, I.; Gimenez, T.; Imparato, J.C.P.; Mendes, F.M.; Braga, M.M.; Raggio, D.P. Management of dental caries among children: A look at the cost-effectiveness. Expert Rev. Pharm. Outcomes Res. 2018, 18, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Alcaino, E.; KIilpatrick, N.M.; Smith, E.D.K. Utilization of day stay general anaesthesia for the provision ofdental treatment to children in New South Wales, Australia. Int. J. Paediatr. Dent. 2000, 10, 206–212. [Google Scholar] [CrossRef]
- Almeida, A.G.; Roseman, M.M.; Sheff, M.; Huntington, N.; Hughes, C.V. Future caries susceptibility in children with early childhood caries following treatment under general anesthesia. Pediatr. Dent. 2000, 22, 302–306. [Google Scholar]
- Alshehri YF, A.; Nicholls, W.; Mai, N.Q.; Park, J.S.; Kruger, E. Cross-sectional analysis of dental treatment under general anaesthesia in hospitalised Western Australian children in 2018–19. Aust. Health Rev. 2021. [Google Scholar] [CrossRef]
- Pitts, N.B.; Zero, D.T.; Marsh, P.D.; Ekstrand, K.; Weintraub, J.A.; Ramos-Gomez, F.; Tagami, J.; Twetman, S.; Tsakos, G.; Ismail, A. Dental caries. Nat. Rev. Dis. Prim. 2017, 3, 17030. [Google Scholar] [CrossRef]
- Marsh, P.D. Are dental diseases examples of ecological catastrophes? Microbiology 2003, 149 Pt. 2, 279–294. [Google Scholar] [CrossRef]
- Bowen, W.; Koo, H. Biology of Streptococcus mutans-derived glucosyltransferases: Role in extracellular matrix formation of cariogenic biofilms. Caries Res. 2011, 45, 69–86. [Google Scholar] [CrossRef] [PubMed]
- Paes Leme, A.F.; Koo, H.; Bellato, C.M.; Bedi, G.; Cury, J.A. The role of sucrose in cariogenic dental biofilm formation—New insight. J. Dent. Res. 2006, 85, 878–887. [Google Scholar] [CrossRef] [PubMed]
- Hajishengallis, E.; Parsaei, Y.; Klein, M.I.; Koo, H. Advances in the microbial etiology and pathogenesis of early childhood caries. Mol. Oral Microbiol. 2017, 32, 24–34. [Google Scholar] [CrossRef]
- Mei, M.L.; Nudelman, F.; Marzec, B.; Walker, J.M.; Lo, E.C.M.; Walls, A.W.; Chu, C.H. Formation of fluorohydroxyapatite with silver diamine fluoride. J. Dent. Res. 2017, 96, 1122–1128. [Google Scholar] [CrossRef] [PubMed]
- Nishino, M.; Yoshida, S.; Sobue, S.; Kato, J.; Nishida, M. Effect of topically applied ammoniacal silver fluoride on dental caries in children. J. Osaka Univ. Dent. Sch. 1969, 9, 149–155. [Google Scholar]
- Horst, J.; Ellenikiotis, H.; Milgrom, P. UCSF Protocol for caries arrest using silver diamine fluoride: Rationale, indications, and consent. J. Calif. Dent. Assoc. 2016, 44, 16–28. [Google Scholar]
- Mei, M.L.; Ito, L.; Cao, Y.; Lo, E.C.; Li, Q.; Chu, C. An ex vivo study of arrested primary teeth caries with silver diamine fluoride therapy. J. Dent. 2014, 42, 395–402. [Google Scholar] [CrossRef]
- Shah, S.; Bhaskar, V.; Chawla, S.; Venkataraghavan, K.; Choudhary, P.; Ganesh, M.; Trivedi, K. Efficacy of silver diamine fluoride as a topical fluoride agent compared to fluoride varnish and acidulated phosphate fluoride gel: An in vivo study. Indian J. Dent. Res. 2013, 24, 575–581. [Google Scholar] [CrossRef]
- Greenwall-Cohen, J.; Greenwall, L.; Barry, S. Silver diamine fluoride—An overview of the literature and current clinical techniques. Br. Dent. J. 2020, 228, 831–838. [Google Scholar] [CrossRef]
- Rajendra, A.; Veitz-Keenan, A.; Oliveira, B.H.; Ruff, R.R.; Wong, M.C.M.; Innes, N.P.T.; Radford, J.; Seifo, N.; Niederman, R. Topical silver diamine fluoride for managing dental caries in children and adults. Cochrane Database Syst. Reviews. 2017, CD012718. [Google Scholar] [CrossRef]
- Mei, M.L.; Ito, L.; Cao, Y.; Li, Q.L.; Lo, E.C.; Chu, C.H. Inhibitory effect of silver diamine fluoride on dentine demineralisation and collagen degradation. J. Dent. 2013, 41, 809–817. [Google Scholar] [CrossRef] [PubMed]
- Fung, M.H.T.; Duangthip, D.; Wong, M.C.M.; Lo, E.C.M.; Chu, C.H. Randomized clinical trial of 12% and 38% silver diamine fluoride treatment. J. Dent. Res. 2018, 97, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Craig, G.G.; Knight, G.M.; McIntyre, J.M. Clinical evaluation of diamine silver fluoride/potassium iodide as a dentine desensitizing agent. A pilot study. Aust. Dent. J. 2012, 57, 308–311. [Google Scholar] [CrossRef] [PubMed]
- Deutsch, A. An alternate technique of care using silver fluoride followed by stannous fluoride in the management of root caries in aged care. Spec. Care Dent. 2016, 36, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Knight, G.M.; McIntyre, J.M.; Craig, G.G.; Mulyani; Zilm, P.S.; Gully, N. An in vitro model to measure the effect of a silver fluoride and potassium. Aust. Dent. J. 2005, 50, 242–245. [Google Scholar] [CrossRef]
- Mei, M.L.; Chu, C.H.; Low, K.H.; Che, C.M.; Lo, E.C. Caries arresting effect of silver diamine fluoride on dentine carious lesion with S. mutans and L. acidophilus dual-species cariogenic biofilm. Med. Oral Patol. Oral Cir. Bucal 2013, 18, e824–e831. [Google Scholar] [CrossRef]
- Mei, M.L.; Lo, E.C.M.; Chu, C.H. Arresting dentine caries with silver diamine fluoride: What’s behind it? J. Dent. Res. 2018, 97, 751–758. [Google Scholar] [CrossRef]
- Mei, M.L.; Li, Q.L.; Chu, C.H.; Yiu, C.K.; Lo, E.C. The inhibitory effects of silver diamine fluoride at different concentrations on matrix metalloproteinases. Dent. Mater. 2012, 28, 903–908. [Google Scholar] [CrossRef]
- Llodra, J.C.; Rodriguez, A.; Ferrer, B.; Menardia, V.; Ramos, T.; Morato, M. Efficacy of silver diamine fluoride for caries reduction in primary teeth and first permanent molars of schoolchildren: 36-month clinical trial. J. Dent. Res. 2005, 84, 721–724. [Google Scholar] [CrossRef]
- Gotjamanos, T. Pulp response in primary teeth with deep residual caries treated with silver fluoride and glass ionorner cement (‘atraumatic’ technique). Aust. Dent. J. 1996, 41, 328–362. [Google Scholar] [CrossRef]
- Hu, S.; Meyer, B.; Duggal, M. A silver renaissance in dentistry. Eur. Arch. Paediatr. Dent. 2018, 19, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Duangthip, D.; Wong, M.C.M.; Chu, C.H.; Lo, E.C.M. Caries arrest by topical fluorides in preschool children: 30-month results. J. Dent. 2018, 70, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Bagher, S.M.; Sabbagh, H.J.; AlJohani, S.M.; Alharbi, G.; Aldajani, M.; Elkhodary, H. Parental acceptance of the utilization of silver diamine fluoride on their child’s primary and permanent teeth. Patient Prefer. Adherence 2019, 13, 829–835. [Google Scholar] [CrossRef] [PubMed]
- Crystal, Y.O.; Janal, M.N.; Hamilton, D.S.; Niederman, R. Parental perceptions and acceptance of silver diamine fluoride staining. J. Am. Dent. Assoc. 2017, 148, 510–518.e4. [Google Scholar] [CrossRef]
- Paolone, G.; Scolavino, S.; Gherlone, E.; Spagnuolo, G. Direct esthetic composite restorations in anterior teeth: Managing symmetry strategies. Symmetry 2021, 13, 797. [Google Scholar] [CrossRef]
- Knight, G.M.; McIntyre, J.M.; Craig, G.G.; Mulyani; Zilm, P.S.; Gully, N.J. Inability to form a biofilm of Streptococcus mutans on silver fluoride- and potassium iodide-treated demineralized dentin. Quintessence Int. 2009, 40, 155–161. [Google Scholar]
- Zhao, I.S.; Chu, S.; Yu, O.Y.; Mei, M.L.; Chu, C.H.; Lo, E.C.M. Effect of silver diamine fluoride and potassium iodide on shear bond strength of glass ionomer cements to caries-affected dentine. Int. Dent. J. 2019, 69, 341–347. [Google Scholar] [CrossRef]
- Roberts, A.; Bradley, J.; Merkley, S.; Pachal, T.; Gopal, J.V.; Sharma, D. Does potassium iodide application following silver diamine fluoride reduce staining of tooth? A systematic review. Aust. Dent. J. 2020, 65, 109–117. [Google Scholar] [CrossRef]
- Haiat, A.; Ngo, H.C.; Samaranayake, L.P.; Fakhruddin, K.S. The effect of the combined use of silver diamine fluoride and potassium iodide in disrupting the plaque biofilm microbiome and alleviating tooth discoloration: A systematic review. PLoS ONE 2021, 16, e0252734. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Lo, E.C.M.; Liu, B.Y.; Wong, M.C.M.; Chu, C.H. Randomized clinical trial on arresting dental root caries through silver diammine fluoride applications in community-dwelling elders. J. Dent. 2016, 51, 15–20. [Google Scholar] [CrossRef]
- Fröhlich, T.T.; Gindri, L.D.; Pedrotti, D.; Cavalheiro, C.P.; Soares, F.; Rocha, R.O. Evaluation of the use of potassium iodide application on stained demineralized dentin under resin composite following silver diamine fluoride application. Pediatr. Dent. 2021, 43, 57–61. [Google Scholar]
- Nagireddy, V.R.; Reddy, D.; Kondamadugu, S.; Puppala, N.; Mareddy, A.A.C. Nanosilver fluoride—A paradigm shift for arrest in dental caries in primary teeth of schoolchildren: A randomized controlled clinical trial. Int. J. Clin. Pediatr. Dent. 2019, 12, 484–490. [Google Scholar] [PubMed]
- Song, H.; Ahmad Nor, Y.; Yu, M.; Yang, Y.; Zhang, J.; Zhang, H.; Xu, C.; Mitter, N.; Yu, C. Silica nanopollens enhance adhesion for long-term bacterial inhibition. J. Am. Chem. Soc. 2016, 138, 6455–6462. [Google Scholar] [CrossRef]
- Cao, W.; Zhang, Y.; Wang, X.; Li, Q.; Xiao, Y.; Li, P.; Wang, L.; Ye, Z.; Xing, X. Novel resin-based dental material with anti-biofilm activity and improved mechanical property by incorporating hydrophilic cationic copolymer functionalized nanodiamond. J. Mater. Sci. Mater. Med. 2018, 29, 162. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.; Snigdha, S.; Bhavitha, K.B.; Babu, S.; Ajith, A.; Radhakrishnan, E.K. Biofabricated silver nanoparticles incorporated polymethyl methacrylate as a dental adhesive material with antibacterial and antibiofilm activity against Streptococcus mutans. 3 Biotech 2018, 8, 404. [Google Scholar] [CrossRef]
- Tirupathi, S.; Svsg, N.; Rajasekhar, S.; Nuvvula, S. Comparative cariostatic efficacy of a novel nano-silver fluoride varnish with 38% silver diamine fluoride varnish a double-blind randomized clinical trial. J. Clin. Exp. Dent. 2019, 11, e105-12. [Google Scholar] [CrossRef] [PubMed]
- Santos, V.E., Jr.; Vasconcelos Filho, A.; Targino, A.G.; Flores, M.A.; Galembeck, A.; Caldas, A.F., Jr.; Rosenblatt, A. A new “silver-bullet” to treat caries in children—Nano silver fluoride: A randomised clinical trial. J. Dent. 2014, 42, 945–951. [Google Scholar] [CrossRef]
- Targino, A.G.; Flores, M.A.; dos Santos Junior, V.E.; de Godoy Bene Bezerra, F.; de Luna Freire, H.; Galembeck, A.; Rosenblatt, A. An innovative approach to treating dental decay in children. A new anti-caries agent. J. Mater. Sci. Mater. Med. 2014, 25, 2041–2047. [Google Scholar] [CrossRef]
- Melaiye, A.; Youngs, W.J. Silver and its application as an antimicrobial agent. Expert Opin. Ther. Pat. 2005, 15, 125–130. [Google Scholar] [CrossRef]
- White, R.J. An historical overview of the use of silver in wound management. Br. J. Community Nurs. 2001, 6 (Suppl. S1), 3–8. [Google Scholar] [CrossRef]
- Barras, F.; Aussel, L.; Ezraty, B. Silver and antibiotic, new facts to an old story. Antibiotics 2018, 7, 79. [Google Scholar] [CrossRef] [PubMed]
- Mijnendonckx, K.; Leys, N.; Mahillon, J.; Silver, S.; Van Houdt, R. Antimicrobial silver: Uses, toxicity and potential for resistance. BioMetals 2013, 26, 609–621. [Google Scholar] [CrossRef] [PubMed]
- Peng, J.J.-Y.; Botelho, M.G.; Matinlinna, J.P. Silver compounds used in dentistry for caries management: A review. J. Dent. 2012, 40, 531–541. [Google Scholar] [CrossRef] [PubMed]
- Stebbins, E. What value has argenti nitras as a therapeutic agent in dentistry? Int. Dent. J. 1891, 12, 661–670. [Google Scholar]
- Seltzer, S. Effective duration of some agents used for dentin sterilization. J. Dent. Res. 1942, 21, 115–123. [Google Scholar] [CrossRef]
- James, P.; Parfitt, G. A clinical note on the use of silver nitrate in the prevention of fissure caries in newly erupted first permanant molars. Britsh Dent. J. 1954, 96, 35–36. [Google Scholar]
- Kidd, E. Caries removal and the pulpo-dentinal complex. Dent. Update 2000, 27, 476–482. [Google Scholar] [CrossRef]
- Silver, S.; Phung le, T.; Silver, G. Silver as biocides in burn and wound dressings and bacterial resistance to silver compounds. J. Ind. Microbiol. Biotechnol. 2006, 33, 627–634. [Google Scholar] [CrossRef]
- Maillard, J.Y.; Hartemann, P. Silver as an antimicrobial: Facts and gaps in knowledge. Crit. Rev. Microbiol. 2013, 39, 373–383. [Google Scholar] [CrossRef]
- Edwards-Jones, V. The benefits of silver in hygiene, personal care and healthcare. Lett. Appl. Microbiol. 2009, 49, 147–152. [Google Scholar] [CrossRef]
- Wijnhoven, S.W.P.; Peijnenburg, W.J.G.M.; Herberts, C.A.; Hagens, W.I.; Oomen, A.G.; Heugens, E.H.W.; Roszek, B.; Bisschops, J.; Gosens, I.; Van De Meent, D.; et al. Nano-silver—A review of available data and knowledge gaps in human and environmental risk assessment. Nanotoxicology 2009, 3, 109–138. [Google Scholar] [CrossRef]
- Hovhannisyan, Z.; Timotina, M.; Manoyan, J.; Gabrielyan, L.; Petrosyan, M.; Kusznierewicz, B.; Bartoszek, A.; Jacob, C.; Ginovyan, M.; Trchounian, K.; et al. Extract-mediated green synthesis and antibacterial action mechanisms of silver nanoparticles. Antibiotics 2022, 11, 1415. [Google Scholar] [CrossRef] [PubMed]
- Bang, S.J.; Jun, S.K.; Kim, Y.J.; Ahn, J.Y.; Vu, H.T.; Mandakhbayar, N.; Han, M.R.; Lee, J.H.; Kim, J.B.; Kim, J.S.; et al. Characterization of physical and biological properties of a caries-arresting liquid containing copper doped bioglass nanoparticles. Pharmaceutics 2022, 14, 1137. [Google Scholar] [CrossRef]
- Favaro, J.C.; de Mello Peixoto, Y.C.T.; Geha, O.; Dias, F.A.; Guiraldo, R.D.; Lopes, M.B.; Berger, S.B. Can silver diamine fluoride or silver nanoparticle-based anticaries agents to affect enamel bond strength? Restor. Dent. Endod. 2021, 46, e7. [Google Scholar] [CrossRef]
- Favaro, J.C.; Detomini, T.R.; Maia, L.P.; Poli, R.C.; Guiraldo, R.D.; Lopes, M.B.; Berger, S.B. Anticaries agent based on silver nanoparticles and fluoride: Characterization and biological and remineralizing effects-an in vitro study. Int. J. Dent. 2022, 2022, 9483589. [Google Scholar] [CrossRef] [PubMed]
- Drabowicz, J.; Mikołajczyk, M. Selenium at higher oxidation state. In Organoselenium Chemistry. Topics in Current Chemistry; Wirth, T., Ed.; Springer: Berlin/Heidelberg, Germany, 2000; Volume 208, pp. 143–176. [Google Scholar]
- Pasdar, H.; Hedayati Saghavaz, B.; Masoumi, M. A simple method for the recovery of selenium from copper anode slime sample using alkaline roasting process. Int. J. New Chem. 2019, 6, 143–150. [Google Scholar]
- Zhu, M.; Niu, G.; Tang, J. Elemental Se: Fundamentals and its optoelectronic applications. J. Mater. Chem. C 2019, 7, 2199–2206. [Google Scholar] [CrossRef]
- McNeal, J.M.; Balistrieri, L.S. Geochemistry and occurrence of selenium: An overview. Selenium Agric. Environ. 1989, 23, 1–13. [Google Scholar]
- Lakin, H.W. Selenium in Our Enviroment. Adv. Chem. 1973, 123, 96–111. [Google Scholar]
- Wallenberg, M.; Misra, S.; Wasik, A.M.; Marzano, C.; Björnstedt, M.; Gandin, V.; Fernandes, A.P. Selenium induces a multi-targeted cell death process in addition to ROS formation. J. Cell. Mol. Med. 2014, 18, 671–684. [Google Scholar] [CrossRef]
- Bai, K.; Hong, B.; He, J.; Hong, Z.; Tan, R. Preparation and antioxidant properties of selenium nanoparticles-loaded chitosan microspheres. Int. J. Nanomed. 2017, 12, 4527. [Google Scholar] [CrossRef] [PubMed]
- Wrobel, J.K.; Power, R.; Toborek, M. Biological activity of selenium: Revisited. IUBMB Life 2016, 68, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Majeed, W.; Zafar, M.; Bhatti, A.; John, P. Therapeutic potential of selenium nanoparticles. J. Nanomed. Nanotechnol. 2018, 9, 1000487. [Google Scholar] [CrossRef]
- Rayman, M.P. Selenium intake, status, and health: A complex relationship. Hormones 2020, 19, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Rayman, M.P. Selenium and human health. Lancet 2012, 379, 1256–1268. [Google Scholar] [CrossRef]
- Khurana, A.; Tekula, S.; Saifi, M.A.; Venkatesh, P.; Godugu, C. Therapeutic applications of selenium nanoparticles. Biomed. Pharmacother. 2019, 111, 802–812. [Google Scholar] [CrossRef]
- Wadhwani, S.A.; Shedbalkar, U.U.; Singh, R.; Chopade, B.A. Biogenic selenium nanoparticles: Current status and future prospects. Appl. Microbiol. Biotechnol. 2016, 100, 2555–2566. [Google Scholar] [CrossRef]
- Stroyuk, A.L.; Raevskaya, A.E.; Kuchmiy, S.Y.; Dzhagan, V.M.; Zahn, D.R.; Schulze, S. Structural and optical characterization of colloidal Se nanoparticles prepared via the acidic decomposition of sodium selenosulfate. Colloids Surf. A Physicochem. Eng. Asp. 2008, 320, 169–174. [Google Scholar] [CrossRef]
- Wang, H.; Zhang, J.; Yu, H. Elemental selenium at nano size possesses lower toxicity without compromising the fundamental effect on selenoenzymes: Comparison with selenomethionine in mice. Free. Radic. Biol. Med. 2007, 42, 1524–1533. [Google Scholar] [CrossRef]
- Kumar, A.; Sevonkaev, I.; Goia, D.V. Synthesis of selenium particles with various morphologies. J. Colloid Interface Sci. 2014, 416, 119–123. [Google Scholar] [CrossRef]
- Tran, P.A.; Webster, T.J. Selenium nanoparticles inhibit Staphylococcus aureus growth. Int. J. Nanomed. 2011, 6, 1553–1558. [Google Scholar]
- Luesakul, U.; Komenek, S.; Puthong, S.; Muangsin, N. Shape-controlled synthesis of cubic-like selenium nanoparticles via the self-assembly method. Carbohydr. Polym. 2016, 153, 435–444. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Yu, H.; Cao, W.; Dong, Y.; Zou, C.; Yang, Y.; Huang, S.; Dai, N.; Zhu, D.-M. Antimony doped cadmium selenium nanobelts with enhanced electrical and optoelectrical properties. Appl. Surf. Sci. 2014, 307, 608–614. [Google Scholar] [CrossRef]
- Nonsuwan, P.; Puthong, S.; Palaga, T.; Muangsin, N. Novel organic/inorganic hybrid flower-like structure of selenium nanoparticles stabilized by pullulan derivatives. Carbohydr. Polym. 2018, 184, 9–19. [Google Scholar] [CrossRef]
- Chaudhary, S.; Chauhan, P.; Kumar, R.; Bhasin, K.K. Toxicological responses of surfactant functionalized selenium nanoparticles: A quantitative multi-assay approach. Sci. Total Environ. 2018, 643, 1265–1277. [Google Scholar] [CrossRef]
- Sarkar, J.; Mridha, D.; Davoodbasha, M.A.; Banerjee, J.; Chanda, S.; Ray, K.; Roychowdhury, T.; Acharya, K.; Sarkar, J. A state-of-the-art systemic review on selenium nanoparticles: Mechanisms and factors influencing biogenesis and its potential applications. Biol. Trace Elem. Res. 2023. [Google Scholar] [CrossRef]
- Shahmoradi, S.; Shariati, A.; Zargar, N.; Yadegari, Z.; Asnaashari, M.; Amini, S.M.; Darban-Sarokhalil, D. Antimicrobial effects of selenium nanoparticles in combination with photodynamic therapy against Enterococcus faecalis biofilm. Photodiagnosis Photodyn. Ther. 2021, 35, 102398. [Google Scholar] [CrossRef]
- Ferro, C.; Florindo, H.F.; Santos, H.A. Selenium nanoparticles for biomedical applications: From development and characterization to therapeutics. Adv. Healthc. Mater. 2021, 10, e2100598. [Google Scholar] [CrossRef]
- Cavalu, S.; Antoniac, I.V.; Fritea, L.; Mates, I.M.; Milea, C.; Laslo, V.; Vicas, S.; Mohan, A. Surface modifications of the titanium mesh for cranioplasty using selenium nanoparticles coating. J. Adhes. Sci. Technol. 2018, 32, 2509–2522. [Google Scholar] [CrossRef]
- Srivastava, P.; Braganca, J.M.; Kowshik, M. In vivo synthesis of selenium nanoparticles by Halococcus salifodinae BK18 and their anti-proliferative properties against HeLa cell line. Biotechnol. Prog. 2014, 30, 1480–1487. [Google Scholar] [CrossRef]
- Liao, G.; Tang, J.; Wang, D.; Zuo, H.; Zhang, Q.; Liu, Y.; Xiong, H. Selenium nanoparticles (SeNPs) have potent antitumor activity against prostate cancer cells through the upregulation of miR-16. World J. Surg. Oncol. 2020, 18, 1–11. [Google Scholar] [CrossRef]
- Galić, E.; Radić, K.; Golub, N.; Vitali Čepo, D.; Kalčec, N.; Vrček, E.; Vinković, T. Utilization of olive pomace in green synthesis of selenium nanoparticles: Physico-chemical characterization, bioaccessibility and biocompatibility. Int. J. Mol. Sci. 2022, 23, 9128. [Google Scholar] [CrossRef] [PubMed]
- Selmani, A.; Ulm, L.; Kasemets, K.; Kurvet, I.; Erceg, I.; Barbir, R.; Pem, B.; Santini, P.; Marion, I.D.; Vinković, T. Stability and toxicity of differently coated selenium nanoparticles under model environmental exposure settings. Chemosphere 2020, 250, 126265. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Fu, Y.; Li, M.; Jiang, D.; Kutyreff, C.J.; Engle, J.W.; Lan, X.; Cai, W.; Chen, T. Chirality-driven transportation and oxidation prevention by chiral selenium nanoparticles. Angew. Chem. 2020, 132, 4436–4444. [Google Scholar] [CrossRef]
- Hariharan, H.; Al-Harbi, N.; Karuppiah, P.; Rajaram, S. Microbial synthesis of selenium nanocomposite using Saccharomyces cerevisiae and its antimicrobial activity against pathogens causing nosocomial infection. Chalcogenide Lett. 2012, 9, 509–515. [Google Scholar]
- Wang, Q.; Larese-Casanova, P.; Webster, T.J. Inhibition of various gram-positive and gram-negative bacteria growth on selenium nanoparticle coated paper towels. Int. J. Nanomed. 2015, 10, 2885. [Google Scholar]
- Tran, P.A.; O’Brien-Simpson, N.; Reynolds, E.C.; Pantarat, N.; Biswas, D.P.; O’Connor, A.J. Low cytotoxic trace element selenium nanoparticles and their differential antimicrobial properties against S. aureus and E. coli. Nanotechnology 2016, 27, 045101. [Google Scholar] [CrossRef]
- Hernandez-Diaz, J.A.; Garza-Garcia, J.J.; Leon-Morales, J.M.; Zamudio-Ojeda, A.; Arratia-Quijada, J.; Velazquez-Juarez, G.; Lopez-Velazquez, J.C.; Garcia-Morales, S. Antibacterial activity of biosynthesized selenium nanoparticles using extracts of calendula officinalis against potentially clinical bacterial strains. Molecules 2021, 26, 5929. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Yang, X.; Ning, Z.; Kwon, S.Y.; Li, M.-L.; Tack, F.M.G.; Kwon, E.E.; Rinklebe, J.; Yin, R. The beneficial and hazardous effects of selenium on the health of the soil-plant-human system: An overview. J. Hazard. Mater. 2022, 422, 126876. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, K.; Ochi, A.; Mihara, H.; Ogra, Y. Comparison of nutritional availability of biogenic selenium nanoparticles and chemically synthesized selenium nanoparticles. Biol. Trace Elem. Res. 2023. [Google Scholar] [CrossRef]
- Hosnedlova, B.; Kepinska, M.; Skalickova, S.; Fernandez, C.; Ruttkay-Nedecky, B.; Peng, Q.; Baron, M.; Melcova, M.; Opatrilova, R.; Zidkova, J. Nano-selenium and its nanomedicine applications: A critical review. Int. J. Nanomed. 2018, 13, 2107. [Google Scholar] [CrossRef] [PubMed]
- Mal, J.; Veneman, W.J.; Nancharaiah, Y.V.; van Hullebusch, E.D.; Peijnenburg, W.J.; Vijver, M.G.; Lens, P.N. A comparison of fate and toxicity of selenite, biogenically, and chemically synthesized selenium nanoparticles to zebrafish (Danio rerio) embryogenesis. Nanotoxicology 2017, 11, 87–97. [Google Scholar] [CrossRef] [PubMed]
- Kong, H.; Yang, J.; Zhang, Y.; Fang, Y.; Nishinari, K.; Phillips, G.O. Synthesis and antioxidant properties of gum arabic-stabilized selenium nanoparticles. Int. J. Biol. Macromol. 2014, 65, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Zhai, X.; Zhao, G.; Ren, F.; Leng, X. Synthesis, characterization, and controlled release of selenium nanoparticles stabilized by chitosan of different molecular weights. Carbohydr. Polym. 2015, 134, 158–166. [Google Scholar] [CrossRef] [PubMed]
- Huang, G.; Liu, Z.; He, L.; Luk, K.H.; Cheung, S.T.; Wong, K.H.; Chen, T. Autophagy is an important action mode for functionalized selenium nanoparticles to exhibit anti-colorectal cancer activity. Biomater. Sci. 2018, 6, 2508–2517. [Google Scholar] [CrossRef]
- Cai, W.; Hu, T.; Bakry, A.M.; Zheng, Z.; Xiao, Y.; Huang, Q. Effect of ultrasound on size, morphology, stability and antioxidant activity of selenium nanoparticles dispersed by a hyperbranched polysaccharide from Lignosus rhinocerotis. Ultrason. Sonochemistry 2018, 42, 823–831. [Google Scholar] [CrossRef] [PubMed]
- Dagmar, H.; Kristyna, C.; Pavel, K.; Vojtech, A.; Rene, K. Selenium nanoparticles and evaluation of their antimicrobial activity on bacterial isolates obtained from clinical specimens. In Proceedings of the Nanocon, Brno, Czech Republic, 14–16 October 2015. [Google Scholar]
- Srivastava, N.; Mukhopadhyay, M. Green synthesis and structural characterization of selenium nanoparticles and assessment of their antimicrobial property. Bioprocess Biosyst. Eng. 2015, 38, 1723–1730. [Google Scholar] [CrossRef]
- Nguyen, T.H.D.; Vardhanabhuti, B.; Lin, M.; Mustapha, A. Antibacterial properties of selenium nanoparticles and their toxicity to Caco-2 cells. Food Control 2017, 77, 17–24. [Google Scholar] [CrossRef]
- Piacenza, E.; Presentato, A.; Zonaro, E.; Lemire, J.A.; Demeter, M.; Vallini, G.; Turner, R.J.; Lampis, S. Antimicrobial activity of biogenically produced spherical Se-nanomaterials embedded in organic material against Pseudomonas aeruginosa and Staphylococcus aureus strains on hydroxyapatite-coated surfaces. Microb. Biotechnol. 2017, 10, 804–818. [Google Scholar] [CrossRef]
- Huang, T.; Holden, J.A.; Heath, D.E.; O’Brien-Simpson, N.M.; O’Connor, A.J. Engineering highly effective antimicrobial selenium nanoparticles through control of particle size. Nanoscale 2019, 11, 14937–14951. [Google Scholar] [CrossRef]
- Muthu, S.; Raju, V.; Gopal, V.B.; Gunasekaran, A.; Narayan, K.S.; Malairaj, S.; Lakshmikanthan, M.; Duraisamy, N.; Krishnan, K.; Perumal, P. A rapid synthesis and antibacterial property of selenium nanoparticles using egg white lysozyme as a stabilizing agent. SN Appl. Sci. 2019, 1, 1543. [Google Scholar] [CrossRef]
- Tran, P.A.; O’Brien-Simpson, N.; Palmer, J.A.; Bock, N.; Reynolds, E.C.; Webster, T.J.; Deva, A.; Morrison, W.A.; O’Connor, A.J. Selenium nanoparticles as anti-infective implant coatings for trauma orthopedics against methicillin-resistant Staphylococcus aureus and epidermidis: In vitro and in vivo assessment. Int. J. Nanomed. 2019, 14, 4613–4624. [Google Scholar] [CrossRef] [PubMed]
- Chandramohan, S.; Sundar, K.; Muthukumaran, A. Reducing agents influence the shapes of selenium nanoparticles (SeNPs) and subsequently their antibacterial and antioxidant activity. Mater. Res. Express 2019, 6, 0850i2. [Google Scholar] [CrossRef]
- Chung, S.; Zhou, R.; Webster, T.J. Green synthesized bsa-coated selenium nanoparticles inhibit bacterial growth while promoting mammalian cell growth. Int. J. Nanomed. 2020, 15, 115–124. [Google Scholar] [CrossRef]
- Menon, S.; Agarwal, H.; Rajeshkumar, S.; Jacquline Rosy, P.; Shanmugam, V.K. Investigating the antimicrobial activities of the biosynthesized selenium nanoparticles and its statistical analysis. BioNanoScience 2020, 10, 122–135. [Google Scholar] [CrossRef]
- Rangrazi, A.; Bagheri, H.; Ghazvini, K.; Boruziniat, A.; Darroudi, M. Synthesis and antibacterial activity of colloidal selenium nanoparticles in chitosan solution: A new antibacterial agent. Mater. Res. Express 2020, 6, 1250h3. [Google Scholar] [CrossRef]
- Filipović, N.; Ušjak, D.; Milenković, M.T.; Zheng, K.; Liverani, L.; Boccaccini, A.R.; Stevanović, M.M. Comparative study of the antimicrobial activity of selenium nanoparticles with different surface chemistry and structure. Front. Bioeng. Biotechnol. 2021, 8, 624621. [Google Scholar] [CrossRef]
- Hasani, S.; Khare, T.; Oak, U. Antibiofilm activity of selenium nanorods against multidrug-resistant staphylococcus aureus. MGM J. Med. Sci. 2021, 8, 415–421. [Google Scholar]
- Miglani, S.; Tani-Ishii, N. Biosynthesized selenium nanoparticles: Characterization, antimicrobial, and antibiofilm activity against Enterococcus faecalis. PeerJ 2021, 9, e11653. [Google Scholar] [CrossRef] [PubMed]
- Alvi, G.B.; Iqbal, M.S.; Ghaith, M.M.S.; Haseeb, A.; Ahmed, B.; Qadir, M.I. Biogenic selenium nanoparticles (SeNPs) from citrus fruit have anti-bacterial activities. Sci. Rep. 2021, 11, 4811. [Google Scholar] [CrossRef]
- Adibian, F.; Ghaderi, R.S.; Sabouri, Z.; Davoodi, J.; Kazemi, M.; Ghazvini, K.; Youssefi, M.; Soleimanpour, S.; Darroudi, M. Green synthesis of selenium nanoparticles using Rosmarinus officinalis and investigated their antimicrobial activity. BioMetals 2022, 35, 147–158. [Google Scholar] [CrossRef] [PubMed]
- Darroudi, M.; Rangrazi, A.; Ghazvini, K.; Bagheri, H.; Boruziniat, A. Antimicrobial activity of colloidal selenium nanoparticles in chitosan solution against streptococcus mutans, lactobacillus acidophilus, and candida albicans. Pesqui. Bras. Em Odontopediatria E Clínica Integr. 2021, 21, e0121. [Google Scholar] [CrossRef]
- Shahmoradi, S.; Shariati, A.; Amini, S.M.; Zargar, N.; Yadegari, Z.; Darban-Sarokhalil, D. The application of selenium nanoparticles for enhancing the efficacy of photodynamic inactivation of planktonic communities and the biofilm of Streptococcus mutans. BMC Res. Notes 2022, 15, 84. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almuqrin, A.; Kaur, I.P.; Walsh, L.J.; Seneviratne, C.J.; Zafar, S. Amelioration Strategies for Silver Diamine Fluoride: Moving from Black to White. Antibiotics 2023, 12, 298. https://doi.org/10.3390/antibiotics12020298
Almuqrin A, Kaur IP, Walsh LJ, Seneviratne CJ, Zafar S. Amelioration Strategies for Silver Diamine Fluoride: Moving from Black to White. Antibiotics. 2023; 12(2):298. https://doi.org/10.3390/antibiotics12020298
Chicago/Turabian StyleAlmuqrin, Amjad, Inder Preet Kaur, Laurence J. Walsh, Chaminda Jayampath Seneviratne, and Sobia Zafar. 2023. "Amelioration Strategies for Silver Diamine Fluoride: Moving from Black to White" Antibiotics 12, no. 2: 298. https://doi.org/10.3390/antibiotics12020298
APA StyleAlmuqrin, A., Kaur, I. P., Walsh, L. J., Seneviratne, C. J., & Zafar, S. (2023). Amelioration Strategies for Silver Diamine Fluoride: Moving from Black to White. Antibiotics, 12(2), 298. https://doi.org/10.3390/antibiotics12020298