

Extended Versus Intermittent Meropenem Infusion in the Treatment of Nosocomial Pneumonia: A Retrospective Single-Center Study

Abstract
:1. Introduction
2. Results
2.1. Baseline Characteristics
2.2. Microbiological Data
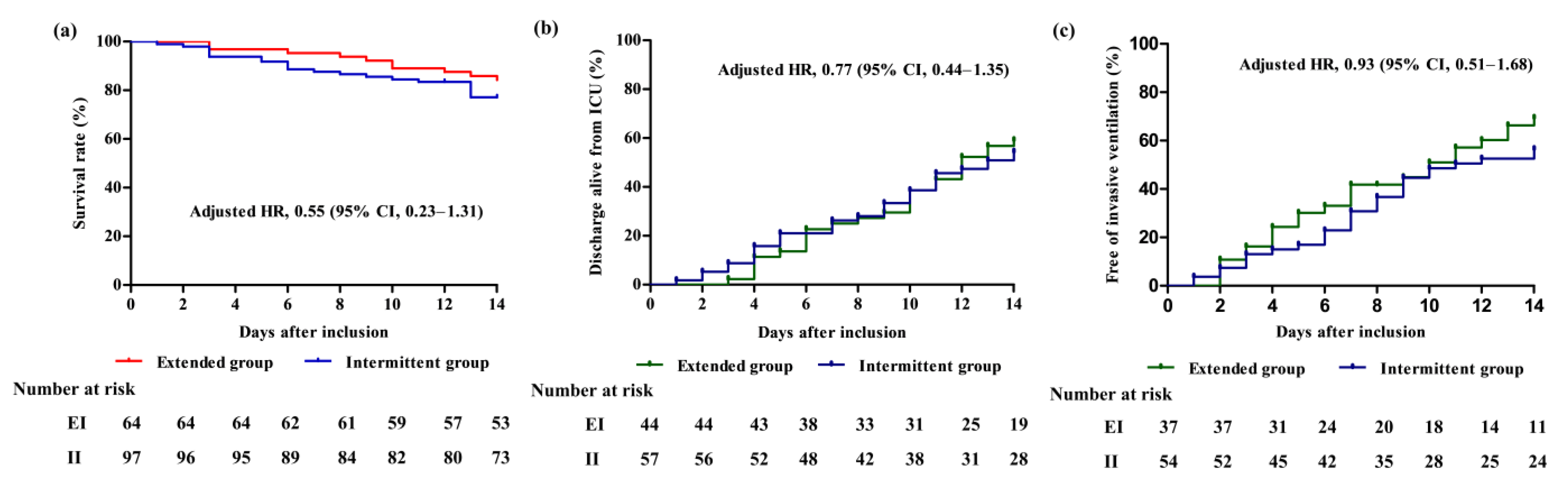
2.3. Outcomes
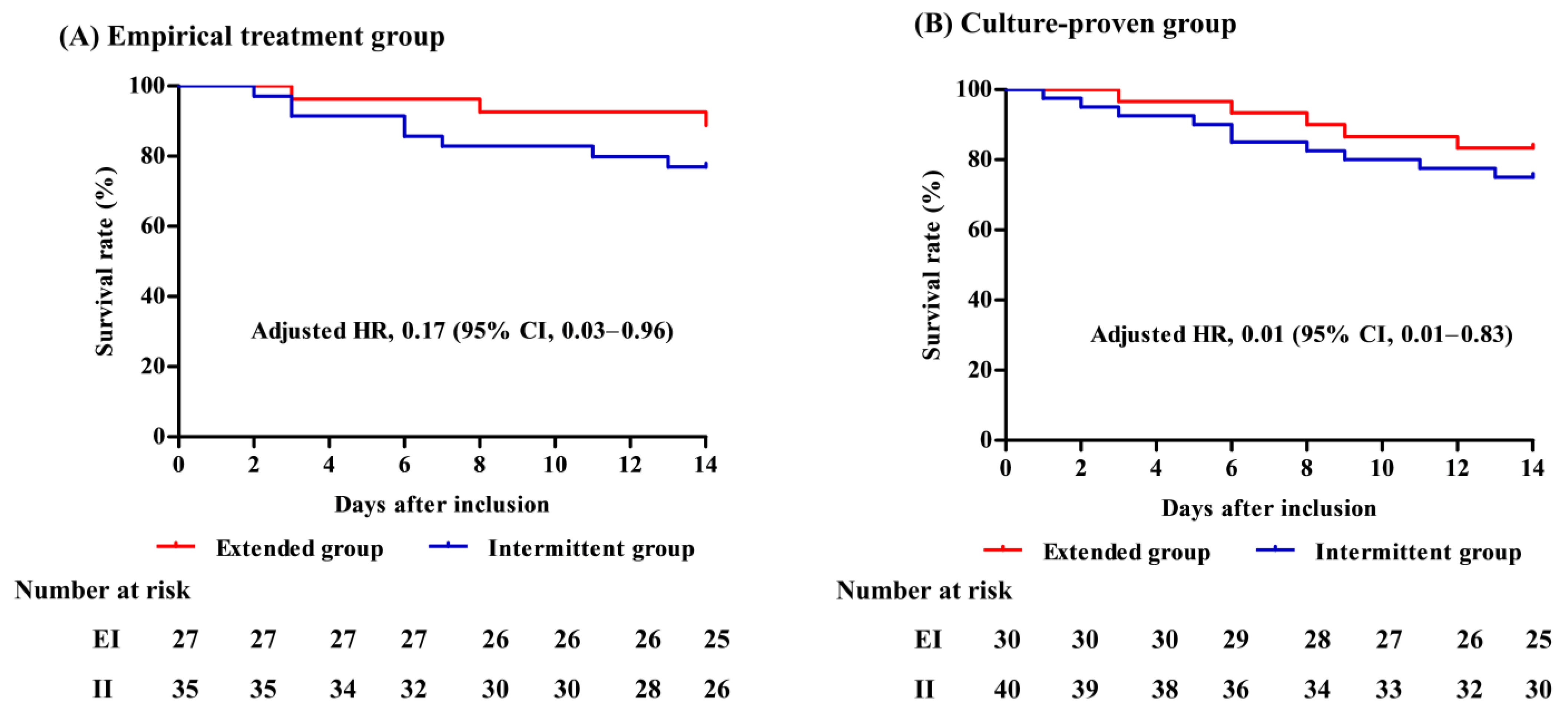
2.4. Subgroup Analysis
3. Discussion
4. Materials and Methods
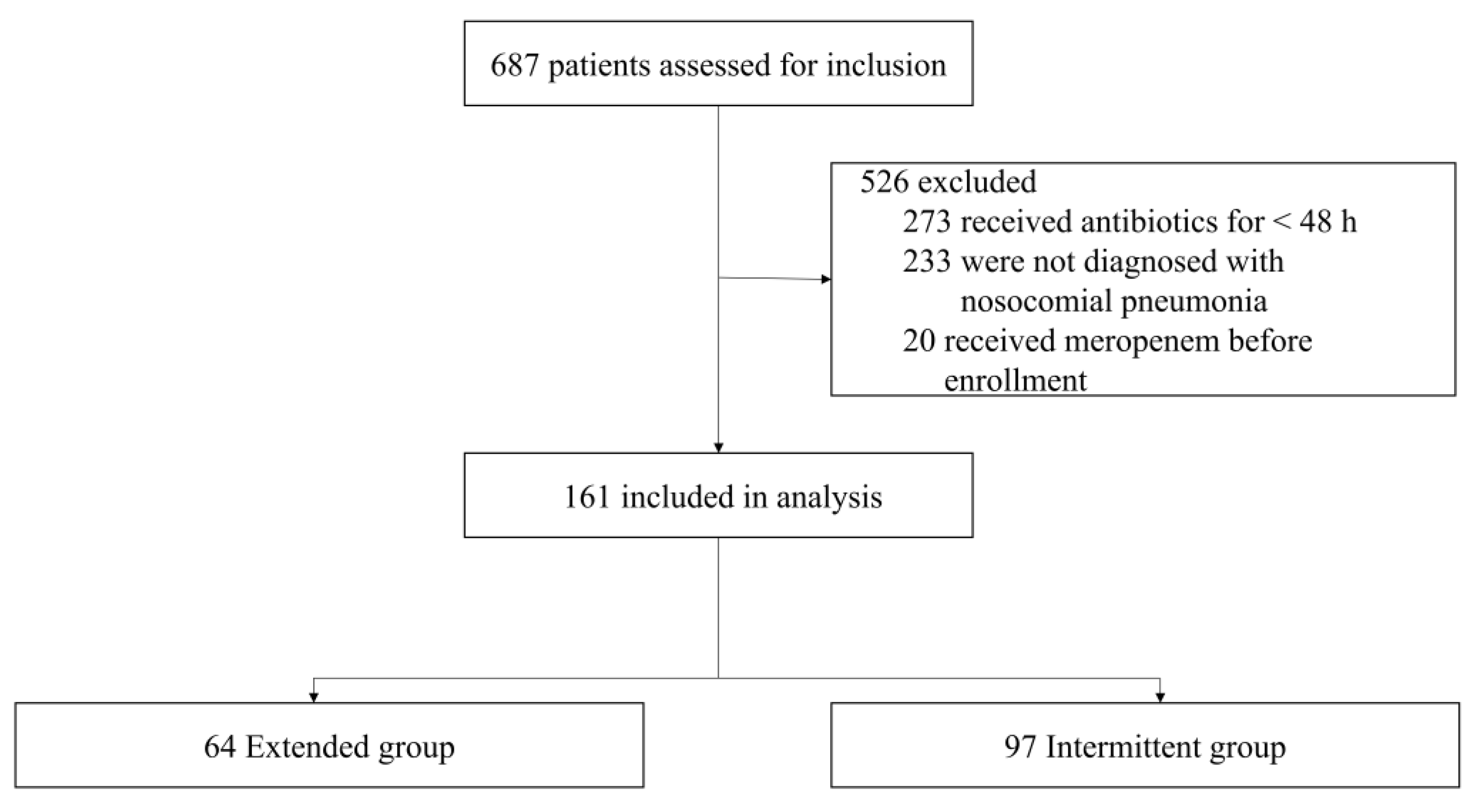
4.1. Study Design and Patients
4.2. Infusion of Meropenem
4.3. Data Collection and Outcomes
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Magill, S.S.; Edwards, J.R.; Bamberg, W.; Beldavs, Z.G.; Dumyati, G.; Kainer, M.A.; Lynfield, R.; Maloney, M.; McAllister-Hollod, L.; Nadle, J.; et al. Multistate point-prevalence survey of health care-associated infections. N. Engl. J. Med. 2014, 370, 1198–1208. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Welte, T.; Wunderink, R.G. Treatment of Gram-negative pneumonia in the critical care setting: Is the beta-lactam antibiotic backbone broken beyond repair? Crit. Care. 2016, 20, 19. [Google Scholar] [CrossRef] [PubMed]
- Koulenti, D.; Tsigou, E.; Rello, J. Nosocomial pneumonia in 27 ICUs in Europe: Perspectives from the EU-VAP/CAP study. Eur. J. Clin. Microbiol. Infect. Dis. 2017, 36, 1999–2006. [Google Scholar] [CrossRef] [PubMed]
- Chung, D.R.; Song, J.H.; Kim, S.H.; Thamlikitkul, V.; Huang, S.G.; Wang, H.; So, T.M.-K.; Yasin, R.M.D.; Hsueh, P.-R.; Carlos, C.C.; et al. High prevalence of multidrug-resistant nonfermenters in hospital-acquired pneumonia in Asia. Am. J. Respir. Crit. Care Med. 2011, 184, 1409–1417. [Google Scholar] [CrossRef] [PubMed]
- Ko, R.E.; Min, K.H.; Hong, S.B.; Baek, A.R.; Lee, H.K.; Cho, W.H.; Kim, C.; Chang, Y.; Lee, S.-S.; Oh, J.Y.; et al. Characteristics, Management, and Clinical Outcomes of Patients with Hospital-Acquired and Ventilator-Associated Pneumonia: A Multicenter Cohort Study in Korea. Tuberc. Respir. Dis. 2021, 84, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Poulakou, G.; Ruppe, E.; Bouza, E.; Van Hal, S.J.; Brink, A. Antimicrobial resistance in the next 30 years, humankind, bugs and drugs: A visionary approach. Intensive Care Med. 2017, 43, 1464–1475. [Google Scholar] [CrossRef] [PubMed]
- Kollef, M.H.; Bassetti, M.; Francois, B.; Burnham, J.; Dimopoulos, G.; Garnacho-Montero, J.; Lipman, J.; Luyt, C.E.; Nicolau, D.P.; Postma, M.J.; et al. The intensive care medicine research agenda on multidrug-resistant bacteria, antibiotics, and stewardship. Intensive Care Med. 2017, 43, 1187–1197. [Google Scholar] [CrossRef]
- Dhaese, S.A.M.; Hoste, E.A.; De Waele, J.J. Why We May Need Higher Doses of Beta-Lactam Antibiotics: Introducing the ‘Maximum Tolerable Dose’. Antibiotics 2022, 11, 889. [Google Scholar] [CrossRef]
- Póvoa, P.; Moniz, P.; Pereira, J.G.; Coelho, L. Optimizing Antimicrobial Drug Dosing in Critically Ill Patients. Microorganisms. 2021, 9, 1401. [Google Scholar] [CrossRef]
- Blot, S.I.; Pea, F.; Lipman, J. The effect of pathophysiology on pharmacokinetics in the critically ill patient–concepts appraised by the example of antimicrobial agents. Adv. Drug. Deliv. Rev. 2014, 77, 3–11. [Google Scholar] [CrossRef]
- Felton, T.W.; McCalman, K.; Malagon, I.; Isalska, B.; Whalley, S.; Goodwin, J.; Bentley, A.M.; Hope, W.W. Pulmonary penetration of piperacillin and tazobactam in critically ill patients. Clin. Pharmacol. Ther. 2014, 96, 438–448. [Google Scholar] [CrossRef]
- Rodvold, K.A.; Hope, W.W.; Boyd, S.E. Considerations for effect site pharmacokinetics to estimate drug exposure: Concentrations of antibiotics in the lung. Curr. Opin. Pharmacol. 2017, 36, 114–123. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.A.; Paul, S.K.; Akova, M.; Bassetti, M.; De Waele, J.J.; Dimopoulos, G.; Kaukonen, K.M.; Koulenti, D.; Martin, C.; Montravers, P.; et al. DALI: Defining antibiotic levels in intensive care unit patients: Are current β-lactam antibiotic doses sufficient for critically ill patients? Clin. Infect. Dis. 2014, 58, 1072–1083. [Google Scholar] [CrossRef]
- Taccone, F.S.; Laterre, P.-F.; Dugernier, T.; Spapen, H.; Delattre, I.; Witebolle, X.; De Backer, D.; Layeux, B.; Wallemacq, P.; Vincent, J.-L.; et al. Insufficient β-lactam concentrations in the early phase of severe sepsis and septic shock. Crit. Care. 2010, 14, R126. [Google Scholar] [CrossRef] [PubMed]
- Yu, Z.; Pang, X.; Wu, X.; Shan, C.; Jiang, S. Clinical outcomes of prolonged infusion (extended infusion or continuous infusion) versus intermittent bolus of meropenem in severe infection: A meta-analysis. PLoS ONE 2018, 13, e0201667. [Google Scholar] [CrossRef]
- Vardakas, K.Z.; Voulgaris, G.L.; Maliaros, A.; Samonis, G.; Falagas, M.E. Prolonged versus short-term intravenous infusion of antipseudomonal β-lactams for patients with sepsis: A systematic review and meta-analysis of randomised trials. Lancet Infect. Dis. 2018, 18, 108–120. [Google Scholar] [CrossRef] [PubMed]
- Kondo, Y.; Ota, K.; Imura, H.; Hara, N.; Shime, N. Prolonged versus intermittent β-lactam antibiotics intravenous infusion strategy in sepsis or septic shock patients: A systematic review with meta-analysis and trial sequential analysis of randomized trials. J. Intensive Care. 2020, 8, 77. [Google Scholar] [CrossRef]
- Drwiega, E.N.; Rodvold, K.A. Penetration of Antibacterial Agents into Pulmonary Epithelial Lining Fluid: An Update. Clin. Pharmacokinet. 2022, 61, 17–46. [Google Scholar] [CrossRef]
- Paal, M.; Scharf, C.; Denninger, A.K.; Ilia, L.; Kloft, C.; Kneidinger, N.; Liebchen, U.; Michel, S.; Schneider, C.; Schröpf, S.; et al. Target Site Pharmacokinetics of Meropenem: Measurement in Human Explanted Lung Tissue by Bronchoalveolar Lavage, Microdialysis, and Homogenized Lung Tissue. Antimicrob. Agents Chemother. 2021, 65, e0156421. [Google Scholar] [CrossRef]
- Frippiat, F.; Musuamba, F.T.; Seidel, L.; Albert, A.; Denooz, R.; Charlier, C.; Van Bambeke, F.; Wallemacq, P.; Descy, J.; Lambermont, B.; et al. Modelled target attainment after meropenem infusion in patients with severe nosocomial pneumonia: The PROMESSE study. J. Antimicrob Chemother. 2015, 70, 207–216. [Google Scholar] [CrossRef]
- Benítez-Cano, A.; Luque, S.; Sorlí, L.; Carazo, J.; Ramos, I.; Campillo, N.; Curull, V.; Sánchez-Font, A.; Vilaplana, C.; Horcajada, J.P.; et al. Intrapulmonary concentrations of meropenem administered by continuous infusion in critically ill patients with nosocomial pneumonia: A randomized pharmacokinetic trial. Crit. Care. 2020, 24, 55. [Google Scholar] [CrossRef] [PubMed]
- Del Bono, V.; Giacobbe, D.R.; Marchese, A.; Parisini, A.; Fucile, C.; Coppo, E.; Marini, V.; Arena, A.; Molin, A.; Martelli, A.; et al. Meropenem for treating KPC-producing Klebsiella pneumoniae bloodstream infections: Should we get to the PK/PD root of the paradox? Virulence 2017, 8, 66–73. [Google Scholar] [PubMed]
- Razzazzadeh, S.; Darazam, I.A.; Hajiesmaeili, M.; Salamzadeh, J.; Mahboubi, A.; Sadeghnezhad, E.; Sahraei, Z. Investigation of pharmacokinetic and clinical outcomes of various meropenem regimens in patients with ventilator-associated pneumonia and augmented renal clearance. Eur. J. Clin. Pharmacol. 2022, 78, 823–829. [Google Scholar] [CrossRef] [PubMed]
- Carrié, C.; Chadefaux, G.; Sauvage, N.; de Courson, H.; Petit, L.; Nouette-Gaulain, K.; Pereira, B.; Biais, M. Increased β-Lactams dosing regimens improve clinical outcome in critically ill patients with augmented renal clearance treated for a first episode of hospital or ventilator-acquired pneumonia: A before and after study. Crit. Care. 2019, 23, 379. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Mularoni, A.; Giacobbe, D.R.; Castaldo, N.; Vena, A. New Antibiotics for Hospital-Acquired Pneumonia and Ventilator-Associated Pneumonia. Semin. Respir. Crit. Care Med. 2022, 43, 280–294. [Google Scholar]
- Torres, A.; Zhong, N.; Pachl, J.; Timsit, J.F.; Kollef, M.; Chen, Z.; Song, J.; Taylor, D.; Laud, P.J.; Stone, G.G.; et al. Ceftazidime-avibactam versus meropenem in nosocomial pneumonia, including ventilator-associated pneumonia (REPROVE): A randomised, double-blind, phase 3 non-inferiority trial. Lancet Infect. Dis. 2018, 18, 285–295. [Google Scholar] [CrossRef] [PubMed]
- Kollef, M.H.; Nováček, M.; Kivistik, Ü.; Réa-Neto, Á.; Shime, N.; Martin-Loeches, I.; Timsit, J.-F.; Wunderink, R.G.; Bruno, C.J.; Huntington, J.A.; et al. Ceftolozane-tazobactam versus meropenem for treatment of nosocomial pneumonia (ASPECT-NP): A randomised, controlled, double-blind, phase 3, non-inferiority trial. Lancet Infect. Dis. 2019, 19, 1299–1311. [Google Scholar] [PubMed]
- Wunderink, R.G.; Matsunaga, Y.; Ariyasu, M.; Clevenbergh, P.; Echols, R.; Kaye, K.S.; Kollef, M.; Menon, A.; Pogue, J.M.; Shorr, A.F.; et al. Cefiderocol versus high-dose, extended-infusion meropenem for the treatment of Gram-negative nosocomial pneumonia (APEKS-NP): A randomised, double-blind, phase 3, non-inferiority trial. Lancet Infect. Dis. 2021, 21, 213–225. [Google Scholar] [CrossRef] [PubMed]
- Tamma, P.D.; Beisken, S.; Bergman, Y.; Posch, A.E.; Avdic, E.; Sharara, S.L.; Cosgrove, S.E.; Simner, P.J. Modifiable Risk Factors for the Emergence of Ceftolozane-tazobactam Resistance. Clin. Infect. Dis. 2021, 73, e4599–e4606. [Google Scholar] [CrossRef]
- Sid Ahmed, M.A.; Khan, F.A.; Hadi, H.A.; Skariah, S.; Sultan, A.A.; Salam, A.; Al Khal, A.L.; Söderquist, B.; Ibrahim, E.B.; Omrani, A.S.; et al. Association of bla(VIM-2), bla(PDC-35), bla(OXA-10), bla(OXA-488) and bla(VEB-9) β-Lactamase Genes with Resistance to Ceftazidime-Avibactam and Ceftolozane-Tazobactam in Multidrug-Resistant Pseudomonas aeruginosa. Antibiotics 2022, 11, 130. [Google Scholar]
- Roberts, J.A.; Roger, C.; De Waele, J.J. Personalized antibiotic dosing for the critically ill. Intensive Care Med. 2019, 45, 715–718. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Shan, T.; Liu, Y.; Ding, S.; Li, C.; Zhai, Q.; Du, B.; Li, Y.; Zhang, J.; Wang, H.; et al. Comparison of 3-hour and 30-minute infusion regimens for meropenem in patients with hospital acquired pneumonia in intensive care unit: A randomized controlled clinical trial. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue 2014, 26, 644–649. [Google Scholar] [PubMed]
- Giacomo, M.; Nikola, B.; Matteo, M.; Aidos, K.; Evgeny, F.; Yuki, K.; Likhvantsev, V.V.; Momesso, E.; Nogtev, P.; Lobreglio, R.; et al. Continuous vs Intermittent Meropenem Administration in Critically Ill Patients With Sepsis: The MERCY Randomized Clinical Trial. JAMA. 2023, 330, L141–L151. [Google Scholar]
- Yang, N.; Wang, J.; Xie, Y.; Ding, J.; Wu, C.; Liu, J.; Pei, Q. External Evaluation of Population Pharmacokinetic Models to Inform Precision Dosing of Meropenem in Critically Ill Patients. Front. Pharmacol. 2022, 13, 838205. [Google Scholar] [CrossRef] [PubMed]
- Imani, S.; Buscher, H.; Marriott, D.; Gentili, S.; Sandaradura, I. Too much of a good thing: A retrospective study of β-lactam concentration-toxicity relationships. J. Antimicrob. Chemother. 2017, 72, 2891–2897. [Google Scholar] [CrossRef] [PubMed]
- An, G.; Creech, C.B.; Wu, N.; Nation, R.L.; Gu, K.; Nalbant, D.; Jimenez-Truque, N.; Fissell, W.; Rolsma, S.; Patel, P.C.; et al. Evaluation of Empirical Dosing Regimens for Meropenem in Intensive Care Unit Patients Using Population Pharmacokinetic Modeling and Target Attainment Analysis. Antimicrob. Agents Chemother. 2023, 67, e0131222. [Google Scholar] [CrossRef]
- Iovleva, A.; Doi, Y. Carbapenem-Resistant Enterobacteriaceae. Clin. Lab. Med. 2017, 37, 303–315. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variable | Extended (n = 64) | Intermittent (n = 97) | p-Value |
|---|---|---|---|
| Age, y | 62.4 ± 14.1 | 64.7 ± 12.0 | 0.255 |
| Sex, male | 42 (65.6) | 75 (77.3) | 0.103 |
| BMI, kg/m2 | 22.9 (19.9–24.8) | 22.1 (19.2–24.5) | 0.111 |
| Comorbidity | |||
| Diabetes mellitus | 17 (26.6) | 31 (32.0) | 0.464 |
| Solid cancer | 13 (20.3) | 26 (26.8) | 0.347 |
| Hematologic malignancy | 16 (25.0) | 17 (17.5) | 0.250 |
| Congestive heart failure | 8 (12.5) | 5 (5.2) | 0.094 |
| Respiratory failure | 17 (26.6) | 20 (20.6) | 0.380 |
| Chronic liver disease | 7 (10.9) | 14 (14.4) | 0.519 |
| End-stage renal disease | 9 (14.1) | 12 (12.4) | 0.755 |
| Immunocompromised | 22 (34.4) | 25 (25.8) | 0.240 |
| Severity of pneumonia | |||
| SOFA score | 10.0 (6.3–12.0) | 10.0 (8.0–13.0) | 0.237 |
| Sepsis | 61 (95.3) | 92 (94.8) | 1.000 |
| Septic shock | 12 (18.8) | 33 (34.0) | 0.035 |
| PaO2/FiO2 ratio, mmHg (n = 157) | 212.3 ± 98.5 | 201.2 ± 133.2 | 0.573 |
| Type of nosocomial pneumonia | 0.854 | ||
| Hospital-acquired pneumonia | 38 (59.4) | 59 (60.8) | |
| Ventilator-associated pneumonia | 26 (40.6) | 38 (39.2) | |
| Parameters of antibiotics | |||
| Duration of meropenem, days | 9.0 (5.3–13.0) | 7.0 (5.0–11.0) | 0.165 |
| Duration of antibiotic, days | 17.0 (8.3–22.0) | 13.0 (7.0–23.5) | 0.357 |
| Discontinuation during ICU stay (n = 143) | 0.135 | ||
| De-escalation or cessation | 42 (73.7) | 53 (61.6) | |
| Escalation or death | 15 (26.3) | 33 (38.4) | |
| Previous antibiotics | |||
| Class of beta-lactam | 36 (56.3) | 66 (68.0) | 0.137 |
| Class of quinolone | 18 (28.1) | 32 (33.0) | 0.514 |
| Class of glycopeptide | 11 (17.2) | 21 (21.6) | 0.487 |
| Concomitant antibiotics | |||
| Use of colistin | 8 (12.5) | 13 (13.4) | 0.868 |
| Use of quinolone | 24 (37.5) | 40 (41.2) | 0.742 |
| Use of others * | 5 (7.8) | 7 (7.2) | 1.000 |
| Coverage for MRSA | 43 (67.2) | 64 (66.0) | 0.874 |
| Laboratory variables | |||
| White cell count, ×103/L | 10.9 ± 8.7 | 13.2 ± 9.3 | 0.112 |
| C-reactive protein, mg/dL (n = 158) | 10.5 ± 8.4 | 12.4 ± 8.8 | 0.182 |
| Organ support at baseline | |||
| Mechanical ventilation | 57 (89.1) | 90 (92.8) | 0.412 |
| Renal replacement therapy | 17 (26.6) | 19 (19.6) | 0.299 |
| Extracorporeal membrane oxygenation | 9 (14.1) | 12 (12.4) | 0.755 |
| Vasopressors | 41 (64.1) | 59 (60.8) | 0.679 |
| Variable | Extended (n = 64) | Intermittent (n = 97) | p-Value |
|---|---|---|---|
| Bacteremia | 8 (12.5) | 5 (5.2) | 0.094 |
| Staphylococcus aureus | 3 (37.5) | 0 (0.0) | |
| Enterococcus faecium | 3 (37.5) | 0 (0.0) | |
| Klebsiella pneumoniae | 2 (25.0) | 0 (0.0) | |
| Pseudomonas aeruginosa | 0 (0.0) | 1 (20.0) | |
| Acinetobacter baumanii | 0 (0.0) | 4 (80.0) | |
| Pathogen of sputum culture | 37 (57.8) | 59 (60.8) | 0.744 |
| Gram(+) pathogen | 4 (6.3) | 6 (6.2) | 1.000 |
| Staphylococcus aureus | 3 (75.0) | 3 (50.0) | |
| Staphylococcus haemolyticus | 1 (25.0) | 0 (0.0) | |
| Corynebacterium striatum | 0 (0.0) | 3 (50.0) | |
| Gram(−) pathogen | 25 (39.1) | 45 (46.4) | 0.418 |
| Escherichia coli | 1 (4.0) | 1 (2.2) | |
| Klebsiella pneumoniae or oxytica | 7 (28.0) | 10 (22.2) | |
| Pseudomonas aeruginosa | 7 (28.0) | 11 (24.4) | |
| Acinetobacter baumannii or iwoffii | 10 (40.0) | 21 (46.7) | |
| Stenotrophomonas maltophilia | 1 (4.0) | 5 (11.1) | |
| Serratia marcescens | 0 (0.0) | 1 (2.2) | |
| CRE | 13 (20.3) | 28 (28.9) | 0.223 |
| CRAB | 7 (10.9) | 21 (21.6) | 0.092 |
| CRPA | 6 (9.4) | 4 (4.1) | 0.197 |
| CPE | 0 (0.0) | 4 (4.1) * | 0.152 |
| MIC distribution ofmeropenem (n = 70) | 0.796 | ||
| ≤1 mg/L | 10 (40.0) | 15 (33.3) | |
| 2–4 mg/L | 2 (8.0) | 3 (6.7) | |
| >4 mg/L | 13 (52.0) | 27 (60.0) | |
| Other pathogens ** | 9 (14.1) | 6 (6.2) | 0.104 |
| Outcome Measure | Extended (n = 64) | Intermittent (n = 97) | p-Value |
|---|---|---|---|
| Mortality | |||
| 14-day mortality | 10 (15.6) | 22 (22.7) | 0.272 |
| 28-day mortality | 16 (25.0) | 29 (29.9) | 0.498 |
| ICU mortality | 21 (32.8) | 40 (41.2) | 0.281 |
| LOS, median (IQR) | |||
| Hospital days | 79.9 ± 76.8 | 81.3 ± 71.7 | 0.906 |
| ICU days | 26.5 ± 35.6 | 20.5 ± 18.2 | 0.223 |
| Ventilator days (n = 146) | 24.8 ± 37.7 | 18.5 ± 17.3 | 0.243 |
| Improvement of CRP level (n = 158) | 41 (65.1) | 61 (64.2) | 1.000 |
| Occurrence of carbapenem resistance (n = 112) | 11 (24.4) | 18 (26.9) | 0.829 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hyun, D.-g.; Seo, J.; Lee, S.Y.; Ahn, J.H.; Hong, S.-B.; Lim, C.-M.; Koh, Y.; Huh, J.W. Extended Versus Intermittent Meropenem Infusion in the Treatment of Nosocomial Pneumonia: A Retrospective Single-Center Study. Antibiotics 2023, 12, 1542. https://doi.org/10.3390/antibiotics12101542
Hyun D-g, Seo J, Lee SY, Ahn JH, Hong S-B, Lim C-M, Koh Y, Huh JW. Extended Versus Intermittent Meropenem Infusion in the Treatment of Nosocomial Pneumonia: A Retrospective Single-Center Study. Antibiotics. 2023; 12(10):1542. https://doi.org/10.3390/antibiotics12101542
Chicago/Turabian StyleHyun, Dong-gon, Jarim Seo, Su Yeon Lee, Jee Hwan Ahn, Sang-Bum Hong, Chae-Man Lim, Younsuck Koh, and Jin Won Huh. 2023. "Extended Versus Intermittent Meropenem Infusion in the Treatment of Nosocomial Pneumonia: A Retrospective Single-Center Study" Antibiotics 12, no. 10: 1542. https://doi.org/10.3390/antibiotics12101542
APA StyleHyun, D.-g., Seo, J., Lee, S. Y., Ahn, J. H., Hong, S.-B., Lim, C.-M., Koh, Y., & Huh, J. W. (2023). Extended Versus Intermittent Meropenem Infusion in the Treatment of Nosocomial Pneumonia: A Retrospective Single-Center Study. Antibiotics, 12(10), 1542. https://doi.org/10.3390/antibiotics12101542