
Transinusal Pathway Removal of an Impacted Third Molar with an Unusual Approach: A Case Report and a Systematic Review of the Literature


 ,
, 
 and
and 
Abstract
:1. Introduction
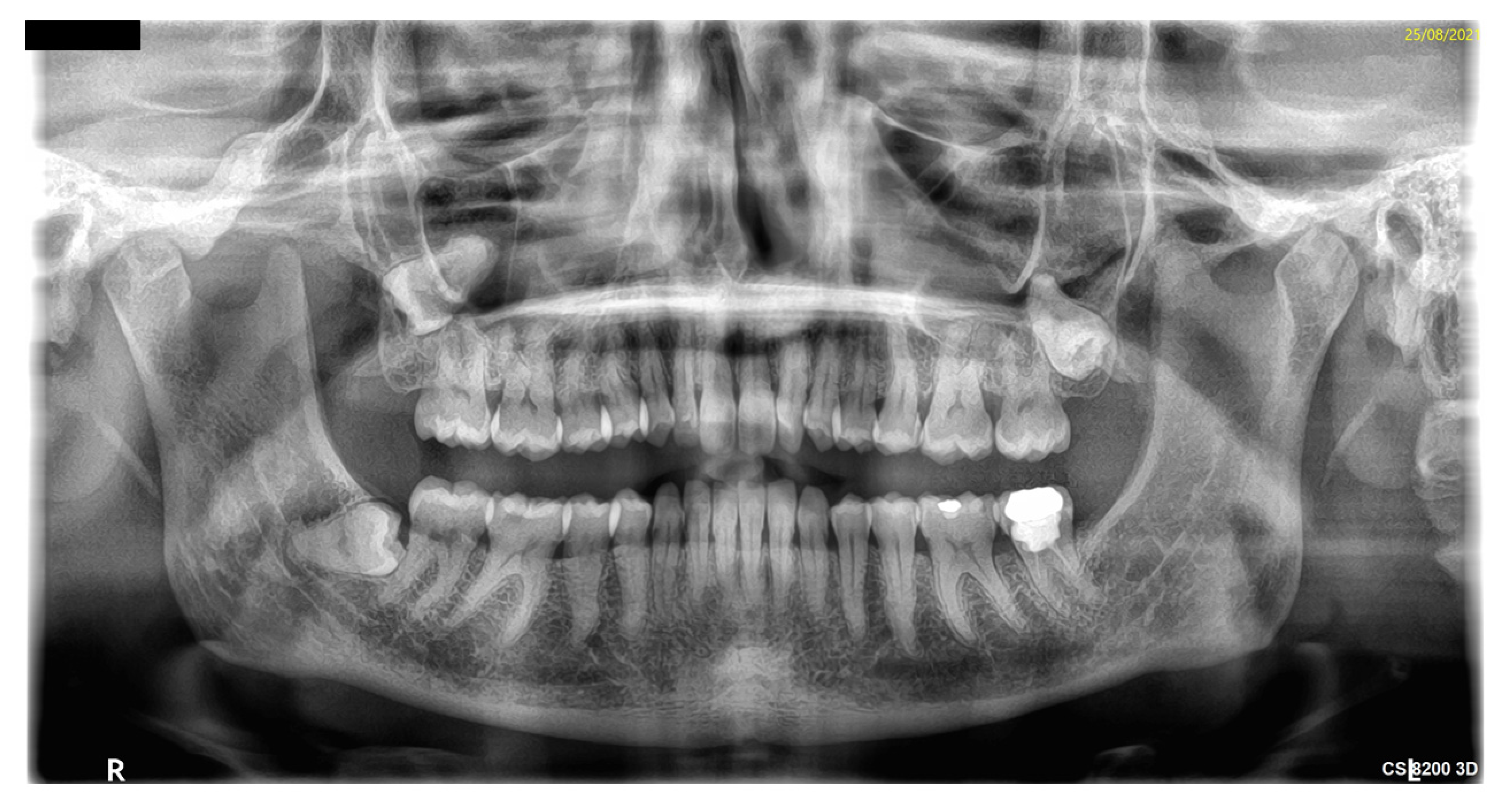
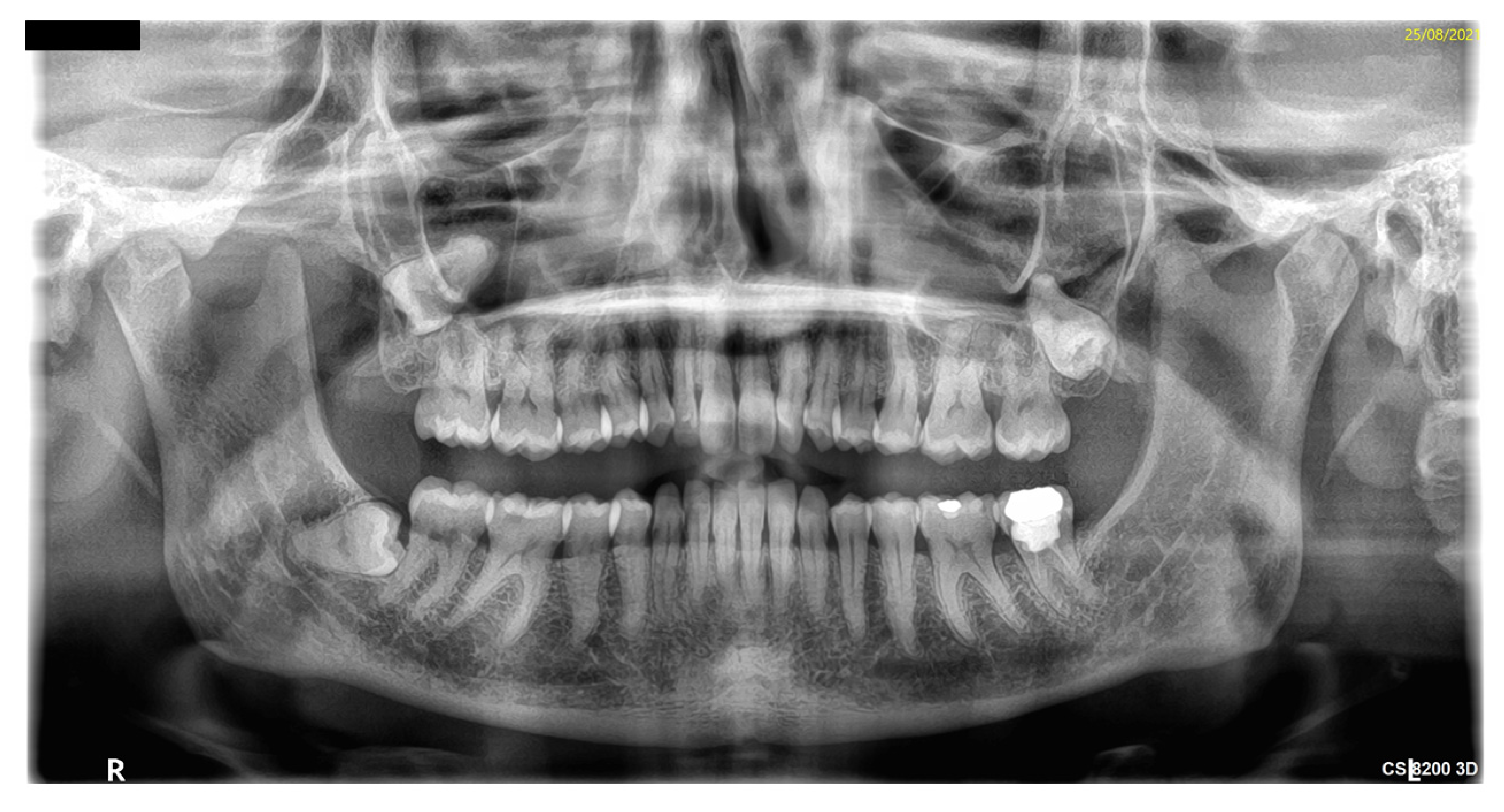
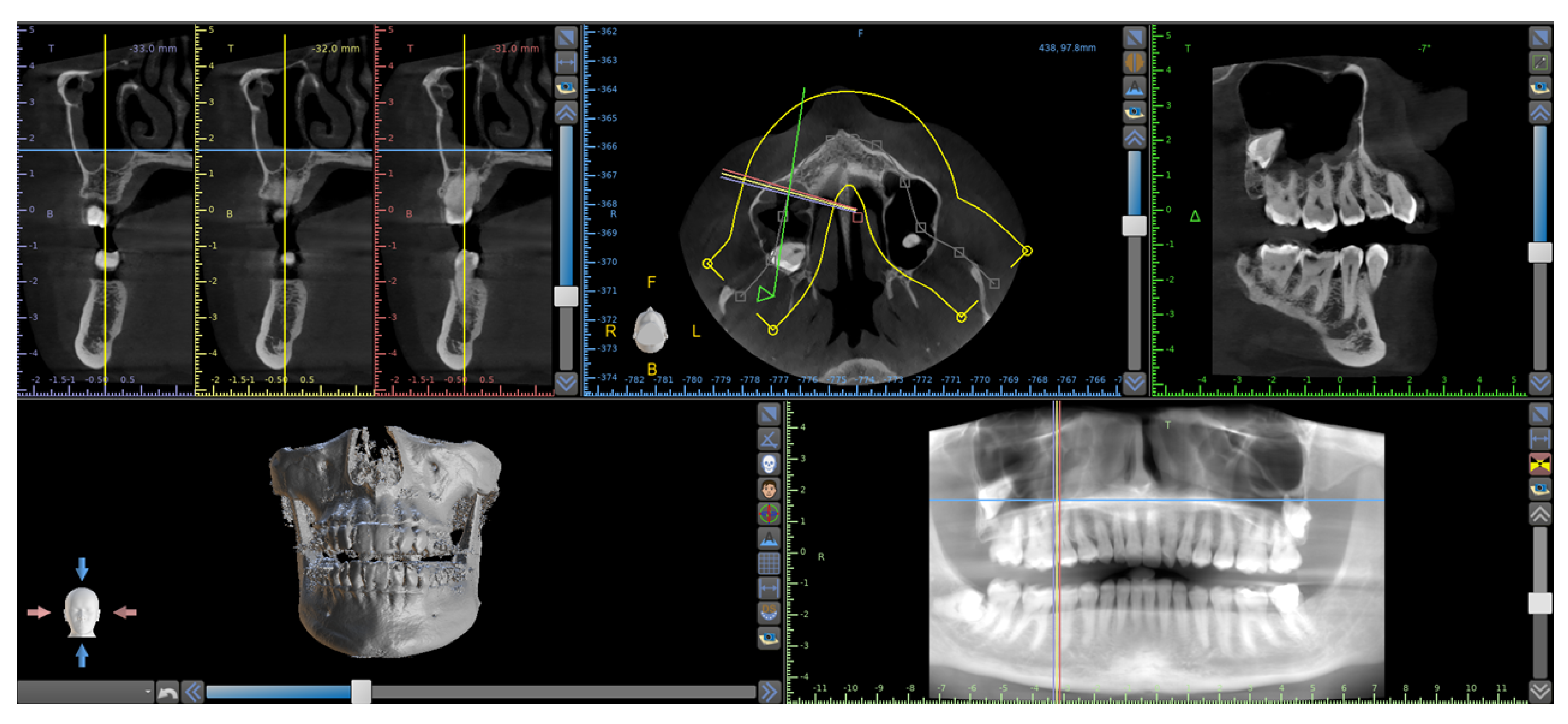
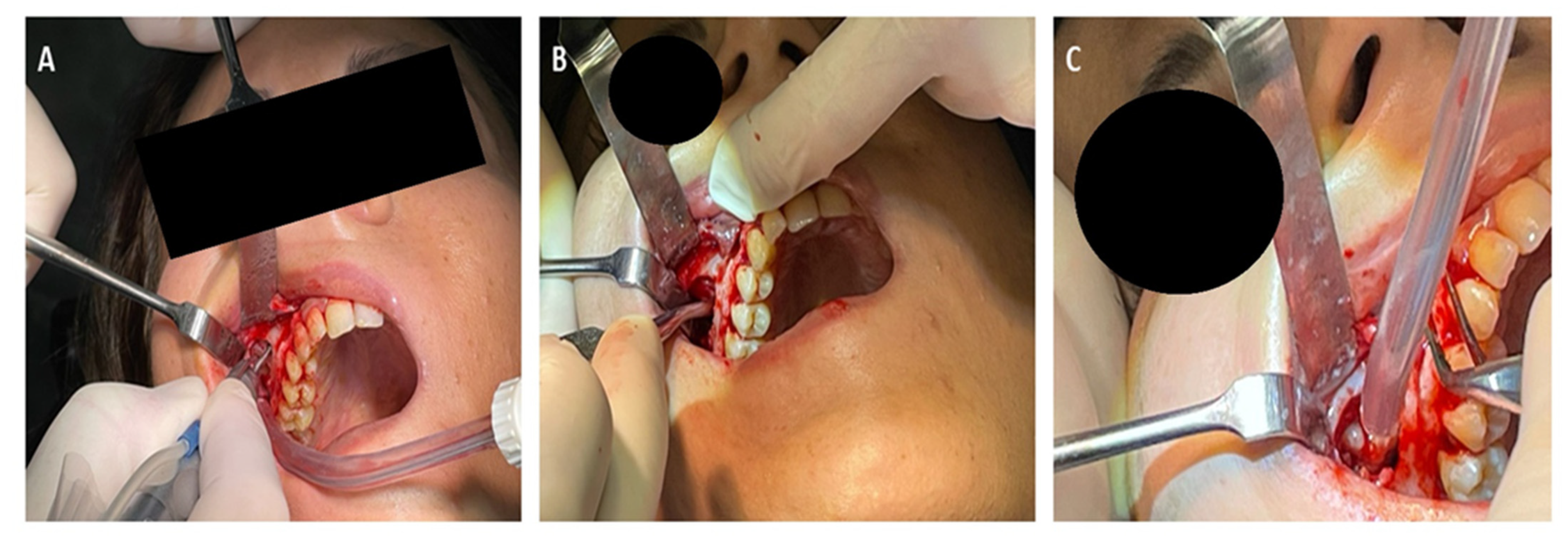
2. Case Report
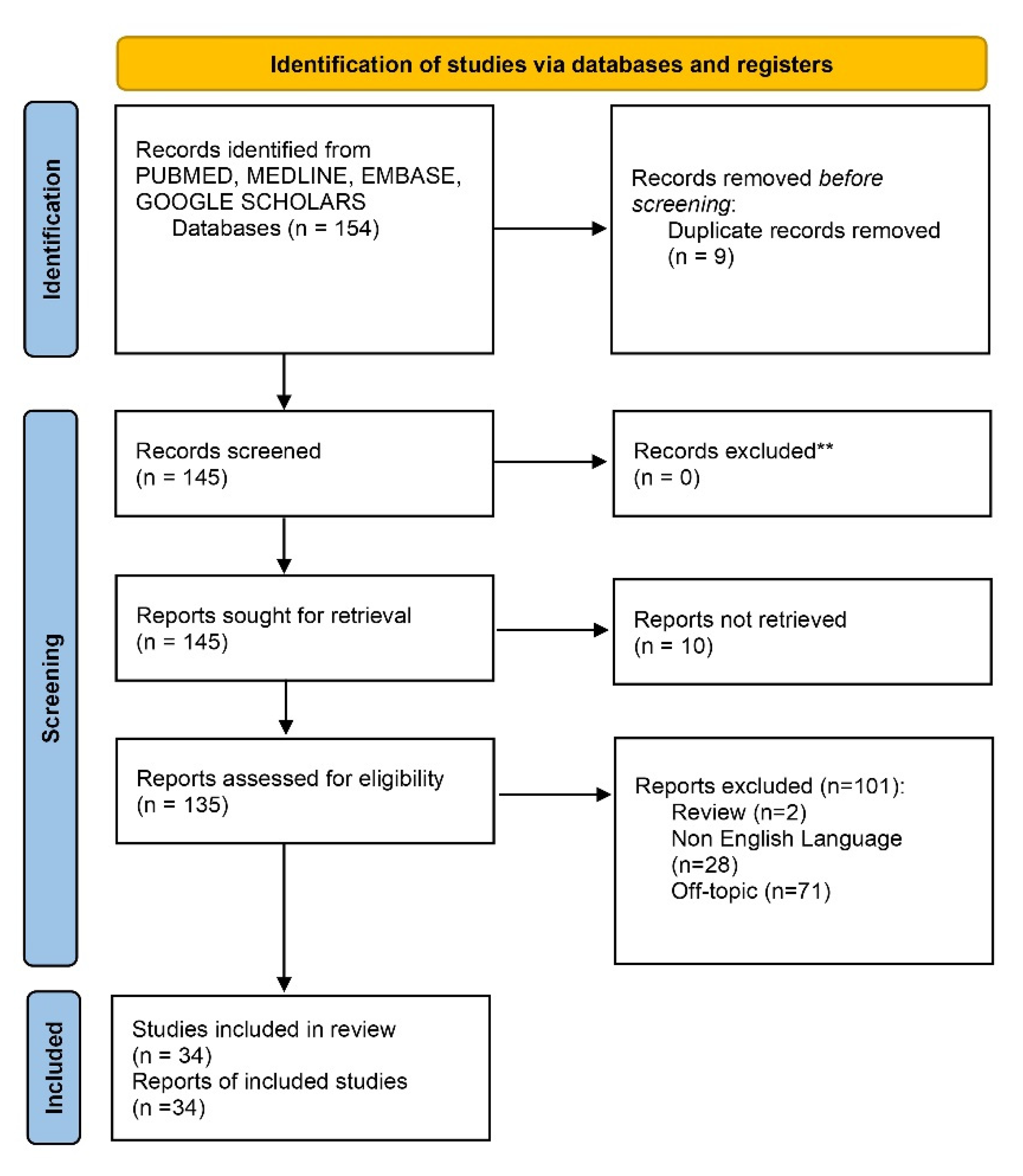
3. Systematic Review Methodology
3.1. Search Strategies
3.2. Inclusion and Exclusion Criteria
3.3. Article Identification Procedure
3.4. Study Assessment
4. Literature Review Results
4.1. Paper Selection: General Characteristics
4.2. Included Study Characteristics
4.3. Drug Administration Protocols
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Scarano, A.; De Oliveira, P.S.; Traini, T.; Lorusso, F. Sinus Membrane Elevation with Heterologous Cortical Lamina: A Randomized Study of a New Surgical Technique for Maxillary Sinus Floor Augmentation without Bone Graft. Materials 2018, 11, 1457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alhashim, F.Y.; Almarhoon, F.S.; Alhashim, H.Y.; Moumen, A. Endonasal endoscopic management of different cases of dentigerous cysts and ectopic teeth. J. Surg. Case Rep. 2021, 4, rjab099. [Google Scholar] [CrossRef] [PubMed]
- Nogami, S.; Yamauchi, K.; Tanuma, Y.; Odashima, K.; Matsui, A.; Tanaka, K.; Takahashi, T. Removal of dental implant displaced into maxillary sinus by combination of endoscopically assisted and bone repositioning techniques: A case report. J. Med Case Rep. 2016, 10, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewusz-Butkiewicz, K.; Kaczor, K.; Nowicka, A. Risk factors in oroantral communication while extracting the upper third molar: Systematic review. Dent. Med. Probl. 2018, 55, 69–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanj, W.; Wayzani, N.; Aoun, G.; Berberi, A. Maxillary Third Molar Tooth Accidentally Displaced in Buccal Space: Two Cases Report. J. Dent. 2021, 22, 308–311. [Google Scholar] [CrossRef]
- Sencimen, M.; Gülses, A.; Secer, S.; Zerener, T.; Özarslantürk, S. Delayed retrieval of a displaced maxillary third molar from infratemporal space via trans-sinusoidal approach: A case report and the review of the literature. Oral Maxillofac. Surg. 2016, 21, 1–6. [Google Scholar] [CrossRef]
- Supplement, D.; Candotto, V.; Oberti, L.; Gabrione, F.; Scarano, A.; Rossi, D.; Romano, M. Complication in third molar extractions. J. Biol. Regul. Homeost Agents 2019, 33, 169–172. [Google Scholar]
- Association, W.M. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [Google Scholar]
- Agha, R.A.; Franchi, T.; Sohrabi, C.; Mathew, G.; Kerwan, A.; Thoma, A.; Beamish, A.J.; Noureldin, A.; Rao, A.; Vasudevan, B.; et al. The SCARE 2020 Guideline: Updating Consensus Surgical CAse REport (SCARE) Guidelines. Int. J. Surg. 2020, 84, 226–230. [Google Scholar] [CrossRef]
- Scarano, A.; Lorusso, F.; Arcangelo, M.; D’Arcangelo, C.; Celletti, R.; De Oliveira, P.S. Lateral Sinus Floor Elevation Performed with Trapezoidal and Modified Triangular Flap Designs: A Randomized Pilot Study of Post-Operative Pain Using Thermal Infrared Imaging. Int. J. Environ. Res. Public Health 2018, 15, 1277. [Google Scholar] [CrossRef] [Green Version]
- Scarano, A.; Barros, R.R.; Iezzi, G.; Piattelli, A.; Novaes, A.B., Jr. Acellular Dermal Matrix Graft for Gingival Augmentation: A Preliminary Clinical, Histologic, and Ultrastructural Evaluation. J. Periodontol. 2009, 80, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Piattelli, A.; Polimeni, A.; Di Iorio, D.; Carinci, F. Bacterial Adhesion on Commercially Pure Titanium and Anatase-Coated Titanium Healing Screws: An In Vivo Human Study. J. Periodontol. 2010, 81, 1466–1471. [Google Scholar] [CrossRef] [PubMed]
- Masalha, M.; Schneider, S.; Kassem, F.; Koren, I.; Eliashar, R.; Margulis, A.; Landsberg, R. Endoscopic treatment of ectopic teeth in the maxillary sinus. J. Clin. Exp. Dent. 2021, 13, e227–e233. [Google Scholar] [CrossRef] [PubMed]
- Allen, D.Z.; Sethia, R.; Hamersley, E.A.; Elmaraghy, C. Presentation of an iatrogenically displaced third molar into the maxillary sinus in a 14-year-old patient successfully removed with an endoscopic approach: A case report and a review of the literature. J. Surg. Case Rep. 2020, 10, rjaa290. [Google Scholar] [CrossRef]
- Yagiz, A.; Ünsal, G. Ghost image of an ectopic tooth in maxillary sinus: A diagnostic challenge. J. Stomatol. Oral Maxillofac. Surg. 2020, 122, 112–114. [Google Scholar] [CrossRef]
- Balaji, S.M.; Balaji, P. Impacted wisdom tooth in the floor of the orbit. Indian J. Dent. Res. 2020, 31, 312–314. [Google Scholar] [CrossRef]
- Liu, J.; Zhou, M.; Liu, Q.; He, X.; Wang, N. Process of ectopic tooth formation in the maxillary sinus: Follow-up observation of one case. J. Int. Med. Res. 2019, 47, 6356–6364. [Google Scholar] [CrossRef] [Green Version]
- Lai, Y.-T.A.; Luk, Y.S.; Fung, K.-H. Anomalous Morphology of an Ectopic Tooth in the Maxillary Sinus on Three-Dimensional Computed Tomography Images. J. Radiol. Case Rep. 2013, 7, 11–16. [Google Scholar] [CrossRef]
- Viterbo, S.; Griffa, A.; Boffano, P. Endoscopic Removal of an Ectopic Tooth in Maxillary Sinus. J. Craniofacial Surg. 2013, 24, e46–e48. [Google Scholar] [CrossRef]
- Capelli, M.; Lombroni, L.; Farronato, G.; Santamaria, G.; Lombroni, D.; Gatti, P. Ectopic teeth in the maxillary sinus: A case report and literature review. Indian J. Dent. Res. 2018, 29, 667. [Google Scholar] [CrossRef]
- Liau, I.; Lynch, N.; Hearn, B.; Cheng, A. Endoscopically Assisted Modified Caldwell-Luc Approach to Enucleation of Dentigerous Cyst with Ectopic Tooth from the Maxillary Sinus. J. Craniofacial Surg. 2018, 29, e568–e570. [Google Scholar] [CrossRef] [PubMed]
- Datli, A.; Pilanci, O.; Cortuk, O.; Saglam, O.; Kuvat, S.V. Ectopic Tooth Superiorly Located in the Maxillary Sinus. J. Craniofacial Surg. 2014, 25, 1927–1928. [Google Scholar] [CrossRef] [PubMed]
- Rai, A.; Rai, N.; Rai, M.; Jain, G. Transoral removal of ectopic maxillary third molar situated superiorly to maxillary antrum and posteroinferiorly to the floor of orbit. Indian J. Dent. Res. 2013, 24, 756. [Google Scholar] [CrossRef] [PubMed]
- Kara, M.I.; Yanik, S.; Altan, A.; Oznalcin, O.; Ay, S. Large dentigerous cyst in the maxillary sinus leading to diplopia and nasal obstruction: Case report. J. Istanb. Univ. Fac. Dent. 2015, 49, 46–50. [Google Scholar] [CrossRef]
- Touiheme, N.; Messary, A. Supernumerary ectopic tooth on the maxillary sinus. Pan Afr. Med J. 2014, 18, 353. [Google Scholar] [CrossRef]
- Júnior, O.L.C.; Moura, L.B.; Sonego, C.L.; de Farias, E.O.C.; Giongo, C.C.; Fonseca, A.A.R. Unusual Case of Sinusitis Related to Ectopic Teeth in the Maxillary Sinus Roof/Orbital Floor: A Report. Craniomaxillofacial Trauma Reconstr. 2016, 9, 260–263. [Google Scholar] [CrossRef] [Green Version]
- Saleem, T.; Khalid, U.; Hameed, A.; Ghaffar, S. Supernumerary, ectopic tooth in the maxillary antrum presenting with recurrent haemoptysis. Head Face Med. 2010, 6, 26. [Google Scholar] [CrossRef] [Green Version]
- Topal, O.; Dayisoylu, E.H. Ectopic Tooth in the Maxillary Sinus. Turk. Arch. Otorhinolaryngol. 2017, 55, 151–152. [Google Scholar] [CrossRef] [Green Version]
- El-Fattah, A.M.A.; Khafagy, Y.W.; El-Sisi, H.; Elkahwagi, M.; Ebada, H.A. Ectopic maxillary sinus third molar with dentigerous cyst in 11 patients: Tailored endoscopic-assisted approaches for a successful outcome. Clin. Otolaryngol. 2021, 46, 1095–1099. [Google Scholar] [CrossRef]
- Guruprasad, Y.; Chauhan, D.S.; Kura, U. Infected Dentigerous Cyst of Maxillary Sinus Arising from an Ectopic Third Molar. J. Clin. Imaging Sci. 2013, 3, 7. [Google Scholar] [CrossRef]
- Di Felice, R.; Lombardi, T. Ectopic third molar in the maxillary sinus. Case Report. Aust. Dent. J. 1995, 40, 236–237. [Google Scholar] [CrossRef] [PubMed]
- Kasat, V.O.; Karjodkar, F.R.; Laddha, R.S. Dentigerous cyst associated with an ectopic third molar in the maxillary sinus: A case report and review of literature. Contemp. Clin. Dent. 2012, 3, 373–376. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Chauhan, J.S. Bilateral ectopic third molars in maxillary sinus associated with dentigerous cyst—A rare case report. Int. J. Surg. Case Rep. 2019, 61, 298–301. [Google Scholar] [CrossRef] [PubMed]
- Jendi, S.K. Ectopic Third Molar: A Hidden Cause for Maxillary Sinusitis—A Rare Case Report. Indian J. Otolaryngol. Head Neck Surg. 2019, 71, 831–834. [Google Scholar] [CrossRef]
- Ramanojam, S.; Hebbale, M.; Bhardwaj, S.; Halli, R. Ectopic tooth in maxillary sinus: Case series. Ann. Maxillofac. Surg. 2013, 3, 89–92. [Google Scholar] [CrossRef]
- Mohan, S.; Harjani, B.; Kankariya, H.; Sharma, H. Ectopic third molar in the maxillary sinus. Natl. J. Maxillofac. Surg. 2011, 2, 222–224. [Google Scholar] [CrossRef] [Green Version]
- Thakur, G.; Nair, P.P.; Thomas, S.; Ahuja, R.; Kothari, R. Dentigerous cyst associated with ectopic maxillary third molar in maxillary antrum. BMJ Case Rep. 2011, 5, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Demirtas, N.; Kazancioglu, H.O.; Ezirganli, S. Ectopic Tooth in the Maxillary Sinus Diagnosed with an Ophthalmic Complication. J. Craniofacial Surg. 2014, 25, e351–e352. [Google Scholar] [CrossRef]
- Prasad, T.S.; Sujatha, G.; Niazi, T.M.; Rajesh, P. Dentigerous cyst associated with an ectopic third molar in the maxillary sinus: A rare entity. Indian J. Dent. Res. 2007, 18, 141–143. [Google Scholar] [CrossRef]
- AlKhudair, B.; AlKhatib, A.; AlAzzeh, G.; AlMomen, A. Bilateral dentigerous cysts and ectopic teeth in the maxillary sinuses: A case report and literature review. Int. J. Surg. Case Rep. 2019, 55, 117–120. [Google Scholar] [CrossRef]
- Aydin, U.; Asik, B.; Ahmedov, A.; Durmaz, A. Osteoma and Ectopic Tooth of the Left Maxillary Sinus: A Unique Coexistence. Balk. Med. J. 2016, 33, 473–476. [Google Scholar] [CrossRef] [PubMed]
- AlMomen, A.; Alkhudair, B.; Alkhatib, A.; Alazzah, G.; Ali, Z.; Al Yaeesh, I.; AlOmairin, A.; Alshuaibi, A.; Albahr, A. Ectopic maxillary tooth as a cause of recurrent maxillary sinusitis: A case report and review of the literature. J. Surg. Case Rep. 2020, 9, rjaa334. [Google Scholar] [CrossRef] [PubMed]
- Buyukkurt, M.; Omezli, M.; Miloglu, O. Dentigerous cyst associated with an ectopic tooth in the maxillary sinus: A report of 3 cases and review of the literature. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2010, 109, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Bodner, L.; Tovi, F.; Bar-Ziv, J. Teeth in the maxillary sinus—Imaging and management. J. Laryngol. Otol. 1997, 111, 820–824. [Google Scholar] [CrossRef]
- Baykul, T.; Doğru, H.; Yasan, H.; Aksoy, M. Clinical impact of ectopic teeth in the maxillary sinus. Auris Nasus Larynx 2006, 33, 277–281. [Google Scholar] [CrossRef]
- Elmorsy, K.; Elsayed, L.K.; El Khateeb, S.M. Case Report: Ectopic third molar in the maxillary sinus with infected dentigerous cyst assessed by cone beam CT. F1000Research 2020, 9, 209. [Google Scholar] [CrossRef]
- Schimmel, M.; Srinivasan, M.; McKenna, G.; Müller, F. Effect of advanced age and/or systemic medical conditions on dental implant survival: A systematic review and meta-analysis. Clin. Oral Implant. Res. 2018, 29, 311–330. [Google Scholar] [CrossRef] [Green Version]
- Trybek, G.; Jaroń, A.; Grzywacz, A. Association of Polymorphic and Haplotype Variants of the MSX1 Gene and the Impacted Teeth Phenomenon. Genes 2021, 12, 577. [Google Scholar] [CrossRef]
- Vámos, D.; Ujpál, M.; Huszár, T.; Vaszilkó, M.; Németh, Z. Dentigerous cyst associated with a wisdom tooth in the maxillary sinus. Case reports, review of the literature. Fogorv. Sz. 2012, 105, 141–146. [Google Scholar]
- Hsu, C.-C.; Lee, L.-C.; Kuo, B.-I.; Lee, C.-J.; Liu, F.-Y. Surgical and Anatomic Consideration in Endoscopic Dacryocystorhinostomy of a Patient with Damaged Sinonasal Anatomy Post–Caldwell-Luc Surgery: A Case Report. Medicina 2022, 58, 78. [Google Scholar] [CrossRef]
- Yang, P.; Liang, H.; Zou, B.; Liu, J.; Yuan, D.; Meng, Z.; Xu, K. Ectopic tooth in maxillary sinus compressing the nasolacrimal canal. Medicine 2021, 100, e25514. [Google Scholar] [CrossRef] [PubMed]
- Findik, Y.; Baykul, T.; Fındık, Y. Ectopic third molar in the mandibular sigmoid notch: Report of a case and literature review. J. Clin. Exp. Dent. 2015, 7, e133–e137. [Google Scholar] [CrossRef] [PubMed]
- Seo, M.-H.; Lee, J.-Y.; Frimpong, P.; Eo, M.-Y.; Kim, S.-M. Modified Endoscopic-Assisted Approach for Removal of Ectopic Third Molar in the Maxillary Sinus. Appl. Sci. 2021, 11, 8446. [Google Scholar] [CrossRef]
- Scarano, A.; Perrotti, V.; Carinci, F.; Shibli, J.A. Removal of a migrated dental implant from the maxillary sinus after 7 years: A case report. Oral Maxillofac. Surg. 2010, 15, 239–243. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Search Strategies | |
|---|---|
| Keywords: | Advanced keywords search: ((ectopic OR wisdom OR Third molar) AND teeth AND maxilla* sinus)) |
| Databases | Pubmed/Medline, EMBASE, Cochrane Library |
| Authors | Journal | Study Design | Age | Principal Symptoms | Lesions | Treatment Protocol | Technique | Post Operative Sequelae | Drug Therapy | Position | Subject(s) | Study Findings |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Masalha et al. [13] | J Clin Exp Dent | Case series | Range 16–61 yo | (1) Sinonasal symptoms (7), (2) asymptomatic (2), (3) oro-antral fistula (1) | dentigerous cyst (8) | Lesion enucleation/exodontia | transnasal endoscopic approach (TEA) | (a) self-limited periorbital emphysema (1) (b) transient cheek numbness (1) (c) early post-operative bleeding (1) | - | (a) Inferior wall (n = 1) (b) Inferior/Medial wall (n = 2) (c) Orbital floor (n = 3) (d) Floor (n = 3) (e) Anterior/medial wall (n = 1) (f) Lateral wall (n = 1) | 10 subjects (11 cases) | Trans-nasal Endoscopic surgery is feasible and safe |
| Allen et al. [14] | J Surg Case Rep | Case report | 14 yo | asymptomatic | - | Exodontia | Caldwell–Luc endoscopic approach with maxillary antrostomy | Postoperative period unremarkable. | - | Posterior inferior maxillary sinus | 1 subject | The transoral removal of the tooth in pediatric subject with no anterior nasal trauma. |
| Yagiz et al. [15] | J Stomatol Oral Maxillofac Surg. | Case report | 38 yo | asymptomatic | - | Exodontia | Intraoral exodontia | Postoperative period unremarkable. | - | Lateral wall | 1 subject | The tooth evidence on the OPT was ghost image of the impacted distomolar at the contralateral side |
| Balaji et al. [16] | Indian J Dent Res | Case report | 42 yo | asymptomatic | dentigerous cyst | Exodontia | Intraoral Caldwell Luc procedure | Postoperative period unremarkable. | Antibiotic coverage and non-steroidal anti-inflammatory drugs were administered for 5 days | Orbit floor | 1 subject | An ectopic distomolar along the floor of the orbit with dentigerous cystic features is rare. |
| Liu et al. [17] | J Int Med Res | Case report | 6 yo | asymptomatic | dentigerous cyst | No intervention | - | Postoperative period unremarkable. | - | Posterior wall | 1 subject | A congenital bone defect was observed in the posterior wall of the maxillary sinus |
| Lai et al. [18] | J Radiol Case Rep | Case report | 52 yo | asymptomatic | - | Exodontia | Intraoral maxillary antrostomy | Postoperative period unremarkable. | - | posterolateral wall | 1 subject | Ectopic tooth in the maxillary sinus is a rare condition |
| Viterbo et al. [19] | J Craniofac Surg | Case report | 29 yo | asymptomatic | - | Exodontia | endoscopic sinus surgery | Postoperative period unremarkable. | Antibiotics was administered from the day before the surgery and prolonged for 5 days postoperatively. Corticosteroid and analgesic administration was provided. | Floor of the orbit | 1 subject | If untreated, this occurrenc could determine infections or develop a cyst |
| Lombroni et al. [20] | Indian J Dent Res | Case report | 37 yo | chronic nasal obstruction and moderate bilateral rhinorrhea | - | radiology follow-up | - | - | Prophylaxis associated to prolonged nasal decongestion therapy was administered | Medial wall | 1 subject | The follow up approach is mainly for asymptomatic patients, preferring periodic checks every 6–8 months |
| Liau et al. [21] | J Craniofac Surg | Case report | 63 yo | chronic nasal obstruction with associated intraoral discharge. Tuber chronic oroantral fistula | dentigerous cyst | Lesion enucleation/exodontia | endoscopic-assisted middle meatal antrostomies surgery | Postoperative period unremarkable. | - | Posterosuperior wall | 1 subject | The combined technique with of endoscopic visualisation for a Caldwell-Luc approach |
| Datli et al. [22] | J Craniofac Surg | Case report | 41 yo | Chronic Sinusitis | dentigerous cyst | Lesion enucleation/exodontia | Caldwell-Luc maxillary antrostomy/Penrose drain | Postoperative period unremarkable. | - | posteromedial-lateral walls | 1 subject | Dentigerous cysts caused by an ectopic tooth should be resected |
| Rai et al. [23] | Indian J Dent Res | Case report | 46 yo | complaints of watering from the left eye, pain and swelling | - | Exodontia | Intraoral maxillary antrostomy | Postoperative period unremarkable. | Amoxicillin (500 mg × 3/day) for a week and diclofenac sodium (50 mg × 2/day) were administered for 5 days | Lateral/superior wall | 1 subject | Intraoral approach is superior to the extraoral and endoscopic approach |
| Kara et al. [24] | J Istanb Univ Fac Dent | Case report | 16 yo | expansile swelling | dentigerous cyst | Lesion enucleation/exodontia | Marsupialization, Caldwell-Luc maxillary antrostomy (2 stage surgery) | Postoperative period unremarkable. | - | Posterosuperior wall | 1 subject | Marsupialization and enucleation was preferred for treatment, because of size of cyst and anatomical relationship of tooth. |
| Touiheme et al. [25] | Pan Afr Med J | Case report | 23 yo | Facial pain, chronic synusitis and mucopurulent rhinorrhoea | Inflammatory cyst | Lesion enucleation/exodontia | Caldwell-Luc maxillary antrostomy | Postoperative period unremarkable. | - | Lateral wall | 1 subject | The extraction can be performed by conventional approach or by transnasal endoscopic approach with less morbidity. |
| Chagas Júnior et al. [26] | Craniomaxillofac Trauma Reconstr | Case report | 60 yo | Facial trauma (age 6), claiming breathing and phonatory difficulties | Inflammatory cyst | Exodontia | combined approach of endoscopic sinus surgery and Caldwell-Luc procedure | recurrent oroantral fistula. | Amoxicillin Clavulanate Potassium (875 mg + 125 mg) each 12 h for two weeks, Nimesulide (100 mg) every 12 h for 4 days, paracetamol (750 mg) every 6 h in case of pain or fever | Medial/superior wall | 1 subject | The Caldwell-Luc was chosen to remove the cyst adjacent |
| Saleem et al. [27] | Head Face Med | Case report | 45 yo | haemoptysis. | - | Exodontia | endonasal endoscopic uncinectomy and Caldwell-Luc maxillary antrostomy | Postoperative period unremarkable. | - | Lateral- superior wall | 1 subject | Presence of foreign bodies and ectopic teeth in paranasal sinuses can be reliably excluded |
| Topal et al. [28] | Turk Arch Otorhinolaryngol | Case report | 32 yo | left buccal mucosa was diffusely edematous. | - | Exodontia | combined approach of endoscopic sinus surgery and Caldwell-Luc procedure | Postoperative period unremarkable. | - | Medial wall | 1 subject | Surgical removal is required for complicated patients. |
| Abd El-Fattah et al. [29] | Clin Otolaryngol | Case series | Range 28–48 yo | Loosening of tooth, Sinusitis, Ocular pain | dentigerous cyst | Lesion enucleation/exodontia | (1) Endoscopic-assisted transoral sublabial approach (2) Endoscopic endonasal through middle meatal antrostomy (3) Endoscopic endonasal pre-lacrimal approach | Postoperative period unremarkable. | - | (a) Inferior wall (n = 5) (b) Superior wall (n = 2) (c) Medial wall (n = 2) (d) Lateral wall (n = 2) | 11 subjects | Ectopic teeth associated with cysts in the could be removed with the endoscopic/endoscopic-assisted approaches |
| Guruprasad et al. [30] | J Clin Imaging Sci | Case report | 21 yo | nasal discharge of pus, Swelling | dentigerous cyst | Lesion enucleation/exodontia | Caldwell-Luc maxillary antrostomy | Postoperative period unremarkable. | - | Lateral wall | 1 subject | Management of dentigerous cyst arising from ectopic third molar in the maxillary sinus is usually enucleation. |
| Di Felice et al. [31] | Aust Dent J | Case report | 35 yo | nasal discharge of pus, Swelling | - | radiology follow-up | - | Solved through antibiotic theraphy | - | Postero-lateral wall | 1 subject | Treatment of ectopic teeth in the maxillary sinus is usually surgical extraction. |
| Kasat et al. [32] | Contemp Clin Dent. | Case report | 22 yo | nasal pus discharge | dentigerous cyst | Lesion enucleation/exodontia | Incisional biopsy, Caldwell-Luc procedure | Postoperative period unremarkable. | - | posteromedial-lateral walls, Oro-antral fistula | 1 subject | Occurrence of an ectopic tooth in the maxillary sinus and association of a dentigerous cyst with it is a rare phenomenon. |
| Sharma et al. [33] | Int J Surg Case Rep | Case report | 27 yo | nasal discharge and facial pain | dentigerous cyst | Lesion enucleation/exodontia | Intraoral Caldwell Luc procedure | Postoperative period unremarkable. | - | medial wall (2) | 1 subject (bilateral) | Dental ectopia may occur in antrumand present |
| Jendi et al. [34] | Indian J Otolaryngol Head Neck Surg | Case report | 24 yo | nasal discharge and heaviness | - | Exodontia | Intraoral Caldwell Luc procedure | Postoperative period unremarkable. | - | Lateral nasal wall | 1 subject | Less invasive transnasal endoscopic shaver-assisted technique has been advocated for the retrieval of any foreign body |
| Ramanojam et al. [35] | Ann Maxillofac Surg | Case series | Range 21–32 yo | Pain and swelling cheek, pain ATM joint (1), Asymptomatic (1) | dentigerous cyst (1) | Exodontia | Caldwell-Luc procedure | Postoperative period unremarkable (5). hypoaesthesia of infraorbital nerve (1) | - | (a) Medial wall | 6 subjects (6 cases) | The endoscopic techniques are being used for removal of an intranasal ectopic tooth |
| Mohan et al. [36] | Natl J Maxillofac Surg | Case report | 28 yo | Pain and swelling, purulent rhinorrhea | - | Exodontia | Caldwell-Luc procedure | Postoperative period unremarkable. | - | Superomedial wall | 1 subject | If untreated, it has the tendency to form a cyst or tumor and/or the lesion may cause perforation of the orbital floor and obliteration of the nasal cavity |
| Thakur et al. [37] | BMJ Case Rep | Case report | 25 yo | Pain and swelling, purulent rhinorrhea | Exodontia | Caldwell-Luc procedure | Postoperative period unremarkable. | - | Lateral- Inferior wall | 1 subject | It is important as certain antral diseases like dentigerous cyst, odontogenic keratocyst may co-exist with an ectopic molar | |
| Demirtas et al. [38] | J Craniofac Surg | Case report | 19 yo | pain, discomfort, and fullness in the right cheek | dentigerous cyst | Lesion enucleation/exodontia | First marsupialization, second enucleation with Caldwell-Luc approach (2 stage surgery) | Postoperative period unremarkable. | - | Floor of the orbit | 1 subject | Early diagnosis and treatment of these lesions allow a reduced patient’s morbidity |
| Srinivasa Prasad et al. [39] | Indian J Dent Res | Case report | 45 yo | recurrent purulent rhinorrhea | dentigerous cyst | Lesion enucleation/exodontia | Caldwell-Luc procedure | Postoperative period unremarkable. | - | Postero-medial wall | 1 subject | The treatment of an ectopic tooth in the maxillary sinus is usually removal |
| AlKhudair et al. [40] | Int J Surg Case Rep | Case report | 19 yo | recurrent sinusitis | dentigerous cyst | Lesion enucleation/exodontia | endoscopic-assisted middle meatal antrostomies surgery | Postoperative period unremarkable. | - | (a) Lateral wall (b) Medial wall | 1 subject (bilateral) | The endonasal endoscopic approach is a minimally invasive approach |
| Aydın et al. [41] | Balkan Med J | Case report | 21 yo | Sinus infection, oro-antral fistula | Osteoma | Lesion enucleation/exodontia | endonasal endoscopic uncinectomy and Caldwell-Luc maxillary antrostomy | recurrent oroantral fistula. | - | Posterior wall | 1 subject | A pediatric maxillofacial trauma might cause the eruption of the tooth |
| Almomen et al. [42] | J Surg Case Rep | Case report | - | Sinusitis, nasal discharge | dentigerous cyst | Lesion enucleation/exodontia | transnasal endoscopic approach (TEA) | Postoperative period unremarkable. | - | medial wall | 1 subject | The endonasal endoscopic approach is a direct minimally invasive procedure |
| Buyukkurt et al. [43] | Oral Surg Oral Med Oral Pathol Oral Radiol Endod | Case series | Range 19–32 yo | Swelling, pain | dentigerous cyst | Lesion enucleation/exodontia | Caldwell-Luc procedure | Postoperative period unremarkable. | - | (a) Latero-inferior wall (1) (b) Postero-inferior wall (1) (c) Lateral wall (1) | 3 subjects (3 cases) | Transnasal extraction may be attempted if the tooth is small and near the ostium |
| Bodner et al. [44] | J Laryngol Otol | Case series | - | Swelling, pain, acurte sinusitis | dentigerous cyst | Lesion enucleation/exodontia | Caldwell-Luc procedure | Postoperative period unremarkable. | - | (a) Inferior-lateral wall (3) (b) Lateral wall (7) Supero-llateral wall | 12 subjects | CT is useful for diagnosis and treatment planning of teeth in the maxillary antrum |
| Baykul et al. [45] | Auris Nasus Larynx | Case series | Range 15–52 yo | Swelling, pain, acurte sinusitis | dentigerous cyst (1) | (a) radiology follow-up (2) (b) lesion enucleation/exodontia (7) | Endoscopyc assisted surgery removal | Postoperative period unremarkable. | - | Postero-lateral wall | 9 subjects (4 cases of ectopic 3rd molar) | Ectopic tooth in the maxillary sinus may lead to the misdiagnosis of sinusitis |
| Elmorsy et al. [46] | F1000Res | Case report | 13 yo | dentigerous cyst | Lesion enucleation/exodontia | Intraoral Caldwell Luc procedure | Postoperative period unremarkable. the bone requiring longer time to form and be detected radiographically | −500 mg amoxicillin/8 h/5 days −325 mg acetaminophen/4 h/day −4 mg betamethasone | posterosuperior wall | 1 subject | Asymptomatic cases should be managed with a similar protocol due to their tendency to form cysts or malignancies. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mavriqi, L.; Lorusso, F.; Tartaglia, G.; Inchingolo, F.; Scarano, A. Transinusal Pathway Removal of an Impacted Third Molar with an Unusual Approach: A Case Report and a Systematic Review of the Literature. Antibiotics 2022, 11, 658. https://doi.org/10.3390/antibiotics11050658
Mavriqi L, Lorusso F, Tartaglia G, Inchingolo F, Scarano A. Transinusal Pathway Removal of an Impacted Third Molar with an Unusual Approach: A Case Report and a Systematic Review of the Literature. Antibiotics. 2022; 11(5):658. https://doi.org/10.3390/antibiotics11050658
Chicago/Turabian StyleMavriqi, Luan, Felice Lorusso, Gianluca Tartaglia, Francesco Inchingolo, and Antonio Scarano. 2022. "Transinusal Pathway Removal of an Impacted Third Molar with an Unusual Approach: A Case Report and a Systematic Review of the Literature" Antibiotics 11, no. 5: 658. https://doi.org/10.3390/antibiotics11050658
APA StyleMavriqi, L., Lorusso, F., Tartaglia, G., Inchingolo, F., & Scarano, A. (2022). Transinusal Pathway Removal of an Impacted Third Molar with an Unusual Approach: A Case Report and a Systematic Review of the Literature. Antibiotics, 11(5), 658. https://doi.org/10.3390/antibiotics11050658