
Epidemiological, Clinical and Microbiological Characteristics of Patients with Bloodstream Infections Due to Carbapenem-Resistant K. Pneumoniae in Southern Italy: A Multicentre Study

 ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Microbiology
2.3. Statistical Analysis
2.4. Ethics Statement
3. Results
3.1. Demographic and Clinical Characteristics of Patients
3.2. Characteristics of Patients According to the Carbapenemase Detected
3.3. Characteristics of Patients According to 7-Day Mortality
3.4. Characteristics of Patients According to 90-Day Mortality
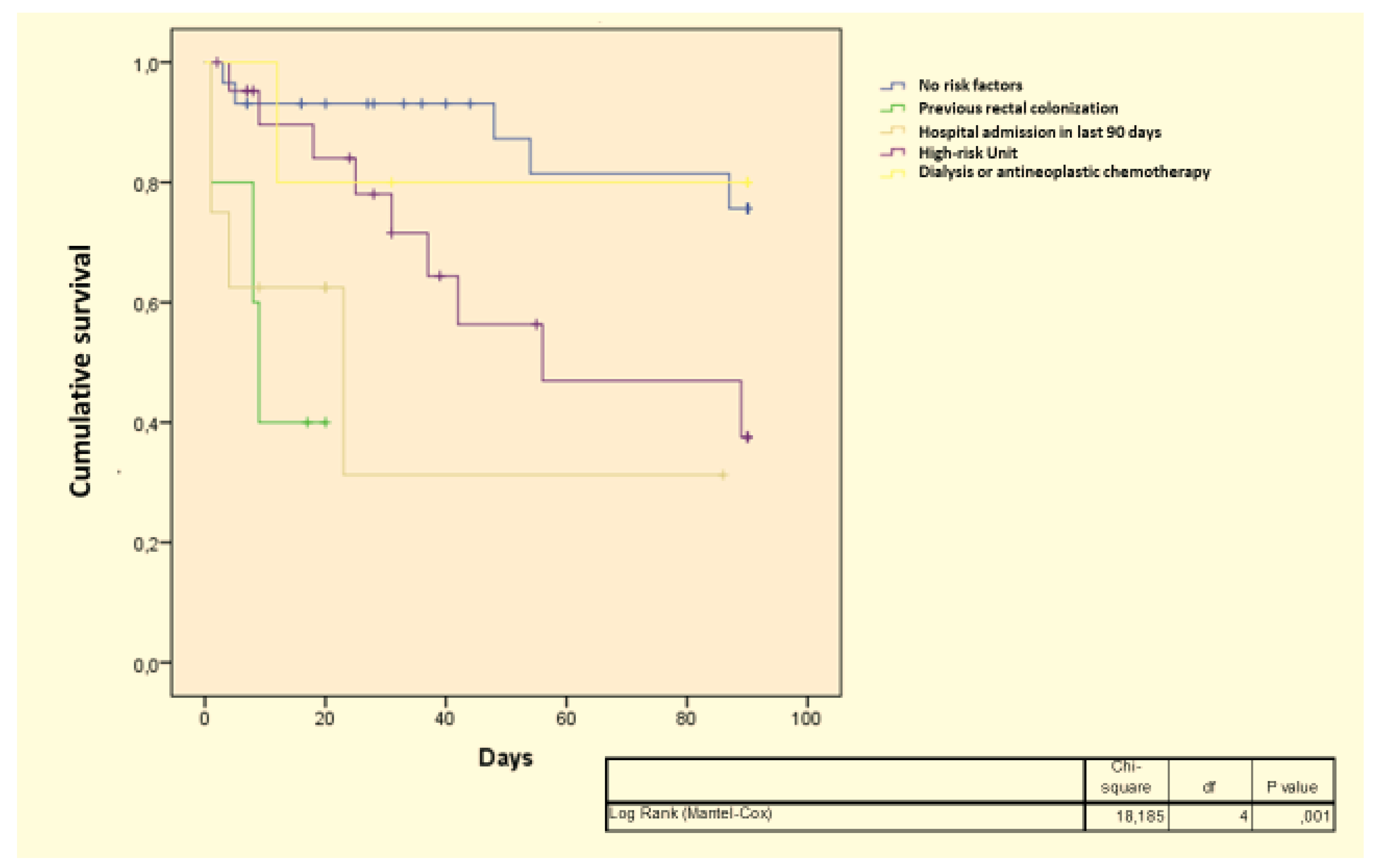
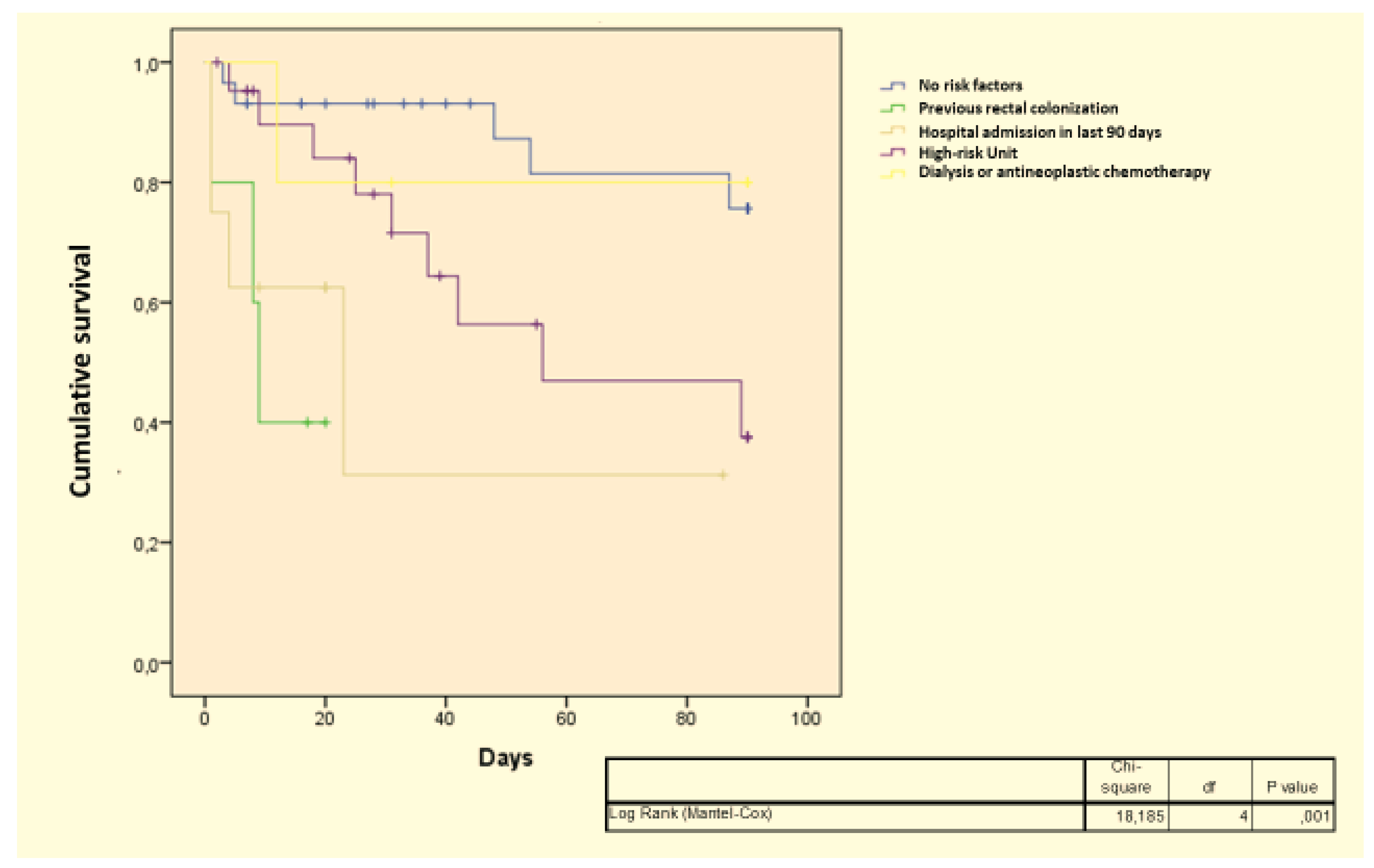
3.5. Independent Predictors of 90-Day Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Laxminarayan, R.; Van Boeckel, T.; Frost, I.; Kariuki, S.; Khan, E.A.; Limmathurotsakul, D.; Larsson, D.G.J.; Levy-Hara, G.; Mendelson, M.; Outterson, K.; et al. The Lancet Infectious Diseases Commission on antimicrobial resistance: 6 years later. Lancet Infect. Dis. 2020, 20, e51–e60. [Google Scholar] [CrossRef]
- ECDC. ECDC Surveillance of antimicrobial resistance in Europe 2020. Ecdc 2020, 1244, 1–71. [Google Scholar]
- Cassini, A.; Högberg, L.D.; Plachouras, D.; Quattrocchi, A.; Hoxha, A.; Simonsen, G.S.; Colomb-Cotinat, M.; Kretzschmar, M.E.; Devleesschauwer, B.; Cecchini, M.; et al. Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European Economic Area in 2015: A population-level modelling analysis. Lancet Infect. Dis. 2019, 19, 56–66. [Google Scholar] [CrossRef] [Green Version]
- Tacconelli, E.; Carrara, E.; Savoldi, A.; Harbarth, S.; Mendelson, M.; Monnet, D.L.; Pulcini, C.; Kahlmeter, G.; Kluytmans, J.; Carmeli, Y.; et al. Discovery, research, and development of new antibiotics: The WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect. Dis. 2018, 18, 318–327. [Google Scholar] [CrossRef]
- Doi, Y. Treatment Options for Carbapenem-resistant Gram-negative Bacterial Infections. Clin. Infect. Dis. 2019, 69, S565–S575. [Google Scholar] [CrossRef] [Green Version]
- Nordmann, P.; Poirel, L. Epidemiology and Diagnostics of Carbapenem Resistance in Gram-negative Bacteria. Clin. Infect. Dis. 2019, 69, S521–S528. [Google Scholar] [CrossRef] [Green Version]
- Palacios-Baena, Z.R.; Giannella, M.; Manissero, D.; Rodríguez-Baño, J.; Viale, P.; Lopes, S.; Wilson, K.; McCool, R.; Longshaw, C. Risk factors for carbapenem-resistant Gram-negative bacterial infections: A systematic review. Clin. Microbiol. Infect. 2021, 27, 228–235. [Google Scholar] [CrossRef]
- Castanheira, M.; Deshpande, L.M.; Mendes, R.E.; Canton, R.; Sader, H.S.; Jones, R.N. Variations in the occurrence of resistance phenotypes and carbapenemase genes among enterobacteriaceae isolates in 20 years of the SENTRY antimicrobial surveillance program. Open Forum Infect. Dis. 2019, 6, S23–S33. [Google Scholar] [CrossRef] [Green Version]
- Sabour, S.; Huang, J.Y.; Bhatnagar, A.; Gilbert, S.E.; Karlsson, M.; Lonsway, D.; Lutgring, J.D.; Rasheed, J.K.; Halpin, A.L.; Stanton, R.A.; et al. Detection and characterization of targeted carbapenem-resistant health care-associated threats: Findings from the antibiotic resistance laboratory network, 2017 to 2019. Antimicrob. Agents Chemother. 2021, 65, e01105-21. [Google Scholar] [CrossRef]
- van Duin, D.; Arias, C.A.; Komarow, L.; Chen, L.; Hanson, B.M.; Weston, G.; Cober, E.; Garner, O.B.; Jacob, J.T.; Satlin, M.J.; et al. Molecular and clinical epidemiology of carbapenem-resistant Enterobacterales in the USA (CRACKLE-2): A prospective cohort study. Lancet Infect. Dis. 2020, 20, 731–741. [Google Scholar] [CrossRef]
- Logan, L.K.; Weinstein, R.A. The epidemiology of Carbapenem-Resistant Enterobacteriaceae: The impact and evolution of a global menace. J. Infect. Dis. 2017, 215, S28–S36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández-Martínez, M.; González-Rico, C.; Gozalo-Margüello, M.; Marco, F.; Gracia-Ahufinger, I.; Aranzamendi, M.; Sánchez-Díaz, A.M.; Vicente-Rangel, T.; Chaves, F.; Calvo Montes, J.; et al. Molecular characterization of multidrug resistant Enterobacterales strains isolated from liver and kidney transplant recipients in Spain. Sci. Rep. 2021, 11, 11875. [Google Scholar] [CrossRef] [PubMed]
- Grundmann, H.; Glasner, C.; Albiger, B.; Aanensen, D.M.; Tomlinson, C.T.; Andrasević, A.T.; Cantón, R.; Carmeli, Y.; Friedrich, A.W.; Giske, C.G.; et al. Occurrence of carbapenemase-producing Klebsiella pneumoniae and Escherichia coli in the European survey of Carbapenemase-Producing Enterobacteriaceae (EuSCAPE): A prospective, multinational study. Lancet Infect. Dis. 2017, 17, 153–163. [Google Scholar] [CrossRef] [Green Version]
- Loconsole, D.; Accogli, M.; De Robertis, A.L.; Capozzi, L.; Bianco, A.; Morea, A.; Mallamaci, R.; Quarto, M.; Parisi, A.; Chironna, M. Emerging high-risk ST101 and ST307 carbapenem-resistant Klebsiella pneumoniae clones from bloodstream infections in Southern Italy. Ann. Clin. Microbiol. Antimicrob. 2020, 19, 24. [Google Scholar] [CrossRef]
- Tang, S.S.L.; Chee, E.; Teo, J.Q.; Chlebicki, M.P.; Kwa, A.L.H. Incidence of a subsequent Carbapenem-Resistant Enterobacteriaceae infection after previous colonisation or infection: A prospective cohort study. Int. J. Antimicrob. Agents 2021, 57, 106340. [Google Scholar] [CrossRef]
- Lin, Q.; Wang, Y.; Yu, J.; Li, S.; Zhang, Y.; Wang, H.; Lai, X.; Liu, D.; Mao, L.; Luo, Y.; et al. Bacterial characteristics of Carbapenem-Resistant Enterobacteriaceae (CRE) colonized strains and their correlation with subsequent infection. BMC Infect. Dis. 2021, 21, 638. [Google Scholar] [CrossRef]
- Gutiérrez-Gutiérrez, B.; Salamanca, E.; de Cueto, M.; Pascual, A.; Rodríguez-Baño, J.; Hsueh, P.R.; Viale, P.; Paño-Pardo, J.R.; Venditti, M.; Tumbarello, M.; et al. A Predictive Model of Mortality in Patients With Bloodstream Infections due to Carbapenemase-Producing Enterobacteriaceae. Mayo Clin. Proc. 2016, 91, 1362–1371. [Google Scholar] [CrossRef] [Green Version]
- Gutiérrez-Gutiérrez, B.; Salamanca, E.; de Cueto, M.; Hsueh, P.R.; Viale, P.; Paño-Pardo, J.R.; Venditti, M.; Tumbarello, M.; Daikos, G.; Cantón, R.; et al. Effect of appropriate combination therapy on mortality of patients with bloodstream infections due to Carbapenemase-Producing Enterobacteriaceae (INCREMENT): A retrospective cohort study. Lancet Infect. Dis. 2017, 17, 726–734. [Google Scholar] [CrossRef]
- Satlin, M.J.; Chen, L.; Patel, G.; Gomez-Simmonds, A.; Weston, G.; Kim, A.C.; Seo, S.K.; Rosenthal, M.E.; Sperber, S.J.; Jenkins, S.G.; et al. Multicenter clinical and molecular epidemiological analysis of bacteremia due to Carbapenem-Resistant Enterobacteriaceae (CRE) in the CRE epicenter of the United States. Antimicrob. Agents Chemother. 2017, 61, e02349-16. [Google Scholar] [CrossRef] [Green Version]
- Ara-Montojo, M.F.; Escosa-García, L.; Alguacil-Guillén, M.; Seara, N.; Zozaya, C.; Plaza, D.; Schuffelmann-Gutiérrez, C.; de la Vega, A.; Fernández-Camblor, C.; Ramos-Boluda, E.; et al. Predictors of mortality and clinical characteristics among carbapenem-resistant or Carbapenemase-Producing Enterobacteriaceae bloodstream infections in Spanish children. J. Antimicrob. Chemother. 2021, 76, 220–225. [Google Scholar] [CrossRef]
- Machuca, I.; Gutiérrez-Gutiérrez, B.; Rivera-Espinar, F.; Cano, A.; Gracia-Ahufinger, I.; Guzman-Puche, J.; Marfil-Pérez, E.; Pérez-Nadales, E.; Castón, J.J.; Bonomo, R.A.; et al. External validation of the INCREMENT-CPE mortality score in a carbapenem-resistant Klebsiella pneumoniae bacteraemia cohort: The prognostic significance of colistin resistance. Int. J. Antimicrob. Agents 2019, 54, 442–448. [Google Scholar] [CrossRef] [PubMed]
- Cano, A.; Gutiérrez-Gutiérrez, B.; Machuca, I.; Gracia-Ahufinger, I.; Pérez-Nadales, E.; Causse, M.; Castón, J.J.; Guzman-Puche, J.; Torre-Giménez, J.; Kindelán, L.; et al. Risks of Infection and Mortality among Patients Colonized with Klebsiella pneumoniae Carbapenemase-Producing K. pneumoniae: Validation of Scores and Proposal for Management. Clin. Infect. Dis. 2018, 66, 1204–1210. [Google Scholar] [PubMed] [Green Version]
- Papadimitriou-Olivgeris, M.; Bartzavali, C.; Georgakopoulou, A.; Kolonitsiou, F.; Mplani, V.; Spiliopoulou, I.; Christofidou, M.; Fligou, F.; Marangos, M. External validation of INCREMENT-CPE score in a retrospective cohort of carbapenemase-producing Klebsiella pneumoniae bloodstream infections in critically ill patients. Clin. Microbiol. Infect. 2021, 27, 915.e1–915.e3. [Google Scholar] [CrossRef] [PubMed]
- Tamma, P.D.; Goodman, K.E.; Harris, A.D.; Tekle, T.; Roberts, A.; Taiwo, A.; Simner, P.J. Comparing the outcomes of patients with carbapenemase-producing and non-carbapenemase- producing Carbapenem-Resistant Enterobacteriaceae bacteremia. Clin. Infect. Dis. 2017, 64, 257–264. [Google Scholar] [CrossRef] [Green Version]
- Hovan, M.R.; Narayanan, N.; Cedarbaum, V.; Bhowmick, T.; Kirn, T.J. Comparing mortality in patients with carbapenemase-producing carbapenem resistant Enterobacterales and non-carbapenemase-producing carbapenem resistant Enterobacterales bacteremia. Diagn. Microbiol. Infect. Dis. 2021, 101, 115505. [Google Scholar] [CrossRef]
- Kassem, A.; Raed, A.; Michael, T.; Sagi, O.; Shimoni, O.; Borer, A.; Saidel-Odes, L. Risk factors and outcomes of patients colonized with carbapenemase-producing and non-carbapenemase-producing Carbapenem-Resistant Enterobacteriaceae. Infect. Control Hosp. Epidemiol. 2020, 41, 1154–1161. [Google Scholar] [CrossRef]

{kind=link}
| N° of patients | 154 |
| Mean age (SD), years | 60.8 (18.9) |
| Males, n° (%) | 97 (63.0) |
| Acquisition, n° (%) | |
| 16 (10.4) 136 (88.3) 78 (50.6) 28 (18.2) 18 (11.7) 12 (7.8) 2 (1.3) |
| Carbapenemase detection, n° (%) | |
| 112 (72.7) 25 (16.2) 17 (11.0) |
| Site of infection | |
| 73 (47.4) 29 (18.8) 19 (12.3) 11 (7.1) 8 (5.2) 4 (2.6) 10 (6.5) |
| Risk factors | |
| 17 (11.0) 22 (14.3) 48 (31.2) 5 (3.2) 62 (40.3) |
| Antibiotic treatment | |
| 39 (25.3) 12 (7.8) 8 (5.2) 15 (9.7) 80 (51.9) |
| 7-day mortality | 50 (32.5) |
| 90-day mortality ** | 62 (41.9) |
| MBL | KPC/OXA-48 | No Carbapenemase Detected | p Value | |
|---|---|---|---|---|
| N° of patients | 25 | 112 | 17 | |
| Mean age (SD), years | 49.1 (29.5) | 63.0 (15.3) | 63.0 (15.9) | 0.24 |
| Males, n° (%) | 13 (52.0) | 74 (66.1) | 10 (58.8) | 0.39 |
| Acquisition, n° (%) | ||||
| 0 (0.0) 24 (96.0) 18 (72.0) 5 (20.0) 0 (0.0) 1 (4.0) 1 (4.0) | 15 (13.4) 96 (85.7) 49 (43.7) 23 (20.5) 16 (14.3) 8 (7.1) 1 (0.9) | 1 (5.9) 16 (94.1) 12 (70.6) 0 (0.0) 3 (17.6) 1 (5.9) 0 (0.0) | 0.20 |
| Site of infection | ||||
| 11 (44.0) 4 (16.0) 5 (20.0) 0 (0.0) 2 (8.0) 1 (4.0) 2 (8.0) | 57 (50.9) 16 (14.3) 12 (10.7) 11 (9.8) 6 (5.4) 3 (2.7) 7 (6.2) | 5 (29.4) 9 (52.9) 2 (11.8) 0 (5.9) 0 (0.0) 0 (0.0) 1 (5.9) | 0.052 |
| Risk factors | ||||
| 15 (60.0) 0 (0.0) 2 (8.0) 8 (32.0) 0 (0.0) | 43 (38.4) 17 (15.2) 17 (15.2) 30 (26.8) 5 (4.5) | 4 (23.5) 0 (0.0) 3 (17.6) 10 (58.8) 0 (0.0) | 0.024 |
| Antibiotic treatment | ||||
| 0 (0.0) 0 (0.0) 2 (8.0) 6 (24.0) 17 (68.0) | 38 (33.9) 9 (8.0) 1 (0.9) 6 (5.3) 58 (51.8) | 1 (5.9) 3 (17.6) 5 (29.4) 3 (17.6) 5 (29.4) | <0.001 |
| 7-day mortality | 4 (16.0) | 41 (36.6) | 5 (29.4) | 0.13 |
| 90-day mortality ** | 6 (24.0) | 47 (43.9) | 9 (56.2) | 0.09 |
| Survivors | Dead | p Value | |
|---|---|---|---|
| N° of patients | 104 | 50 | |
| Mean age (SD), years | 59.6 (20.0) | 63.1 (16.6) | 0.26 |
| Males, n° (%) | 60 (57.7) | 37 (74.0) | 0.049 |
| Acquisition, n° (%) | |||
| 10 (9.6) 93 (89.4) 48 (46.1) 23 (22.1) 13 (12.5) 9 (5.8) 1 (0.9) | 6 (12.0) 43 (86.0) 30 (60.0) 5 (10.0) 5 (10.0) 3 (6.0) 1 (2.0) | 0.77 |
| Carbapenemase detection, n° (%) | |||
| 71 (68.3) 21 (20.2) 12 (11.5) | 41 (82.0) 4 (8.0) 5 (10.0) | 0.13 |
| Site of infection | |||
| 46 (44.2) 21 (20.2) 15 (14.4) 6 (5.8) 5 (4.8) 2 (1.9) 9 (8.6) | 27 (54) 8 (16) 4 (8) 5 (10) 3 (6) 2 (4) 1 (2) | 0.57 |
| Risk factors | |||
| 6 (5.8) 12 (11.5) 31 (29.8) 4 (3.8) 51 (49.0) | 11 (22) 10 (20) 17 (34) 1 (2) 11 (22) | 0.003 |
| Antibiotic treatment | |||
| 31 (29.8) 7 (6.7) 6 (5.8) 11 (10.6) 49 (47.1) | 8 (16.0) 5 (10.0) 2 (4.0) 4 (8.0) 31 (62.0) | 0.29 |
| Survivors | Dead | p Value | |
|---|---|---|---|
| N° of patients | 86 | 62 | |
| Mean age (SD), years | 58.2 (20.9) | 62.7 (15.7) | 0.14 |
| Males, n° (%) | 50 (58.1) | 44 (71.0) | 0.11 |
| Acquisition, n° (%) | |||
| 9 (10.5) 76 (88.4) 38 (44.2) 20 (23.2) 11 (12.8) 7 (8.1) 1 (1.2) | 6 (9.7) 55 (88.7) 39 (62.9) 7 (11.3) 5 (8.1) 4 (6.4) 1 (1.6) | 0.96 |
| Carbapenemase detection, n° (%) | |||
| 60 (69.8) 19 (22.1) 7 (8.1) | 47 (75.8) 6 (9.7) 9 (14.5) | 0.09 |
| Site of infection | |||
| 38 (44.2) 13 (15.1) 14 (16.3) 6 (7.0) 4 (4.7) 2 (2.3) 9 (10.5) | 32 (51.6) 14 (22.6) 5 (8.1) 5 (8.1) 3 (4.8) 2 (3.2) 1 (1.6) | 0.25 |
| Risk factors | |||
| 3 (3.5) 10 (11.6) 22 (25.6) 4 (4.7) 47 (54.7) | 11 (17.7) 10 (16.1) 25 (40.3) 1 (1.6) 15 (24.2) | 0.001 |
| Antibiotic treatment | |||
| 23 (26.7) 5 (5.8) 5 (5.8) 11 (12.8) 42 (48.8) | 13 (21.0) 7 (11.3) 3 (4.8) 4 (6.5) 35 (56.5) | 0.44 |
| OR | 95% Confidence Interval | p Value | ||
|---|---|---|---|---|
| Lower | Upper | |||
| Age | 1.014 | 0.992 | 1.036 | 0.214 |
| Sex (M vs. F) | 1.757 | 0.766 | 4.033 | 0.184 |
| No carbapenemase detected (ref.) | ||||
| 0.53 0.369 | 0.163 0.081 | 1.717 1.68 | 0.289 0.197 |
| Presence of risk factors | 2.715 | 1.215 | 6.068 | 0.015 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Onorato, L.; Sarnelli, B.; D’Agostino, F.; Signoriello, G.; Trama, U.; D’Argenzio, A.; Montemurro, M.V.; Coppola, N. Epidemiological, Clinical and Microbiological Characteristics of Patients with Bloodstream Infections Due to Carbapenem-Resistant K. Pneumoniae in Southern Italy: A Multicentre Study. Antibiotics 2022, 11, 633. https://doi.org/10.3390/antibiotics11050633
Onorato L, Sarnelli B, D’Agostino F, Signoriello G, Trama U, D’Argenzio A, Montemurro MV, Coppola N. Epidemiological, Clinical and Microbiological Characteristics of Patients with Bloodstream Infections Due to Carbapenem-Resistant K. Pneumoniae in Southern Italy: A Multicentre Study. Antibiotics. 2022; 11(5):633. https://doi.org/10.3390/antibiotics11050633
Chicago/Turabian StyleOnorato, Lorenzo, Bruno Sarnelli, Federica D’Agostino, Giuseppe Signoriello, Ugo Trama, Angelo D’Argenzio, Maria Vittoria Montemurro, and Nicola Coppola. 2022. "Epidemiological, Clinical and Microbiological Characteristics of Patients with Bloodstream Infections Due to Carbapenem-Resistant K. Pneumoniae in Southern Italy: A Multicentre Study" Antibiotics 11, no. 5: 633. https://doi.org/10.3390/antibiotics11050633
APA StyleOnorato, L., Sarnelli, B., D’Agostino, F., Signoriello, G., Trama, U., D’Argenzio, A., Montemurro, M. V., & Coppola, N. (2022). Epidemiological, Clinical and Microbiological Characteristics of Patients with Bloodstream Infections Due to Carbapenem-Resistant K. Pneumoniae in Southern Italy: A Multicentre Study. Antibiotics, 11(5), 633. https://doi.org/10.3390/antibiotics11050633