
Intraosseous Regional Administration of Prophylactic Antibiotics in Total Knee Arthroplasty

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Antibiotic Prophylaxis in Arthroplasty
3. Regional Antibiotic Delivery
4. Intraosseous Antibiotic Delivery
5. High BMI and Revision TKA
6. Reduced Tourniquet Use
7. Current Guidelines
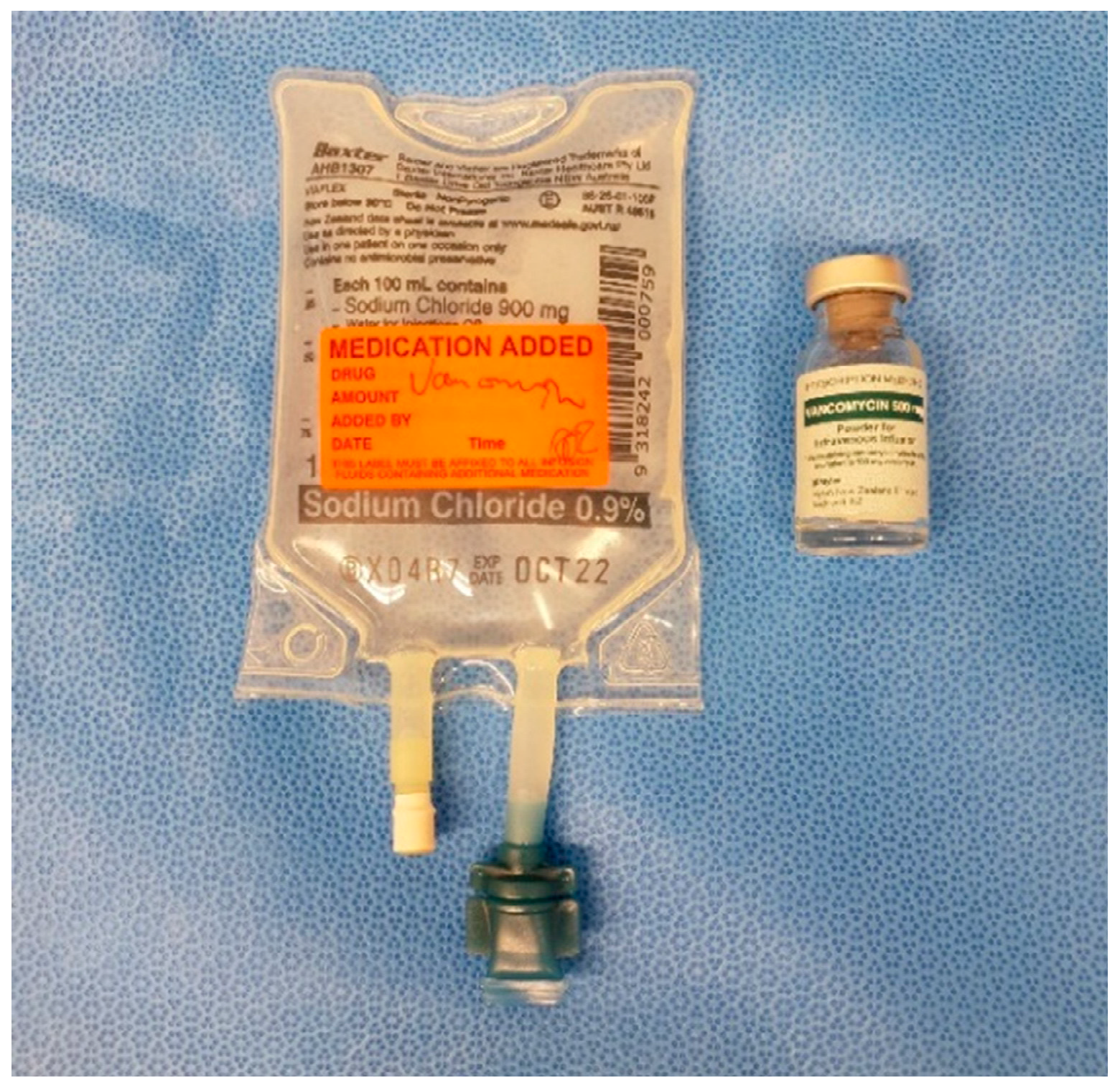
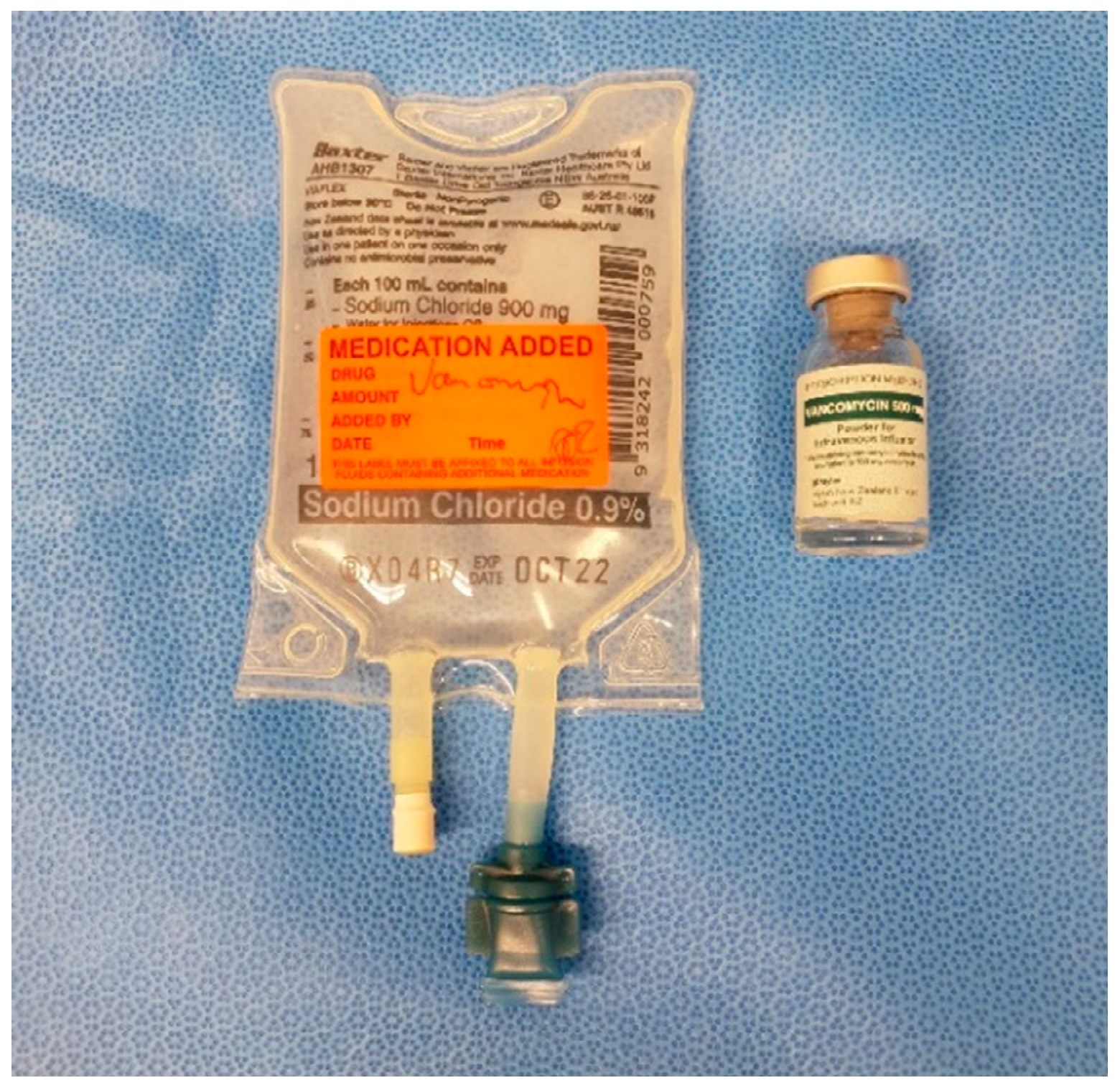
7.1. Antibiotic Solution
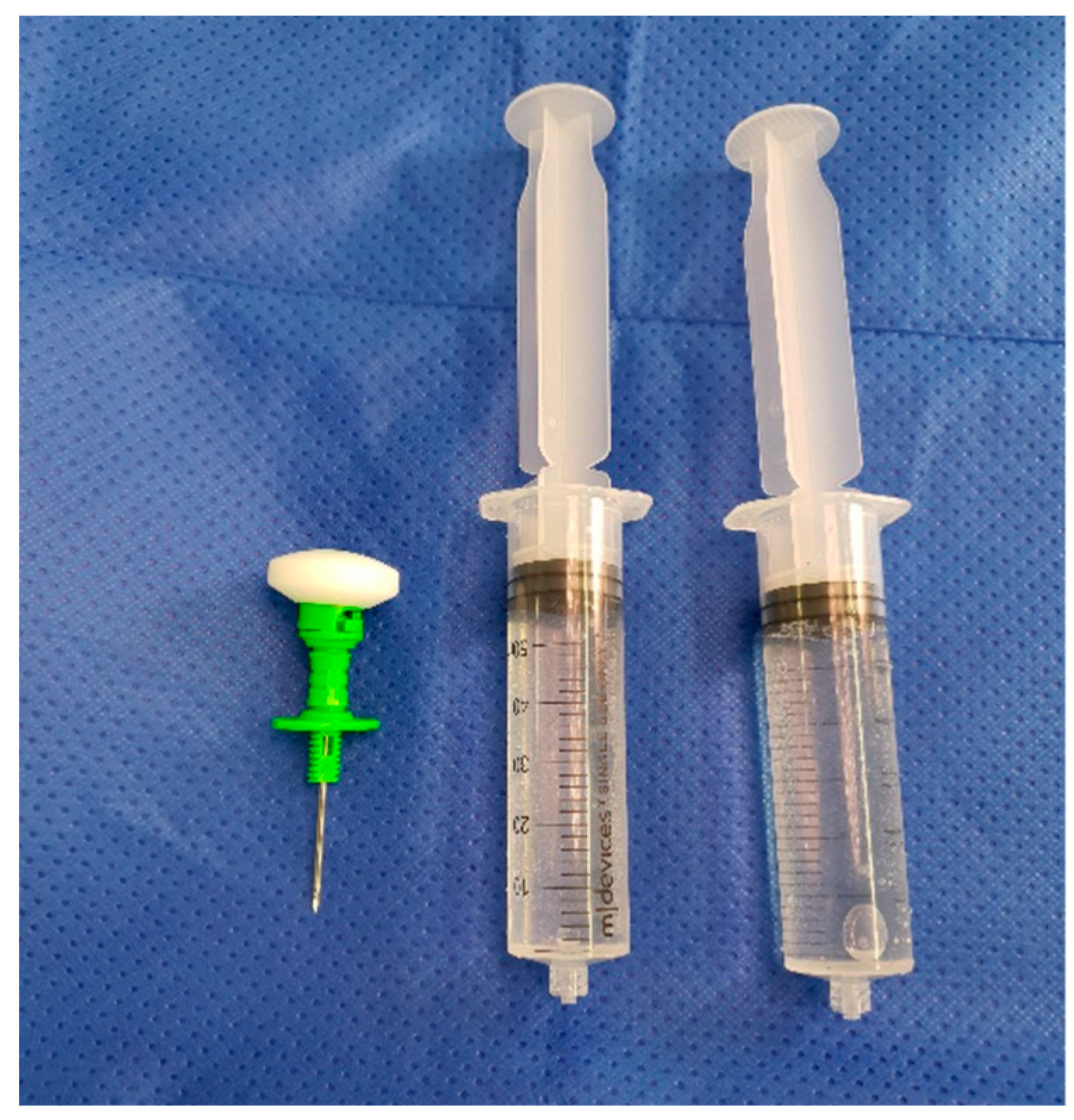
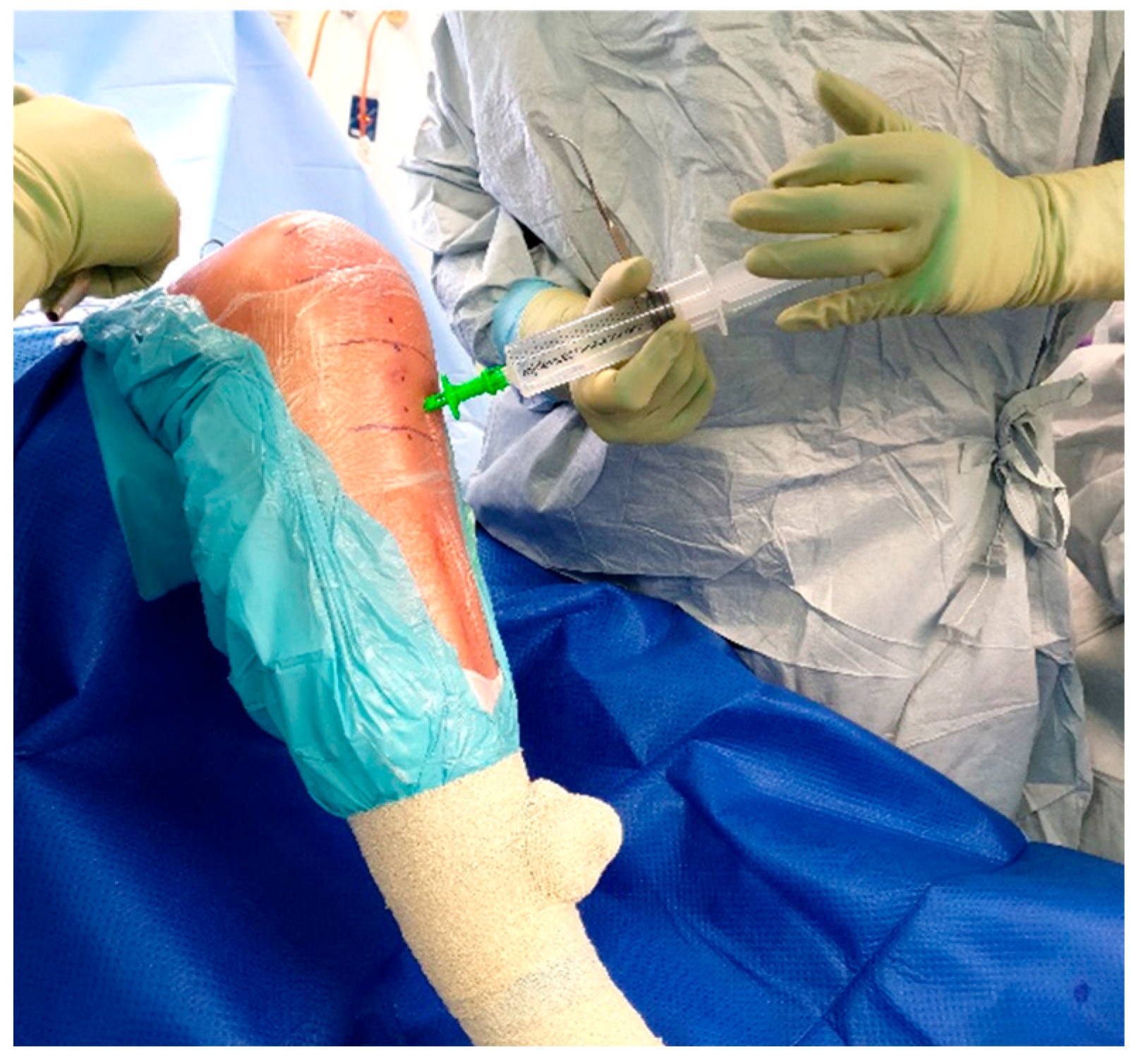
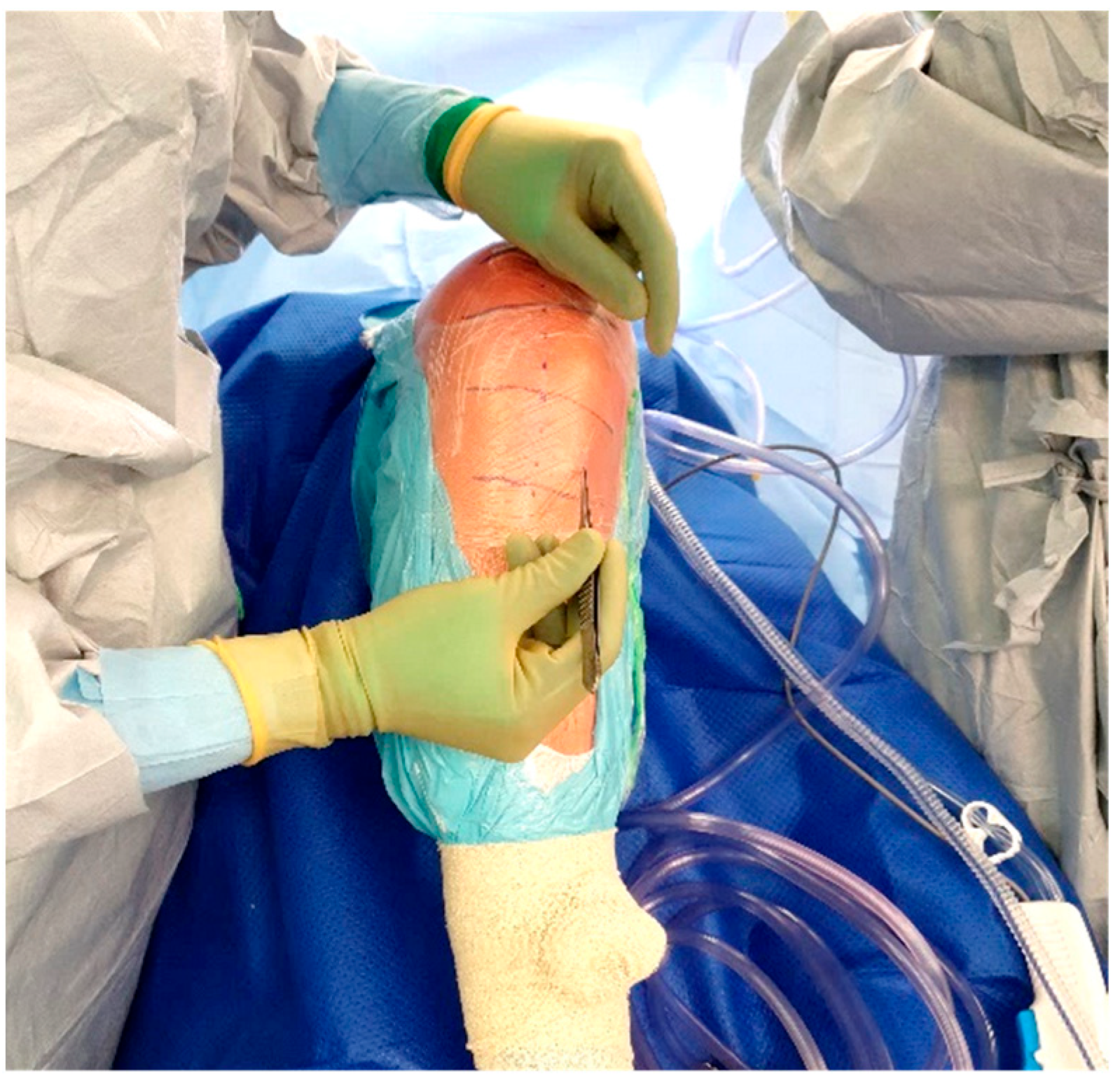
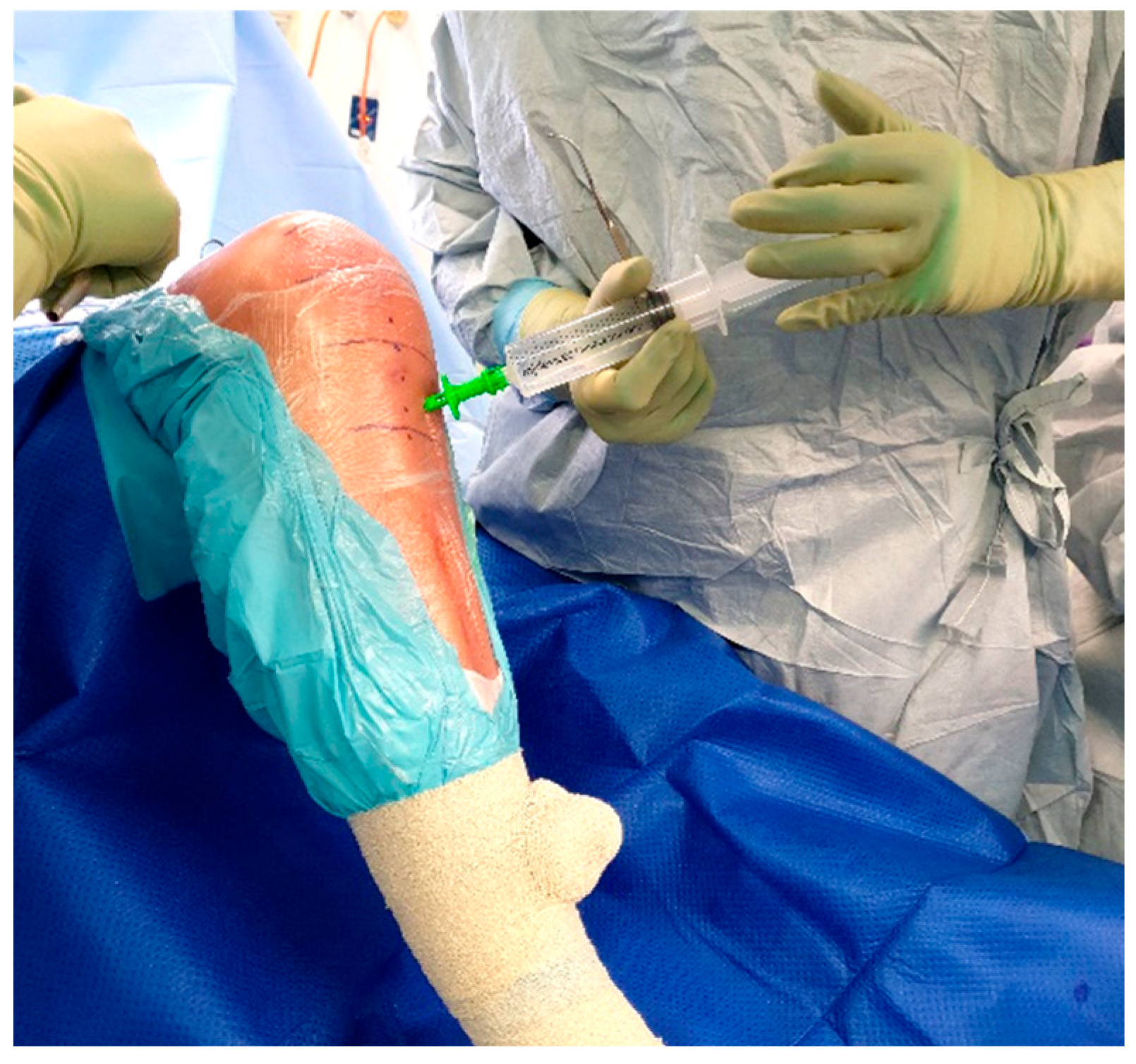
7.2. Procedure
8. In Clinical Practice
9. Discussion
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Holland, S.; Young, S.W. Local Delivery of Antibiotics. In Essentials of Cemented Knee Arthroplasty; Hansen, E., Kühn, K.D., Eds.; Springer: Berlin/Heidelberg, Germany, 2022; pp. 661–671. [Google Scholar] [CrossRef]
- Blom, A.W.; Brown, J.; Taylor, A.H.; Pattison, G.; Whitehouse, S.; Bannister, G.C. Infection after total knee arthroplasty. J. Bone Jt. Surg. Br. 2004, 86, 688–691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurtz, S.M.; Lau, E.; Watson, H.; Schmier, J.K.; Parvizi, J. Economic burden of periprosthetic joint infection in the United States. J. Arthroplast. 2012, 27, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Yamada, K.; Matsumoto, K.; Tokimura, F.; Okazaki, H.; Tanaka, S. Are bone and serum cefazolin concentrations adequate for antimicrobial prophylaxis? Clin. Orthop. Relat. Res. 2011, 469, 3486–3494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoddinott, C.; Lovering, A.M.; Fernando, H.C.; Dixon, J.H.; Reeves, D.S. Determination of bone and fat concentrations following systemic cefamandole and regional cefuroxime administration in patients undergoing knee arthroplasty. J. Antimicrob. Chemother. 1990, 26, 823–829. [Google Scholar] [CrossRef] [PubMed]
- De Lalla, F.; Novelli, A.; Pellizzer, G.; Milocchi, F.; Viola, R.; Rigon, A.; Stecca, C.; Dal Pizzol, V.; Fallani, S.; Periti, P. Regional and systemic prophylaxis with teicoplanin in monolateral and bilateral total knee replacement procedures: Study of pharmacokinetics and tissue penetration. Antimicrob. Agents Chemother. 1993, 37, 2693–2698. [Google Scholar] [CrossRef] [Green Version]
- De Lalla, F.; Viola, R.; Pellizzer, G.; Lazzarini, L.; Tramarin, A.; Fabris, P. Regional prophylaxis with teicoplanin in monolateral or bilateral total knee replacement: An open study. Antimicrob. Agents Chemother. 2000, 44, 316–319. [Google Scholar] [CrossRef] [Green Version]
- Young, S.W.; Zhang, M.; Freeman, J.T.; Vince, K.G.; Coleman, B. Higher cefazolin concentrations with intraosseous regional prophylaxis in TKA. Clin. Orthop. Relat. Res. 2013, 471, 244–249. [Google Scholar] [CrossRef] [Green Version]
- Young, S.W.; Zhang, M.; Freeman, J.T.; Mutu-Grigg, J.; Pavlou, P.; Moore, G.A. The Mark Coventry Award: Higher tissue concentrations of vancomycin with low-dose intraosseous regional versus systemic prophylaxis in TKA: A randomized trial. Clin. Orthop. Relat. Res. 2014, 472, 57–65. [Google Scholar] [CrossRef] [Green Version]
- Young, S.W.; Roberts, T.; Johnson, S.; Dalton, J.P.; Coleman, B.; Wiles, S. Regional Intraosseous Administration of Prophylactic Antibiotics is More Effective Than Systemic Administration in a Mouse Model of TKA. Clin. Orthop. Relat. Res. 2015, 473, 3573–3584. [Google Scholar] [CrossRef] [Green Version]
- Chin, S.J.; Moore, G.A.; Zhang, M.; Clarke, H.D.; Spangehl, M.J.; Young, S.W. The AAHKS Clinical Research Award: Intraosseous Regional Prophylaxis Provides Higher Tissue Concentrations in High BMI Patients in Total Knee Arthroplasty: A Randomized Trial. J. Arthroplast. 2018, 33, S13–S18. [Google Scholar] [CrossRef]
- Young, S.W.; Zhang, M.; Moore, G.A.; Pitto, R.P.; Clarke, H.D.; Spangehl, M.J. The John N. Insall Award: Higher Tissue Concentrations of Vancomycin Achieved With Intraosseous Regional Prophylaxis in Revision TKA: A Randomized Controlled Trial. Clin. Orthop. Relat. Res. 2018, 476, 66–74. [Google Scholar] [CrossRef] [PubMed]
- Arthur, J.R.; Bingham, J.S.; Clarke, H.D.; Spangehl, M.J.; Young, S.W. Intraosseous Regional Administration of Antibiotic Prophylaxis in Total Knee Arthroplasty. JBJS Essent Surg. Tech. 2020, 10, e20.00001. [Google Scholar] [CrossRef] [PubMed]
- Spangehl, M.J.; Clarke, H.D.; Moore, G.A.; Zhang, M.; Probst, N.E.; Young, S.W. Higher Tissue Concentrations of Vancomycin Achieved With Low-Dose Intraosseous Injection vs Intravenous Despite Limited Tourniquet Duration in Primary Total Knee Arthroplasty: A Randomized Trial. J. Arthroplast. 2022, 37, 857–863. [Google Scholar] [CrossRef] [PubMed]
- Klasan, A.; Patel, C.K.; Young, S.W. Intraosseous Regional Administration of Vancomycin in Primary Total Knee Arthroplasty Does Not Increase the Risk of Vancomycin-Associated Complications. J. Arthroplast. 2021, 36, 1633–1637. [Google Scholar] [CrossRef] [PubMed]
- Harper, K.D.; Lambert, B.S.; O’Dowd, J.; Sullivan, T.; Incavo, S.J. Clinical outcome evaluation of intraosseous vancomycin in total knee arthroplasty. Arthroplast Today 2020, 6, 220–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parkinson, B.; McEwen, P.; Wilkinson, M.; Hazratwala, K.; Hellman, J.; Kan, H.; McLean, A.; Panwar, Y.; Doma, K.; Grant, A. Intraosseous Regional Prophylactic Antibiotics Decrease the Risk of Prosthetic Joint Infection in Primary TKA: A Multicenter Study. Clin. Orthop. Relat. Res. 2021, 479, 2504–2512. [Google Scholar] [CrossRef]
- Doyon, F.; Evrard, J.; Mazas, F. Evaluation of therapeutic trials published apropos of antibiotic prophylaxis in orthopedic surgery. Rev. Chir. Orthop. Reparatrice L’appareil Moteur. 1989, 75, 72–76. [Google Scholar]
- Carlson, Ä.S.; Lidgren, L.; Lindberg, L. Prophylactic Antibiotics Against Early and late Deep Infections after total Hip Replacements. Acta Orthop. Scand. 1977, 48, 405–410. [Google Scholar] [CrossRef]
- Espehaug, B.; Engesaeter, L.B.; Vollset, S.E.; Havelin, L.I.; Langeland, N. Antibiotic prophylaxis in total hip arthroplasty. J. Bone Jt. Surg. 1997, 79, 590–595. [Google Scholar] [CrossRef]
- Nickinson, R.S.J.; Board, T.N.; Gambhir, A.K.; Porter, M.L.; Kay, P.R. The microbiology of the infected knee arthroplasty. Int. Orthop. 2010, 34, 505–510. [Google Scholar] [CrossRef] [Green Version]
- Batty, L.M.; Lanting, B. Contemporary Strategies to Prevent Infection in Hip and Knee Arthroplasty. Curr. Rev. Musculoskelet. Med. 2020, 13, 400–408. [Google Scholar] [CrossRef] [PubMed]
- Hill, C.; Mazas, F.; Flamant, R.; Evrard, J. Prophylactic Cefazolin Versus Placebo In Total Hip Replacement Report of a Multicentre Double-blind Randomised Trial. Lancet 1981, 317, 795–797. [Google Scholar] [CrossRef]
- Andrews, J.M. Determination of minimum inhibitory concentrations. J. Antimicrob. Chemother. 2001, 48 (Suppl. 1), 5–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tenover, F.C.; Moellering, R.C. The Rationale for Revising the Clinical and Laboratory Standards Institute Vancomycin Minimal Inhibitory Concentration Interpretive Criteria for Staphylococcus aureus. Clin. Infect. Dis. 2007, 44, 1208–1215. [Google Scholar] [CrossRef] [PubMed]
- Quintilliani, R. Pharmacodynamics of Antimicrobial Agents: Time-Dependent vs. Concentration-Dependent Killing. Available online: http://www.antimicrobe.org/h04c.files/history/PK-PD%20Quint.asp (accessed on 19 April 2022).
- Symonds, T.; Parkinson, B.; Hazratwala, K.; McEwen, P.; Wilkinson, M.; Grant, A. Use of regional administration of prophylactic antibiotics in total knee arthroplasty. ANZ J. Surg. 2018, 88, 848–853. [Google Scholar] [CrossRef]
- Bull, A.L.; Worth, L.J.; Richards, M.J. Impact of Vancomycin Surgical Antibiotic Prophylaxis on the Development of Methicillin-Sensitive Staphylococcus aureus Surgical Site Infections. Ann. Surg. 2012, 256, 1089–1092. [Google Scholar] [CrossRef]
- Garey, K.W. Timing of vancomycin prophylaxis for cardiac surgery patients and the risk of surgical site infections. J. Antimicrob. Chemother. 2006, 58, 645–650. [Google Scholar] [CrossRef] [Green Version]
- Courtney, M.P.; Melnic, C.M.; Zimmer, Z.; Anari, J.; Lee, G.C. Addition of Vancomycin to Cefazolin Prophylaxis Is Associated With Acute Kidney Injury After Primary Joint Arthroplasty. Clin. Orthop. Relat. Res. 2015, 473, 2197–2203. [Google Scholar] [CrossRef] [Green Version]
- Butt, T.D.; Bailey, J.V.; Dowling, P.M.; Fretz, P.B. Comparison of 2 techniques for regional antibiotic delivery to the equine forelimb: Intraosseous perfusion vs. intravenous perfusion. Can. Vet. J. Rev. Vet. Can. 2001, 42, 617–622. [Google Scholar]
- Hoddinott, C.; Lovering, A. Regional prophylactic antibiotic in knee arthroplasty. J. Bone Jt. Surg. Br. Vol. 1993, 75, 157–158. [Google Scholar] [CrossRef]
- Lazzarini, L.; Novelli, A.; Marzano, N.; Timillero, L.; Fallani, S.; Viola, R.; de Lalla, F. Regional and systemic prophylaxis with teicoplanin in total knee arthroplasty A tissue penetration study. J. Arthroplast. 2003, 18, 342–346. [Google Scholar] [CrossRef] [PubMed]
- Voigt, J.; Waltzman, M.; Lottenberg, L. Intraosseous Vascular Access for In-Hospital Emergency Use. Pediatric Emerg. Care 2012, 28, 185–199. [Google Scholar] [CrossRef] [PubMed]
- Kheir, M.M.; Tan, T.L.; Azboy, I.; Tan, D.D.; Parvizi, J. Vancomycin Prophylaxis for Total Joint Arthroplasty: Incorrectly Dosed and Has a Higher Rate of Periprosthetic Infection Than Cefazolin. Clin. Orthop. Relat. Res. 2017, 475, 1767–1774. [Google Scholar] [CrossRef] [Green Version]
- Mortazavi, J.S.M.; Schwartzenberger, J.; Austin, M.S.; Purtill, J.J.; Parvizi, J. Revision Total Knee Arthroplasty Infection: Incidence and Predictors. Clin. Orthop. Relat. Res. 2010, 468, 2052–2059. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurtz, S.M.; Lau, E.C.; Son, M.S.; Chang, E.T.; Zimmerli, W.; Parvizi, J. Are We Winning or Losing the Battle With Periprosthetic Joint Infection: Trends in Periprosthetic Joint Infection and Mortality Risk for the Medicare Population. J. Arthroplast. 2018, 33, 3238–3245. [Google Scholar] [CrossRef]
- Scholten, R.; Leijtens, B.; Hannink, G.; Kamphuis, E.T.; Somford, M.P.; van Susante, J.L.C. General anesthesia might be associated with early periprosthetic joint infection: An observational study of 3909 arthroplasties. Acta Orthop. 2019, 90, 554–558. [Google Scholar] [CrossRef] [Green Version]
- Park, K.J.; Chapleau, J.; Sullivan, T.C.; Clyburn, T.A.; Incavo, S.J. 2021 Chitranjan S. Ranawat Award: Intraosseous vancomycin reduces periprosthetic joint infection in primary total knee arthroplasty at 90-day follow-up. Bone Jt. J. 2021, 103, 13–17. [Google Scholar] [CrossRef]
- Donlan, R.M. Biofilms: Microbial life on surfaces. Emerg. Infect. Dis. 2002, 8, 881–890. [Google Scholar] [CrossRef]
- Kildow, B.J.; Patel, S.P.; Otero, J.E.; Fehring, K.A.; Curtin, B.M.; Springer, B.D.; Fehring, T.K. Results of debridement, antibiotics, and implant retention for periprosthetic knee joint infection supplemented with the use of intraosseous antibiotics. Bone Jt. J. 2021, 103-B, 185–190. [Google Scholar] [CrossRef]
- Buller, L.T.; Sabry, F.Y.; Easton, R.W.; Klika, A.K.; Barsoum, W.K. The Preoperative Prediction of Success Following Irrigation and Debridement With Polyethylene Exchange for Hip and Knee Prosthetic Joint Infections. J. Arthroplast. 2012, 27, 857–864. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wells, Z.; Zhu, M.; Young, S.W. Intraosseous Regional Administration of Prophylactic Antibiotics in Total Knee Arthroplasty. Antibiotics 2022, 11, 634. https://doi.org/10.3390/antibiotics11050634
Wells Z, Zhu M, Young SW. Intraosseous Regional Administration of Prophylactic Antibiotics in Total Knee Arthroplasty. Antibiotics. 2022; 11(5):634. https://doi.org/10.3390/antibiotics11050634
Chicago/Turabian StyleWells, Zoe, Mark Zhu, and Simon W. Young. 2022. "Intraosseous Regional Administration of Prophylactic Antibiotics in Total Knee Arthroplasty" Antibiotics 11, no. 5: 634. https://doi.org/10.3390/antibiotics11050634
APA StyleWells, Z., Zhu, M., & Young, S. W. (2022). Intraosseous Regional Administration of Prophylactic Antibiotics in Total Knee Arthroplasty. Antibiotics, 11(5), 634. https://doi.org/10.3390/antibiotics11050634