
Nonalcoholic Fatty Liver Disease—A Novel Risk Factor for Recurrent Clostridioides difficile Infection


Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Study Design and Patients
4.2. Data Collection, Outcomes, and Definitions
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Magill, S.S.; Edwards, J.R.; Bamberg, W.; Beldavs, Z.G.; Dumyati, G.; Kainer, M.A.; Lynfield, R.; Maloney, M.; McAllister-Hollod, L.; Nadle, J.; et al. Multistate point-prevalence survey of health care-associated infections. N. Engl. J. Med. 2014, 370, 1198–1208. [Google Scholar] [CrossRef] [Green Version]
- Crobach, M.J.T.; Vernon, J.J.; Loo, V.G.; Kong, L.Y.; Pechine, S.; Wilcox, M.H.; Kuijper, E.J. Understanding Clostridium difficile Colonization. Clin. Microbiol. Rev. 2018, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Louie, T.J.; Miller, M.A.; Mullane, K.M.; Weiss, K.; Lentnek, A.; Golan, Y.; Gorbach, S.; Sears, P.; Shue, Y.K.; Group, O.P.T.C.S. Fidaxomicin versus vancomycin for Clostridium difficile infection. N. Engl. J. Med. 2011, 364, 422–431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pepin, J.; Alary, M.E.; Valiquette, L.; Raiche, E.; Ruel, J.; Fulop, K.; Godin, D.; Bourassa, C. Increasing risk of relapse after treatment of Clostridium difficile colitis in Quebec, Canada. Clin. Infect. Dis. 2005, 40, 1591–1597. [Google Scholar] [CrossRef] [Green Version]
- Song, J.H.; Kim, Y.S. Recurrent Clostridium difficile Infection: Risk Factors, Treatment, and Prevention. Gut Liver 2019, 13, 16–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deshpande, A.; Pasupuleti, V.; Thota, P.; Pant, C.; Rolston, D.D.; Hernandez, A.V.; Donskey, C.J.; Fraser, T.G. Risk factors for recurrent Clostridium difficile infection: A systematic review and meta-analysis. Infect. Control Hosp. Epidemiol. 2015, 36, 452–460. [Google Scholar] [CrossRef]
- Lin, H.J.; Hung, Y.P.; Liu, H.C.; Lee, J.C.; Lee, C.I.; Wu, Y.H.; Tsai, P.J.; Ko, W.C. Risk factors for Clostridium difficile-associated diarrhea among hospitalized adults with fecal toxigenic C. difficile colonization. J. Microbiol. Immunol. Infect. 2015, 48, 183–189. [Google Scholar] [CrossRef] [Green Version]
- Shakov, R.; Salazar, R.S.; Kagunye, S.K.; Baddoura, W.J.; DeBari, V.A. Diabetes mellitus as a risk factor for recurrence of Clostridium difficile infection in the acute care hospital setting. Am. J. Infect. Control 2011, 39, 194–198. [Google Scholar] [CrossRef]
- Bishara, J.; Farah, R.; Mograbi, J.; Khalaila, W.; Abu-Elheja, O.; Mahamid, M.; Nseir, W. Obesity as a risk factor for Clostridium difficile infection. Clin. Infect. Dis. 2013, 57, 489–493. [Google Scholar] [CrossRef] [Green Version]
- Czepiel, J.; Drozdz, M.; Pituch, H.; Kuijper, E.J.; Perucki, W.; Mielimonka, A.; Goldman, S.; Wultanska, D.; Garlicki, A.; Biesiada, G. Clostridium difficile infection: Review. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 1211–1221. [Google Scholar] [CrossRef] [Green Version]
- European Association for the Study of The Liver; European Association for the Study of Diabetes; European Association for the Study of Obesity (EASO). EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J. Hepatol. 2016, 64, 1388–1402. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef]
- Haas, J.T.; Francque, S.; Staels, B. Pathophysiology and Mechanisms of Nonalcoholic Fatty Liver Disease. Annu. Rev. Physiol. 2016, 78, 181–205. [Google Scholar] [CrossRef]
- Jayakumar, S.; Loomba, R. Review article: Emerging role of the gut microbiome in the progression of nonalcoholic fatty liver disease and potential therapeutic implications. Aliment. Pharmacol. Ther. 2019, 50, 144–158. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, M.J.; Macfarlane, G.T. Changes in predominant bacterial populations in human faeces with age and with Clostridium difficile infection. J. Med. Microbiol. 2002, 51, 448–454. [Google Scholar] [CrossRef]
- Papic, N.; Jelovcic, F.; Karlovic, M.; Maric, L.S.; Vince, A. Nonalcoholic fatty liver disease as a risk factor for Clostridioides difficile infection. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 569–574. [Google Scholar] [CrossRef]
- Nseir, W.B.; Hussein, S.H.H.; Farah, R.; Mahamid, M.N.; Khatib, H.H.; Mograbi, J.M.; Peretz, A.; Amara, A.E. Nonalcoholic fatty liver disease as a risk factor for Clostridium difficile-associated diarrhea. QJM 2020, 113, 320–323. [Google Scholar] [CrossRef]
- Olsen, M.A.; Yan, Y.; Reske, K.A.; Zilberberg, M.D.; Dubberke, E.R. Recurrent Clostridium difficile infection is associated with increased mortality. Clin. Microbiol. Infect. 2015, 21, 164–170. [Google Scholar] [CrossRef] [Green Version]
- Cozar, A.; Ramos-Martinez, A.; Merino, E.; Martinez-Garcia, C.; Shaw, E.; Marrodan, T.; Calbo, E.; Bereciartua, E.; Sanchez-Munoz, L.A.; Salavert, M.; et al. High delayed mortality after the first episode of Clostridium difficile infection. Anaerobe 2019, 57, 93–98. [Google Scholar] [CrossRef]
- Adenote, A.; Dumic, I.; Madrid, C.; Barusya, C.; Nordstrom, C.W.; Rueda Prada, L. NAFLD and Infection, a Nuanced Relationship. Can. J. Gastroenterol. Hepatol. 2021, 2021, 5556354. [Google Scholar] [CrossRef] [PubMed]
- Mari, A.; Abu Baker, F. Recurrent Urinary Tract Infection: Time to Recommend Weight Loss? Isr. Med. Assoc. J. 2019, 21, 412–413. [Google Scholar] [PubMed]
- Nseir, W.; Artul, S.; Nasrallah, N.; Mahamid, M. The association between primary bacteremia of presumed gastrointestinal origin and nonalcoholic fatty liver disease. Dig. Liver Dis. 2016, 48, 343–344. [Google Scholar] [CrossRef] [PubMed]
- Nseir, W.; Taha, H.; Khateeb, J.; Grosovski, M.; Assy, N. Fatty liver is associated with recurrent bacterial infections independent of metabolic syndrome. Dig. Dis. Sci. 2011, 56, 3328–3334. [Google Scholar] [CrossRef] [PubMed]
- Nseir, W.B.; Mograbi, J.M.; Amara, A.E.; Abu Elheja, O.H.; Mahamid, M.N. Non-alcoholic fatty liver disease and 30-day all-cause mortality in adult patients with community-acquired pneumonia. QJM 2019, 112, 95–99. [Google Scholar] [CrossRef]
- Gjurasin, B.; Butic, I.; Vince, A.; Papić, N. Non-Alcoholic Fatty Liver Disease is Associated with an Increased Mortality in Adult Patients with Group B Streptococcus Invasive Disease. Croat. J. Infect. 2020, 40, 124–128. [Google Scholar] [CrossRef]
- Damms-Machado, A.; Mitra, S.; Schollenberger, A.E.; Kramer, K.M.; Meile, T.; Konigsrainer, A.; Huson, D.H.; Bischoff, S.C. Effects of surgical and dietary weight loss therapy for obesity on gut microbiota composition and nutrient absorption. Biomed. Res. Int. 2015, 2015, 806248. [Google Scholar] [CrossRef]
- Loomba, R.; Seguritan, V.; Li, W.; Long, T.; Klitgord, N.; Bhatt, A.; Dulai, P.S.; Caussy, C.; Bettencourt, R.; Highlander, S.K.; et al. Gut Microbiome-Based Metagenomic Signature for Non-invasive Detection of Advanced Fibrosis in Human Nonalcoholic Fatty Liver Disease. Cell Metab. 2019, 30, 607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Herck, M.A.; Weyler, J.; Kwanten, W.J.; Dirinck, E.L.; De Winter, B.Y.; Francque, S.M.; Vonghia, L. The Differential Roles of T Cells in Non-alcoholic Fatty Liver Disease and Obesity. Front. Immunol. 2019, 10, 82. [Google Scholar] [CrossRef] [Green Version]
- Punni, E.; Pula, J.L.; Asslo, F.; Baddoura, W.; DeBari, V.A. Is obesity a risk factor for Clostridium difficile infection? Obes. Res. Clin. Pract. 2015, 9, 50–54. [Google Scholar] [CrossRef]
- Chandradas, S.; Khalili, H.; Ananthakrishnan, A.; Wayman, C.; Reidel, W.; Waalen, J.; Konijeti, G.G. Does Obesity Influence the Risk of Clostridium difficile Infection Among Patients with Ulcerative Colitis? Dig. Dis. Sci. 2018, 63, 2445–2450. [Google Scholar] [CrossRef]
- Gosai, F.; Covut, F.; Alomari, M.; Hitawala, A.; Singh, A.; Kisangani, G.; Lopez, R.; Shen, B. Obesity Is Associated with Decreased Risk of Clostridium difficile Infection in Hospitalized Patients with Pouchitis. Dig. Dis. Sci. 2020, 65, 1423–1428. [Google Scholar] [CrossRef]
- Lopez-de-Andres, A.; Esteban-Vasallo, M.D.; de Miguel-Diez, J.; Hernandez-Barrera, V.; de Miguel-Yanes, J.M.; Mendez-Bailon, M.; Jimenez-Garcia, R. Incidence and in-hospital outcomes of Clostridium difficile infection among type 2 diabetes patients in Spain. Int. J. Clin. Pract. 2018, 72, e13251. [Google Scholar] [CrossRef] [PubMed]
- Wenisch, J.M.; Schmid, D.; Kuo, H.W.; Simons, E.; Allerberger, F.; Michl, V.; Tesik, P.; Tucek, G.; Wenisch, C. Hospital-acquired Clostridium difficile infection: Determinants for severe disease. Eur. J. Clin. Microbiol. Infect. Dis. 2012, 31, 1923–1930. [Google Scholar] [CrossRef]
- Karlsson, F.H.; Tremaroli, V.; Nookaew, I.; Bergstrom, G.; Behre, C.J.; Fagerberg, B.; Nielsen, J.; Backhed, F. Gut metagenome in European women with normal, impaired and diabetic glucose control. Nature 2013, 498, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Eliakim-Raz, N.; Fishman, G.; Yahav, D.; Goldberg, E.; Stein, G.Y.; Zvi, H.B.; Barsheshet, A.; Bishara, J. Predicting Clostridium difficile infection in diabetic patients and the effect of metformin therapy: A retrospective, case-control study. Eur. J. Clin. Microbiol. Infect. Dis. 2015, 34, 1201–1205. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Yadav, H. Metformin reduces Clostridium difficile infection. FASEB J. 2021, 35. [Google Scholar] [CrossRef]
- Eddi, R.; Malik, M.N.; Shakov, R.; Baddoura, W.J.; Chandran, C.; Debari, V.A. Chronic kidney disease as a risk factor for Clostridium difficile infection. Nephrology 2010, 15, 471–475. [Google Scholar] [CrossRef]
- Yousuf, K.; Saklayen, M.G.; Markert, R.J.; Barde, C.J.; Gopalswamy, N. Clostridium difficile-associated diarrhea and chronic renal insufficiency. South. Med. J. 2002, 95, 681–683. [Google Scholar] [PubMed]
- Kim, S.C.; Seo, M.Y.; Lee, J.Y.; Kim, K.T.; Cho, E.; Kim, M.G.; Jo, S.K.; Cho, W.Y.; Kim, H.K. Advanced chronic kidney disease: A strong risk factor for Clostridium difficile infection. Korean J. Intern. Med. 2016, 31, 125–133. [Google Scholar] [CrossRef]
- Keddis, M.T.; Khanna, S.; Noheria, A.; Baddour, L.M.; Pardi, D.S.; Qian, Q. Clostridium difficile infection in patients with chronic kidney disease. Mayo Clin. Proc. 2012, 87, 1046–1053. [Google Scholar] [CrossRef] [Green Version]
- Adedinsewo, D.; Taka, N.; Agasthi, P.; Sachdeva, R.; Rust, G.; Onwuanyi, A. Prevalence and Factors Associated With Statin Use Among a Nationally Representative Sample of US Adults: National Health and Nutrition Examination Survey, 2011–2012. Clin. Cardiol. 2016, 39, 491–496. [Google Scholar] [CrossRef] [PubMed]
- Ferri, N.; Corsini, A.; Bellosta, S. Pharmacology of the new P2Y12 receptor inhibitors: Insights on pharmacokinetic and pharmacodynamic properties. Drugs 2013, 73, 1681–1709. [Google Scholar] [CrossRef] [PubMed]
- Wijarnpreecha, K.; Panjawatanan, P.; Thongprayoon, C.; Ungprasert, P. Statins & risk of Clostridium difficile infection: A meta-analysis. Indian J. Med. Res. 2019, 150, 359–364. [Google Scholar] [CrossRef] [PubMed]
- Nolan, J.A.; Skuse, P.; Govindarajan, K.; Patterson, E.; Konstantinidou, N.; Casey, P.G.; MacSharry, J.; Shanahan, F.; Stanton, C.; Hill, C.; et al. The influence of rosuvastatin on the gastrointestinal microbiota and host gene expression profiles. Am. J. Physiol. Gastrointest. Liver Physiol. 2017, 312, G488–G497. [Google Scholar] [CrossRef]
- Vieira-Silva, S.; Falony, G.; Belda, E.; Nielsen, T.; Aron-Wisnewsky, J.; Chakaroun, R.; Forslund, S.K.; Assmann, K.; Valles-Colomer, M.; Nguyen, T.T.D.; et al. Statin therapy is associated with lower prevalence of gut microbiota dysbiosis. Nature 2020, 581, 310–315. [Google Scholar] [CrossRef]
- Dias, A.M.; Cordeiro, G.; Estevinho, M.M.; Veiga, R.; Figueira, L.; Reina-Couto, M.; Magro, F.; the Clinical Pharmacology Unit, São João Hospital University Centre. Gut bacterial microbiome composition and statin intake-A systematic review. Pharmacol. Res. Perspect. 2020, 8, e00601. [Google Scholar] [CrossRef]
- Al-Ani, B. Simvastatin inhibits neutrophil degranulation induced by anti-neutrophil cytoplasm auto-antibodies and N-formyl-methionine-leucine-phenylalanine (fMLP) peptide. Saudi Med. J. 2013, 34, 477–483. [Google Scholar]
- Fishbein, M.; Castro, F.; Cheruku, S.; Jain, S.; Webb, B.; Gleason, T.; Stevens, W.R. Hepatic MRI for fat quantitation: Its relationship to fat morphology, diagnosis, and ultrasound. J. Clin. Gastroenterol. 2005, 39, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Siegelman, E.S.; Rosen, M.A. Imaging of hepatic steatosis. Semin. Liver Dis. 2001, 21, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Petrella, L.A.; Sambol, S.P.; Cheknis, A.; Nagaro, K.; Kean, Y.; Sears, P.S.; Babakhani, F.; Johnson, S.; Gerding, D.N. Decreased cure and increased recurrence rates for Clostridium difficile infection caused by the epidemic C. difficile BI strain. Clin. Infect. Dis. 2012, 55, 351–357. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- McDonald, L.C.; Gerding, D.N.; Johnson, S.; Bakken, J.S.; Carroll, K.C.; Coffin, S.E.; Dubberke, E.R.; Garey, K.W.; Gould, C.V.; Kelly, C.; et al. Clinical Practice Guidelines for Clostridium difficile Infection in Adults and Children: 2017 Update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA). Clin. Infect. Dis. 2018, 66, e1–e48. [Google Scholar] [CrossRef] [PubMed]
- Debast, S.B.; Bauer, M.P.; Kuijper, E.J.; European Society of Clinical, M.; Infectious, D. European Society of Clinical Microbiology and Infectious Diseases: Update of the treatment guidance document for Clostridium difficile infection. Clin. Microbiol. Infect. 2014, 20 (Suppl. 2), 1–26. [Google Scholar] [CrossRef] [Green Version]
- Ooijevaar, R.E.; van Beurden, Y.H.; Terveer, E.M.; Goorhuis, A.; Bauer, M.P.; Keller, J.J.; Mulder, C.J.J.; Kuijper, E.J. Update of treatment algorithms for Clostridium difficile infection. Clin. Microbiol. Infect. 2018, 24, 452–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, M.A.; Louie, T.; Mullane, K.; Weiss, K.; Lentnek, A.; Golan, Y.; Kean, Y.; Sears, P. Derivation and validation of a simple clinical bedside score (ATLAS) for Clostridium difficile infection which predicts response to therapy. BMC Infect. Dis. 2013, 13, 148. [Google Scholar] [CrossRef] [Green Version]
- Sterling, R.K.; Lissen, E.; Clumeck, N.; Sola, R.; Correa, M.C.; Montaner, J.; Sulkowski, M.S.; Torriani, F.J.; Dieterich, D.T.; Thomas, D.L.; et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology 2006, 43, 1317–1325. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Papic, N.; Maric, L.S.; Vince, A. Efficacy of oral vancomycin in primary prevention of Clostridium Difficile infection in elderly patients treated with systemic antibiotic therapy. Infect. Dis. 2018, 50, 483–486. [Google Scholar] [CrossRef] [PubMed]
- Van Hise, N.W.; Bryant, A.M.; Hennessey, E.K.; Crannage, A.J.; Khoury, J.A.; Manian, F.A. Efficacy of Oral Vancomycin in Preventing Recurrent Clostridium difficile Infection in Patients Treated With Systemic Antimicrobial Agents. Clin. Infect. Dis 2016, 63, 651–653. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Characteristics | Clostridioides difficile Infection (n = 222) | Recurrent Clostridioides difficile Infection (n = 107) | p-Value a |
|---|---|---|---|
| Age, median (IQR b) | 77 (71–81) | 78 (74–84) | 0.011 |
| Female, No. (%) | 135 (60.8%) | 61 (57.0%) | 0.549 |
| Nursing Home Resident | 74 (33.3%) | 40 (37.4%) | 0.536 |
| Charlson Age–Comorbidity Index | 5 (4–6) | 6 (5–7) | <0.001 |
| Hospital Admission within 3 months | 153 (68.9%) | 87 (81.3%) | 0.018 |
| Comorbidities | |||
| Diabetes Mellitus | 54 (24.3%) | 34 (31.8%) | 0.183 |
| Arterial Hypertension | 108 (48.6%) | 59 (55.1%) | 0.291 |
| Cardiovascular Disease | 57 (25.7%) | 18 (16.8%) | 0.092 |
| Peripheral Vascular Disease | 20 (9.0%) | 9 (8.4%) | >0.999 |
| Hyperlipidemia | 54 (24.3%) | 25 (23.4%) | 0.891 |
| Solid Tumor | 22 (9.9%) | 14 (13.1%) | 0.451 |
| Chronic Kidney Disease | 15 (6.8%) | 28 (26.2%) | <0.001 |
| Chronic Obstructive Pulmonary Disease | 51 (22.9%) | 19 (17.8%) | 0.316 |
| Neurological Diseases | 51 (22.9%) | 27 (25.2%) | 0.679 |
| Obesity (BMI > 30 kg/m2) | 23 (10.4%) | 18 (16.8%) | 0.109 |
| Body Mass Index (BMI) c | 25 (23–28) | 27 (24–30) | 0.010 |
| Nonalcoholic Fatty Liver Disease | 41 (18.5%) | 37 (34.6%) | 0.002 |
| Use of Chronic Medications | |||
| Statins | 52 (23.4%) | 14 (13.1%) | 0.028 |
| Metformin | 15 (6.8%) | 13 (12.1%) | 0.138 |
| Other Perioral Anti-diabetic | 13 (5.9%) | 10 (9.3%) | 0.255 |
| Insulin | 22 (9.9%) | 15 (14.0%) | 0.269 |
| Histamine-2 Receptor Antagonist and/or Proton Pump Inhibitor | 97 (43.7%) | 51 (47.7%) | 0.554 |
| Immunosuppressive Agents | 20 (9.0%) | 7 (6.5%) | 0.525 |
| Antibiotic Therapy before the 1st Episode of CDI | |||
| Fluoroquinolones | 60 (27.0%) | 32 (29.9%) | 0.510 |
| 1st Generation Cephalosporins | 1 (0.4%) | 1 (0.9%) | 0.545 |
| 2nd Generation Cephalosporins | 18 (8.1%) | 7 (6.5%) | 0.824 |
| 3rd Generation Cephalosporins | 30 (13.5%) | 22 (20.5%) | 0.108 |
| 4th Generation Cephalosporins | 3 (1.3%) | 1 (0.9%) | >0.999 |
| Amoxicillin/Clavulanate | 49 (22.1%) | 21 (19.6%) | 0.668 |
| Piperacillin/Tazobactam | 18 (8.1%) | 9 (8.4%) | >0.999 |
| Carbapenems | 7 (3.1%) | 5 (4.7%) | 0.536 |
| Macrolides | 22 (9.9%) | 8 (7.5%) | 0.544 |
| Clindamycin | 12 (5.4%) | 10 (9.3%) | 0.237 |
| Others | 6 (2.7%) | 6 (5.6%) | 0.214 |
| Characteristics | Clostridioides difficile Infection (n = 222) | Recurrent Clostridioides difficile Infection (n = 107) | p-Value a |
|---|---|---|---|
| CDI Severity | |||
| Nonsevere | 95 (42.8%) | 45 (42.0%) | 0.377 |
| Severe | 100 (45.0%) | 54 (50.5%) | |
| Fulminant | 27 (12.2%) | 8 (7.5%) | |
| ATLAS Score | 5 (4–7) | 5 (4–7) | 0.503 |
| Laboratory Findings on Admission | |||
| C-reactive Protein, mg/L | 107.5 (54–172) | 94.1 (54.6–147.0) | 0.294 |
| White Blood Cells Count, ×109/L | 14.5 (10.0–20.0) | 13.2 (10.1–19.6) | 0.487 |
| Hemoglobin, g/L | 120 (107–129) | 120 (108–130) | 0.851 |
| Platelets, ×109 | 251 (198–327) | 256 (190–327) | 0.859 |
| Urea, mmol/L | 8.1 (5.3–13.0) | 7.1 (4.97–11.63) | 0.256 |
| Creatinine, μmol/L | 103 (77.0–153.0) | 109 (75–145) | 0.890 |
| Aspartate Aminotransferase, IU/L | 19 (14–28) | 19 (13–24) | 0.146 |
| Alanine Aminotransferase, IU/L | 15 (10–23) | 14 (10–22) | 0.581 |
| Serum Albumins, g/L | 27.8 (23.9–32.4) | 28.8 (24.8–33.9) | 0.194 |
| CDI Treatment Regiment | |||
| Metronidazole | 77 (34.7%) | 41 (38.3%) | 0.541 |
| Vancomycin | 122 (54.9%) | 60 (56.1%) | 0.906 |
| Metronidazole + vancomycin | 23 (10.4%) | 6 (5.6%) | 0.212 |
| Other Antimicrobials (not for C. difficile) | |||
| Any Systemic Antibiotic | 150 (67.6%) | 67 (62.6%) | 0.387 |
| Fluoroquinolones | 9 (4.0%) | 8 (7.5%) | 0.194 |
| 1st Generation Cephalosporins | 2 (0.9%) | 0 | >0.999 |
| 2nd Generation Cephalosporins | 2 (0.9%) | 1 (0.9%) | >0.999 |
| 3rd Generation Cephalosporins | 48 (21.6%) | 25 (23.4%) | 0.777 |
| 4th Generation Cephalosporins | 2 (0.9%) | 2 (1.9%) | 0.598 |
| Amoxicillin Clavulanate | 18 (8.1%) | 8 (7.5%) | >0.999 |
| Piperacillin/Tazobactam | 41 (18.5%) | 25 (23.4%) | 0.307 |
| Carbapenems | 33 (14.9%) | 11 (10.3%) | 0.301 |
| Macrolides | 5 (2.2%) | 5 (4.7%) | 0.304 |
| Clindamycin | 1 (0.4%) | 1 (0.9%) | 0.545 |
| Others | 8 (3.6%) | 5 (4.7%) | 0.763 |
| No. of Antibiotic Classes Used per Patient | 1 (0–3) | 1 (0–3) | 0.889 |
| Variable | Hazard Ratio | 95% CI | p-Value |
|---|---|---|---|
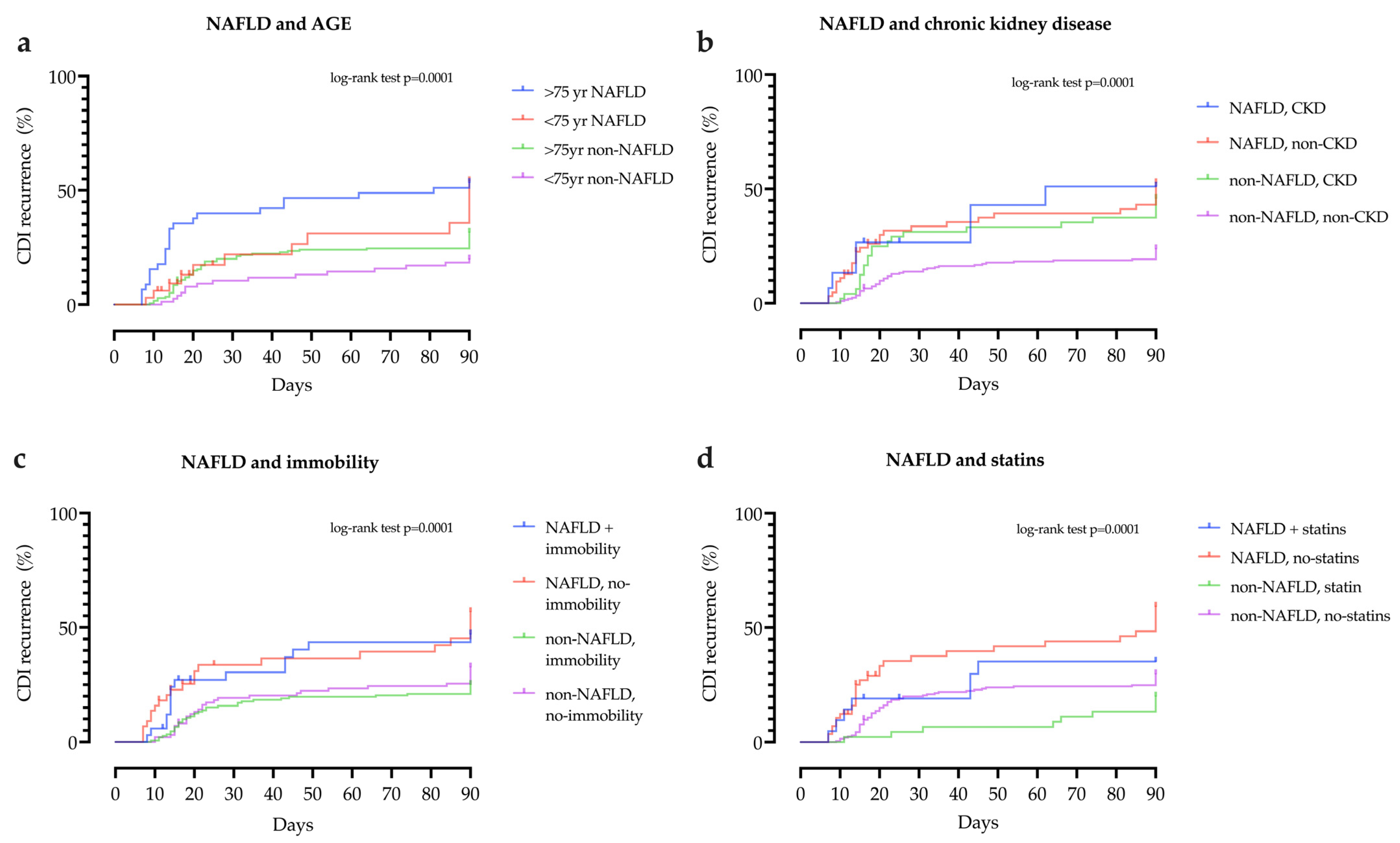
| Age > 75 Years | 1.88 | 1.20 to 2.97 | 0.006 |
| Charlson Age–Comorbidity Index (CACI) > 6 | 1.97 | 1.32 to 2.92 | <0.001 |
| Immobility | 1.73 | 1.16 to 2.56 | 0.006 |
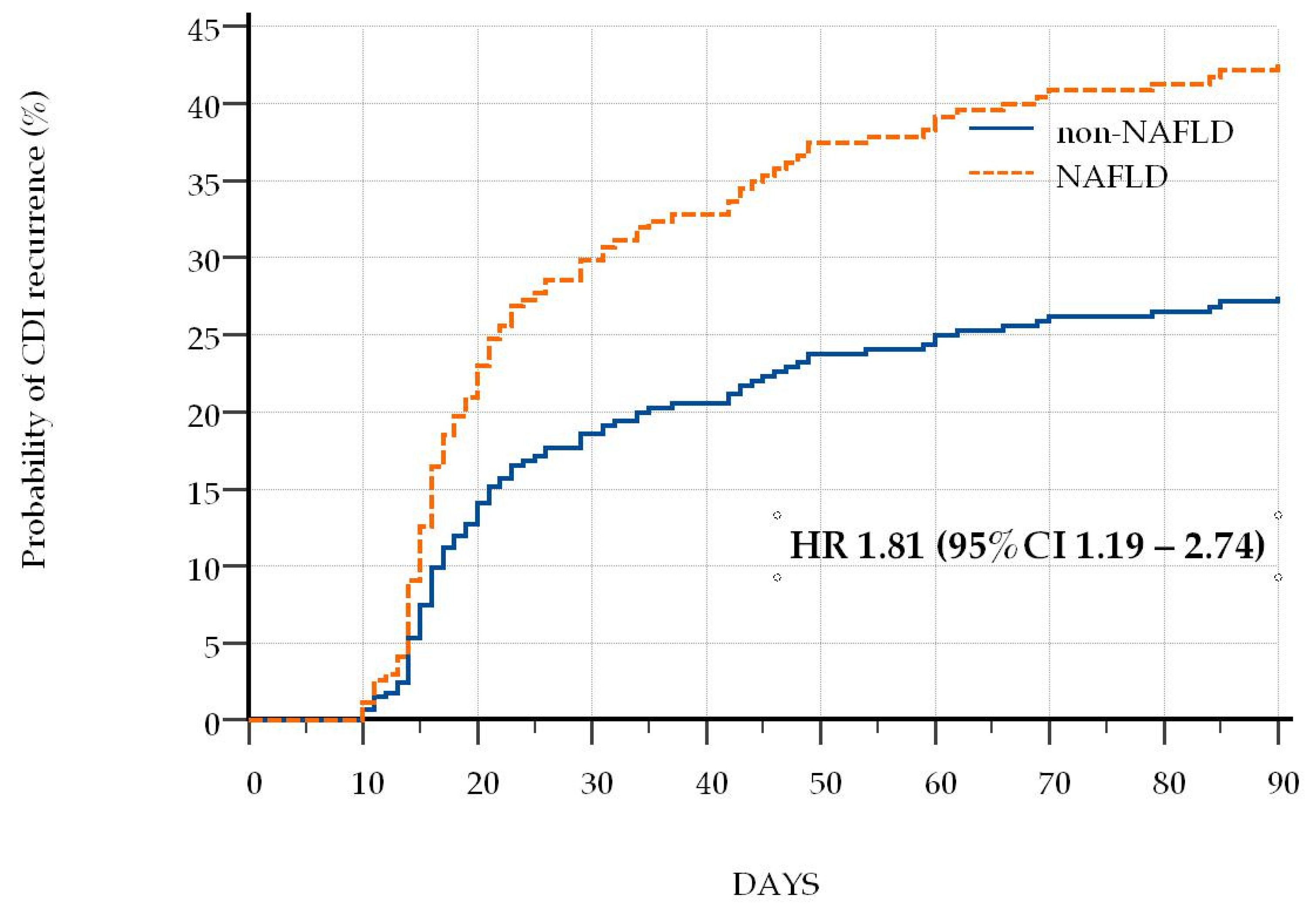
| Nonalcoholic Fatty Liver Disease | 1.81 | 1.19 to 2.74 | 0.005 |
| Chronic Kidney Disease | 1.86 | 1.19 to 2.88 | 0.006 |
| Statins | 0.24 | 0.11 to 0.52 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Šamadan, L.; Jeličić, M.; Vince, A.; Papić, N. Nonalcoholic Fatty Liver Disease—A Novel Risk Factor for Recurrent Clostridioides difficile Infection. Antibiotics 2021, 10, 780. https://doi.org/10.3390/antibiotics10070780
Šamadan L, Jeličić M, Vince A, Papić N. Nonalcoholic Fatty Liver Disease—A Novel Risk Factor for Recurrent Clostridioides difficile Infection. Antibiotics. 2021; 10(7):780. https://doi.org/10.3390/antibiotics10070780
Chicago/Turabian StyleŠamadan, Lara, Mia Jeličić, Adriana Vince, and Neven Papić. 2021. "Nonalcoholic Fatty Liver Disease—A Novel Risk Factor for Recurrent Clostridioides difficile Infection" Antibiotics 10, no. 7: 780. https://doi.org/10.3390/antibiotics10070780
APA StyleŠamadan, L., Jeličić, M., Vince, A., & Papić, N. (2021). Nonalcoholic Fatty Liver Disease—A Novel Risk Factor for Recurrent Clostridioides difficile Infection. Antibiotics, 10(7), 780. https://doi.org/10.3390/antibiotics10070780