
The Role of Non-Enzymatic Degradation of Meropenem—Insights from the Bottle to the Body

 and
and
Abstract
1. Introduction
2. Results
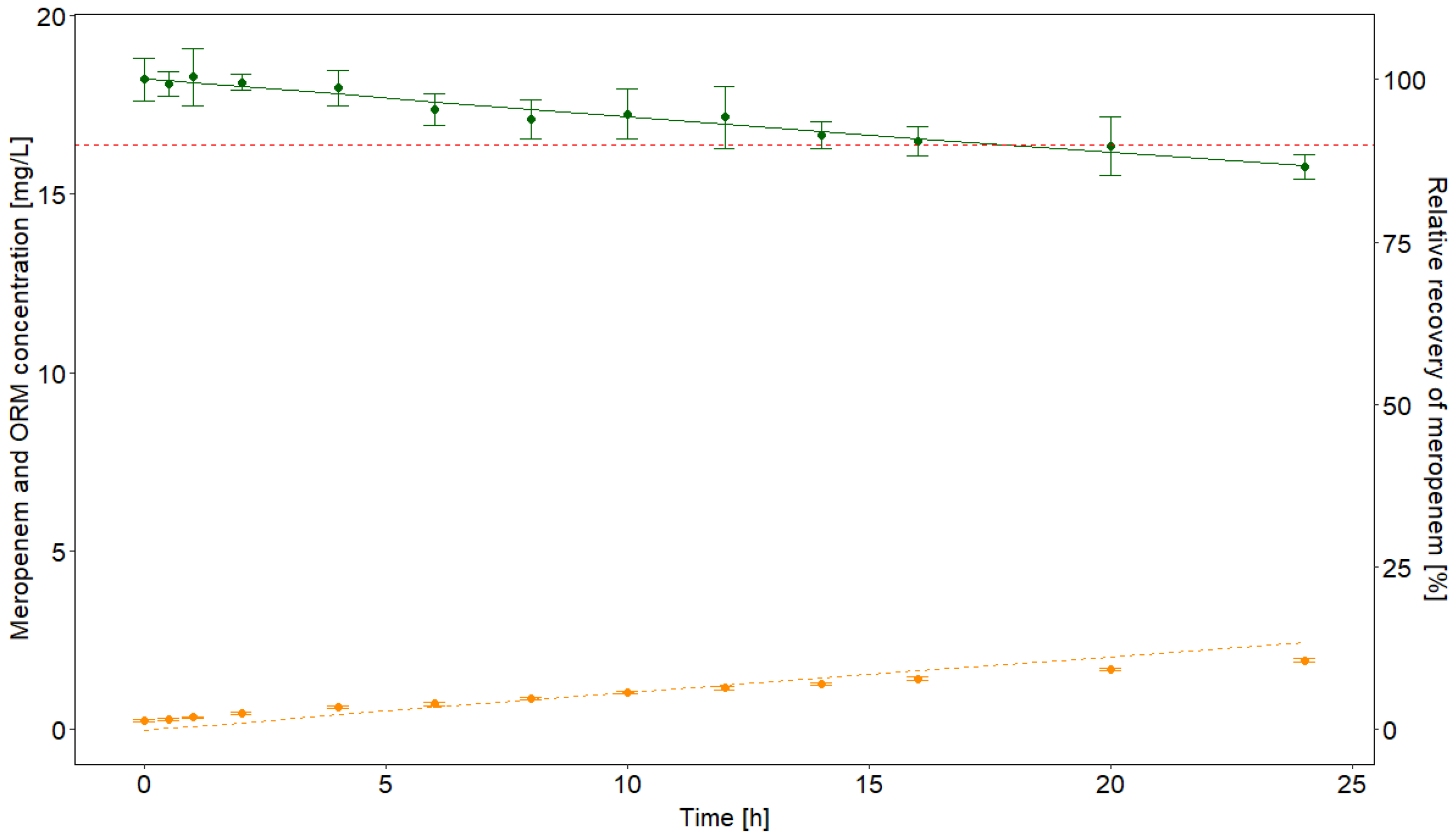
2.1. Infusate Stability at Room Temperature
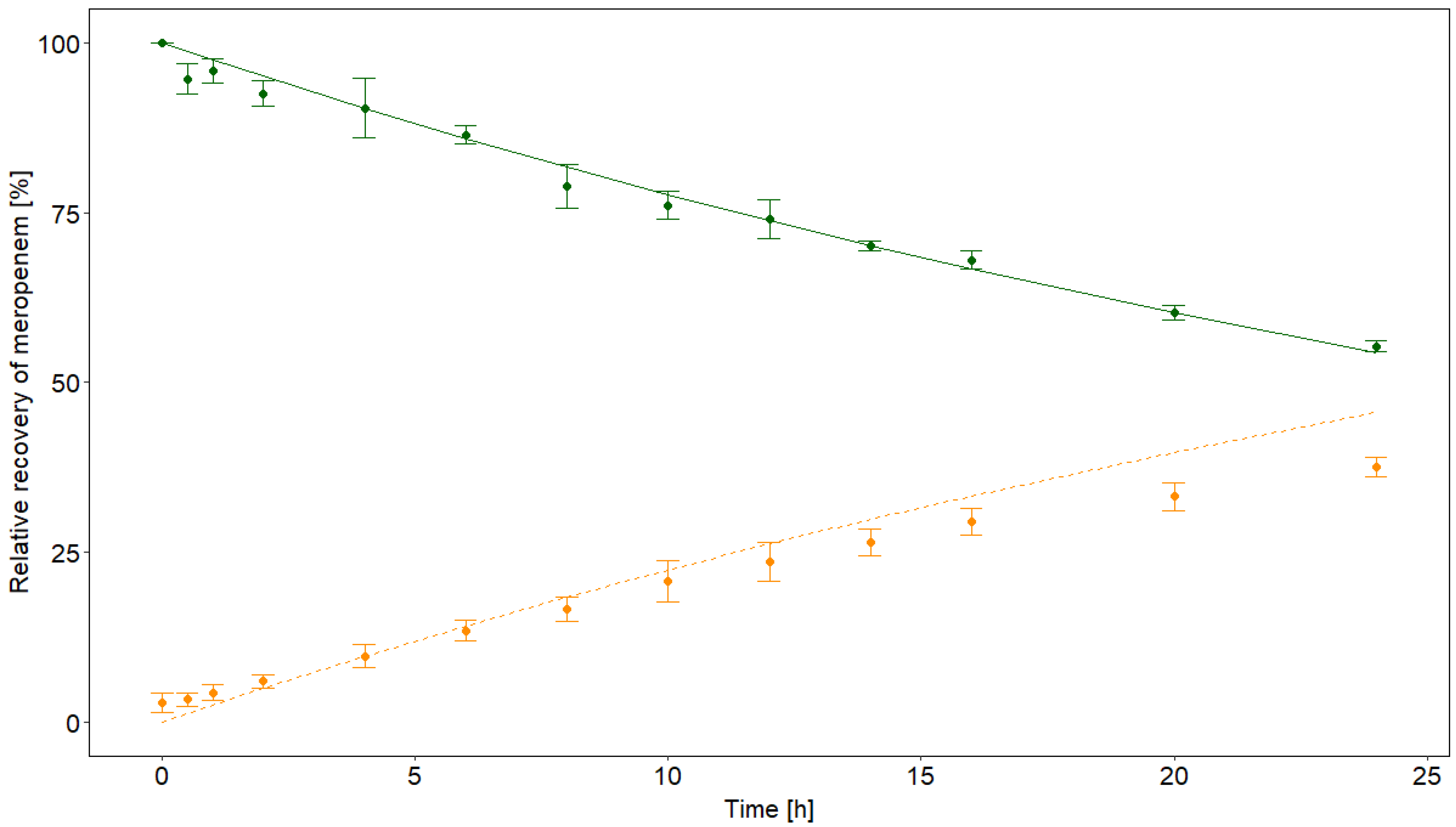
2.2. Stability in Serum
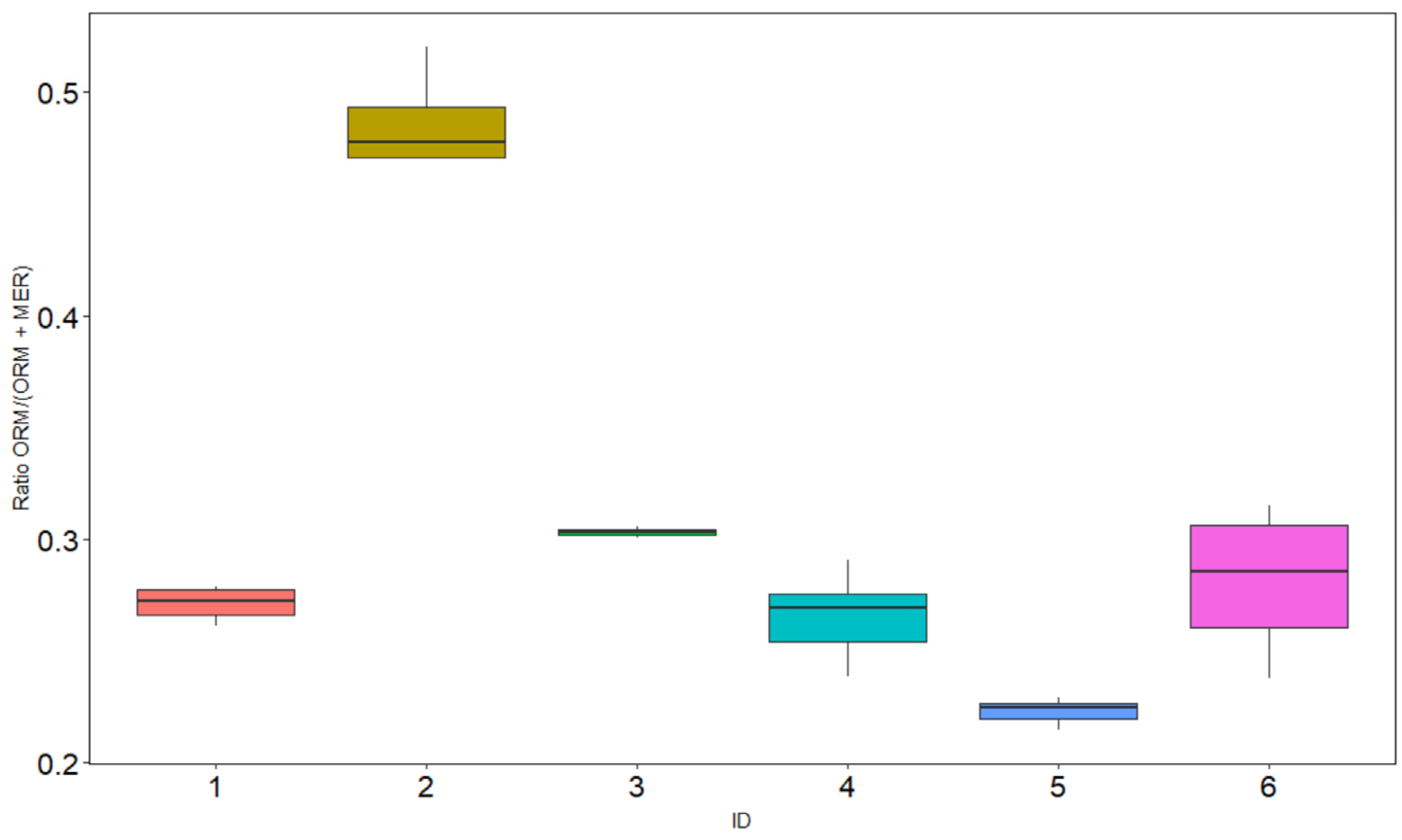
2.3. Pharmacokinetics in Patients
3. Discussion
4. Materials and Methods
4.1. Chemicals and Reagents
4.2. Infusate Stability at Room Temperature
4.3. Stability in Serum
4.4. Laboratory Testing and ID-LC-MS/MS Analysis
4.5. Calculation of In Vitro Elimination Rate Constants
4.6. Patient Serum Testing
4.7. Population Pharmacokinetic Modelling
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Baldwin, C.M.; Lyseng-Williamson, K.A.; Keam, S.J. Meropenem: A review of its use in the treatment of serious bacterial infections. Drugs 2008, 68, 803–838. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.A.; Norris, R.; Paterson, D.; Martin, J. Therapeutic drug monitoring of antimicrobials. Br. J. Clin. Pharmacol. 2011, 73, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Guilhaumou, R.; Benaboud, S.; Bennis, Y.; Dahyot-Fizelier, C.; Dailly, E.; Gandia, P.; Goutelle, S.; Lefeuvre, S.; Mongardon, N.; Roger, C.; et al. Optimization of the treatment with beta-lactam antibiotics in critically ill pa-tients-guidelines from the French Society of Pharmacology and Therapeutics (Societe Francaise de Pharmacologie et Thera-peutique-SFPT) and the French Society of Anaesthesia and Intensive Care Medicine (Societe Francaise d’Anesthesie et Rean-imation-SFAR). Crit. Care 2019, 23, 104. [Google Scholar] [PubMed]
- Ehmann, L.; Zoller, M.; Minichmayr, I.K.; Scharf, C.; Maier, B.; Schmitt, M.V.; Hartung, N.; Huisinga, W.; Vogeser, M.; Frey, L.; et al. Role of renal function in risk assessment of target non-attainment after standard dosing of meropenem in critically ill patients: A prospective observational study. Crit. Care 2017, 21, 1–14. [Google Scholar] [CrossRef]
- Wu, C.-C.; Tai, C.H.; Liao, W.-Y.; Wang, C.-C.; Kuo, C.-H.; Lin, S.-W.; Ku, S.-C. Augmented renal clearance is associated with inadequate antibiotic pharmacokinetic/pharmacodynamic target in Asian ICU population: A prospective observational study. Infect. Drug Resist. 2019, 12, 2531–2541. [Google Scholar] [CrossRef] [PubMed]
- Scharf, C.; Paal, M.; Schroeder, I.; Vogeser, M.; Draenert, R.; Irlbeck, M.; Zöller, M.; Liebchen, U. Therapeutic Drug Monitoring of Meropenem and Piperacillin in Critical Illness—Experience and Recommendations from One Year in Routine Clinical Practice. Antibiotics 2020, 9, 131. [Google Scholar] [CrossRef] [PubMed]
- Paul-Ehrlich-Gesellschaft für Chemotherapie e.V. (PEG). S2k Leitlinie: Kalkulierte Parenterale Initialtherapie Bakterieller Erkrankungen bei Erwachsenen–Update 2018. Available online: https://www.Awmf.Org/uploads/tx_szleitlinien/082-006l_s2k_parenterale_antibiotika_2019-08.Pdf (accessed on 15 March 2021).
- Chen, P.; Chen, F.; Lei, J.; Zhou, B. Clinical outcomes of continuous vs intermittent meropenem infusion for the treatment of sepsis: A systematic review and meta-analysis. Adv. Clin. Exp. Med. 2020, 29, 993–1000. [Google Scholar] [CrossRef]
- Liebchen, U.; Paal, M.; Scharf, C.; Schroeder, I.; Grabein, B.; Zander, J.; Siebers, C.; Zoller, M. The ONTAI study—A survey on anti-microbial dosing and the practice of therapeutic drug monitoring in German intensive care units. J. Crit. Care 2020, 60, 260–266. [Google Scholar] [CrossRef]
- Farmer, E.C.W.; Seaton, R.A. Recent innovations and new applications of outpatient parenteral antimicrobial therapy. Expert Rev. Anti Infect. Ther. 2021, 19, 55–64. [Google Scholar] [CrossRef]
- Pharmacopoeia, J. European Pharmacopoeia, 10th ed.; Supplement 10.1, 10.2 and 10.3; Council of Europe: Strasbourg, France, 2020. [Google Scholar]
- United States Pharmacopeia: United States Pharmacopeia and National Formulary (USP 41-NF 36). 2016. Available online: https://online.uspnf.com/uspnf/document/GUID-AC788D41-90A2-4F36-A6E7-769954A9ED09_1_en-US (accessed on 15 February 2021).
- Takeuchi, Y.; Sunagawa, M.; Isobe, Y.; Hamazume, Y.; Noguchi, T. Stability of a 1.BETA.-Methylcarbapenem Antibiotic, Meropenem (SM-7338) in Aqueous Solution. Chem. Pharm. Bull. 1995, 43, 689–692. [Google Scholar] [CrossRef]
- Patel, P.R.; Cook, S.E. Stability of meropenem in intravenous solutions. Am. J. Health Syst. Pharm. 1997, 54, 412–421. [Google Scholar] [CrossRef]
- Mendez, A.S.; Dalomo, J.; Steppe, M.; Schapoval, E. Stability and degradation kinetics of meropenem in powder for injection and reconstituted sample. J. Pharm. Biomed. Anal. 2006, 41, 1363–1366. [Google Scholar] [CrossRef]
- Franceschi, L.; Cojutti, P.G.; Baraldo, M.; Pea, F. Stability of Generic Meropenem Solutions for Administration by Continuous Infusion at Normal and Elevated Temperatures. Ther. Drug Monit. 2014, 36, 674–676. [Google Scholar] [CrossRef] [PubMed]
- Carlier, M.; Stove, V.; Verstraete, A.; De Waele, J.J. Stability of generic brands of meropenem reconstituted in isotonic saline. Minerva Anestesiol. 2014, 81, 283–287. [Google Scholar] [PubMed]
- Takasu, Y.; Yoshida, M.; Tange, M.; Asahara, K.; Uchida, T. Prediction of the Stability of Meropenem in Intravenous Mixtures. Chem. Pharm. Bull. 2015, 63, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Mendes, K.; Harmanjeet, H.; Sedeeq, M.; Modi, A.; Wanandy, T.; Zaidi, S.T.R.; Ming, L.C.; Castelino, R.L.; Sud, K.; Peterson, G.M.; et al. Stability of Meropenem and Piperacillin/Tazobactam with Heparin in Various Peritoneal Dialysis Solutions. Perit. Dial. Int. 2018, 38, 430–440. [Google Scholar] [CrossRef] [PubMed]
- Foy, F.; Luna, G.; Martinez, J.; Nizich, Z.; Seet, J.; Lie, K.; Sunderland, B.; Czarniak, P. An investigation of the stability of meropenem in elastomeric infusion devices. Drug Des. Dev. Ther. 2019, 13, 2655–2665. [Google Scholar] [CrossRef] [PubMed]
- Fawaz, S.; Barton, S.; Whitney, L.; Swinden, J.; Nabhani-Gebara, S. Stability of Meropenem after Reconstitution for Administration by Prolonged Infusion. Hosp. Pharm. 2019, 54, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Jamieson, C.; Allwood, M.C.; Stonkute, D.; Wallace, A.; Wilkinson, A.-S.; Hills, T. Investigation of meropenem stability after reconstitution: The influence of buffering and challenges to meet the NHS Yellow Cover Document compliance for continuous infusions in an outpatient setting. Eur. J. Hosp. Pharm. 2019, 27, e53–e57. [Google Scholar] [CrossRef] [PubMed]
- Akahane, M.; Enoki, Y.; Saiki, R.; Hayashi, Y.; Hiraoka, K.; Honma, K.; Itagaki, M.; Gotoda, M.; Shinoda, K.; Hanyu, S.; et al. Stability of antimicrobial agents in an elastomeric infusion pump used for outpatient parenteral antimicrobial therapy. Int. J. Infect. Dis. 2021, 103, 464–468. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, F.D.S.; Pezzi, L.C.; Tsao, M.; Macedo, S.M.D.; Oliveira, T.; Schapoval, E.E.; Mendez, A.S. Stability in clinical use and stress testing of meropenem antibiotic by direct infusion ESI-Q-TOF: Quantitative method and identification of degradation products. J. Pharm. Biomed. Anal. 2020, 179, 112973. [Google Scholar] [CrossRef] [PubMed]
- Moon, Y.S.K.; Chung, K.C.; Gill, M.A. Pharmacokinetics of Meropenem in Animals, Healthy Volunteers, and Patients. Clin. Infect. Dis. 1997, 24, S249–S255. [Google Scholar] [CrossRef]
- Mattioli, F.; Fucile, C.; Del Bono, V.; Marini, V.; Parisini, A.; Molin, A.; Zuccoli, M.L.; Milano, G.; Danesi, R.; Marchese, A.; et al. Population pharmacokinetics and probability of target attainment of meropenem in critically ill patients. Eur. J. Clin. Pharmacol. 2016, 72, 839–848. [Google Scholar] [CrossRef] [PubMed]
- Manning, L.; Wright, C.; Ingram, P.R.; Whitmore, T.J.; Heath, C.H.; Manson, I.; Page-Sharp, M.; Salman, S.; Dyer, J.; Davis, T.M.E. Continuous Infusions of Meropenem in Ambulatory Care: Clinical Efficacy, Safety and Stability. PLoS ONE 2014, 9, e102023. [Google Scholar] [CrossRef]
- Kuti, J.L.; Nightingale, C.H.; Knauft, R.F.; Nicolau, D.P. Pharmacokinetic properties and stability of continuous-infusion mero-penem in adults with cystic fibrosis. Clin. Ther. 2004, 26, 493–501. [Google Scholar] [CrossRef]
- Venugopalan, V.; Manigaba, K.; Borgert, S.J.; Cope, J.A.; Peloquin, C.; Klinker, K.P. Training a Drug to Do New Tricks: Insights on Stability of Meropenem Administered as a Continuous Infusion. Microbiol. Insights 2018, 11, 1178636118804549. [Google Scholar] [CrossRef]
- Legg, A.; Halford, M.; McCarthy, K. Plasma concentrations resulting from continuous infusion of meropenem in a communi-ty-based outpatient program: A case series. Am. J. Health Syst. Pharm. 2020, 77, 2074–2080. [Google Scholar] [CrossRef] [PubMed]
- Berthoin, K.; Le Duff, C.S.; Marchand-Brynaert, J.; Carryn, S.; Tulkens, P.M. Stability of meropenem and doripenem solutions for administration by continuous infusion. J. Antimicrob. Chemother. 2010, 65, 1073–1075. [Google Scholar] [CrossRef]
- Gijsen, M.; Filtjens, B.; Annaert, P.; Armoudjian, Y.; Debaveye, Y.; Wauters, J.; Slaets, P.; Spriet, I. Meropenem Stability in Human Plasma at −20 degrees C: Detailed Assessment of Degradation. Antibiotics 2021, 10, 449. [Google Scholar] [CrossRef] [PubMed]
- Harrison, M.P.; Haworth, S.J.; Moss, S.R.; Wilkinson, D.M.; Featherstone, A. The disposition and metabolic fate of 14C-meropenem in man. Xenobiotica 1993, 23, 1311–1323. [Google Scholar] [CrossRef] [PubMed]
- Craig, W.A. The Pharmacology of Meropenem, a New Carbapenem Antibiotic. Clin. Infect. Dis. 1997, 24, S266–S275. [Google Scholar] [CrossRef]
- Ljungberg, B.; Nilsson-Ehle, I. Pharmacokinetics of meropenem and its metabolite in young and elderly healthy men. Antimicrob. Agents Chemother. 1992, 36, 1437–1440. [Google Scholar] [CrossRef][Green Version]
- Christensson, B.; Nilsson-Ehle, I.; Hutchison, M.; Haworth, S.J.; Oqvist, B.; Norrby, S.R. Pharmacokinetics of meropenem in subjects with various degrees of renal impairment. Antimicrob. Agents Chemother. 1992, 36, 1532–1537. [Google Scholar] [CrossRef] [PubMed]
- Leroy, A.; Fillastre, J.P.; Borsa-Lebas, F.; Etienne, I.; Humbert, G. Pharmacokinetics of meropenem (ICI 194,660) and its metabolite (ICI 213,689) in healthy subjects and in patients with renal impairment. Antimicrob. Agents Chemother. 1992, 36, 2794–2798. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Minichmayr, I.K.; Roberts, J.A.; Frey, O.R.; Roehr, A.C.; Kloft, C.; Brinkmann, A. Development of a dosing nomogram for con-tinuous-infusion meropenem in critically ill patients based on a validated population pharmacokinetic model. J. Antimicrob. Chemother. 2018, 73, 1330–1339. [Google Scholar] [CrossRef] [PubMed]
- Ehmann, L.; Zoller, M.; Minichmayr, I.K.; Scharf, C.; Huisinga, W.; Zander, J.; Kloft, C. Development of a dosing algorithm for meropenem in critically ill patients based on a population pharmacokinetic/pharmacodynamic analysis. Int. J. Antimicrob. Agents 2019, 54, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Kratzer, A.; Liebchen, U.; Schleibinger, M.; Kees, M.G.; Kees, F. Determination of free vancomycin, ceftriaxone, cefazolin and ertapenem in plasma by ultrafiltration: Impact of experimental conditions. J. Chromatogr. B 2014, 961, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Rakete, S.; Schuster, C.; Paal, M.; Vogeser, M. An isotope-dilution LC-MS/MS method for the simultaneous quantification of meropenem and its open-ring metabolite in serum. J. Pharm. Biomed. Anal. 2021, 197, 113944. [Google Scholar] [CrossRef] [PubMed]
- Seger, C.; Salzmann, L. After another decade: LC–MS/MS became routine in clinical diagnostics. Clin. Biochem. 2020, 82, 2–11. [Google Scholar] [CrossRef]
- Chapman, A.L.N.; Patel, S.; Horner, C.; Gilchrist, M.; Seaton, R.A. Outpatient parenteral antimicrobial therapy: Updated recommendations from the UK. J. Antimicrob. Chemother. 2019, 74, 3125–3127. [Google Scholar] [CrossRef] [PubMed]
- Liebchen, U.; Dorn, C.; Kees, M.; Schiesser, S.; Hitzenbichler, F.; Kees, F.; Paal, M. Comment on “Meropenem, Cefepime, and Piperacillin Protein Binding in Patient Samples”. Ther. Drug Monit. 2020, 42, 909–910. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristic [Unit] | Number/Median (Range) |
|---|---|
| No. of patients | 6 |
| No. of male patients | 4 |
| No. of samples | 24 |
| Meropenem concentration [mg/L] | 19.74 (7.25–31.25) |
| Open-ring metabolite (ORM) concentration [mg/L] | 7.73 (2.71–23.37) |
| Meropenem daily dose [g/24 h] | 6 (3–6) |
| Age [years] | 46 (35–72) |
| Weight [kg] | 86 (47–170) |
| Glomerular filtration rate [mL/min] | 139 (28–307) |
| Parameter Estimates (RSE, %) [Shrinkage, %] | |
|---|---|
| Meropenem | |
| Parameter [unit] | 1-CMT Model |
| OFV | 121.8 |
| Fixed-effects Parameter | |
| CLGFR [L/h] | 7.1 |
| CLnonGFR | 3.6 (28) |
| CLdecay | 0.66 |
| V [L] | 26.2 |
| Interindividual variability | |
| ω CL (CV %) | 14.9 (18) [2] |
| Residual variability | |
| σ Prop. (CV %) | 13.5% (20) [11] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liebchen, U.; Rakete, S.; Vogeser, M.; Arend, F.M.; Kinast, C.; Scharf, C.; Zoller, M.; Schönermarck, U.; Paal, M. The Role of Non-Enzymatic Degradation of Meropenem—Insights from the Bottle to the Body. Antibiotics 2021, 10, 715. https://doi.org/10.3390/antibiotics10060715
Liebchen U, Rakete S, Vogeser M, Arend FM, Kinast C, Scharf C, Zoller M, Schönermarck U, Paal M. The Role of Non-Enzymatic Degradation of Meropenem—Insights from the Bottle to the Body. Antibiotics. 2021; 10(6):715. https://doi.org/10.3390/antibiotics10060715
Chicago/Turabian StyleLiebchen, Uwe, Sophie Rakete, Michael Vogeser, Florian M. Arend, Christina Kinast, Christina Scharf, Michael Zoller, Ulf Schönermarck, and Michael Paal. 2021. "The Role of Non-Enzymatic Degradation of Meropenem—Insights from the Bottle to the Body" Antibiotics 10, no. 6: 715. https://doi.org/10.3390/antibiotics10060715
APA StyleLiebchen, U., Rakete, S., Vogeser, M., Arend, F. M., Kinast, C., Scharf, C., Zoller, M., Schönermarck, U., & Paal, M. (2021). The Role of Non-Enzymatic Degradation of Meropenem—Insights from the Bottle to the Body. Antibiotics, 10(6), 715. https://doi.org/10.3390/antibiotics10060715