
Assessment of Appropriateness of Antimicrobial Therapy in Resource-Constrained Settings: Development and Piloting of a Novel Tool—AmRAT

 ,
,
Abstract
:1. Introduction
2. Methodology
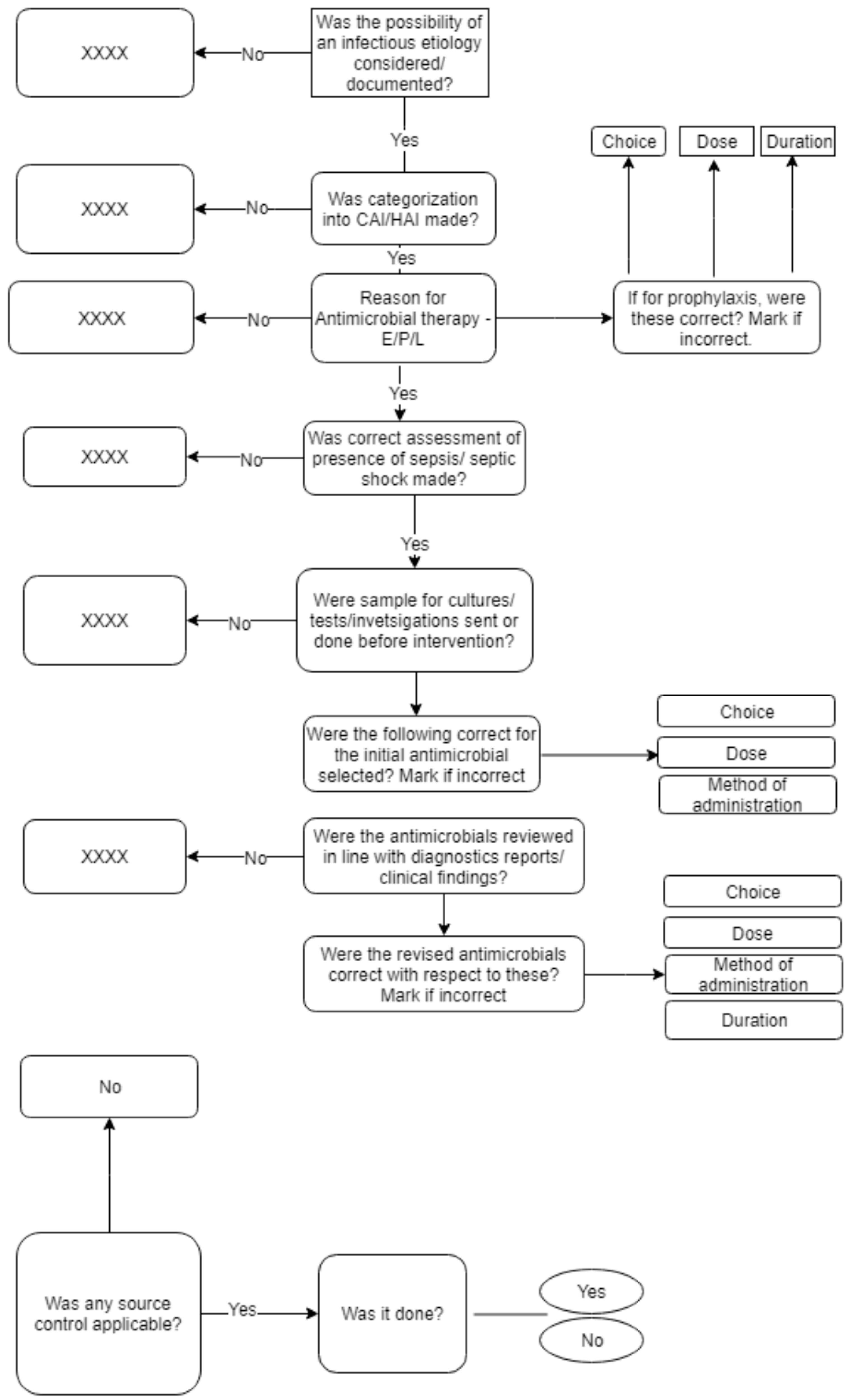
2.1. Development of Antimicrobial Rational Assessment Tool (AmRAT)
2.2. Piloting the AmRAT
2.3. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Ad hoc Interagency Coordination Group on Antimicrobial Resistance. No Time to Wait: Securing the Future from Drug-Resistant Infections. Available online: https://www.who.int/antimicrobial-resistance/interagency-coordination-group/IACG_final_report_EN.pdf?ua=1 (accessed on 21 December 2020).
- Klein, E.Y.; Milkowska-Shibata, M.; Tseng, K.K.; Sharland, M.; Gandra, S.; Pulcini, C.; Laxminarayan, R. Assessment of WHO antibiotic consumption and access targets in 76 countries, 2000–2015: An analysis of pharmaceutical sales data. Lancet Infect. Dis. 2021, 21, 107–115. [Google Scholar] [CrossRef]
- Panditrao, A.M.; Shafiq, N.; Chatterjee, S.; Pathak, A.; Trivedi, N.; Sadasivam, B.; Kshirsagar, N.; Kaul, R.; Biswal, M.; Kakkar, A.; et al. A multicentre point prevalence survey (PPS) of antimicrobial use amongst admitted patients in tertiary care centres in India. J. Antimicrob. Chemother. 2020. [Google Scholar] [CrossRef]
- Klein, E.Y.; Van Boeckel, T.P.; Martinez, E.M.; Pant, S.; Gandra, S.; Levin, S.A.; Goossens, L.; Laxminarayan, R. Global increase and geographic convergence in antibiotic con-sumption between 2000 and 2015. Proc. Natl. Acad. Sci. USA 2018, 10, E3463–E3470. [Google Scholar] [CrossRef] [Green Version]
- McCloskey, B.; Dar, O.; Zumla, A.; Heymann, D.L. Emerging infectious diseases and pandemic potential: Status quo and reducing risk of global spread. Lancet Infect. Dis. 2014, 14, 1001–1010. [Google Scholar] [CrossRef]
- World Health Organization. Regional Office for South-East Asia. A Brief Guide to Emerging Infectious Diseases and Zoonoses. 2014. Available online: https://apps.who.int/iris/handle/10665/204722 (accessed on 25 January 2021).
- Napolitani, M.; Troiano, G.; Bedogni, C.; Messina, G.; Nante, N. Kocuria kristinae: An emerging pathogen in medical practice. J. Med. Microbiol. 2019, 68, 1596–1603. [Google Scholar] [CrossRef]
- Holmes, A.H.; Moore, L.S.P.; Sundsfjord, A.; Steinbakk, M.; Regmi, S.; Karkey, A.; Guerin, P.J.; Piddock, L.J.V. Understanding the mechanisms and drivers of antimicrobial resistance. Lancet 2016, 387, 176–187. [Google Scholar] [CrossRef]
- Laxminarayan, R.; Chaudhury, R.R. Antibiotic resistance in India: Drivers and opportunities for action. PLoS Med. 2016, 13, e1001974. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. WHO Fact Sheet. Antimicrobial Resistance. Available online: https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance (accessed on 15 December 2020).
- Castro-Sánchez, E.; Moore, L.S.P.; Husson, F.; Holmes, A.H. What are the factors driving antimicrobial resistance? Perspectives from a public event in London, England. BMC Infect. Dis. 2016, 16, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Butler, M.S.; Paterson, D.L. Antibiotics in the clinical pipeline in October 2019. J. Antibiot. 2020, 73, 329–364. [Google Scholar] [CrossRef]
- Slogan and Theme Announced for World Antimicrobial Awareness Week (WAAW). Available online: https://www.who.int/news/item/21-06-2020-slogan-and-theme-announced-for-world-antimicrobial-awareness-week-(waaw) (accessed on 7 January 2021).
- Global Action Plan on Antimicrobial Resistance. Available online: https://www.who.int/antimicrobial-resistance/global-action-plan/en/ (accessed on 24 August 2020).
- WHO Report on Surveillance of Antibiotic Consumption: 2016-2018 Early Implementation; World Health Organization: Genève, Switzerland, 2018.
- Cecchini, M.; Langer, J.; Slawomirski, L. Antimicrobial Resistance in G7 Countries and Beyond—Economic Issues, Policies and Options for Action; Organisation for Economic Co-operation and Development: Paris, France, 2015; pp. 1–75. [Google Scholar]
- Office-Related Antibiotic Prescribing for Persons Aged ≤14 Years-United States, 1993–1994 to 2007–2008. Available online: https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6034a1.htm (accessed on 21 December 2020).
- Pichichero, M.E. Dynamics of antibiotic prescribing for children. JAMA 2002, 287, 3133–3135. [Google Scholar] [CrossRef]
- Shapiro, D.J.; Hicks, L.A.; Pavia, A.T.; Hersh, A.L. Antibiotic prescribing for adults in ambulatory care in the USA, 2007–2009. J. Antimicrob. Chemother. 2014, 69, 234–240. [Google Scholar] [CrossRef] [Green Version]
- Morrill, H.J.; Caffrey, A.R.; Gaitanis, M.M.; LaPlante, K.L. Impact of a prospective audit and feedback antimicrobial stewardship program at a veterans affairs medical center: A six-point assessment. PLoS ONE 2016, 15, e0150795. [Google Scholar] [CrossRef] [PubMed]
- Fowler, S.; Webber, A.; Cooper, B.S.; Phimister, A.; Price, K.; Carter, Y.; Kibbler, C.C.; Simpson, A.J.H.; Stone, S.P. Successful use of feedback to improve antibiotic prescribing and reduce Clostridium difficile infection: A controlled interrupted time series. J. Antimicrob. Chemother. 2007, 59, 990–995. [Google Scholar] [CrossRef] [PubMed]
- Crayton, E.; Richardson, M.; Fuller, C.; Smith, C.; Liu, S.; Forbes, G.; Anderson, N.; Shallcross, L.; Michie, S.; Hayward, A.; et al. Interventions to improve appropriate antibiotic prescribing in long-term care facilities: A systematic review. BMC Geriatr. 2020, 20, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Arnold, F.W.; McDonald, L.C.; Smith, R.S.; Newman, D.; Ramirez, J.A. Improving antimicrobial use in the hospital setting by providing usage feed-back to prescribing physicians. Infect Control Hosp Epidemiol. 2006, 27, 378–382. [Google Scholar] [CrossRef] [PubMed]
- Rawson, T.M.; Moore, L.S.; Hernandez, B.; Charani, E.; Castro-Sanchez, E.; Herrero, P.; Hayhoe, B.; Hope, W.; Georgiou, P.; Holmes, A.H. A systematic review of clinical decision support sys-tems for antimicrobial management: Are we failing to investigate these interventions appropriately? Clin. Microbiol. Infect. 2017, 1, 524–532. [Google Scholar] [CrossRef] [Green Version]
- Kakkar, A.K.; Shafiq, N.; Malhotra, S. Ensuring access to ‘access’ antibiotics: An imminent consideration for sustainable antimicrobial steward-ship in the developing world. Infect Dis. 2019, 51, 395–398. [Google Scholar] [CrossRef]
- Kakkar, A.K.; Shafiq, N.; Malhotra, S. Cefazolin shortages in the developing world: The same, but different too. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Kakkar, A.K.; Shafiq, N.; Singh, G.; Ray, P.; Gautam, V.; Agarwal, R.; Muralidharan, J.; Arora, P. Antimicrobial stewardship programs in resource constrained environ-ments: Understanding and addressing the need of the systems. Front. Public Health 2020, 8. Available online: https://www.frontiersin.org/articles/10.3389/fpubh.2020.00140/full (accessed on 3 January 2021). [CrossRef]
- Kunin, C.M.; Tupasi, T.; Craig, W.A. Use of antibiotics. A brief exposition of the problem and some tentative solutions. Ann. Intern Med. 1973, 79, 555–560. [Google Scholar] [CrossRef]
- Implementation Resources | Antibiotic Use | CDC 2020. Available online: https://www.cdc.gov/antibiotic-use/core-elements/implementation.html (accessed on 7 January 2021).
- Guidance on Antimicrobial Stewardship: Start Smart-Then Focus. Available online: https://www.gov.uk/government/publications/antimicrobial-stewardship-start-smart-then-focus (accessed on 7 January 2021).
- Monnier, A.; Eisenstein, B.E.; Hulscher, M.; Gyssens, I.C.; Adriaenssens, N.; Huttner, B.; Le Maréchal, M.; Milanič, R.; Pulcini, C.; Benić, M.S.; et al. Towards a global definition of responsible antibiotic use: Results of an international multidisciplinary consensus procedure. J. Antimicrob. Chemother. 2018, 73, vi3–vi16. [Google Scholar] [CrossRef]
- Home-Sanford Guide-Antimicrobial Stewardship. Available online: https://www.sanfordguide.com/ (accessed on 7 January 2021).
- Evidence-Based Clinical Decision Support at the Point of Care | UpToDate. Available online: https://www.uptodate.com/home (accessed on 7 January 2021).
- An Introduction to the Bootstrap; Routledge & CRC Press; Available online: https://www.routledge.com/An-Introduction-to-the-Bootstrap/Efron-Tibshirani/p/book/9780412042317 (accessed on 7 January 2021).
- Lee, J.; Fung, K. Confidence interval of the kappa coefficient by bootstrap resampling. Psychiatry Res. 1993, 49, 97–98. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- StataCorp, Version, Stata Statistical Software: Release 16; StataCorp LLC.: College Station, TX, USA, 2019.
- Spivak, E.S.; Cosgrove, S.E.; Srinivasan, A. Measuring appropriate antimicrobial use: Attempts at opening the black box. Clin. Infect. Dis. 2016, 63, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Casaroto, E.; Marra, A.R.; Camargo, T.Z.S.; De Souza, A.R.A.; De Almeida, C.E.S.; Pedroti, E.P.; Victor, E.D.S.; Dos Santos, O.F.; Edmond, M.B.; Campos, A.H. Agreement on the prescription of antimicrobial drugs. BMC Infect. Dis. 2015, 15, 248. [Google Scholar] [CrossRef] [Green Version]
- Bebell, L.; Muiru, A. Antibiotic use and emerging resistance—how can resource-limited countries turn the tide? Glob. Heart 2014, 9, 347–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cusini, A.; Rampini, S.K.; Bansal, V.; Ledergerber, B.; Kuster, S.P.; Ruef, C.; Weber, R. Different patterns of inappropriate antimicrobial use in surgical and medical units at a tertiary care hospital in switzerland: A prevalence survey. PLoS ONE 2010, 5, e14011. [Google Scholar] [CrossRef]
- Grtler, N.; Erba, A.; Giehl, C.; Tschudin-Sutter, S.; Bassetti, S.; Osthoff, M.; Gürtler, N.; Giehl, C. Appropriateness of antimicrobial prescribing in a Swiss tertiary care hospital: A repeated point prevalence survey. Swiss Med. Wkly. 2019, 149, w20135. [Google Scholar] [CrossRef] [PubMed]
- Seaton, R.A.; Nathwani, D.; Burton, P.; McLaughlin, C.; MacKenzie, A.R.; Dundas, S.; Ziglam, H.; Gourlay, Y.; Beard, K.; Douglas, E. Point prevalence survey of antibiotic use in Scottish hos-pitals utilising the Glasgow Antimicrobial Audit Tool (GAAT). Int. J. Antimicrob. Agents 2007, 29, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Ellis, P.; Peters, C.; Ahsan, M.; Chateau, D.; Arabi, Y.; Roberts, D.; Light, B.; Parrillo, J.E.; Dodek, P.; et al. Initiation of inappropriate antimicrobial therapy results in a fivefold reduction of survival in human septic shock. Chest 2009, 136, 1237–1248. [Google Scholar] [CrossRef]
- Gyssens, I.C.; van den Broek, P.J.; Kullberg, B.J.; Hekster, Y.; van der Meer, J.W. Optimizing antimicrobial therapy. A method for antimicrobial drug use evaluation. J. Antimicrob. Chemother. 1992, 30, 724–727. [Google Scholar] [CrossRef]
- Raveh, D.; Levy, Y.; Schlesinger, Y.; Greenberg, A.; Rudensky, B.; Yinnon, A.M. Longitudinal surveillance of antibiotic use in the hospital. QJM Int. J. Med. 2001, 94, 141–152. [Google Scholar] [CrossRef] [Green Version]
- James, R.; Upjohn, L.; Cotta, M.; Luu, S.; Marshall, C.; Buising, K.; Thursky, K. Measuring antimicrobial prescribing quality in Australian hospitals: Devel-opment and evaluation of a national antimicrobial prescribing survey tool. J. Antimicrob. Chemother. 2015, 70, 1912–1918. [Google Scholar] [CrossRef] [Green Version]
- Feinstein, A.R.; Cicchetti, D.V. High agreement but low Kappa: I. the problems of two paradoxes. J. Clin. Epidemiol. 1990, 43, 543–549. [Google Scholar] [CrossRef]
- Viera, A.J.; Garrett, J.M. Understanding interobserver agreement: The kappa statistic. Fam. Med. 2005, 37, 360–363. [Google Scholar] [PubMed]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]

{kind=link}
| Observer | Agreement | Kappa (95% CI) | |
|---|---|---|---|
| Choice of antimicrobial | |||
| Group A | 1 | 93.3% | 0.79 (0.50,1.00) |
| 2 | 76.7% | 0.38 (−0.02,0.78) | |
| 3 | 73.3% | 0.4 (0.03,0.77) | |
| Mean | 81.1% | ||
| Group B | 1 | 86.7% | 0.66 (0.33,0.98) |
| 2 | 76.7% | 0.46 (0.10,0.82) | |
| 3 | 80.0% | 0.28 (−0.18,0.74) | |
| Mean | 81.1% | ||
| Group C | 1 | 83.3% | 0.56 (0.19,0.92) |
| 2 | 86.7% | 0.66 (0.33,0.98) | |
| 3 | 76.7% | 0.31 (−0.11,0.74) | |
| 4 | 80.0% | 0.38 (−0.06,0.81) | |
| Mean | 81.7% | ||
| Dose | |||
| Group A | 1 | 83.3% | 0.35 (−0.13,0.83) |
| 2 | 80.0% | 0.28 (−0.18,0.74) | |
| 3 | 80.0% | 0.49 (0.11,0.86) | |
| Mean | 81.1% | ||
| Group B | 1 | 86.7% | 0.66 (0.33,0.98) |
| 2 | 80.0% | 0.52 (0.17,0.88) | |
| 3 | 90.0% | 0.67 (0.30,1.00) | |
| Mean | 85.6% | ||
| Group C | 1 | 86.7% | 0.63 (0.27,0.98) |
| 2 | 86.7% | 0.63 (0.27,0.98) | |
| 3 | 83.3% | 0.51 (0.11,0.91) | |
| 4 | 86.7% | 0.58 (0.19,0.97) | |
| Mean | 85.8% | ||
| Duration | |||
| Group A | 1 | 79.0% | 0.5 (0.02,0.98) |
| 2 | 87.5% | 0.73 (0.28,1) | |
| 3 | 100.0% | 1.00 (0.72,1.00) | |
| Mean | 88.0% | ||
| Group B | 1 | 81.2 % | 0.56 (0.03,1.00) |
| 2 | 87.5% | 0.73 (0.28,1.00) | |
| 3 | 86.7% | 0.68 (0.17,1.00) | |
| Mean | 85.1% | ||
| Group C | 1 | 76.5% | 0.48 (−0.03,0.99) |
| 2 | 81.3% | 0.57 (0.05,1.00) | |
| 3 | 100.0% | 1.00 (0.65,1.00) | |
| 4 | 92.9% | 0.84 (0.41,1.00) | |
| Mean | 86.7% | ||
| Overall rationality | |||
| Group A | 1 | 80.0% | 0.57 (0.25,0.89) |
| 2 | 76.7% | 0.52 (0.19,0.85) | |
| 3 | 73.3% | 0.47 (0.13,0.80) | |
| Mean | 76.7% | ||
| Group B | 1 | 73.3% | 0.46 (0.13,0.80) |
| 2 | 63.3% | 0.22 (−0.15,0.60) | |
| 3 | 70.0% | 0.34 (−0.03,0.71) | |
| Mean | 68.9% | ||
| Group C | 1 | 80.0% | 0.60 (0.29,0.90) |
| 2 | 80.0% | 0.60 (0.29,0.90) | |
| 3 | 80.0% | 0.59 (0.28,0.90) | |
| 4 | 70.0% | 0.37 (0.00,0.73) | |
| Mean | 77.5% | ||
| % Agreement (95% CI) | Kappa (95% CI) | |
|---|---|---|
| Group A | ||
| Choice | 64.4 (51.8,77.1) | 0.19 (−0.1,0.47) |
| Dose | 77.8 (65.8,89.7) | 0.15 (−0.03,0.33) |
| Duration | 81.3 (56.2,100) | 0.60 (0.2,1.00) |
| Overall rationality | 62.2 (49.7,74.8) | 0.21 (−0.06,0.47) |
| Group B | ||
| Choice | 71.1 (58.6,83.7) | 0.31 (0.04,0.59) |
| Dose | 75.6 (63.4,87.8) | 0.38 (0.09,0.66) |
| Duration | 81.3 (60.1,100) | 0.59 (0.2,0.99) |
| Overall rationality | 55.6 (43.6,67.5) | 0.11 (−0.13,0.35) |
| Group C | ||
| Choice | 68.9 (58.3,79.5) | 0.20 (−0.01,0.42) |
| Dose | 79.4 (69,89.9) | 0.38 (0.14,0.61) |
| Duration | 82.3 (61.7,100) | 0.62 (0.27,0.98) |
| Overall rationality | 66.1 (55.3,76.9) | 0.30 (0.09,0.51) |
| Percent | 95% CI | ||
|---|---|---|---|
| Choice of Antimicrobial | |||
| Sensitivity | 82.5% | 77.1% | 87.1% |
| Specificity | 76.7% | 64.0% | 86.6% |
| Dose | |||
| Sensitivity | 91.3% | 86.9% | 94.6% |
| Specificity | 61.4% | 49.0% | 72.8% |
| Duration | |||
| Sensitivity | 92.4% | 84.9% | 96.9% |
| Specificity | 78.5% | 66.5% | 87.7% |
| Overall Rationality | |||
| Sensitivity | 80.00% | 73.00% | 85.90% |
| Specificity | 68.60% | 60.20% | 76.10% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kakkar, A.K.; Shafiq, N.; Sahni, N.; Mohindra, R.; Kaur, N.; Gamad, N.; Panditrao, A.; Kondal, D.; Malhotra, S.; Kumar M, P.; et al. Assessment of Appropriateness of Antimicrobial Therapy in Resource-Constrained Settings: Development and Piloting of a Novel Tool—AmRAT. Antibiotics 2021, 10, 200. https://doi.org/10.3390/antibiotics10020200
Kakkar AK, Shafiq N, Sahni N, Mohindra R, Kaur N, Gamad N, Panditrao A, Kondal D, Malhotra S, Kumar M P, et al. Assessment of Appropriateness of Antimicrobial Therapy in Resource-Constrained Settings: Development and Piloting of a Novel Tool—AmRAT. Antibiotics. 2021; 10(2):200. https://doi.org/10.3390/antibiotics10020200
Chicago/Turabian StyleKakkar, Ashish Kumar, Nusrat Shafiq, Neeru Sahni, Ritin Mohindra, Navjot Kaur, Nanda Gamad, Aditi Panditrao, Dimple Kondal, Samir Malhotra, Praveen Kumar M, and et al. 2021. "Assessment of Appropriateness of Antimicrobial Therapy in Resource-Constrained Settings: Development and Piloting of a Novel Tool—AmRAT" Antibiotics 10, no. 2: 200. https://doi.org/10.3390/antibiotics10020200
APA StyleKakkar, A. K., Shafiq, N., Sahni, N., Mohindra, R., Kaur, N., Gamad, N., Panditrao, A., Kondal, D., Malhotra, S., Kumar M, P., Rohilla, R., Bhattacharjee, S., Kumar, A., Bhandari, R. K., Pandey, A. K., Rather, I., Mothsara, C., Harish, C., Belavagi, D., & Vishwas, G. (2021). Assessment of Appropriateness of Antimicrobial Therapy in Resource-Constrained Settings: Development and Piloting of a Novel Tool—AmRAT. Antibiotics, 10(2), 200. https://doi.org/10.3390/antibiotics10020200