Recent Progress in Surface Plasmon Resonance Biosensors (2016 to Mid-2018)


Abstract
1. Introduction
2. Stages of Biosensor Development
- The biosensor is used only for the detection of a marker;
- The biosensor is characterized in terms of quantitative marker determination (calibration graph, the marker concentration range covered by the biosensor);
- The biosensor and related analytical procedure are validated (precision, recovery, interferences, comparison of results with another procedure such as ELISA, examples of natural samples, e.g., blood plasma);
- The mature biosensor and the analytical procedure are used for investigation of the marker in significant series of clinical samples, including long control series of healthy donors;
- A fifth stage may be distinguished when the mature SPR biosensor and procedure are used in clinical investigation.
3. Fluidic vs. Non-Fluidic Measurements
4. Receptors
5. Enhancement of the SPR Signal
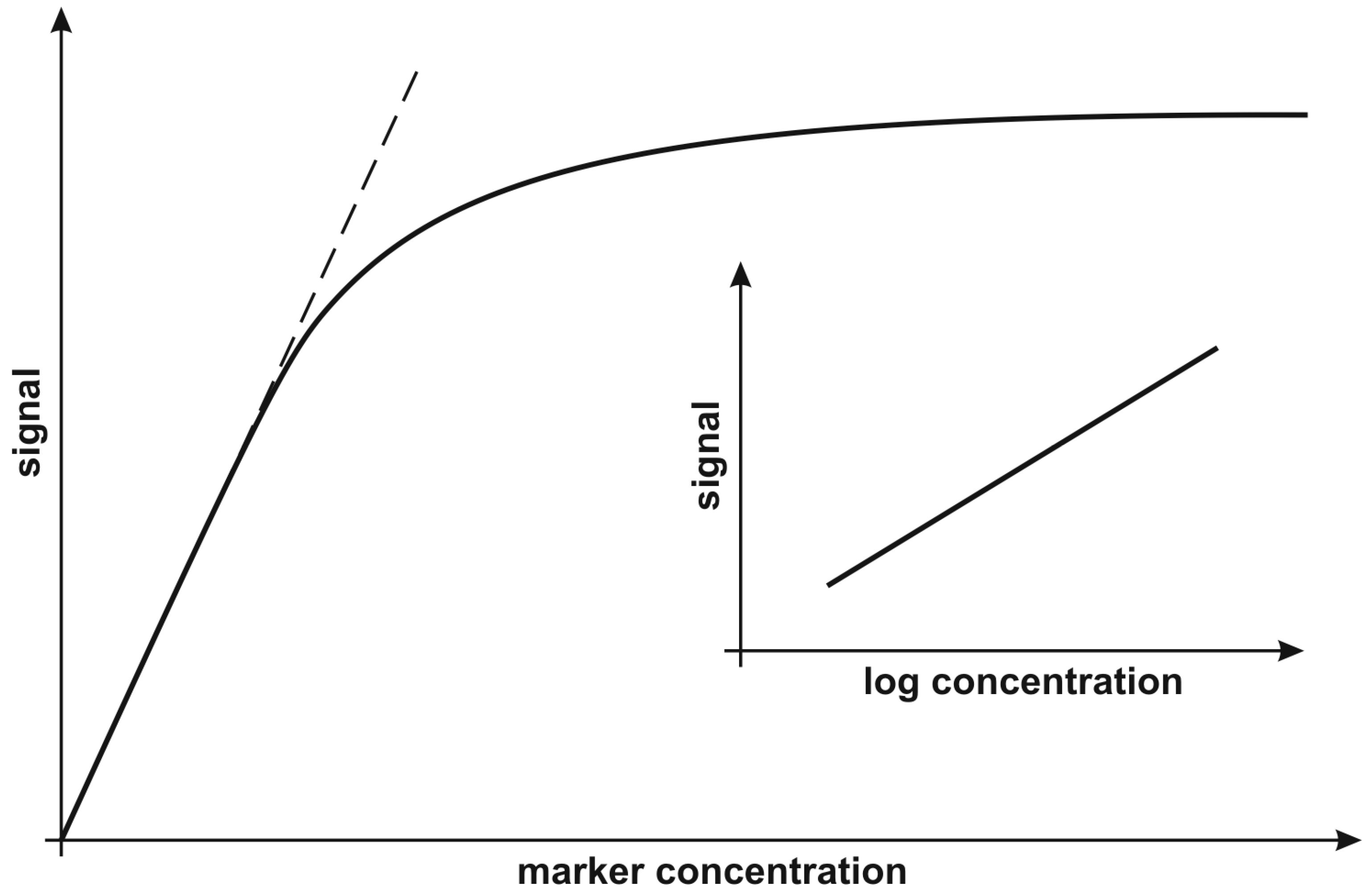
6. Calibration Strategy
7. Markers
8. Molecular Interactions
9. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Masson, J.-F. Surface Plasmon Resonance clinical biosensors for medical diagnostics. ACS Sens. 2017, 2, 16–30. [Google Scholar] [CrossRef] [PubMed]
- Ferhan, A.R.; Jackman, J.A.; Park, J.H.; Cho, N.-J.; Kim, D.-H. Nanoplasmonic sensors for detecting circulating cancer biomarkers. Adv. Drug Deliv. Rev. 2018, 125, 48–77. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, J.P.; de Oliveira, J.H.; Radovanovic, E.; Brolo, A.G.; Girotto, E.M. Microfluidic plasmonic biosensor for breast cancer antigen detection. Plasmonics 2016, 11, 45–51. [Google Scholar] [CrossRef]
- Xu, J.; Chen, Y. Surface Plasmon Resonance sensing with adjustable sensitivity based on a flexible liquid core coupling unit. Talanta 2018, 184, 468–474. [Google Scholar] [CrossRef] [PubMed]
- Ribaut, C.; Loyez, M.; Larrieu, J.-C.; Chevineau, S.; Lambert, P.; Remmelink, M.; Wattiez, R.; Caucheteur, C. Cancer biomarker sensing using packaged plasmonic optical fiber gratings: Towards in vivo diagnosis. Biosens. Bioelectr. 2017, 92, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Stojanović, I.; van Hal, Y.; van der Velden, T.J.G.; Schasfoort, R.B.M.; Terstappen, L.W.M.M. Detection of apoptosis in cancer cell lines using Surface Plasmon Resonance imaging. Sens. Bio-Sens. Res. 2016, 7, 48–54. [Google Scholar] [CrossRef]
- Chiu, N.-F.; Lin, T.-L.; Kuo, C.-T. Highly sensitive carboxyl-graphene oxide-based Surface Plasmon Resonance immunosensor for the detection of lung cancer for cytokeratin 19 biomarker in human plasma. Sens. Actuators B 2018, 265, 264–272. [Google Scholar] [CrossRef]
- Primo, E.N.; Bollo, S.; Rubianes, S.M.D.; Rivas, G.A. Immobilization of graphene-derived materials at gold surfaces: Towards a rational design of protein-based platforms for electrochemical and plasmonic applications. Electrochim. Acta 2018, 259, 723–732. [Google Scholar] [CrossRef]
- Jiang, L.; Zeng, S.; Xu, Z.; Ouyang, Q.; Zhang, D.-H.; Chong, P.H.J.; Coquet, P.; He, S.; Yong, K.-T. Multifunctional hyperbolic nanogroove metasurface for submolecular detection. Small 2017, 13, 1700600. [Google Scholar] [CrossRef]
- Chiu, N.-F.; Fan, S.-Y.; Yang, C.-D.; Huang, T.-Y. Carboxyl-functionalized graphene oxide composites as SPR biosensors with enhanced sensitivity for immunoaffinity detection. Biosens. Bioelectron. 2017, 89, 370–376. [Google Scholar] [CrossRef]
- Mayang, Y.; He, X.; Chen, L.; Zhang, Y. Detection of transferrin by using a Surface Plasmon Resonance sensor functionalized with a boronic acid monolayer. Microchim. Acta 2017, 184, 2749–2757. [Google Scholar] [CrossRef]
- Cao, Y.; Griffith, B.; Bhomkar, P.; Wishart, D.S.; McDermott, M.T. Functionalized gold nanoparticle-enhanced competitive assay for sensitive small-molecule metabolite detection using Surface Plasmon Resonance. Analyst 2018, 143, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Haber, J.M.; Gascoyne, P.R.C.; Sokolov, K. Rapid real-time recirculating PCR using Localized Surface Plasmon Resonance (LSPR) and piezoelectric pumping. Lab Chip 2017, 17, 2821–2830. [Google Scholar] [CrossRef] [PubMed]
- Erturk, G.; Ozen, H.; Tumer, M.A.; Mattiasson, B.; Denizli, A. Microcontact imprinting based Surface Plasmon Resonance (SPR) biosensor for real-time and ultrasensitive detection of prostate specific antigen (PSA) from clinical samples. Sens. Actuators B 2016, 224, 823–832. [Google Scholar] [CrossRef]
- Kim, D.-H.; Cho, I.-H.; Park, J.-N.; Paek, S.-H.; Cho, H.-M.; Paek, S.-H. Semi-continuous, real-time monitoring of protein biomarker using a recyclable Surface Plasmon Resonance sensor. Biosens. Bioelectr. 2017, 88, 232–239. [Google Scholar] [CrossRef]
- Palladino, P.; Minunni, M.; Scarano, S. Cardiac Troponin T capture and detection in real-time via epitope-imprinted polymer and optical biosensing. Biosens. Bioelectr. 2018, 106, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Sahu, V.; Gupta, A.; Kumar, R.; Gupta, T.; Mohan, A.; Dey, S. Quantification of Rac1 and Rac1b in serum of non small cell lung cancer by label free real time assay. Clin. Chim. Acta 2016, 460, 231–235. [Google Scholar] [CrossRef]
- Kumar, R.; Singh, A.K.; Kumar, M.; Shekhar, S.; Rai, N.; Kaur, P.; Parshad, R.; Dey, S. Serum 5-LOX: A progressive protein marker for breast cancer and new approach for therapeutic target. Carcinogenesis 2016, 37, 912–917. [Google Scholar] [CrossRef]
- Banerjee, J.; Pradhan, R.; Gupta, A.; Kumar, R.; Sahu, V.; Upadhyay, A.D.; Chaterjee, P.; Dwivedi, S.; Dey, S.; Dey, A.B. CDK4 in lung, and head and neck cancers in old age: Evaluation as a biomarker. Clin. Transl. Oncol. 2017, 19, 571–578. [Google Scholar] [CrossRef]
- Sankiewicz, A.; Romanowicz, L.; Laudanski, P.; Zelazowska-Rutkowska, B.; Puzan, B.; Cylwik, B.; Gorodkiewicz, E. SPR imaging biosensor for determination of laminin-5 as a potential cancer marker in biological material. Anal. Bioanal. Chem. 2016, 408, 5269–5276. [Google Scholar] [CrossRef]
- Sankiewicz, A.; Lukaszewski, Z.; Trojanowska, K.; Gorodkiewicz, E. Determination of collagen type IV by Surface Plasmon Resonance Imaging using a specific biosensor. Anal. Biochem. 2016, 515, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Tokarzewicz, A.; Romanowicz, L.; Sveklo, I.; Gorodkiewicz, E. The development of a matrix metalloproteinase-1 biosensor based on the Surface Plasmon Resonance imaging technique. Anal. Methods 2016, 8, 6428–6435. [Google Scholar] [CrossRef]
- Sankiewicz, A.; Markowska, A.; Lukaszewski, Z.; Puzan, B.; Gorodkiewicz, E. Methods for 20S Immunoproteasome and 20S Constitutive Proteasome Determination Based on SPRI Biosensors. Cell. Mol. Bioeng. 2017, 10, 174–185. [Google Scholar] [CrossRef]
- Tokarzewicz, A.; Romanowicz, L.; Sveklo, I.; Matuszczak, E.; Hermanowicz, A.; Gorodkiewicz, E. SPRI biosensors for quantitative determination of matrix metalloproteinase-2. Anal. Methods 2017, 9, 2407–2414. [Google Scholar] [CrossRef]
- Naglot, S.; Aggarwal, P.; Dey, S.; Dalal, K. Estimation of serum YKL-40 by Real-time Surface Plasmon Resonance Technology in North-Indian asthma patients. Clin. Lab. Anal. 2017, 31, e22028. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.P.; Bajaj, T.; Gupta, D.; Singh, S.B.; Chakrawarty, A.; Goyal, V.; Dey, A.B.; Dey, S. Serum mortalin correlated with α synuclein as serum markers, in Parkinson’s Disease: A Pilot Study. Neuromol. Med. 2018, 20, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Sankiewicz, A.; Romanowicz, L.; Pyc, M.; Hermanowicz, A.; Gorodkiewicz, E. SPR imaging biosensor for the quantitation of fibronectin concentration in blood samples. J. Pharm. Biomed. Anal. 2018, 150, 1–8. [Google Scholar] [CrossRef]
- Sankiewicz, A.; Guszcz, T.; Mena-Hortelano, R.; Zukowski, K.; Gorodkiewicz, E. Podoplanin serum and urine concentration in transitional bladder cancer. Cancer Biomark. 2016, 16, 343–350. [Google Scholar] [CrossRef]
- Matuszczak, E.; Tylicka, M.; Hermanowicz, A.; Debek, W.; Sankiewicz, A.; Gorodkiewicz, E. Application of SPR imaging biosensor for the measurement of 20S proteasomes in blood plasma of children with thermal injury. Annal. Clin. Lab. Sci. 2016, 46, 407–411. [Google Scholar]
- Tokarzewicz, A.; Guszcz, T.; Onopiuk, A.; Kozlowski, R.; Gorodkiewicz, E. Utility of cystatin C as a potential bladder tumour biomarker confirmed by Surface Plasmon Resonance technique. Indian J. A Med. Res. 2018, 218, 46–50. [Google Scholar] [CrossRef]
- Matuszczak, E.; Sankiewicz, A.; Debek, W.; Gorodkiewicz, E.; Hermanowicz, A. Immunoproteasome in the blood plasma of children with acute appendicitis, and its correlation with proteasome and UCHL1 measured by SPR imaging biosensors. Clin. Exp. Immun. 2018, 191, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Weremijewicz, A.; Matuszczak, E.; Sankiewicz, A.; Tylicka, M.; Komarowska, M.; Tokarzewicz, A.; Debek, W.; Gorodkiewicz, E.; Hermanowicz, A. Matrix metalloproteinase-2 and its correlation with basal membrane components laminin-5 and collagen type IV in paediatric burn patients measured with Surface Plasmon Resonance Imaging (SPRI) biosensors. Burns 2018, 44, 931–940. [Google Scholar] [CrossRef]
- Toliczenko-Bernatowicz, D.; Matuszczak, E.; Tylicka, M.; Szymańska, B.; Komarowska, M.; Gorodkiewicz, E.; Debek, W.; Hermanowicz, A. Overexpression of ubiquitin carboxyl-terminal hydrolase 1 (UCHL1) in boys with cryptorchidism. PLoS ONE 2018, 13, e0191806. [Google Scholar] [CrossRef] [PubMed]
- Matuszczak, E.; Tylicka, M.; Dębek, W.; Sankiewicz, A.; Gorodkiewicz, E.; Hermanowicz, A. Concentration of Proteasome in the Blood Plasma of Children with Acute Appendicitis, Before and After Surgery, and Its Correlation with CRP. World J. Surg. 2018, 42, 2259–2264. [Google Scholar] [CrossRef]
- Matuszczak, E.; Tylicka, M.; Dębek, W.; Sankiewicz, A.; Gorodkiewicz, E.; Hermanowicz, A. Overexpression of ubiquitin carboxyl-terminal hydrolase L1 (UCHL1) in serum of children after thermal injury. Adv. Med. Sci. 2017, 62, 83–86. [Google Scholar] [CrossRef] [PubMed]
- Matuszczak, E.; Tylicka, M.; Dębek, W.; Tokarzewicz, A.; Gorodkiewicz, E.; Hermanowicz, A. Concentration of UHCL1 in the serum of children with acute appendicitis, before and after surgery, and its correlation with CRP and prealbumin. J. Investig. Surg. 2018, 31, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Toliczenko-Bernatowicz, D.; Matuszczak, E.; Tylicka, M.; Sankiewicz, A.; Komarowska, M.; Gorodkiewicz, E.; Debek, W.; Hermanowicz, A. 20S proteasome in the blood plasma of boys with cryptorchidism. J. Endocrinol. Investig. 2018, 41, 1103–1106. [Google Scholar] [CrossRef]
- Springer, T.; Chadtová Song, X.; Ermini, M.L.; Lamačová, J.; Homola, J. Functional gold nanoparticles for optical affinity biosensing. Anal. Bioanal. Chem. 2017, 409, 4087–4097. [Google Scholar] [CrossRef]
- Zhang, N.M.Y.; Li, K.; Shum, P.P.; Yu, X.; Zeng, S.; Wu, Z.; Wang, Q.J.; Yong, K.T.; Wei, L. Hybrid graphen/gold plasmonic fiber-optic biosensor. Adv. Mater. Technol. 2017, 2, 1600185. [Google Scholar] [CrossRef]
- Blanchard-Dionne, A.-P.; Meunier, M. Multiperiodic nanohole array for high precision sensing. Photonics 2018, 5, 15. [Google Scholar] [CrossRef]
- He, L.; Pagneux, Q.; Larroulet, I.; Serrano, A.Y.; Pesquera, A.; Zurutuza, A.; Mandler, D.; Boukherroub, R.; Szunerits, S. Label-free femtomolar cancer biomarker detection in human serum using graphene-coated Surface Plasmon Resonance chips. Biosens. Bioelectr. 2017, 89, 606–611. [Google Scholar] [CrossRef] [PubMed]
- Rizal, T. Magneto-optic Surface Plasmon Resonance Ti/Au/Co/Au/Pc configuration and sensitivity. Magnetochem. 2018, 4, 35. [Google Scholar] [CrossRef]
- Eletxigerra, U.; Martinez-Perdiguero, J.; Barderas, R.; Pingarron, J.M.; Campuzano, S.; Merino, S. Surface Plasmon Resonance immunosensor for ErbB2 breast cancer biomarker determination in human serum and raw cancer cell lysates. Anal. Chim. Acta 2016, 905, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Loo, J.F.-C.; Yang, C.; Tsang, H.-L.; Lau, P.-M.; Yong, K.-T.; Ho, H.P.; Kong, S.K. An Aptamer Bio-barCode (ABC) assay using SPR, RNase H, and probes with RNA and gold-nanorods for anti-cancer drug screening. Analyst 2017, 142, 3579–3587. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Wang, X.; Wang, J.; Fu, W.; Yao, C. A SPR biosensor based on signal amplification using antibody-QD conjugates for quantitative determination of multiple tumor markers. Sci. Rep. 2016, 6, 33140. [Google Scholar] [CrossRef] [PubMed]
- Wu, Q.; Sun, Y.; Zhang, D.; Li, S.; Zhang, Y.; Ma, P.; Yu, Y.; Wang, X.; Song, D. Ultrasensitive magnetic field-assisted Surface Plasmon Resonance immunoassay for human cardiac troponin I. Biosens. Bioelectr. 2017, 96, 288–293. [Google Scholar] [CrossRef] [PubMed]
- Lamberti, I.; Scarano, S.; Esposito, C.L.; Antoccia, A.; Antonini, G.; Tanzarella, C.; De Franciscis, V.; Minunni, M. In vitro selection of RNA aptamers against CA125 tumor marker in ovarian cancer and its study by optical biosensing. Methods 2016, 97, 58–68. [Google Scholar] [CrossRef]
- David, D.; Surendran, A.; Thulaseedharan, J.V.; Nair, A.S. Regulation of CNKSR2 protein stability by the HECT E3 ubiquitin ligase Smurf2, and its role in breast cancer progression. BMC Cancer 2018, 18, 284. [Google Scholar] [CrossRef]
- Zhang, T.; Zheng, Y.; Zhao, D.; Yan, J.; Sun, C.; Zhou, Y.; Tai, G. Multiple approaches to assess pectin binding to galectin-3. Int. J. Biol. Macromol. 2016, 91, 994–1001. [Google Scholar] [CrossRef]
- Fernández, M.M.; Ferragut, F.; Cárdenas Delgado, V.M.; Bracalente, C.; Bravo, A.I.; Cagnoni, A.J.; Nuñez, M.; Morosi, L.G.; Quinta, H.R.; Espelt, M.V.; et al. Glycosylation-dependent binding of galectin-8 to activated leukocyte cel adhesion molecule (ALCAM/CD166) promotes its surface segregation on breast cancer cells. Biochim. Biophys. Acta 2016, 1860, 2255–2268. [Google Scholar] [CrossRef]
- Han, Y.; Gao, Y.; He, T.; Wang, D.; Guo, N.; Zhang, X.; Chen, S.; Wang, H. PD-1/PD-L1 inhibitor screening of caffeoylquinic acid compounds using Surface Plasmon Resonance spectroscopy. Anal. Biochem. 2018, 547, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Damborsky, P.; Zamorova, M.; Katrlık, J. Determining the binding affinities of prostate-specific antigen to lectins: SPR and microarray approaches. Proteomics 2016, 16, 3096–3104. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Gu, K.; Zhang, C.-H.; Chen, X.-T.; Jiang, Y.; Melcher, K.; Zhang, J.; Wang, M.; Xu, H.E. Generation and characterization of a human nanobody against VEGFR-2. Acta Pharmacol. Sin. 2016, 37, 857–864. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Stage | Marker | SPR Type | Fluidic/Non Fluidic | Chip | Linker/Receptor | Receptor Immobilization | Reference |
|---|---|---|---|---|---|---|---|
| i | HER2 | SPR | Micro-fluidic | Nano-whole array | Cysteamina/Sandwich/2Antibodies | Biotin/streptavidin | [3] |
| i | CEA | SPR | Fluidic | Slide/Cr/Au | MUA/antibody | EDC/NHS | [4] |
| i | Cytokeratin 17 | SPR | Non fluidic | Optical fiber/Au | S2PEG6COOH/antibody | EDC/NHS | [5] |
| i | Cytochrom C | SPRi | Fluidic | Easy2Spot | Antibody | Sensor pre-activated G-type Senseye | [6] |
| i | BSA | SPR | Fluidic or Non fluidic | Prism/Au | Cysteamine/GOCOOOH/antibody | EDC/NHS | [7] |
| i | BSA | SPR | Non fluidic | Slide/Au | Mercapto-propane sulfonate/modified GO | EDC/NHS | [8] |
| i | BSA Biotin | SPR | Micro-fluidic | Nanogroove metasurface | None streptavidin | Physisorption/Streptavidin/biotin | [9] |
| ii | Cytokeratin-19 | SPR | Fluidic or Non fluidic | Prism | Cysteamine/GOCOOOH/antibody | EDC/NHS | [10] |
| ii | Transferrin | SPR | Fluidic | Slide/Au | 4-Mercapto phenylboronic | 4-Mercapto phenylboronic | [11] |
| ii | Folic acid | SPR | Fluidic | Prism/Ti/Au/graphen | FAP | Hydrophobic interaction | [12] |
| ii | DNA E. coli | LSPR | Micro-fluidic | Slide/Ag nano prism | 5′[C6-thiol] DNA probe | DNA probe-DNA target interaction | [13] |
| Stage | Marker | SPR Type | Fluidic/Non Fluidic | Chip | Linker/Receptor | Receptor Immobilization | Reference |
|---|---|---|---|---|---|---|---|
| Iii | PSA | SPRi | Fluidic | Slide/Au | Allyl mercaptan | PSA imprinted polymer | [14] |
| Iii | CBP | SPR | Fluidic | CM5 chip | Dextran-COOH/Antibody | EDC/NHS | [15] |
| Iii | Troponin T | SPR | Fluidic | Slide/Au | Polydopamine/Epitop/ | Polymer Imprinted epitop | [16] |
| Iv | Rac1, Rac1b | SPR | Fluidic | CM5 chip | Dextran-COOH/Antibody | EDC/NHS | [17] |
| Iv | 5LOX | SPR | Fluidic | CM5 chip | Dextran-COOH/Antibody | EDC/NHS | [18] |
| Iv | CDK4 | SPR | Fluidic | CM5 chip | Dextran-COOH/Antibody | EDC/NHS | [19] |
| Iv | Laminin-5 | SPRi | Non fluidic | Slide/Au/array | Cysteamine/Antibody | EDC/NHS | [20] |
| Iv | Collagen IV | SPRi | Non fluidic | Slide/Au/array | Cysteamine/Antibody | EDC/NHS | [21] |
| Iv | MMP1 | SPRi | Non fluidic | Slide/Au/array | Cysteamine/Antibody | EDC/NHS | [22] |
| Iv | 20S immune-proteasome | SPRi | Non fluidic | Slide/Au/array | 1-octadecano-thiol/Inhibitor ONX 0914 | Hydrophobic interaction | [23] |
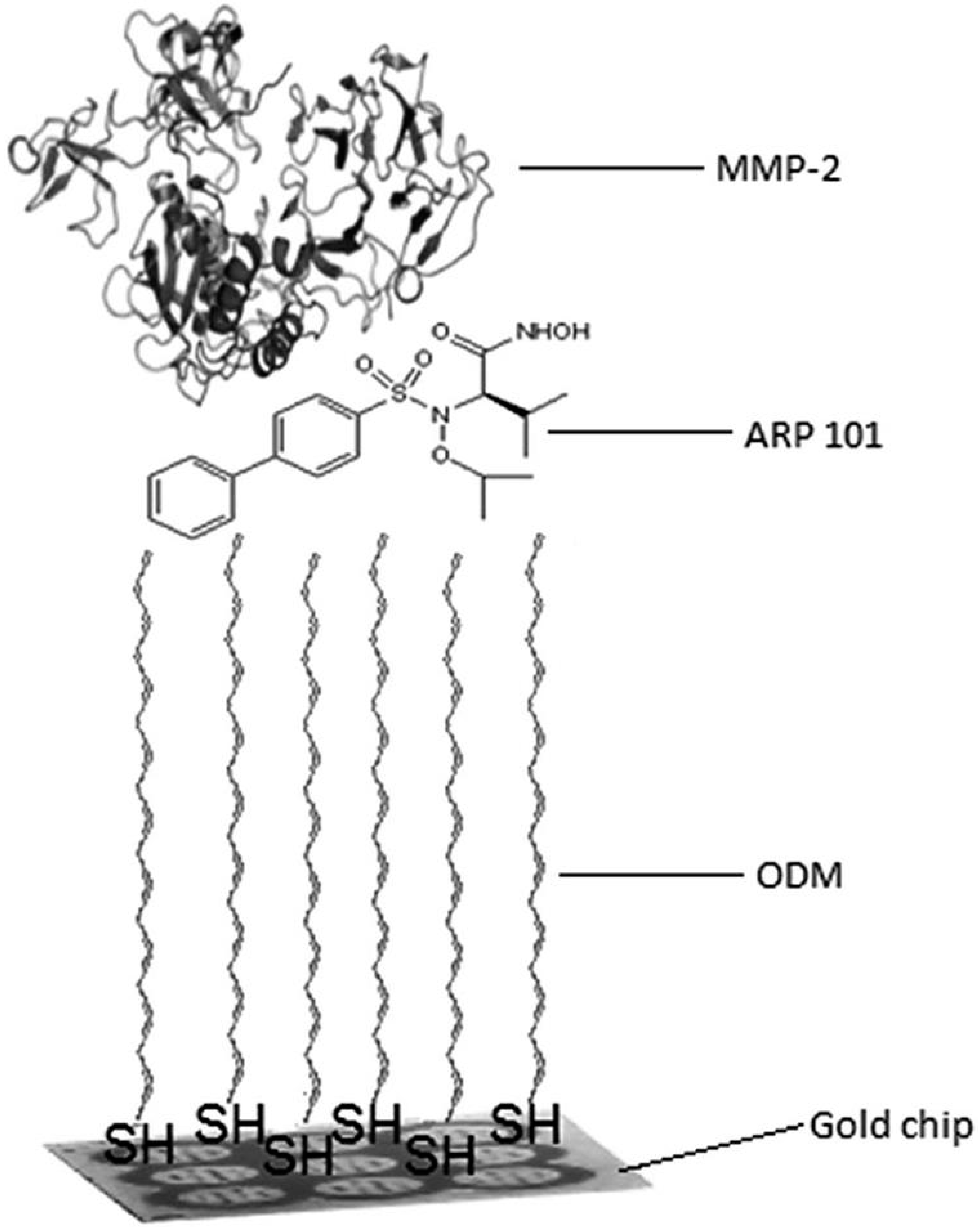
| Iv | MMP2 | SPRi | Non fluidic | Slide/Au/array | 1-octadecano-thiol/Inhibitor ARP 101 | Hydrophobic interaction | [24] |
| Iv | YKL40 | SPR | Fluidic | CM5 chip | Dextran-COOH/Antibody | EDC/NHS | [25] |
| Iv | Mortalin and αSynuclein | SPR | Fluidic | CM5 chip | Dextran-COOH/Antibody | EDC/NHS | [26] |
| Iv | Fibronectin | SPRi | Non fluidic | Slide/Au/array | Cysteamine/Antibody | EDC/NHS | [27] |
| Stage | Marker | SPR Type | Fluidic/Non Fluidic | Chip | Linker/Receptor | Receptor Immobilization | Reference |
|---|---|---|---|---|---|---|---|
| V | podoplanin | SPRi | Non fluidic | Slide/Au/array | Cysteamine/Antibody | EDC/NHS | [28] |
| V | 20S proteasome | SPRi | Non fluidic | Slide/Au/array | Cysteamine/Inhibitor PSI | EDC/NHS | [29] |
| V | Cystatin C | SPRi | Non fluidic | Slide/Au/array | Cysteamine/Antibody | EDC/NHS | [30] |
| V | UCHL1 | SPRi | Non fluidic | Slide/Au/array | Cysteamine/Antibody | EDC/NHS | [31] |
| V | MMP2 Laminin5 Collagen IV | SPRi | Non fluidic | Slide/Au/array | 1-octadecano-thiol/Inhibitor ONX 0914 Cysteamine/antibody | Hydrophobic Interaction EDC/NHS | [32] |
| V | UCHL1 | SPRi | Non fluidic | Slide/Au/array | Cysteamine/Antibody | EDC/NHS | [33] |
| V | 20S proteasome | SPRi | Non fluidic | Slide/Au/array | Cysteamine/Inhibitor PSI | EDC/NHS | [34] |
| V | UCHL1 | SPRi | Non fluidic | Slide/Au/array | Cysteamine/Antibody | EDC/NHS | [35,36] |
| V | 20S proteasome | SPRi | Non fluidic | Slide/Au/array | Cysteamine/Inhibitor PSI | EDC/NHS | [37] |
| Stage | Marker | SPR Type | Fluidic/Non Fluidic | Chip/NP | Sandwich/Other | Receptors Immobilization (Chip/Antibody) | Reference |
|---|---|---|---|---|---|---|---|
| ii | Folic acid | SPRi | Non fluidic | Array/Cr/Au/FA-AuNP | Sandwich | HS-(CH2)11-EG3-NTA/polyhistidine | [12] |
| ii | Troponin I | SPR | Fluidic | Slide/Au/HGNP/MMWCNTs-PDA | Sandwich/MMWCNTs-PDA | Polydopamine/Polydopamine | [45] |
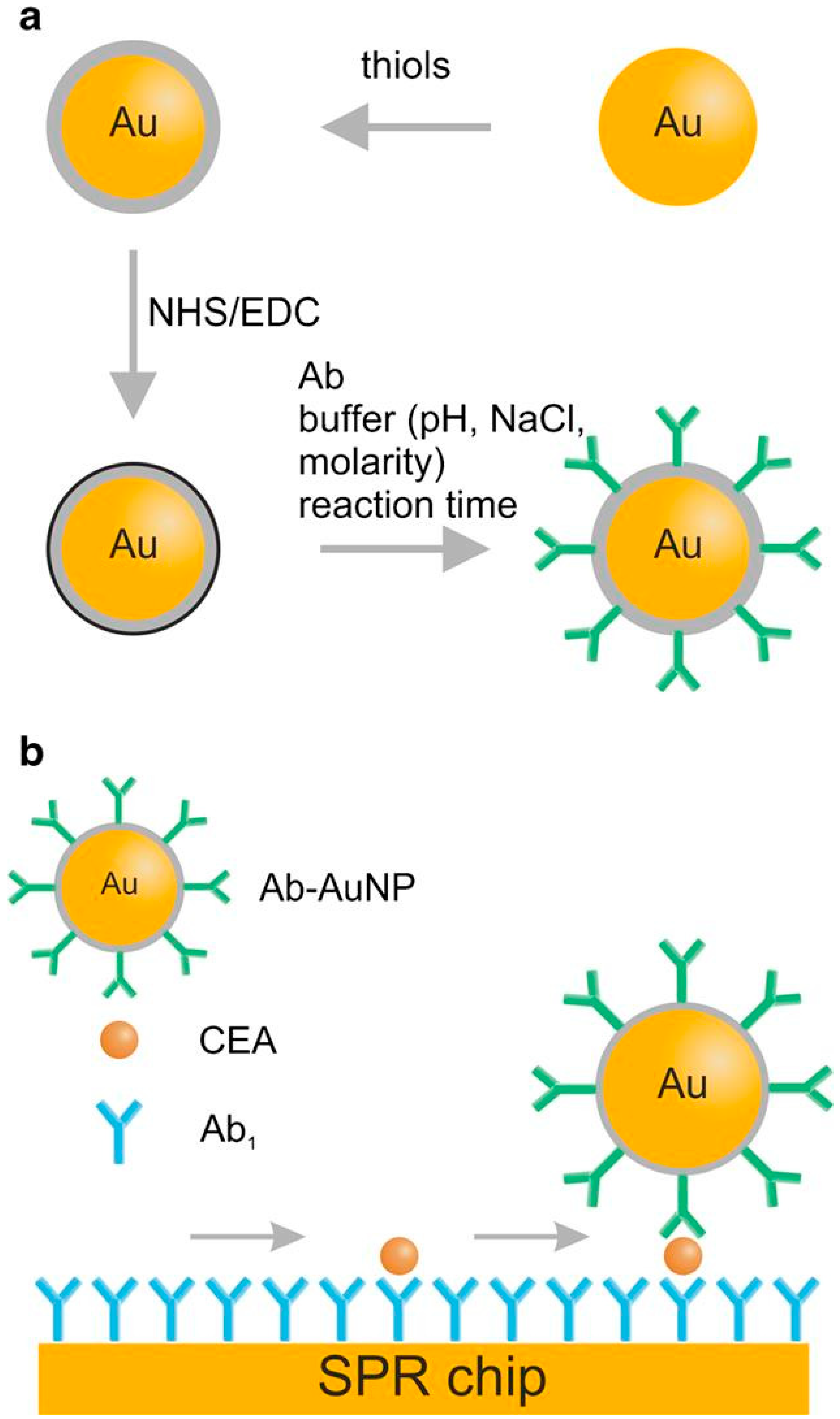
| iii | CEA | SPR | Fluidic | Slide/Ti/Au/AuNP | Sandwich | HS-OEG-COOH/HS-OEG-COOH/EDC/NHS | [38] |
| iii | HER 2 | SPR | Micro-fluidic | Prism/Au/SAv-GNPs | Sandwich | MUA/EDC/NHS/biotinylated antibody | [43] |
| iv | Cytochrom C | SPR | Fluidic | Slide/Au/AuNR | Sandwich/MMP | Straptavidin/biotinylated aptamer/antibody/MMP | [44] |
| iv | AFP, CEA CYFRA 21-1 | SPR | Micro-fluidic | Prism/Au | Sandwich/QD | Hexanedithiol/antibody/DTBE | [46] |
| Marker | Abbrev. | Cancer/or Other Disease | Body Fluid | Reference |
|---|---|---|---|---|
| Arachidonate 5-lipoxygenase | 5LOX/ALOX5 | Breast cancer | Blood plasma | [18] |
| Carcinoembryonic antigen | CEA | Colorectal cancer | Blood serum | [4] |
| Calcium Binding Protein | CBP | Acute myocardial infarction | Blood serum | [15] |
| Chitinase-3-like protein 1 | CHI3L1/YKL-40 | Asthma | Blood serum | [25] |
| Collagen IV | Breast cancer/burns | Blood serum | [21] | |
| Cyclin-dependent kinase 4 | CDK4 | Lung, head and neck cancers | Blood serum | [19] |
| Cystatin C | Bladder cancer | Blood serum, urine | [30] | |
| Cytochrom C | Apoptosis | No information | [6] | |
| Cytokeratin 17 | CK 17 | Lung cancer | No information | [5] |
| Cytokeratin 19 | CK19 | Lung cancer | Blood plasma | [10] |
| Epidermal receptor protein-2 antigen | HER | Breast cancer | No information | [3] |
| Fibronectin | Burns | Blood plasma | [27] | |
| Folic acid | FA | Megaloblastic anemia | blood | [12] |
| 20S-immunoproteasom | 20Si | Acute leukemia | Blood plasma | [23] |
| Laminin 5 | Bladder cancer/burns | Blood plasma | [20,32] | |
| Matrix metalloproteinase-1 | MMP1 | Bladder cancer/acute appendicitis | Blood serum | [22] |
| Matrix metalloproteinase-2 | MMP2 | Burns | Blood plasma | [24,32] |
| Mortalin/mitochondrial 70 kDa heat shock protein | mtHsp70 | Parkinson’s Disease | Blood serum | [26] |
| Podoplanin | Bladder cancer | Blood serum, urine | [28] | |
| 20S-proteasom | 20Sc | Burns, acute appendicitis, Cryptorchidism | Blood plasma | [34] |
| Prostate specific antigen | PSA | Prostate cancer | Blood serum | [14] |
| Ras-related C3 botulinum toxin substrate 1 | Rac1 | Non-Small Cell Lung Cancer | Blood serum | [17] |
| Ras-related C3 botulinum toxin substrate 1b | Rac1b | Non-Small Cell Lung Cancer | Blood serum | [17] |
| Transferrin | Trf | Hypertension, primary renal disease, diabetes. | Artificial urine | [11] |
| Troponin T | TnT | Acute myocardial infarction | Blood serum | [16] |
| Ubiquitin carboxyl-terminal hydrolase L1 | UCHL1 | Burns, cryptorchidism, Acute Appendicitis | Blood serum | [31,35,36] |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gorodkiewicz, E.; Lukaszewski, Z. Recent Progress in Surface Plasmon Resonance Biosensors (2016 to Mid-2018). Biosensors 2018, 8, 132. https://doi.org/10.3390/bios8040132
Gorodkiewicz E, Lukaszewski Z. Recent Progress in Surface Plasmon Resonance Biosensors (2016 to Mid-2018). Biosensors. 2018; 8(4):132. https://doi.org/10.3390/bios8040132
Chicago/Turabian StyleGorodkiewicz, Ewa, and Zenon Lukaszewski. 2018. "Recent Progress in Surface Plasmon Resonance Biosensors (2016 to Mid-2018)" Biosensors 8, no. 4: 132. https://doi.org/10.3390/bios8040132
APA StyleGorodkiewicz, E., & Lukaszewski, Z. (2018). Recent Progress in Surface Plasmon Resonance Biosensors (2016 to Mid-2018). Biosensors, 8(4), 132. https://doi.org/10.3390/bios8040132