A Novel Working Memory Task-Induced EEG Response (WM-TIER) Feature Extraction Framework for Detecting Alzheimer’s Disease and Mild Cognitive Impairment

 , , ,
, , ,  and
and
Abstract
1. Introduction
- (1)
- To the best of our knowledge, the proposed WM-TIER feature extraction architecture is novel and has not been proposed before. It offers two main advantages: (1) it reduces the influence of the inter-individual variability, and (2) it leverages the often-overlooked information embedded in the inter-state changes of EEG dynamics.
- (2)
- Given that the FB-PLI WM-TIER features encapsulate information on EEG connectivity across different frequency bands and the dynamics of EEG changes from rest to task and are further optimized using a machine learning-based feature selection strategy, we hypothesize that these features will achieve more effective classification between AD/MCI and HC compared to either rsEEG or task EEG PLI features. This hypothesis will be substantiated by our results in Section 3.1.
- (3)
- Additionally, we investigated the differences in FB-PLI connectivity features extracted under the WM-TIER framework (i.e., the FB-PLI WM-TIER features) between the three groups: HC, MCI, and AD (Section 3.2 and Section 3.3). This approach allows an in-depth examination of PLI variations within the same group across different states and highlights the differences in state transitions among the different groups. The results of this analysis provide interpretable neural markers that could be used as references for auxiliary assessments in future applications. Furthermore, these markers hold the potential to be used as objective indicators for evaluating treatment outcomes should real clinical applications arise in the future.
2. Materials and Methods
2.1. Participants
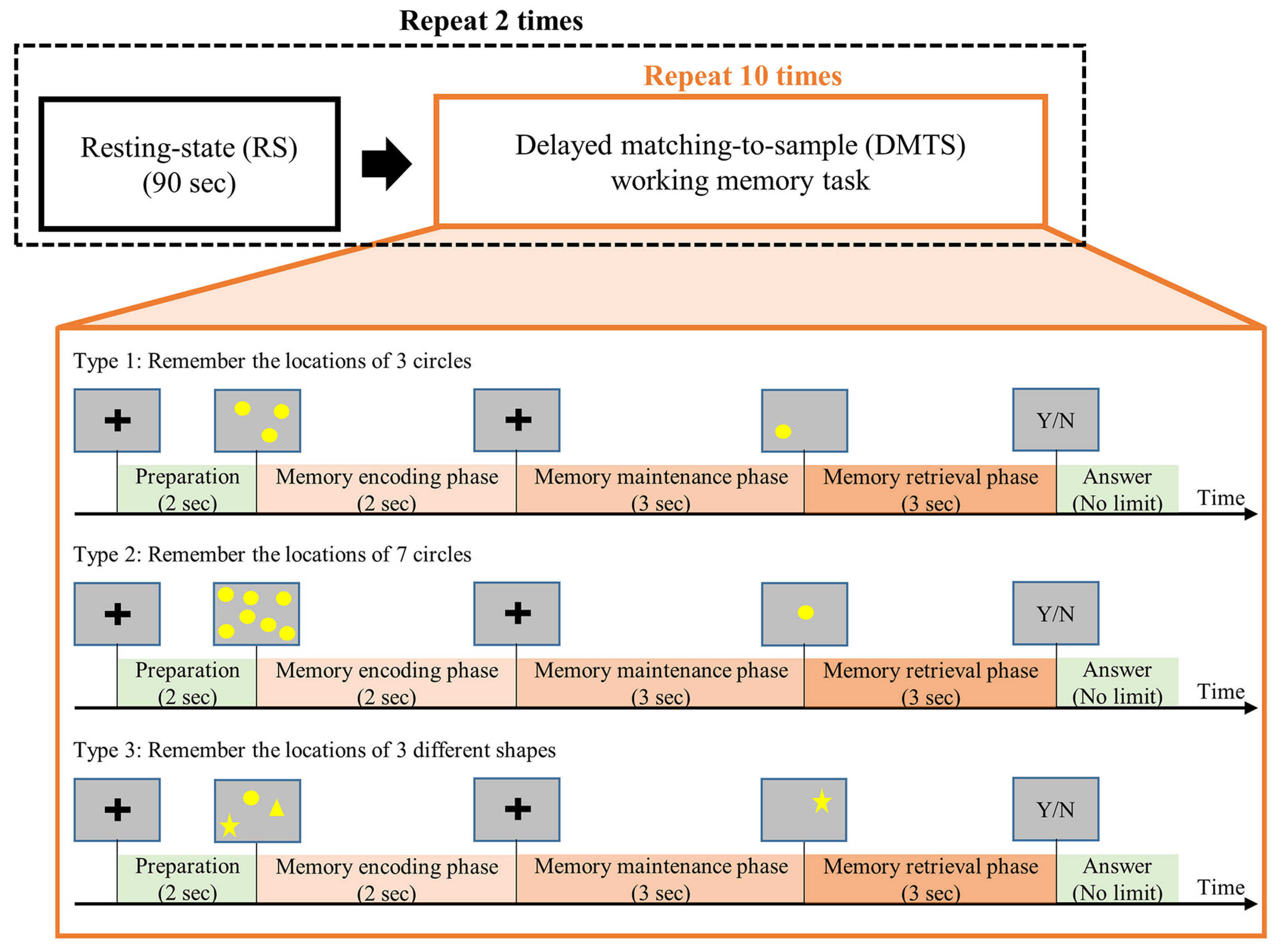
2.2. Task Procedures
2.3. EEG Data Acquisition and Preprocessing
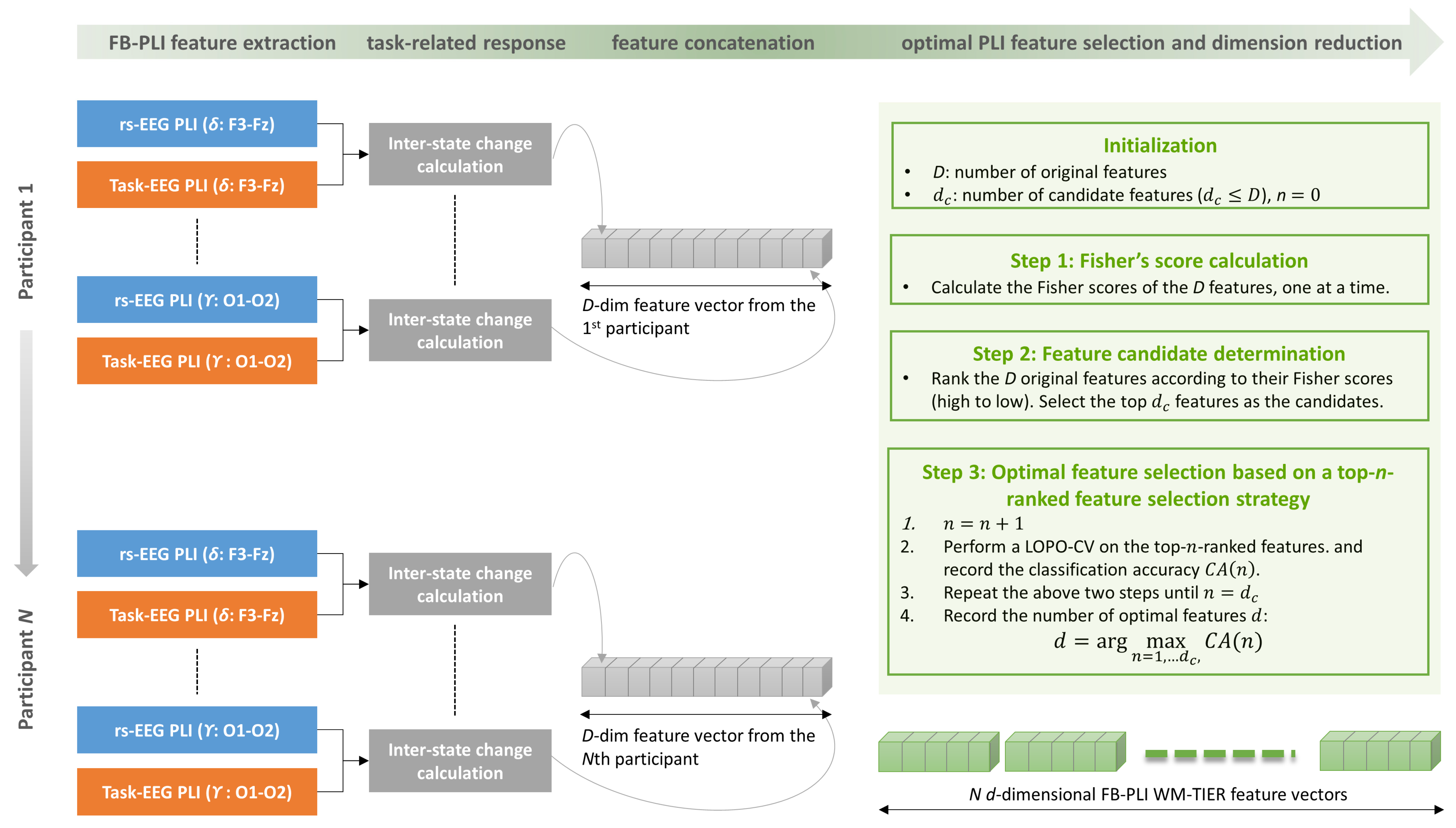
2.4. FB-PLI WM-TIER Feature Extraction
2.4.1. Stage 1: FB-PLI Feature Extraction
Relative Power (RP)
Coherence (Coh)
2.4.2. Stage 2: Task-Related Response Calculation and Feature Concatenation
2.4.3. Stage 3: Optimal PLI Feature Selection and Dimension Reduction
2.5. Classifiers and Classification Tasks
2.5.1. Classifiers
2.5.2. Classification
- (1)
- Task EEG features (i.e., ME-EEG and MM-EEG features) refer to those directly extracted from either the ME or MM phases without calculating the inter-state changes.
- (2)
- Furthermore, task EEG features of RP, Coh, and FB-PLI were separately optimized by employing the top-n-feature ranked feature selection strategy combined with the LOPO-CV (i.e., the stage 3 in Figure 2).
- (3)
- The features “TIER” are the features that went through the three stages shown in Figure 2. For example, ME-TIER of the RP feature is also a d-dimensional feature vector obtained by the WM-TIER feature extraction framework. Moreover, in the case of FB-PLI, both ME-TIER and MM-TIER are FB-PLI WM-TIER features.
3. Results
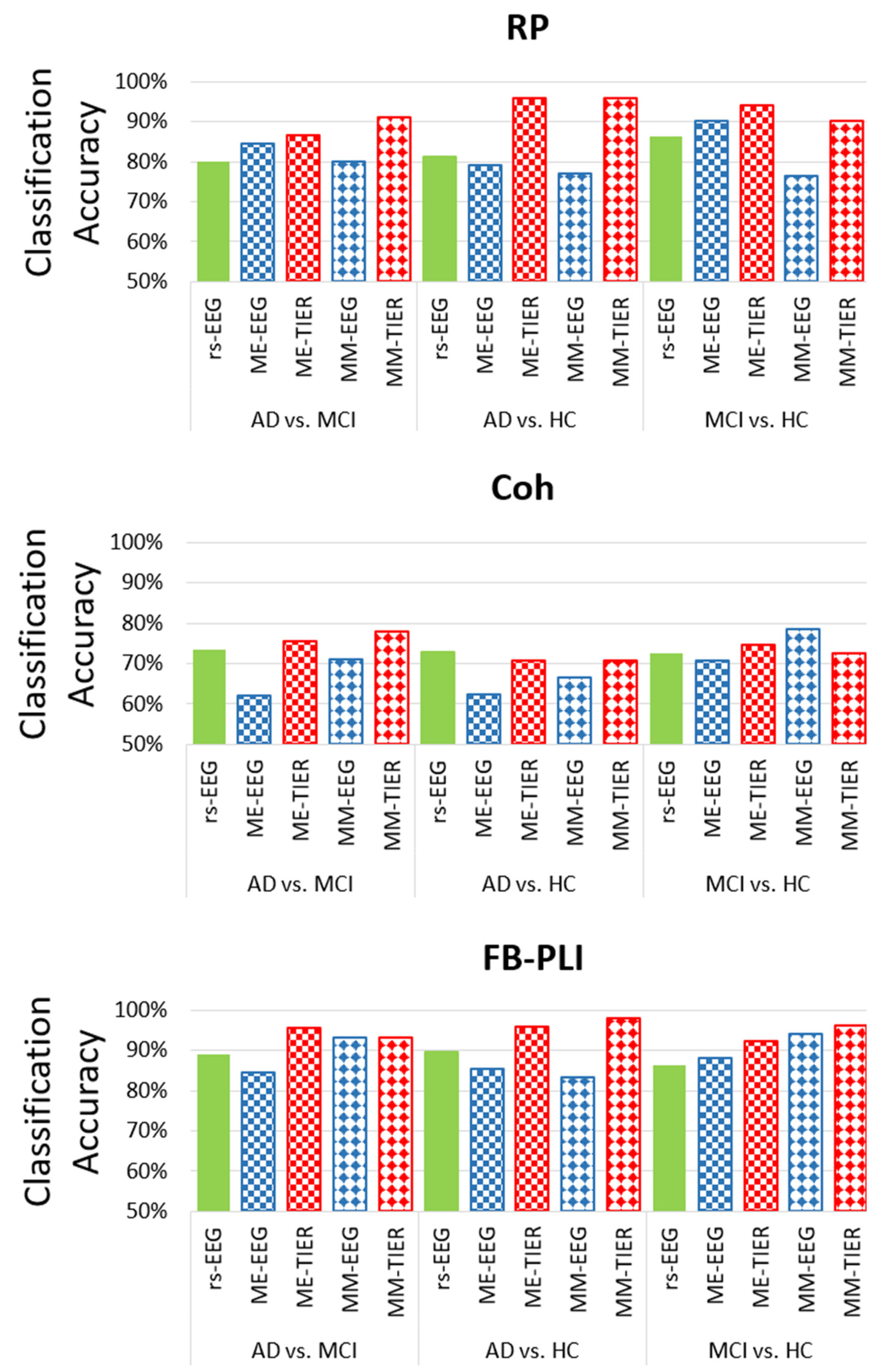
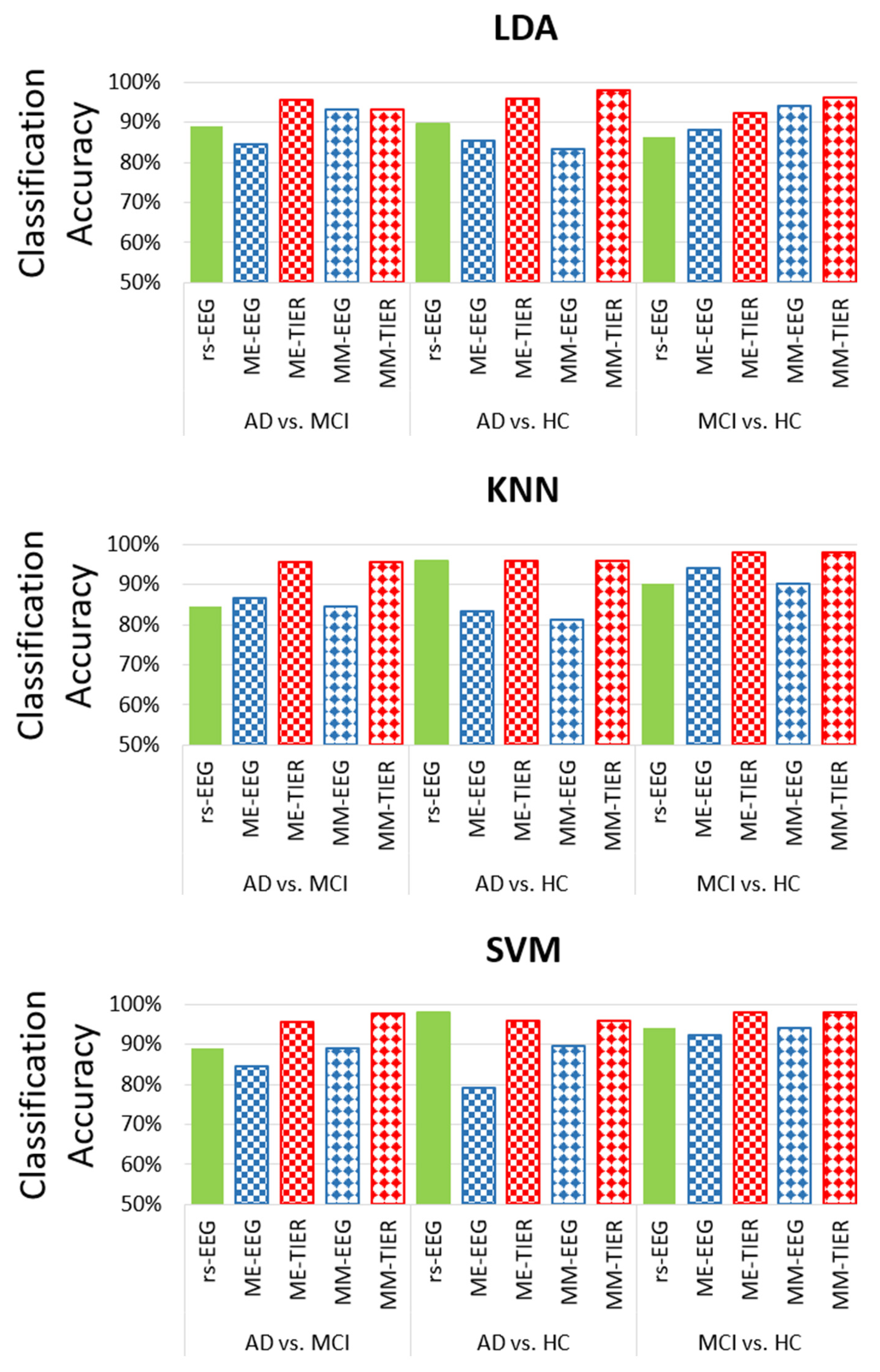
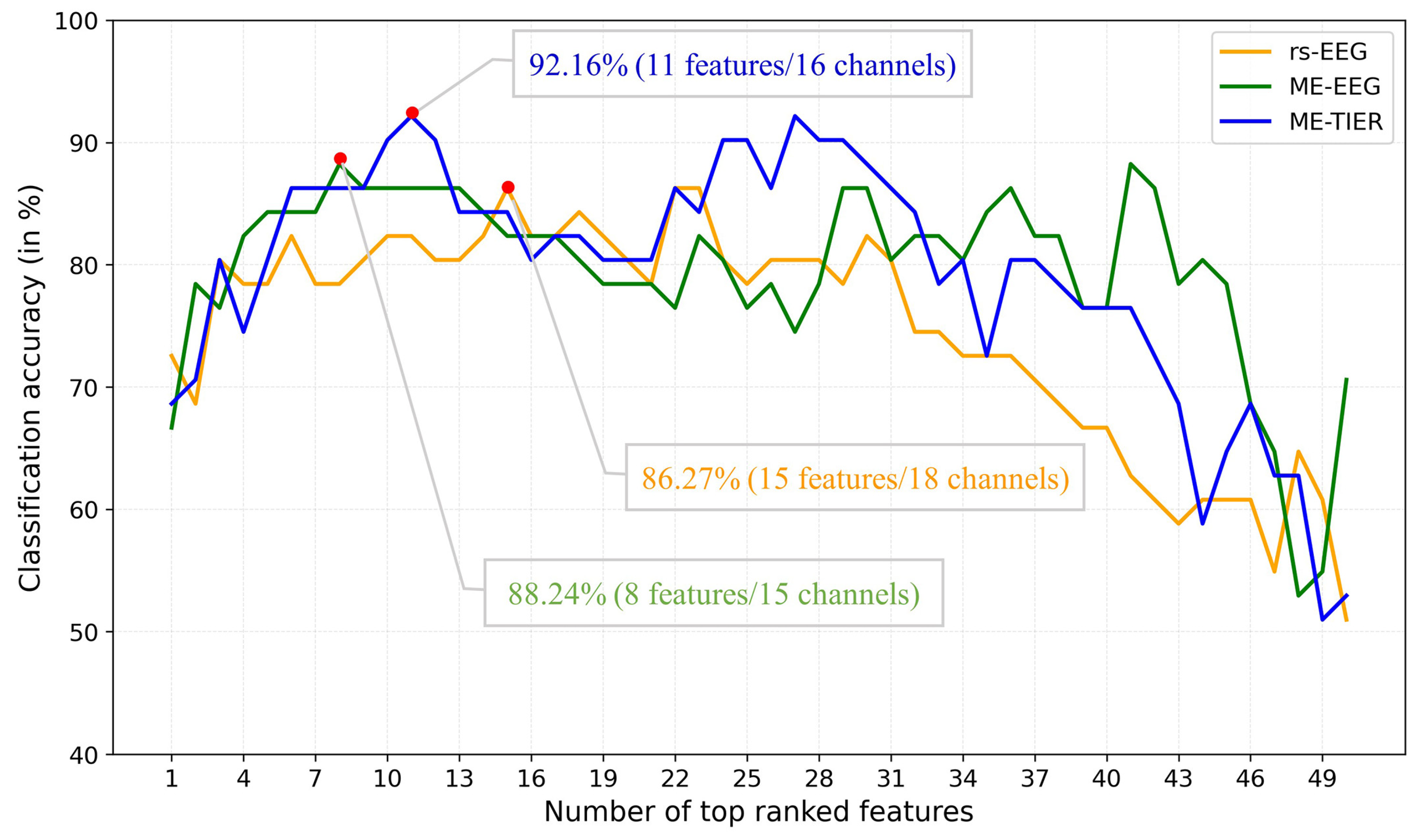
3.1. Comparision of Classification Accuracy Obtained from rsEEG, Task EEG, and WM-TIER Using Different Types of Features
3.2. The Inter-State Change of Theta Band PLI-Based Connectivity Within the AD, MCI, and HC Groups
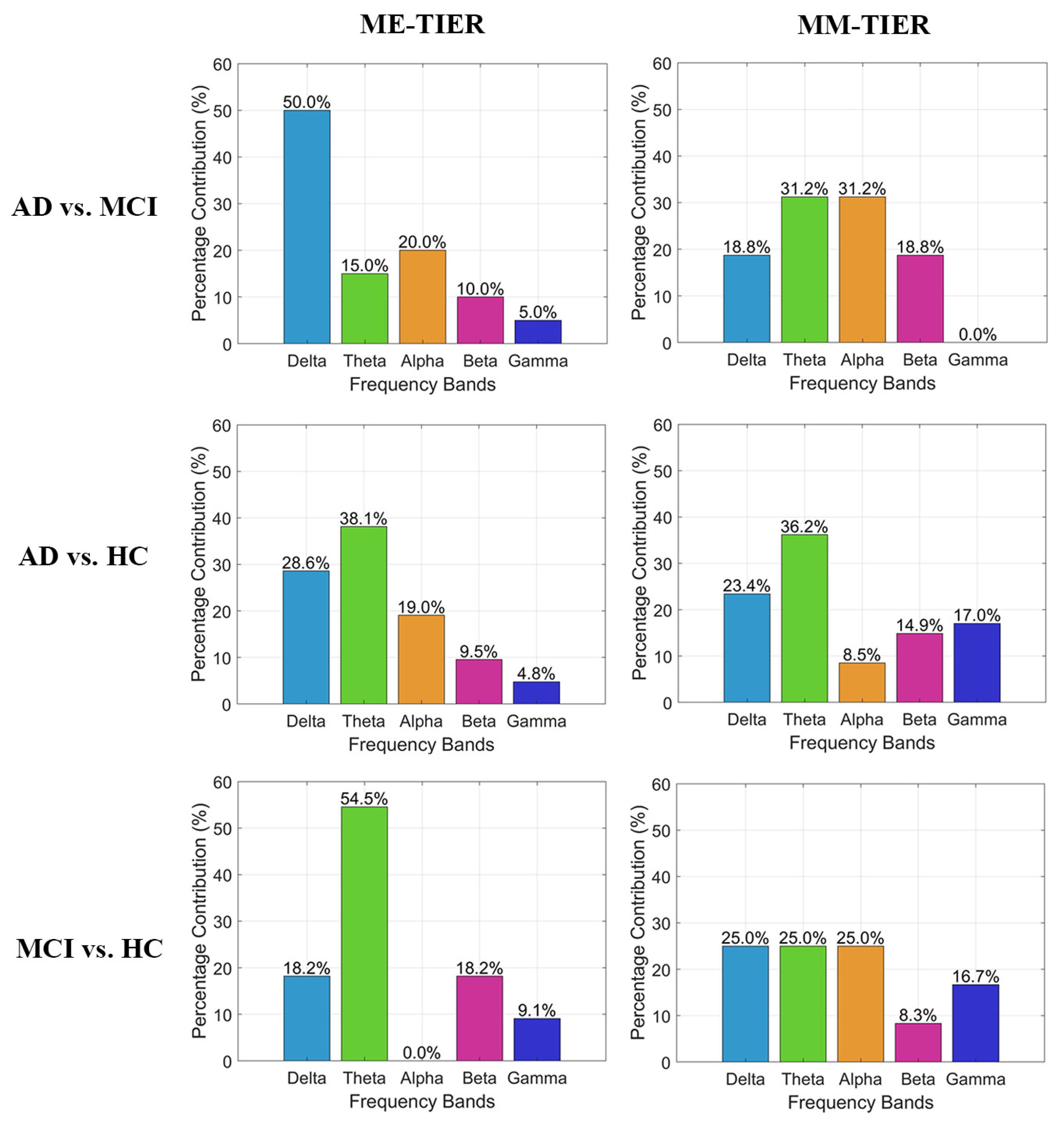
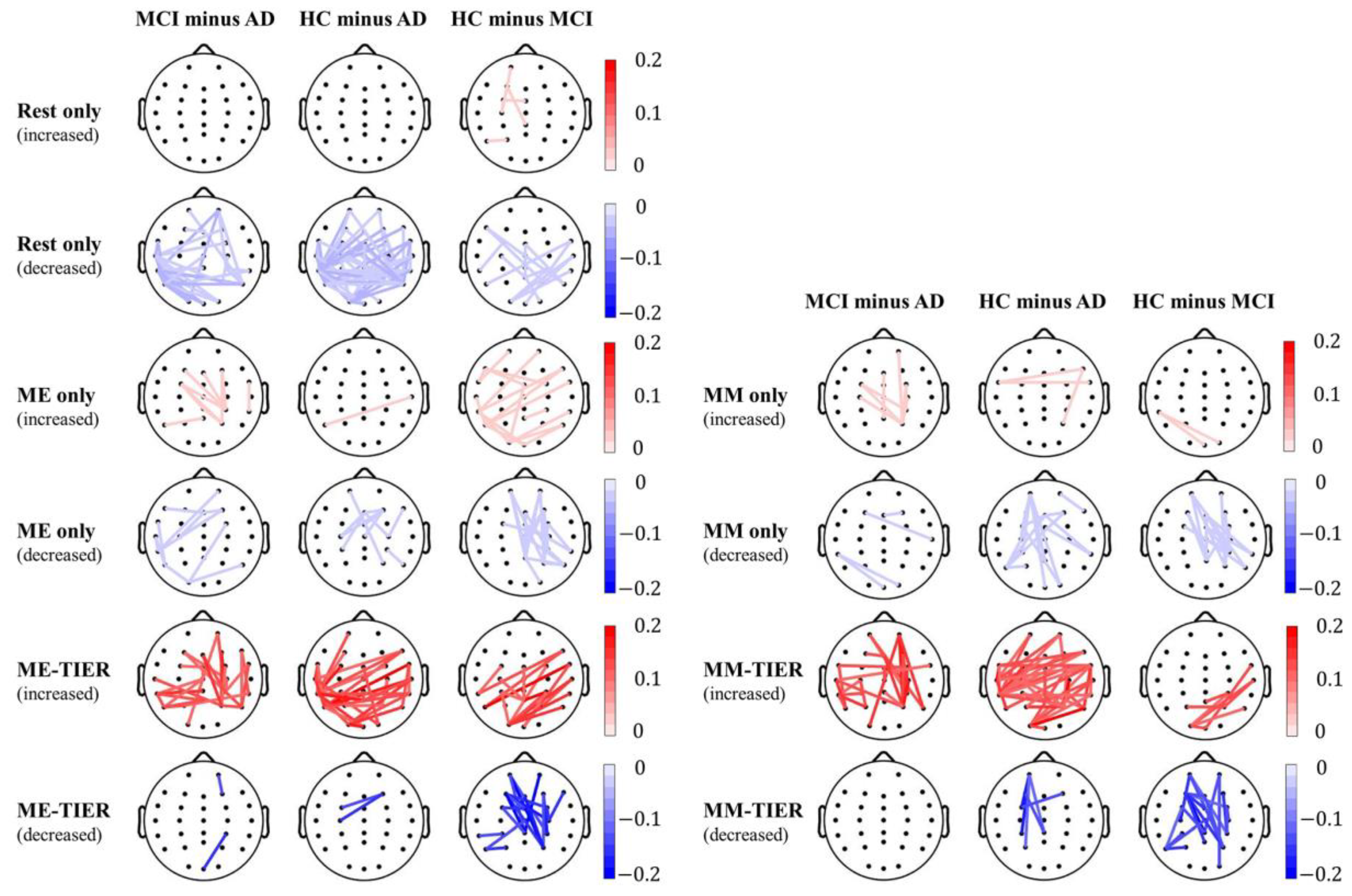
3.3. The Between-Group Difference of Theta Band PLI-Based Connectivity in rsEEG, Task EEG, and WM-TIER
4. Discussion
4.1. The Effectiveness of rsEEG, Task EEG, and WM-TIER in Classification Between Groups
4.2. Increase of Theta Band Functional Connectivity During Resting State Due to Cognitive Decline
4.3. Reduction of EEG Connectivity from Rest to Task Condition Due to Cognitive Decline
4.4. Practical Use of the Proposed Diagnosis Approach
4.5. Limitations and Future Works
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Permutation-Based Multiple Comparison Correction for Between-State Analysis
| Algorithm A1. Permutation-based correction for multiple between-state comparisons |
 |
Appendix B. Permutation-Based Multiple Comparison Correction for Between-Group Analysis
| Algorithm A2. Permutation-based correction for multiple between-group comparisons |
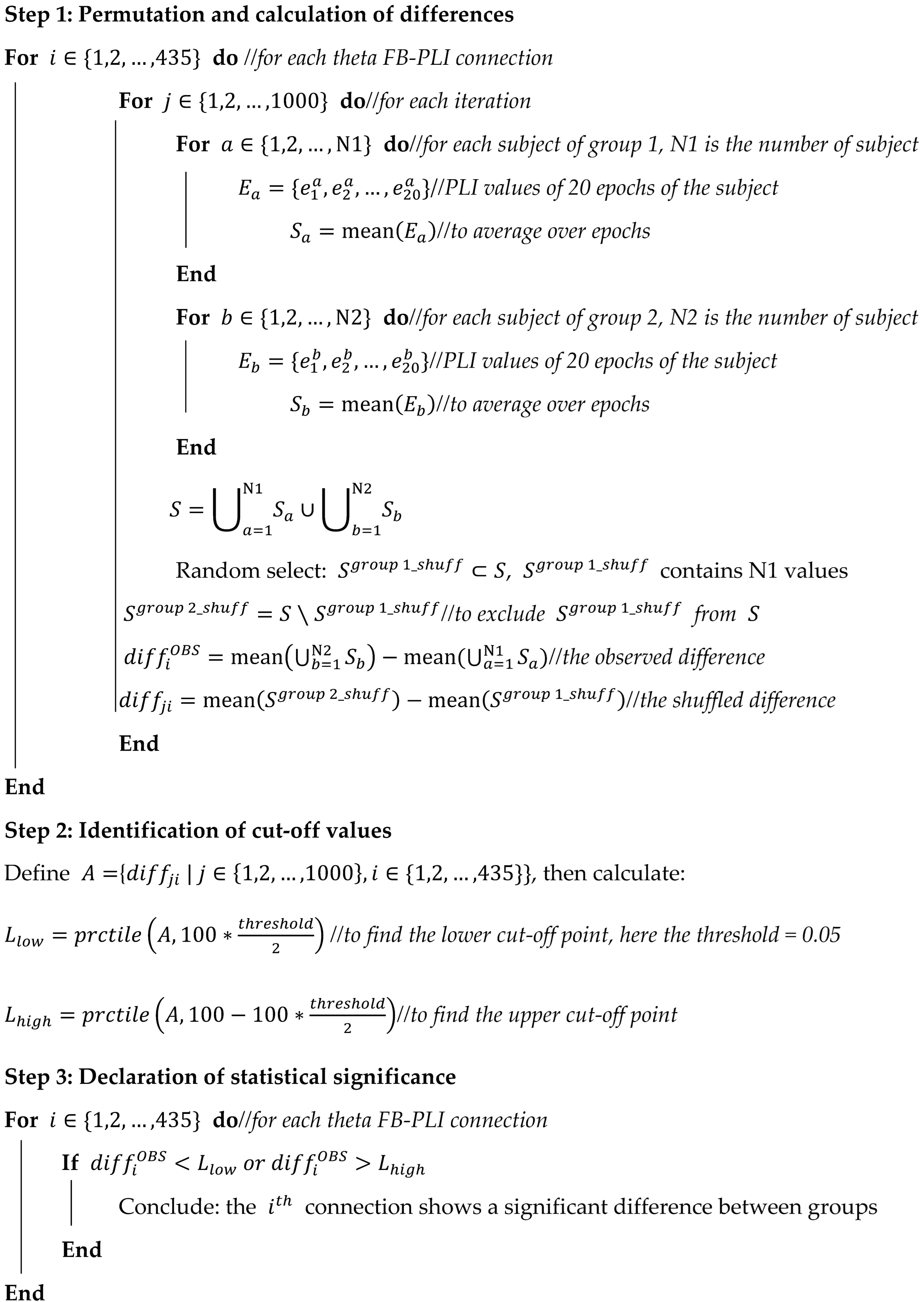 |
References
- Kim, S. Exploring the Field Application of Combined Cognitive-Motor Program with Mild Cognitive Impairment Elderly Patients. J. Exerc. Rehabil. 2018, 14, 817–820. [Google Scholar] [CrossRef]
- Reinhart, R.M.G.; Nguyen, J.A. Working Memory Revived in Older Adults by Synchronizing Rhythmic Brain Circuits. Nat. Neurosci. 2019, 22, 820–827. [Google Scholar] [CrossRef] [PubMed]
- Lazarou, I.; Stavropoulos, T.G.; Meditskos, G.; Andreadis, S.; Kompatsiaris, I.Y.; Tsolaki, M. Long-Term Impact of Intelligent Monitoring Technology on People with Cognitive Impairment: An Observational Study. JAD 2019, 70, 757–792. [Google Scholar] [CrossRef] [PubMed]
- Mancioppi, G.; Fiorini, L.; Timpano Sportiello, M.; Cavallo, F. Novel Technological Solutions for Assessment, Treatment, and Assistance in Mild Cognitive Impairment. Front. Neuroinform. 2019, 13, 58. [Google Scholar] [CrossRef] [PubMed]
- Morris, J.C.; Storandt, M.; Miller, J.P.; McKeel, D.W.; Price, J.L.; Rubin, E.H.; Berg, L. Mild Cognitive Impairment Represents Early-Stage Alzheimer Disease. Arch. Neurol. 2001, 58, 397–405. [Google Scholar] [CrossRef]
- Mistridis, P.; Krumm, S.; Monsch, A.U.; Berres, M.; Taylor, K.I. The 12 Years Preceding Mild Cognitive Impairment Due to Alzheimer’s Disease: The Temporal Emergence of Cognitive Decline. JAD 2015, 48, 1095–1107. [Google Scholar] [CrossRef]
- Petersen, R.C.; Doody, R.; Kurz, A.; Mohs, R.C.; Morris, J.C.; Rabins, P.V.; Ritchie, K.; Rossor, M.; Thal, L.; Winblad, B. Current Concepts in Mild Cognitive Impairment. Arch. Neurol. 2001, 58, 1985. [Google Scholar] [CrossRef]
- Petersen, R.C.; Caracciolo, B.; Brayne, C.; Gauthier, S.; Jelic, V.; Fratiglioni, L. Mild Cognitive Impairment: A Concept in Evolution. J. Intern. Med. 2014, 275, 214–228. [Google Scholar] [CrossRef]
- Langa, K.M.; Levine, D.A. The Diagnosis and Management of Mild Cognitive Impairment: A Clinical Review. JAMA 2014, 312, 2551. [Google Scholar] [CrossRef]
- Vega, J.N.; Newhouse, P.A. Mild Cognitive Impairment: Diagnosis, Longitudinal Course, and Emerging Treatments. Curr. Psychiatry Rep. 2014, 16, 490. [Google Scholar] [CrossRef]
- Jack, C.R., Jr.; Andrews, J.S.; Beach, T.G.; Buracchio, T.; Dunn, B.; Graf, A.; Hansson, O.; Ho, C.; Jagust, W.; McDade, E.; et al. Revised Criteria for Diagnosis and Staging of Alzheimer’s Disease: Alzheimer’s Association Workgroup. Alzheimer’s Dement. 2024, 20, 5143–5169. [Google Scholar] [CrossRef] [PubMed]
- Ding, Y.; Chu, Y.; Liu, M.; Ling, Z.; Wang, S.; Li, X.; Li, Y. Fully Automated Discrimination of Alzheimer’s Disease Using Resting-State Electroencephalography Signals. Quant. Imaging Med. Surg. 2022, 12, 1063–1078. [Google Scholar] [CrossRef] [PubMed]
- Ando, M.; Nobukawa, S.; Kikuchi, M.; Takahashi, T. Identification of Electroencephalogram Signals in Alzheimer’s Disease by Multifractal and Multiscale Entropy Analysis. Front. Neurosci. 2021, 15, 667614. [Google Scholar] [CrossRef] [PubMed]
- Blinowska, K.J.; Rakowski, F.; Kaminski, M.; De Vico Fallani, F.; Del Percio, C.; Lizio, R.; Babiloni, C. Functional and Effective Brain Connectivity for Discrimination between Alzheimer’s Patients and Healthy Individuals: A Study on Resting State EEG Rhythms. Clin. Neurophysiol. 2017, 128, 667–680. [Google Scholar] [CrossRef]
- Cai, L.; Wei, X.; Liu, J.; Zhu, L.; Wang, J.; Deng, B.; Yu, H.; Wang, R. Functional Integration and Segregation in Multiplex Brain Networks for Alzheimer’s Disease. Front. Neurosci. 2020, 14, 51. [Google Scholar] [CrossRef]
- Chen, Y.; Cai, L.; Wang, R.; Song, Z.; Deng, B.; Wang, J.; Yu, H. DCCA Cross-Correlation Coefficients Reveals the Change of Both Synchronization and Oscillation in EEG of Alzheimer Disease Patients. Phys. A Stat. Mech. Its Appl. 2018, 490, 171–184. [Google Scholar] [CrossRef]
- Colloby, S.J.; Cromarty, R.A.; Peraza, L.R.; Johnsen, K.; Jóhannesson, G.; Bonanni, L.; Onofrj, M.; Barber, R.; O’Brien, J.T.; Taylor, J.-P. Multimodal EEG-MRI in the Differential Diagnosis of Alzheimer’s Disease and Dementia with Lewy Bodies. J. Psychiatr. Res. 2016, 78, 48–55. [Google Scholar] [CrossRef]
- Durongbhan, P.; Zhao, Y.; Chen, L.; Zis, P.; De Marco, M.; Unwin, Z.C.; Venneri, A.; He, X.; Li, S.; Zhao, Y.; et al. A Dementia Classification Framework Using Frequency and Time-Frequency Features Based on EEG Signals. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 27, 826–835. [Google Scholar] [CrossRef]
- Ge, Q.; Lin, Z.-C.; Gao, Y.-X.; Zhang, J.-X. A Robust Discriminant Framework Based on Functional Biomarkers of EEG and Its Potential for Diagnosis of Alzheimer’s Disease. Healthcare 2020, 8, 476. [Google Scholar] [CrossRef]
- Jalili, M. Graph Theoretical Analysis of Alzheimer’s Disease: Discrimination of AD Patients from Healthy Subjects. Inf. Sci. 2017, 384, 145–156. [Google Scholar] [CrossRef]
- Kulkarni, N.N.; Bairagi, V.K. Extracting Salient Features for EEG-Based Diagnosis of Alzheimer’s Disease Using Support Vector Machine Classifier. IETE J. Res. 2017, 63, 11–22. [Google Scholar] [CrossRef]
- Li, K.; Wang, J.; Li, S.; Yu, H.; Zhu, L.; Liu, J.; Wu, L. Feature Extraction and Identification of Alzheimer’s Disease Based on Latent Factor of Multi-Channel EEG. IEEE Trans. Neural Syst. Rehabil. Eng. 2021, 29, 1557–1567. [Google Scholar] [CrossRef]
- Song, Z.; Deng, B.; Wang, J.; Wang, R. Biomarkers for Alzheimer’s Disease Defined by a Novel Brain Functional Network Measure. IEEE Trans. Biomed. Eng. 2019, 66, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Trambaiolli, L.R.; Spolaôr, N.; Lorena, A.C.; Anghinah, R.; Sato, J.R. Feature Selection before EEG Classification Supports the Diagnosis of Alzheimer’s Disease. Clin. Neurophysiol. 2017, 128, 2058–2067. [Google Scholar] [CrossRef] [PubMed]
- Tzimourta, K.D.; Giannakeas, N.; Tzallas, A.T.; Astrakas, L.G.; Afrantou, T.; Ioannidis, P.; Grigoriadis, N.; Angelidis, P.; Tsalikakis, D.G.; Tsipouras, M.G. EEG Window Length Evaluation for the Detection of Alzheimer’s Disease over Different Brain Regions. Brain Sci. 2019, 9, 81. [Google Scholar] [CrossRef]
- Jiao, B.; Li, R.; Zhou, H.; Qing, K.; Liu, H.; Pan, H.; Lei, Y.; Fu, W.; Wang, X.; Xiao, X.; et al. Neural Biomarker Diagnosis and Prediction to Mild Cognitive Impairment and Alzheimer’s Disease Using EEG Technology. Alzheimer’s Res. Ther. 2023, 15, 32. [Google Scholar] [CrossRef]
- Chu, K.-T.; Lei, W.-C.; Wu, M.-H.; Fuh, J.-L.; Wang, S.-J.; French, I.T.; Chang, W.-S.; Chang, C.-F.; Huang, N.E.; Liang, W.-K.; et al. A Holo-Spectral EEG Analysis Provides an Early Detection of Cognitive Decline and Predicts the Progression to Alzheimer’s Disease. Front. Aging Neurosci. 2023, 15, 1195424. [Google Scholar] [CrossRef]
- Khare, S.K.; Acharya, U.R. Adazd-Net: Automated Adaptive and Explainable Alzheimer’s Disease Detection System Using EEG Signals. Knowl. Based Syst. 2023, 278, 110858. [Google Scholar] [CrossRef]
- Puri, D.V.; Gawande, J.P.; Rajput, J.L.; Nalbalwar, S.L. A Novel Optimal Wavelet Filter Banks for Automated Diagnosis of Alzheimer’s Disease and Mild Cognitive Impairment Using Electroencephalogram Signals. Decis. Anal. J. 2023, 9, 100336. [Google Scholar] [CrossRef]
- Nour, M.; Senturk, U.; Polat, K. A Novel Hybrid Model in the Diagnosis and Classification of Alzheimer’s Disease Using EEG Signals: Deep Ensemble Learning (DEL) Approach. Biomed. Signal Process. Control 2024, 89, 105751. [Google Scholar] [CrossRef]
- Farina, F.R.; Emek-Savaş, D.D.; Rueda-Delgado, L.; Boyle, R.; Kiiski, H.; Yener, G.; Whelan, R. A Comparison of Resting State EEG and Structural MRI for Classifying Alzheimer’s Disease and Mild Cognitive Impairment. Neuroimage 2020, 215, 116795. [Google Scholar] [CrossRef] [PubMed]
- Hsiao, Y.-T.; Tsai, C.-F.; Wu, C.-T.; Trinh, T.-T.; Lee, C.-Y.; Liu, Y.-H. MCI Detection Using Kernel Eigen-Relative-Power Features of EEG Signals. Actuators 2021, 10, 152. [Google Scholar] [CrossRef]
- Hsiao, Y.-T.; Wu, C.-T.; Tsai, C.-F.; Liu, Y.-H.; Trinh, T.-T.; Lee, C.-Y. EEG-Based Classification Between Individuals with Mild Cognitive Impairment and Healthy Controls Using Conformal Kernel-Based Fuzzy Support Vector Machine. Int. J. Fuzzy Syst. 2021, 23, 2432–2448. [Google Scholar] [CrossRef]
- Ieracitano, C.; Mammone, N.; Bramanti, A.; Hussain, A.; Morabito, F.C. A Convolutional Neural Network Approach for Classification of Dementia Stages Based on 2D-Spectral Representation of EEG Recordings. Neurocomputing 2019, 323, 96–107. [Google Scholar] [CrossRef]
- Ieracitano, C.; Mammone, N.; Hussain, A.; Morabito, F.C. A Novel Multi-Modal Machine Learning Based Approach for Automatic Classification of EEG Recordings in Dementia. Neural Netw. 2020, 123, 176–190. [Google Scholar] [CrossRef]
- Kashefpoor, M.; Rabbani, H.; Barekatain, M. Automatic Diagnosis of Mild Cognitive Impairment Using Electroencephalogram Spectral Features. J. Med. Signals Sens. 2016, 6, 25–32. [Google Scholar]
- Ruiz-Gómez, S.J.; Gómez, C.; Poza, J.; Gutiérrez-Tobal, G.C.; Tola-Arribas, M.A.; Cano, M.; Hornero, R. Automated Multiclass Classification of Spontaneous EEG Activity in Alzheimer’s Disease and Mild Cognitive Impairment. Entropy 2018, 20, 35. [Google Scholar] [CrossRef]
- Sadegh-Zadeh, S.-A.; Fakhri, E.; Bahrami, M.; Bagheri, E.; Khamsehashari, R.; Noroozian, M.; Hajiyavand, A.M. An Approach toward Artificial Intelligence Alzheimer’s Disease Diagnosis Using Brain Signals. Diagnostics 2023, 13, 477. [Google Scholar] [CrossRef]
- Van Diessen, E.; Numan, T.; van Dellen, E.; van der Kooi, A.W.; Boersma, M.; Hofman, D.; van Lutterveld, R.; van Dijk, B.W.; van Straaten, E.C.W.; Hillebrand, A.; et al. Opportunities and Methodological Challenges in EEG and MEG Resting State Functional Brain Network Research. Clin. Neurophysiol. 2015, 126, 1468–1481. [Google Scholar] [CrossRef]
- Diaz, B.A.; Van Der Sluis, S.; Moens, S.; Benjamins, J.S.; Migliorati, F.; Stoffers, D.; Den Braber, A.; Poil, S.-S.; Hardstone, R.; Van’t Ent, D.; et al. The Amsterdam Resting-State Questionnaire Reveals Multiple Phenotypes of Resting-State Cognition. Front. Hum. Neurosci. 2013, 7, 446. [Google Scholar] [CrossRef]
- Van Der Vinne, N.; Vollebregt, M.A.; Van Putten, M.J.A.M.; Arns, M. Frontal Alpha Asymmetry as a Diagnostic Marker in Depression: Fact or Fiction? A Meta-Analysis. NeuroImage Clin. 2017, 16, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Riddle, J.; Frohlich, F. Mental Activity as the Bridge between Neural Biomarkers and Symptoms of Psychiatric Illness. Clin. EEG Neurosci. 2023, 54, 399–408. [Google Scholar] [CrossRef] [PubMed]
- López Zunini, R.A.; Thivierge, J.-P.; Kousaie, S.; Sheppard, C.; Taler, V. Alterations in Resting-State Activity Relate to Performance in a Verbal Recognition Task. PLoS ONE 2013, 8, e65608. [Google Scholar] [CrossRef]
- Das, S.; Puthankattil, S.D. Complex Network Analysis of MCI-AD EEG Signals under Cognitive and Resting State. Brain Res. 2020, 1735, 146743. [Google Scholar] [CrossRef]
- Gagnon, L.G.; Belleville, S. Working Memory in Mild Cognitive Impairment and Alzheimer’s Disease: Contribution of Forgetting and Predictive Value of Complex Span Tasks. Neuropsychology 2011, 25, 226–236. [Google Scholar] [CrossRef] [PubMed]
- Kessels, R.P.C.; Molleman, P.W.; Oosterman, J.M. Assessment of Working-Memory Deficits in Patients with Mild Cognitive Impairment and Alzheimer’s Dementia Using Wechsler’s Working Memory Index. Aging Clin. Exp. Res. 2011, 23, 487–490. [Google Scholar] [CrossRef]
- San-Martin, R.; Johns, E.; Quispe Mamani, G.; Tavares, G.; Phillips, N.A.; Fraga, F.J. A Method for Diagnosis Support of Mild Cognitive Impairment through EEG Rhythms Source Location during Working Memory Tasks. Biomed. Signal Process. Control 2021, 66, 102499. [Google Scholar] [CrossRef]
- Kim, S.-K.; Kim, H.; Kim, S.H.; Kim, J.B.; Kim, L. Electroencephalography-Based Classification of Alzheimer’s Disease Spectrum during Computer-Based Cognitive Testing. Sci. Rep. 2024, 14, 5252. [Google Scholar] [CrossRef]
- Laskaris, N.A.; Tarnanas, I.; Tsolaki, M.N.; Vlaikidis, N.; Karlovasitou, A.K. Improved Detection of Amnestic MCI by Means of Discriminative Vector Quantization of Single-Trial Cognitive ERP Responses. J. Neurosci. Methods 2013, 212, 344–354. [Google Scholar] [CrossRef]
- Tarnanas, I.; Laskaris, N.; Tsolaki, M.; Muri, R.; Nef, T.; Mosimann, U.P. On the Comparison of a Novel Serious Game and Electroencephalography Biomarkers for Early Dementia Screening. Adv. Exp. Med. Biol. 2015, 821, 63–77. [Google Scholar] [CrossRef]
- Dimitriadis, S.I.; Laskaris, N.A.; Bitzidou, M.P.; Tarnanas, I.; Tsolaki, M.N. A Novel Biomarker of Amnestic MCI Based on Dynamic Cross-Frequency Coupling Patterns during Cognitive Brain Responses. Front. Neurosci. 2015, 9, 350. [Google Scholar] [CrossRef] [PubMed]
- Khatun, S.; Morshed, B.I.; Bidelman, G.M. A Single-Channel EEG-Based Approach to Detect Mild Cognitive Impairment via Speech-Evoked Brain Responses. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 27, 1063–1070. [Google Scholar] [CrossRef] [PubMed]
- McBride, J.C.; Zhao, X.; Munro, N.B.; Jicha, G.A.; Schmitt, F.A.; Kryscio, R.J.; Smith, C.D.; Jiang, Y. Sugihara Causality Analysis of Scalp EEG for Detection of Early Alzheimer’s Disease. NeuroImage Clin. 2015, 7, 258–265. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.; Yan, Z.; Sheng, C.; Wang, M.; Guan, Q.; Yu, Z.; Han, Y.; Jiang, J. A Novel Detection Tool for Mild Cognitive Impairment Patients Based on Eye Movement and Electroencephalogram. J. Alzheimers Dis. 2019, 72, 389–399. [Google Scholar] [CrossRef]
- Michalopoulos, K.; Zervakis, M.; Deiber, M.-P.; Bourbakis, N. Classification of EEG Single Trial Microstates Using Local Global Graphs and Discrete Hidden Markov Models. Int. J. Neural Syst. 2016, 26, 1650036. [Google Scholar] [CrossRef]
- Kongwudhikunakorn, S.; Kiatthaveephong, S.; Thanontip, K.; Leelaarporn, P.; Piriyajitakonkij, M.; Charoenpattarawut, T.; Autthasan, P.; Chaisaen, R.; Dujada, P.; Sudhawiyangkul, T.; et al. A Pilot Study on Visually Stimulated Cognitive Tasks for EEG-Based Dementia Recognition. IEEE Trans. Instrum. Meas. 2021, 70, 1–10. [Google Scholar] [CrossRef]
- Li, J.; Broster, L.S.; Jicha, G.A.; Munro, N.B.; Schmitt, F.A.; Abner, E.; Kryscio, R.; Smith, C.D.; Jiang, Y. A Cognitive Electrophysiological Signature Differentiates Amnestic Mild Cognitive Impairment from Normal Aging. Alzheimers Res. Ther. 2017, 9, 3. [Google Scholar] [CrossRef]
- Timothy, L.T.; Krishna, B.M.; Nair, U. Classification of Mild Cognitive Impairment EEG Using Combined Recurrence and Cross Recurrence Quantification Analysis. Int. J. Psychophysiol. 2017, 120, 86–95. [Google Scholar] [CrossRef]
- Wang, P.; Li, R.; Yu, J.; Huang, Z.; Li, J. Frequency-Dependent Brain Regional Homogeneity Alterations in Patients with Mild Cognitive Impairment during Working Memory State Relative to Resting State. Front. Aging Neurosci. 2016, 8, 60. [Google Scholar] [CrossRef]
- Wang, P.; Li, R.; Yu, J.; Huang, Z.; Yan, Z.; Zhao, K.; Li, J. Altered Distant Synchronization of Background Network in Mild Cognitive Impairment during an Executive Function Task. Front. Behav. Neurosci. 2017, 11, 174. [Google Scholar] [CrossRef]
- Stam, C.J.; Nolte, G.; Daffertshofer, A. Phase Lag Index: Assessment of Functional Connectivity from Multi Channel EEG and MEG with Diminished Bias from Common Sources. Hum. Brain Mapp. 2007, 28, 1178–1193. [Google Scholar] [CrossRef] [PubMed]
- Yu, M. Benchmarking Metrics for Inferring Functional Connectivity from Multi-Channel EEG and MEG: A Simulation Study. Chaos 2020, 30, 123124. [Google Scholar] [CrossRef] [PubMed]
- Nolte, G.; Bai, O.; Wheaton, L.; Mari, Z.; Vorbach, S.; Hallett, M. Identifying True Brain Interaction from EEG Data Using the Imaginary Part of Coherency. Clin. Neurophysiol. 2004, 115, 2292–2307. [Google Scholar] [CrossRef]
- Nobukawa, S.; Yamanishi, T.; Kasakawa, S.; Nishimura, H.; Kikuchi, M.; Takahashi, T. Classification Methods Based on Complexity and Synchronization of Electroencephalography Signals in Alzheimer’s Disease. Front. Psychiatry 2020, 11, 255. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Gómez, S.J.; Hornero, R.; Poza, J.; Maturana-Candelas, A.; Pinto, N.; Gómez, C. Computational Modeling of the Effects of EEG Volume Conduction on Functional Connectivity Metrics. Application to Alzheimer’s Disease Continuum. J. Neural Eng. 2019, 16, 066019. [Google Scholar] [CrossRef]
- Buscema, M.; Vernieri, F.; Massini, G.; Scrascia, F.; Breda, M.; Rossini, P.M.; Grossi, E. An Improved I-FAST System for the Diagnosis of Alzheimer’s Disease from Unprocessed Electroencephalograms by Using Robust Invariant Features. Artif. Intell. Med. 2015, 64, 59–74. [Google Scholar] [CrossRef]
- Siuly, S.; Alcin, O.F.; Kabir, E.; Sengur, A.; Wang, H.; Zhang, Y.; Whittaker, F. A New Framework for Automatic Detection of Patients With Mild Cognitive Impairment Using Resting-State EEG Signals. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 1966–1976. [Google Scholar] [CrossRef]
- Chen, S.; Xie, H.; Yang, H.; Fan, C.; Hou, Z.; Zhang, C. A Classification Framework Based on Multi-Modal Features for Detection of Cognitive Impairments. In Intelligent Robotics; Yu, Z., Hei, X., Li, D., Song, X., Lu, Z., Eds.; Communications in Computer and Information Science; Springer Nature Singapore: Singapore, 2023; Volume 1770, pp. 349–361. ISBN 978-981-99-0300-9. [Google Scholar]
- Cao, Y.; Cai, L.; Wang, J.; Wang, R.; Yu, H.; Cao, Y.; Liu, J. Characterization of Complexity in the Electroencephalograph Activity of Alzheimer’s Disease Based on Fuzzy Entropy. Chaos Interdiscip. J. Nonlinear Sci. 2015, 25, 083116. [Google Scholar] [CrossRef]
- Gallego-Jutglà, E.; Solé-Casals, J.; Vialatte, F.-B.; Dauwels, J.; Cichocki, A. A Theta-Band EEG Based Index for Early Diagnosis of Alzheimer’s Disease. JAD 2014, 43, 1175–1184. [Google Scholar] [CrossRef]
- Gallego-Jutglà, E.; Solé-Casals, J.; Vialatte, F.-B.; Elgendi, M.; Cichocki, A.; Dauwels, J. A Hybrid Feature Selection Approach for the Early Diagnosis of Alzheimer’s Disease. J. Neural Eng. 2015, 12, 016018. [Google Scholar] [CrossRef]
- Ueda, T.; Musha, T.; Asada, T.; Yagi, T. Classification Method for Mild Cognitive Impairment Based on Power Variability of EEG Using Only a Few Electrodes. Elect. Comm. Jpn. 2016, 99, 107–114. [Google Scholar] [CrossRef]
- Wallace, B.; Knoefel, F.; Goubran, R.; Lopez Zunini, R.A.; Ren, Z.; Maccosham, A. EEG/ERP: Within Episodic Assessment Framework for Cognition. IEEE Trans. Instrum. Meas. 2017, 66, 2525–2534. [Google Scholar] [CrossRef]
- McBride, J.C.; Zhao, X.; Munro, N.; Jicha, G.; Smith, C.; Jiang, Y. Discrimination of Mild Cognitive Impairment and Alzheimer’s Disease Using Transfer Entropy Measures of Scalp EEG. J. Healthc. Eng. 2015, 6, 55–70. [Google Scholar] [CrossRef]
- McBride, J.C.; Zhao, X.; Munro, N.B.; Smith, C.D.; Jicha, G.A.; Hively, L.; Broster, L.S.; Schmitt, F.A.; Kryscio, R.J.; Jiang, Y. Spectral and Complexity Analysis of Scalp EEG Characteristics for Mild Cognitive Impairment and Early Alzheimer’s Disease. Comput. Methods Programs Biomed. 2014, 114, 153–163. [Google Scholar] [CrossRef] [PubMed]
- Trinh, T.-T.; Tsai, C.-F.; Hsiao, Y.-T.; Lee, C.-Y.; Wu, C.-T.; Liu, Y.-H. Identifying Individuals With Mild Cognitive Impairment Using Working Memory-Induced Intra-Subject Variability of Resting-State EEGs. Front. Comput. Neurosci. 2021, 15, 700467. [Google Scholar] [CrossRef] [PubMed]
- Chai, J.; Wu, R.; Li, A.; Xue, C.; Qiang, Y.; Zhao, J.; Zhao, Q.; Yang, Q. Classification of Mild Cognitive Impairment Based on Handwriting Dynamics and qEEG. Comput. Biol. Med. 2023, 152, 106418. [Google Scholar] [CrossRef]
- Li, X.; Yang, C.; Xie, P.; Han, Y.; Su, R.; Li, Z.; Liu, Y. The Diagnosis of Amnestic Mild Cognitive Impairment by Combining the Characteristics of Brain Functional Network and Support Vector Machine Classifier. J. Neurosci. Methods 2021, 363, 109334. [Google Scholar] [CrossRef]
- Liu, X.; Zhang, C.; Ji, Z.; Ma, Y.; Shang, X.; Zhang, Q.; Zheng, W.; Li, X.; Gao, J.; Wang, R.; et al. Multiple Characteristics Analysis of Alzheimer’s Electroencephalogram by Power Spectral Density and Lempel-Ziv Complexity. Cogn. Neurodyn 2016, 10, 121–133. [Google Scholar] [CrossRef]
- Bairagi, V. EEG Signal Analysis for Early Diagnosis of Alzheimer Disease Using Spectral and Wavelet Based Features. Int. J. Inf. Technol. 2018, 10, 403–412. [Google Scholar] [CrossRef]
- Vecchio, F.; Miraglia, F.; Alù, F.; Menna, M.; Judica, E.; Cotelli, M.; Rossini, P.M. Classification of Alzheimer’s Disease with Respect to Physiological Aging with Innovative EEG Biomarkers in a Machine Learning Implementation. J. Alzheimer’s Dis. 2020, 75, 1253–1261. [Google Scholar] [CrossRef]
- Klepl, D.; He, F.; Wu, M.; Blackburn, D.J.; Sarrigiannis, P.G. Cross-Frequency Multilayer Network Analysis with Bispectrum-Based Functional Connectivity: A Study of Alzheimer’s Disease. Neuroscience 2023, 521, 77–88. [Google Scholar] [CrossRef]
- Albert, M.S.; DeKosky, S.T.; Dickson, D.; Dubois, B.; Feldman, H.H.; Fox, N.C.; Gamst, A.; Holtzman, D.M.; Jagust, W.J.; Petersen, R.C.; et al. The Diagnosis of Mild Cognitive Impairment Due to Alzheimer’s Disease: Recommendations from the National Institute on Aging-Alzheimer’s Association Workgroups on Diagnostic Guidelines for Alzheimer’s Disease. Alzheimers Dement. 2011, 7, 270–279. [Google Scholar] [CrossRef]
- McKhann, G.M.; Knopman, D.S.; Chertkow, H.; Hyman, B.T.; Jack, C.R.; Kawas, C.H.; Klunk, W.E.; Koroshetz, W.J.; Manly, J.J.; Mayeux, R.; et al. The Diagnosis of Dementia Due to Alzheimer’s Disease: Recommendations from the National Institute on Aging-Alzheimer’s Association Workgroups on Diagnostic Guidelines for Alzheimer’s Disease. Alzheimers Dement. 2011, 7, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool For Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Tsai, C.-F.; Lee, W.-J.; Wang, S.-J.; Shia, B.-C.; Nasreddine, Z.; Fuh, J.-L. Psychometrics of the Montreal Cognitive Assessment (MoCA) and Its Subscales: Validation of the Taiwanese Version of the MoCA and an Item Response Theory Analysis. Int. Psychogeriatr. 2012, 24, 651–658. [Google Scholar] [CrossRef]
- Sahakian, B.J.; Morris, R.G.; Evenden, J.L.; Heald, A.; Levy, R.; Philpot, M.; Robbins, T.W. A Comparative Study of Visuospatial Memory and Learning in Alzheimer-Type Dementia and Parkinson’s Disease. Brain 1988, 111 Pt 3, 695–718. [Google Scholar] [CrossRef]
- Fowler, K.S.; Saling, M.M.; Conway, E.L.; Semple, J.M.; Louis, W.J. Computerized Delayed Matching to Sample and Paired Associate Performance in the Early Detection of Dementia. Appl. Neuropsychol. 1995, 2, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Delorme, A.; Makeig, S. EEGLAB: An Open Source Toolbox for Analysis of Single-Trial EEG Dynamics Including Independent Component Analysis. J. Neurosci. Methods 2004, 134, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Mognon, A.; Jovicich, J.; Bruzzone, L.; Buiatti, M. ADJUST: An Automatic EEG Artifact Detector Based on the Joint Use of Spatial and Temporal Features. Psychophysiology 2011, 48, 229–240. [Google Scholar] [CrossRef]
- Kashefpoor, M.; Rabbani, H.; Barekatain, M. Supervised Dictionary Learning of EEG Signals for Mild Cognitive Impairment Diagnosis. Biomed. Signal Process. Control 2019, 53, 101559. [Google Scholar] [CrossRef]
- Wu, C.-T.; Huang, H.-C.; Huang, S.; Chen, I.-M.; Liao, S.-C.; Chen, C.-K.; Lin, C.; Lee, S.-H.; Chen, M.-H.; Tsai, C.-F.; et al. Resting-State EEG Signal for Major Depressive Disorder Detection: A Systematic Validation on a Large and Diverse Dataset. Biosensors 2021, 11, 499. [Google Scholar] [CrossRef] [PubMed]
- Challis, R.E.; Kitney, R.I. Biomedical Signal Processing (in Four Parts). Part 3. The Power Spectrum and Coherence Function. Med. Biol. Eng. Comput. 1991, 29, 225–241. [Google Scholar] [CrossRef] [PubMed]
- Gu, Q.; Li, Z.; Han, J. Generalized Fisher Score for Feature Selection. arXiv 2012, arXiv:1202.3725. [Google Scholar]
- Lin, Y.-P.; Wang, C.-H.; Jung, T.-P.; Wu, T.-L.; Jeng, S.-K.; Duann, J.-R.; Chen, J.-H. EEG-Based Emotion Recognition in Music Listening. IEEE Trans. Biomed. Eng. 2010, 57, 1798–1806. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.-T.; Dillon, D.G.; Hsu, H.-C.; Huang, S.; Barrick, E.; Liu, Y.-H. Depression Detection Using Relative EEG Power Induced by Emotionally Positive Images and a Conformal Kernel Support Vector Machine. Appl. Sci. 2018, 8, 1244. [Google Scholar] [CrossRef]
- Abdumalikov, S.; Kim, J.; Yoon, Y. Performance Analysis and Improvement of Machine Learning with Various Feature Selection Methods for EEG-Based Emotion Classification. Appl. Sci. 2024, 14, 10511. [Google Scholar] [CrossRef]
- Garn, H.; Waser, M.; Deistler, M.; Schmidt, R.; Dal-Bianco, P.; Ransmayr, G.; Zeitlhofer, J.; Schmidt, H.; Seiler, S.; Sanin, G.; et al. Quantitative EEG in Alzheimer’s Disease: Cognitive State, Resting State and Association with Disease Severity. Int. J. Psychophysiol. 2014, 93, 390–397. [Google Scholar] [CrossRef]
- Barzegaran, E.; van Damme, B.; Meuli, R.; Knyazeva, M.G. Perception-Related EEG Is More Sensitive to Alzheimer’s Disease Effects than Resting EEG. Neurobiol. Aging 2016, 43, 129–139. [Google Scholar] [CrossRef]
- Timothy, L.T.; Krishna, B.M.; Nair, U. Recurrence Quantification Analysis of MCI EEG under Resting and Visual Memory Task Conditions. Biomed. Eng. Appl. Basis Commun. 2019, 31, 1950025. [Google Scholar] [CrossRef]
- Amezquita-Sanchez, J.P.; Mammone, N.; Morabito, F.C.; Adeli, H. A New Dispersion Entropy and Fuzzy Logic System Methodology for Automated Classification of Dementia Stages Using Electroencephalograms. Clin. Neurol. Neurosurg. 2021, 201, 106446. [Google Scholar] [CrossRef]
- Pirrone, D.; Weitschek, E.; Di Paolo, P.; De Salvo, S.; De Cola, M.C. EEG Signal Processing and Supervised Machine Learning to Early Diagnose Alzheimer’s Disease. Appl. Sci. 2022, 12, 5413. [Google Scholar] [CrossRef]
- Huggins, C.J.; Escudero, J.; Parra, M.A.; Scally, B.; Anghinah, R.; Vitória Lacerda De Araújo, A.; Basile, L.F.; Abasolo, D. Deep Learning of Resting-State Electroencephalogram Signals for Three-Class Classification of Alzheimer’s Disease, Mild Cognitive Impairment and Healthy Ageing. J. Neural Eng. 2021, 18, 046087. [Google Scholar] [CrossRef]
- Schoonhoven, D.N.; Briels, C.T.; Hillebrand, A.; Scheltens, P.; Stam, C.J.; Gouw, A.A. Sensitive and Reproducible MEG Resting-State Metrics of Functional Connectivity in Alzheimer’s Disease. Alzheimer’s Res. Ther. 2022, 14, 38. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Zhan, P.; Wang, G.; Yu, X.; Liu, H.; Wang, W. Changes of Brain Functional Network in Alzheimer’s Disease and Frontotemporal Dementia: A Graph-Theoretic Analysis. BMC Neurosci. 2024, 25, 30. [Google Scholar] [CrossRef]
- Sankari, Z.; Adeli, H.; Adeli, A. Intrahemispheric, Interhemispheric, and Distal EEG Coherence in Alzheimer’s Disease. Clin. Neurophysiol. 2011, 122, 897–906. [Google Scholar] [CrossRef] [PubMed]
- Wada, Y.; Nanbu, Y.; Kikuchi, M.; Koshino, Y.; Hashimoto, T.; Yamaguchi, N. Abnormal Functional Connectivity in Alzheimer’s Disease: Intrahemispheric EEG Coherence during Rest and Photic Stimulation. Eur. Arch. Psychiatry Clin. Neurosci. 1998, 248, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Grady, C.; Maisog, J.; Horwitz, B.; Ungerleider, L.; Mentis, M.; Salerno, J.; Pietrini, P.; Wagner, E.; Haxby, J. Age-Related Changes in Cortical Blood Flow Activation during Visual Processing of Faces and Location. J. Neurosci. 1994, 14, 1450–1462. [Google Scholar] [CrossRef]
- Morcom, A.M.; Henson, R.N.A. Increased Prefrontal Activity with Aging Reflects Nonspecific Neural Responses Rather than Compensation. J. Neurosci. 2018, 38, 7303–7313. [Google Scholar] [CrossRef]
- Davis, S.W.; Dennis, N.A.; Daselaar, S.M.; Fleck, M.S.; Cabeza, R. Que PASA? The Posterior-Anterior Shift in Aging. Cereb. Cortex 2008, 18, 1201–1209. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | HC | MCI | AD | p | Effect Size |
|---|---|---|---|---|---|
| n = 27 | n = 24 | n = 21 | |||
| Gender | 17F, 10M | 14F, 10M | 8F, 13M | 0.202 | 0.211 |
| Age | 69.93 (4.98) | 70.96 (8.20) | 71.19 (5.04) | 0.750 | 0.008 |
| Education (years) | 13.44 (3.18) | 12.13 (3.76) | 11.48 (3.82) | 0.153 | 0.053 |
| MMSE | 28.26 (1.79) | 26.58 (1.89) | 21.62 (6.03) | <0.001 | 0.379 |
| MoCA | 25.89 (3.29) | 23.08 (4.11) | 16.52 (6.67) | <0.001 | 0.405 |
| LDA | KNN | SVM | LR | ||||||
|---|---|---|---|---|---|---|---|---|---|
| ACC | ACC | ACC | ACC | ||||||
| AD vs. MCI | rsEEG | 88.89 | 13/16 | 84.44 | 18/20 | 88.89 | 11/15 | 88.89 | 11/15 |
| ME-EEG | 84.44 | 44/29 | 86.67 | 23/20 | 84.44 | 12/13 | 86.67 | 25/22 | |
| ME-TIER | 95.56 | 20/21 | 95.56 | 9/13 | 95.56 | 11/14 | 95.56 | 23/21 | |
| MM-EEG | 93.33 | 9/12 | 84.44 | 16/18 | 88.89 | 23/21 | 82.22 | 43/26 | |
| MM-TIER | 93.33 | 16/17 | 95.56 | 41/26 | 97.78 | 42/26 | 97.78 | 41/26 | |
| AD vs. HC | rsEEG | 89.58 | 12/16 | 95.83 | 15/17 | 97.92 | 17/21 | 89.58 | 32/25 |
| ME-EEG | 85.42 | 8/12 | 83.33 | 30/27 | 79.17 | 2/4 | 85.42 | 41/30 | |
| ME-TIER | 95.83 | 21/21 | 95.83 | 45/27 | 95.83 | 27/22 | 93.75 | 14/18 | |
| MM-EEG | 83.33 | 6/7 | 81.25 | 15/14 | 89.58 | 6/7 | 81.25 | 42/28 | |
| MM-TIER | 97.92 | 47/26 | 95.83 | 38/25 | 95.83 | 34/24 | 97.92 | 38/25 | |
| MCI vs. HC | rsEEG | 86.27 | 15/18 | 90.20 | 47/29 | 94.12 | 45/28 | 90.20 | 28/26 |
| ME-EEG | 88.24 | 8/15 | 94.12 | 36/27 | 92.16 | 49/28 | 94.12 | 38/27 | |
| ME-TIER | 92.16 | 11/16 | 98.04 | 43/27 | 98.04 | 44/27 | 98.04 | 41/26 | |
| MM-EEG | 94.12 | 12/16 | 90.20 | 10/14 | 94.12 | 40/28 | 90.20 | 31/28 | |
| MM-TIER | 96.08 | 12/17 | 98.04 | 44/27 | 98.04 | 21/25 | 98.04 | 28/26 | |
| AD vs. MCI vs. HC | rsEEG | 70.83 | 10/13 | 75.00 | 68/29 | 75.00 | 36/24 | 72.22 | 37/24 |
| ME-EEG | 66.67 | 12/15 | 61.11 | 68/29 | 73.61 | 71/29 | 72.22 | 67/29 | |
| ME-TIER | 76.39 | 31/22 | 83.33 | 52/27 | 91.67 | 65/28 | 84.72 | 53/27 | |
| MM-EEG | 70.83 | 22/22 | 70.83 | 40/27 | 80.56 | 63/30 | 75.00 | 52/28 | |
| MM-TIER | 79.17 | 67/29 | 83.33 | 71/29 | 91.67 | 68/29 | 93.06 | 67/29 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, Y.-H.; Trinh, T.-T.; Tsai, C.-F.; Yang, J.-K.; Lee, C.-Y.; Wu, C.-T. A Novel Working Memory Task-Induced EEG Response (WM-TIER) Feature Extraction Framework for Detecting Alzheimer’s Disease and Mild Cognitive Impairment. Biosensors 2025, 15, 289. https://doi.org/10.3390/bios15050289
Liu Y-H, Trinh T-T, Tsai C-F, Yang J-K, Lee C-Y, Wu C-T. A Novel Working Memory Task-Induced EEG Response (WM-TIER) Feature Extraction Framework for Detecting Alzheimer’s Disease and Mild Cognitive Impairment. Biosensors. 2025; 15(5):289. https://doi.org/10.3390/bios15050289
Chicago/Turabian StyleLiu, Yi-Hung, Thanh-Tung Trinh, Chia-Fen Tsai, Jie-Kai Yang, Chun-Ying Lee, and Chien-Te Wu. 2025. "A Novel Working Memory Task-Induced EEG Response (WM-TIER) Feature Extraction Framework for Detecting Alzheimer’s Disease and Mild Cognitive Impairment" Biosensors 15, no. 5: 289. https://doi.org/10.3390/bios15050289
APA StyleLiu, Y.-H., Trinh, T.-T., Tsai, C.-F., Yang, J.-K., Lee, C.-Y., & Wu, C.-T. (2025). A Novel Working Memory Task-Induced EEG Response (WM-TIER) Feature Extraction Framework for Detecting Alzheimer’s Disease and Mild Cognitive Impairment. Biosensors, 15(5), 289. https://doi.org/10.3390/bios15050289