1. Introduction
Nowadays, there has been a growing interest in studying factors affecting female physiological response to exercise, such as oxygen saturation variations [
1,
2,
3,
4,
5]. However, throughout history, women have had to fight for their self-improvement in the sports world until they had the right to participate in specific sports and certain competitions like the Olympic Games [
6]. The restriction was partly based on the idea that vigorous physical activity could impair women’s health and adversely affect their reproductive capacity. These myths still survive today in some countries and have limited women’s access to sports due to several factors such as social, political, religious, or biological [
7,
8,
9,
10,
11,
12]. Traditionally, it has been believed that the anatomical differences between men and women make men more suitable for strength sports and women for those sports that require greater flexibility [
13,
14,
15]. However, women’s participation has reached areas previously considered exclusive to men, such as weightlifting or marathon running [
16,
17,
18,
19]. Therefore, recent decades have witnessed a remarkable expansion of women’s sport, specifically in long-duration activities [
20,
21,
22,
23,
24,
25], dispelling myths from other times based more on socio-cultural attitudes than on scientific research data.
Alterations in lung gas exchange occur during intense physical exercise [
26,
27,
28,
29]. These differences typically manifest as a decrease in arterial partial pressure of oxygen (
), known as hypoxemia, and an associated increase in the alveolar–arterial
difference
-
, which, potentially, represents a significant barrier to endurance performance [
30]. Studies of the oxygen saturation (
) evolution in women during maximal exercise have shown an early decrease in oxygen saturation at markedly lower oxygen intakes than in men [
31,
32]. Some studies supported the controversial hypothesis that healthy active women experience a certain exercise-induced arterial hypoxia (EIAH) because of a lower vital capacity of the lung with airways of smaller diameter and smaller diffusion surface than in men of similar age, height, and body mass index (BMI), implying that the lung structure may compromise oxygen diffusion [
33,
34,
35]. However, more recent studies performed in women in both normoxic and hyperoxic environments assert that the oxygen desaturation observed in women is the main limiting factor in achieving a higher maximum oxygen uptake,
, levels rather than the lung size or pulmonary capacity [
28,
36,
37,
38,
39,
40,
41].
The current progress of wearable sensors for continuous monitoring of physiological variable parameters has given evidence that using this technology to measure and quantify human responses to exercise has worthiness in improving the understanding of the exercise effects [
42,
43,
44,
45,
46,
47]. In particular, heart rate (HR) and oxygen saturation determination by photoplethysmography (PPG) constitute a key factor that provides relevant information to personalize training interventions [
48,
49,
50,
51,
52]. The PPG sensor monitors differences in the light intensity between blood and the surrounding tissue [
53,
54]. These differences are associated with small variations in the tissue’s blood perfusion, providing information about the cardiovascular system, in particular, the pulse rate, oxygen saturation, blood pressure, and blood vessel stiffness [
55,
56]. The
in tissues is determined by optically quantifying the concentration of oxyhemoglobin and deoxy-hemoglobin [
57,
58,
59].
Continuous monitoring by pulse oximetry is a useful, simple, fairly accurate, reproducible, and non-invasive optical technique to study oxygenation during physical effort [
60,
61,
62,
63,
64,
65,
66,
67,
68]. Although it has some limitations, essentially due to cold-related deficient blood circulation [
69,
70], dark skin pigmentation [
71,
72,
73], or movement artifacts [
74,
75,
76]. Its interest does not lie in obtaining absolute values of peripheral oxygen saturation, but in the continuous recording of eventual changes. Therefore, pulse oximetry can be applied to evaluate the physical performance of different disciplines athletes adapted to the physiological responses obtaining broad correlations with oxygen uptake [
59,
62,
77].
The aerobic threshold (AeT) represents the limit between the slight and moderate intensity of exercise (lowest intensity zone) known as the first ventilatory threshold
. Exercising around
allows stimulating aerobic metabolisms while above
, blood lactate and pH start to increase and decrease, respectively [
78,
79,
80,
81]. The anaerobic threshold (AnT) represents the limit between moderate and high intensity of exercise (highest intensity zone) known as the second ventilatory threshold,
, which is not sustainable for a long duration [
82,
83]. Determining the
and
is of significant importance for both performance monitoring and training prescription because it allows us to establish different physical work zones [
84,
85,
86,
87].
This study aims to analyze the correlations between blood oxygen saturation variations and the ventilatory thresholds ( or AeT and or AnT) during a maximum stress test in female athletes with different skin pigmentation and different physical fitness condition. Correlation analyses were carried out between the occurrence time of the significant drops and the AeT and the AnT, the total test time, the maximum oxygen uptake, and the anthropometric variables.
3. Results
The results obtained from the stress test for the total population of 25 light-skinned and 2 dark-skinned healthy female athletes are shown in
Table 2 and
Table 3. Following the protocol described in
Section 2.2, we recorded the maximum HR, the basal
, the
values, and the maximum oxygen uptake,
.
The participants were classified according to their physical fitness condition based on their maximum oxygen uptake,
, as is shown in
Table 2. The
of participants were classified by medium physical fitness condition with a
between 30 and 40 mL/kg/min, the
of the athletes showed a good physical condition with a consumption between 40 and 50 mL/kg/min, while the remaining
showed an excellent physical condition with a
greater than 50 mL/kg/min.
Since the main objective of this study was assessing whether oxygen saturation variations could be related to the AeT or AnT appearance, the
value was continuous monitored. The basal saturation was also recorded at the beginning of the test in order to analyze the differences.
Table 3 shows the ergospirometry measured variables obtained from the stress test expressed by their average value ± standard deviation,
± SD, and the average times related to the significant drops, expressed by
SD.
The maximum HR observed ranged between values of 168 and 205 bpm, with a mean value of (189.81 ± 8.54) bpm. The basal ranged from 1.7 to 7.8 mL/kg/min with a mean value of (4.69 ± 1.53) mL/kg/min. The ranged from 37.09 to 64.78 mL/kg/min, with a mean value of (48.9 ± 7.61) mL/kg/min. The basal saturation ranged from 97% to 99%, with a mean value of (98.07 ± 7.61)%. To evaluate whether a higher decrease could influence some other variables such as the AeT or AnT appearance, the minimum value observed and the time of occurrence was recorded.
Figure 4 shows a flowchart representing the different events during the effort test. The time to observe the first and the second
drops (desaturation prior to the AeT and the maximum desaturation prior to AnT) are marked by the yellow arrows with the corresponding saturation values shown in the yellow circles. The first
drop value was
occurring at
min. The minimum
value,
was found between 6.28 and 10.83 min with a mean time of
= (8.97 ± 1.32) min marked by the pink arrow. We also defined
min as the time to reach the AeT from the first drop,
min as the time to observe the second
drop prior to AnT, and
min as the time to reach the AnT from the second
drop, depicted by red arrows. Besides, the blue arrows correspond to the AeT appearance time fluctuated between 4.33 and 8.17 min, with a mean value of
= (6.06 ± 0.96) min, and the AnT appearance time ranged between 6.83 and 11.83 min, with a mean value of
= (9.69 ± 1.20) min. The green squares correspond to the start and the end of the test. The total test time ranged between 7.83 and 14.00 min, with a mean value of
= (10.76 ± 1.45) min.
A common behavior of the
evolution during the incremental exercise test was observed in all female athletes. First, we observed a
decrease before the AeT or
followed by a second significant drop before the AnT or
, as it is also shown in
Figure 4. The temporal evolution of the oxygen saturation
and the HR obtained from the ECG signal for two athletes is depicted in
Figure 5. The blue lines correspond to the
temporal series while the red and pink lines correspond to the HR dataset in bmp. The continuous line correspond to an athlete with a medium physical fitness condition according to the criterion established in
Table 2. The dash-dotted lines correspond to a dark-skinned athlete with an excellent physical fitness condition. We found several differences between both athletes. The
values range from 87% to 100% while the
ranged from 70 bmp to 188 bmp for the dark-skinned athlete with an excellent physical fitness condition. On the contrary, for the light-skinned athlete with medium excellent physical fitness condition the
values range from 91% to 99% and the HR from 67 bmp to 181 bmp. The total test time was also longer for the athlete with a better physical fitness condition, i.e., higher
. It can be also observed that the second saturation drop (prior to AT) occurs a few seconds after the
is reached. Once the minimum value of
is reached, the recovery phase begins. In this phase,
increases while HR decreases. Small differences were also found in the recovery time between both athletes. The recovery time, time to reach lower HR values and higher saturation values, was shorter in athletes with a better physical fitness condition.
A statistical study of Pearson’s correlations was performed concerning the evolutionary and temporal parameters of the oxygen saturation values obtained by ergospirometry. For this purpose, a univariate study was made for the different time events of the effort test shown in
Figure 4 and their relationship with the study’s independent variables.
Table 4 shows the Pearson’s correlation coefficients between the different time events during the effort test shown in
Figure 4, i.e., AeT, the AnT, the desaturation time, total test time, and
with age, height, weight, body mass index (BMI), basal
,
, and maximum HR reached during the test for each participant. The values with a significance level
p < 0.05 are marked in bold. Statistically significant correlations were found for the maximum oxygen uptake,
concerning the appearance of the AeT, the AnT, the total test time,
, the maximum desaturation time,
, and
. However, no significant correlations were found between the rest of the variables and these times.
Furthermore,
Table 5 shows an analysis of covariance to study the relationship between the appearance time of both thresholds (AeT and AnT), the desaturation time
, the total test time
, and the time to observe the second
drop value after the AeT,
, with respect to the skin pigmentation, physical fitness condition and type of practiced sport. The values with a significance level
p < 0.05 are marked in bold. Statistically significant Pearson correlations were found for the physical fitness condition variable concerning the AnT occurrence, the total test time, the desaturation time, and
. We also found correlations between the skin pigmentation and the AnT or
appearance. However, there were no correlations for the type of practiced sport.
In order to study the dependence of the
variations with the AeT appearance,
Table 6 shows the Pearson correlations analyzed regarding the times
and
. The values with a significance level
p < 0.05 are marked in bold. We could not find any correlations between the AeT and these times. However, when comparing how
and
could influence each other, we observed a negative correlation between them with a negative Pearson coefficient of −0.789, i.e., as
increases,
decreases.
Figure 6 shows the regression model relating both times with a coefficient of determination
and
, which indicates that for every minute that
increases,
decreases by 0.73 min.
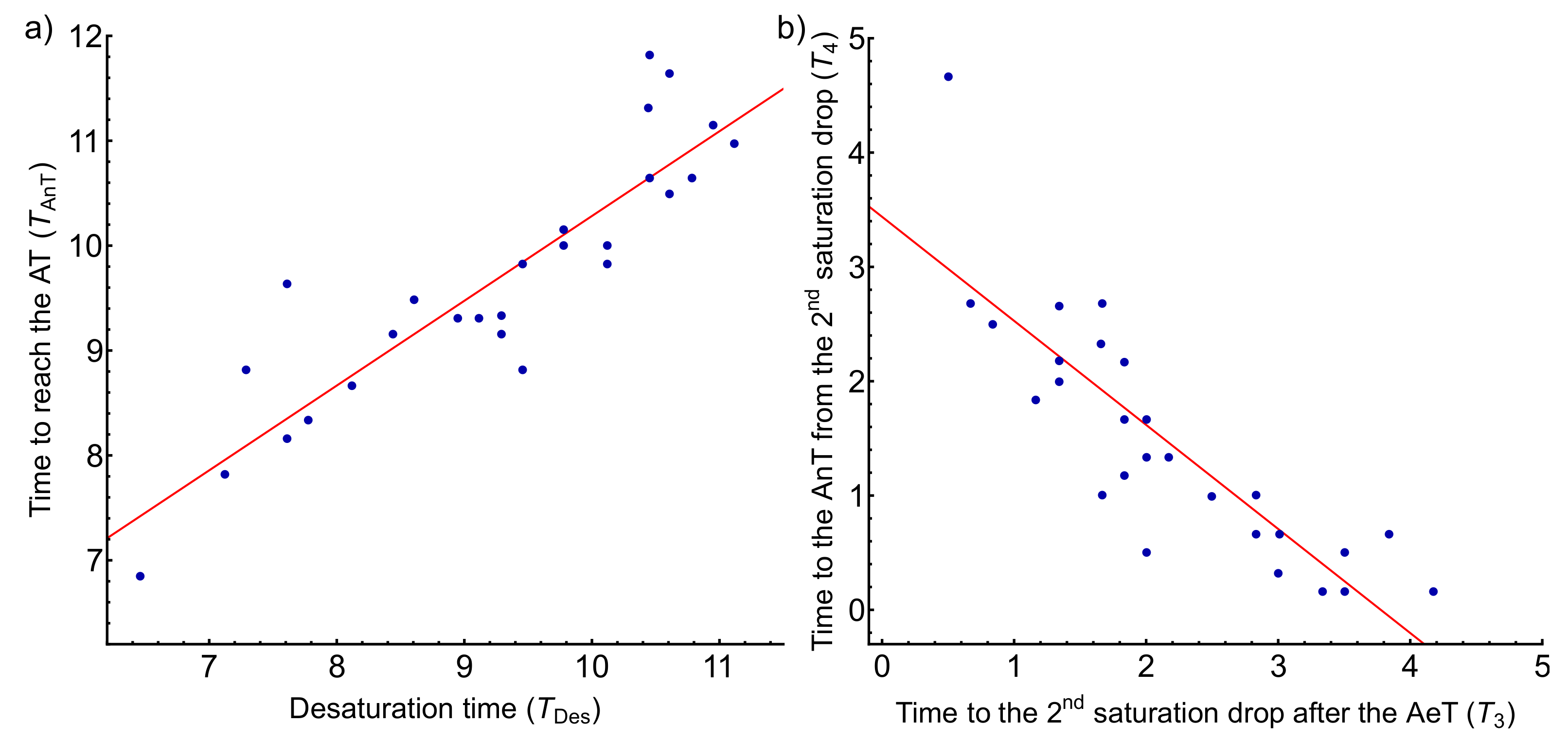
We proceeded in the same way to analyze the influence of the AnT appearance with the previous parameters.
Table 7 shows the Pearson correlations for the AnT appearance and the times derived from the
variations occurring after the AeT. A statistically significant Pearson correlation coefficient close to 1 (0.892) when correlating the AnT appearance time with the desaturation time
is observed. The
corresponds to
+
+
+
while the desaturation time corresponds to
+
+
, as depicted in
Figure 4. Panel a of
Figure 7 shows the regression model between both times with a coefficient of determination of
, that is, it explains
of the variability of the AnT as a function of the desaturation time.
gives the regression line; hence it can be prophesied that for every minute that desaturation takes to appear, the AnT takes 0.81 min to appear. Furthermore, when comparing how
and
could influence each other, we observed a strong negative correlation between them (−0.849), i.e., as
increases,
decreases. Panel b of
Figure 7 corresponds to the regression model between these two times with a coefficient of determination of
and
. The time
is also correlated with the AnT appearance with a statistically significant Pearson coefficient of 0.383.
To sum up,
Table 8 summarizes the most statistically significant correlations found in this study. The maximum oxygen uptake,
, is the variable that presented the most independent correlations with each time event. However, the variables with the highest correlations were the desaturation time,
, and the appearance of the AnT.
4. Discussion
The athletes subjected to the study practiced different multi-sprint-based sports. In particular, 14 volunteers practiced 11-a-side football (aerobic-anaerobic sport), 10 long-distance athletics (aerobic sport), 1 sprint athletics (anaerobic sport), and 2 basketball (aerobic–anaerobic sport). Therefore, of the sample practiced aerobic-type sports, practiced anaerobic-type sports, and practiced mixed-type sports.
When comparing the validity of the population sample size with other similar studies, it turned out to be positive. In particular, the study by Harms [
31] was conducted on a sample of 29 women, the study by St. Croix et al. [
34] included 28 women. The sample size was 27 in more recent studies such as Wetter et al. [
88], and even smaller in the one by Yoshiga and Higuchi who tested 16 women [
89] and the performed by Zavorsky et al. and Woorons et al. [
90] with only 14 females [
91].
According to the physical fitness condition, although we found a study that specified the maximum oxygen uptake [
31], the vast majority of the studies did not specify a quantitative scale to classify the physical fitness condition of the sample population. In these studies, the authors refer to a very varied physical level from sedentary to more trained people with maximum oxygen uptake in a range between 31 and 70 mL/kg/min [
34,
88,
89,
90,
91]. A performed study in men and women mountaineering trainees at 4350 m above sea level showed that the reduction of maximum aerobic capacity was lower in women than in men under similar modes of ascent [
92]. On the other hand, recent studies have shown that women tend to perform better in long-duration activities such as marathons, ultra-cycling, or long-distance swimming [
22,
23,
24]. Taking this into account, it is striking that some studies attribute the presence of decreases in peripheral oxygen saturation in women to inconclusive problems of the respiratory system’s inadequacy to physical exertion. It should be pointed out that oxygen consumption is not a parameter that defines lung function, but instead helps to determine an individual’s physical fitness condition. Therefore, studies that rely on this parameter to check lung function can lead to erroneous conclusions. Detailed sex comparisons are difficult because the number of subjects studied to date has been woefully small, and more subjects are needed to be tested to confirm the hypothesis mentioned above [
27,
40,
41,
92,
93,
94,
95].
Although there is evidence that hypoventilation may play a role in decreased pulmonary gas exchange in women during exercise, it appears that ventilation cannot fully compensate for the increased
A-
[
35,
91,
93]. Other studies assert that acute ventilatory response to hypoxia (AHVR) is not related to the development of EIAH during maximal exercise in trained endurance and untrained individuals (men or woman) [
29,
96,
97]. Indeed, concerning the degree of EIAH at the onset of high-intensity exercise, prolonging exercise to exhaustion had no other deleterious effects on
A-
, and the degree of gas exchange impairment was not related to individual differences in small or large airway function or reactivity [
88]. The AHVR was related to the peak of oxygen consumption, but not to oxygen saturation. Oxyhemoglobin saturation
values were lower in trained men
and women
compared to untrained men and women
vs.
, respectively [
96]. Trained female cyclists demonstrated EIAH to the same degree as trained male cyclists and that some individual untrained females who also exhibited EIAH [
97,
98]. On the other hand, other studies have shown that athletes training for endurance sports can produce arterial blood desaturation during exercise at sea level [
88,
99,
100]. These observations support the idea that, among the limiting factors of maximal oxygen uptake, in addition to the arteriovenous difference,
A-
, the role of hemoglobin oxygen saturation should be considered.
Other studies describe a
decrease at maximum effort and an apparent increase in the desaturation time,
, proportional to the
[
49,
60,
101]. For example, the highest
values reported in trained subjects were obtained in individuals engaged in endurance modalities with values above 75 mL/kg/min [
102]. However, values below 65 mL/kg/min for females are easily detected in high-level athletes in endurance competitions, while sedentary female subjects are closer to values of 40 mL/kg/min. These data are broadly coincident with those reported in our study, in which
sorted the physical condition of the athletes. Besides, regarding the maximum HR reached during the test, we found a difference from our study with a mean value of (189.81 ± 8.54) bpm (ranging from 168 to 205 bpm) when compared with the results of Yoshiga and Higuchi [
89], who obtained a mean value of (196 ± 8) bpm or Lauresen et al. who measured a mean of (199 ± 5) bmp [
103]. This difference can be associated with our sample being competitive athletes, who have a lower HR due to adaptations that exercise produces on the cardiovascular system.
In this framework, pulse oximetry is an appropriate method for determining the limit of cardiopulmonary stress in exercise testing characterized by a significant drop in oxygen saturation value [
63,
68,
104,
105]. Therefore, its application may be extended to the medical clinic to continuously monitor arterial blood oxygenation during exertion in people with known diseases [
106,
107,
108,
109,
110] and at high altitudes [
39,
111,
112,
113,
114,
115].
4.1. Analysis of Correlations between Stress Test and Transcutaneous Oximetry
Correlations were sought for the different time events of the effort test with the variables from ergospirometry and anthropometric variables such as age, height, weight, BMI, basal
,
, and maximum HR as shown in
Table 4. We only found a statistically significant Pearson correlation concerning the
between the different times. Furthermore, when comparing the same time events with respect to the skin pigmentation, physical fitness condition, and type of practiced sport variables (see
Table 5), we found correlations for the physical fitness condition, classified based on the
. In the case of the desaturation time,
, and the total test time,
, we found that the better the physical condition, the longer it takes to reach desaturation and the longer the total test time. When comparing the three levels of physical fitness, significant differences were observed between the medium and good level and the medium and excellent, with no differences between the good and excellent.
Regarding correlations between the anthropometric variables, although some studies have found a weak negative correlation for BMI and
[
116,
117] in healthy adults, other studies performed in healthy boys did not find any significant correlations [
118]. Our results do not show any correlations with BMI, or any other anthropometric variable as size, weight or age as it is shown in
Table 4.
4.2. Analysis of Correlations between the Time of Occurrence of Oxygen Desaturation, , and the Appearance of the Aerobic and Anaerobic Thresholds, and
A common tendency in the
evolution during the effort test characterized by two drops before and after the AeT was observed in all athletes was observed. These findings agree with some other authors’ observations who found equivalent oxygen desaturation in males with
mL/kg/min and females with
with 40–55 mL/kg/min [
31,
32]. In our case, we observed a maximum of
desaturations in all-female athletes with a
ranged from 37 to 64 mL/kg/min.
Table 4 shows a Pearson coefficient of 0.469 between the
and the AeT appearance. We also compared the AeT appearance time with the skin pigmentation, the type of practiced sport (aerobic, anaerobic, or mixed), and the physical fitness condition. Statistical significance was only found when comparing the different levels of physical fitness condition based on the maximum oxygen uptake, as shown in
Table 5.
To study the
variations as a factor associated with the appearance of the AeT we analyzed the time to observe the first
drop before the AeT,
, and the time from reaching this minimum value until the AeT appearance,
(see
Figure 4). A possible relationship between these two times and the AeT appearance was sought by calculating Pearson’s linear correlation coefficient and linear regression. No correlations were found between
and
with the AeT appearance. However, we found a negative correlation between
and
with a Pearson’s coefficient of −0.789, with
decreasing as
increases by
, as shown in
Figure 6.
Few studies have made comparisons between the AeT appearance and its relationship with oxygen saturation. For example, Gaston et al. investigate the impact of EIAH developed at sea level on exercise responses at moderate acute altitude in biathletes [
99] based on the continuous monitoring of
,
, and
. Besides, the occurrence of EIAH at sea level was associated with specific muscle and cerebral oxygenation responses to exercise under both normoxia and moderate hypoxia in [
111], but a relationship with the AeT was not established.
Furthermore, we also studied
variations as a factor associated with the AnT appearance and the times
and
by calculating Pearson’s linear correlation coefficient and linear regression. We found a weak correlation with
showing a Pearson coefficient of 0.383. However, the most significant result was obtained when correlating the AnT appearance time (
+
+
+
) with the desaturation time (
+
+
), with a statistically significant Pearson correlation of 0.892. Panel a of
Figure 7 shows the regression model between these two times fitted by the line
with a coefficient of determination of
. Hence, it can be prophesied that for every minute that desaturation takes to appear, the AnT takes 0.81 min to appear.
A statistically significant Pearson correlation of 0.671 was found between AnT and the maximal oxygen uptake,
, as shown in
Table 4. This correlation seems logical, clearly explaining that an athlete with a better physical condition (higher
) takes longer to reach the AnT. Furthermore, regarding
Table 5, we also found correlations between AnT and the skin pigmentation variable. We found we found that dark-skinned athletes took an average of 1 min 46 s longer to reach the AnT. This difference may be attributed to dark-skinned female athletes were in better physical condition than light-skinned female athletes. However, these results are not representative since the sample size of dark-skinned female athletes was relatively small (
N = 2).
In summary, concerning the influence on the appearance of the AnT, it seems clear that desaturation time plays an important role. We also found a weak correlation with
, which agrees with the study of Nikooie et al. who found statistically significant correlations between the desaturation time,
, and the appearance of the AnT or
[
119].
5. Conclusions
Transcutaneous oximetry during physical exertion allows more generalized and frequent monitoring of oxygen saturation evolution at peripheral level and the physical performance evaluation of the athletes. This evaluation can be perfectly adapted to the characteristics of each sport, obtaining broad correlations with maximum oxygen uptake. Our results reaffirm the importance of the use of pulse oximetry as an appropriate method for determining the limit of cardiopulmonary stress, characterized by a significant drop in oxygen saturation values.
We observed a common behavior of the transcutaneous oxygen saturation evolution during the incremental exercise test in all female athletes. First, a
decrease before the AeT followed by a second significant drop between the AeT and the AnT. Statistically significant correlations were found between the ergospirometry measured variables obtained from the stress test and the different time events related to the saturation drops.
Table 8 summarizes the most statistically significant correlations found in this study. The maximum oxygen uptake,
, is the variable that presented the most independent correlations with each time event. However, there is no evidence of a relationship between a higher decrease in oxygen saturation with the
, which seems to indicate that the athlete’s physical fitness condition does not depend on the magnitude of the oxygen desaturation, but instead with the time to reach the maximum desaturation,
.
Correlations were found between the times related to the AeT or first ventilatory threshold, and , with a linear dependence given by . Besides, the times related to the AnT or second ventilatory threshold, and , were also correlated following a linear relationship fitted by .
The highest correlations were found between the desaturation time,
, and the appearance of the AnT. The linear regression model of the
with the AnT appearance time in female athletes predicts that for every minute that desaturation takes to appear, the AnT takes 0.81 min (
) and predicts the
of the values (
), as shown in
Figure 7. This result is of great interest because it indicates the oxygen saturation value as an indicator with future potential in determining the second ventilatory threshold,
. Besides, the AnT appearance is also correlated with the physical condition level, which suggests that the physiological cause of the oxygen decrease saturation in female athletes is the level of the physical fitness condition. Therefore, it should not represent a limiting factor of physical performance in women. Despite increasing evidence in sex-based differences in respiratory physiology, a holistic understanding of the impact on the respiratory response to exercise remains incomplete and research in a more heterogeneous population is required.

 ,
, 







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}