


Comparison of the Trueness of Complete Dentures Fabricated Using Liquid Crystal Display 3D Printing According to Build Angle and Natural Light Exposure




Abstract
1. Introduction
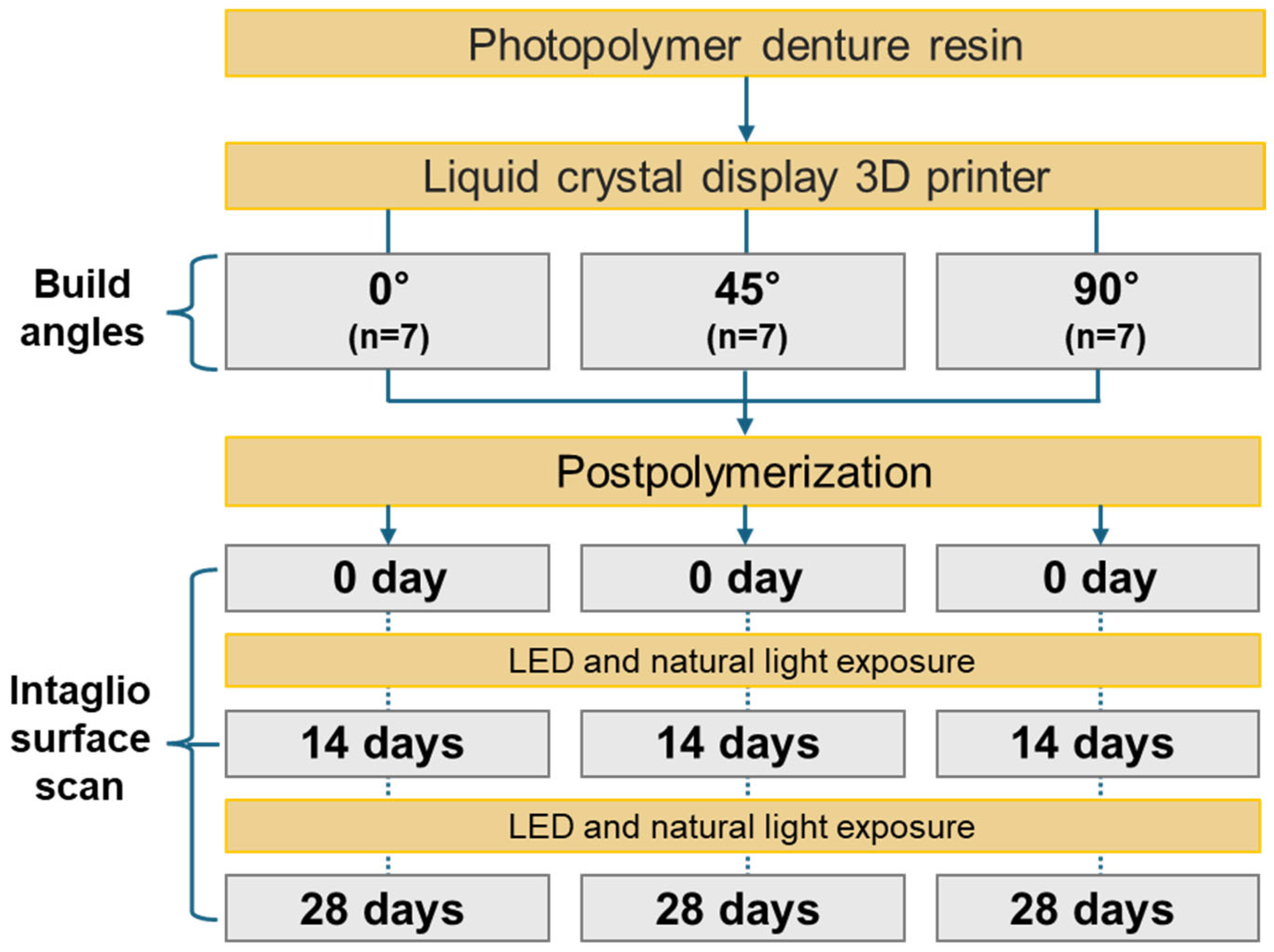
2. Materials and Methods
3. Results
3.1. Effect of Build Angle on the Intaglio Surface Trueness of Complete Dentures
3.2. Effect of Natural Light Exposure Duration on Intaglio Surface Trueness
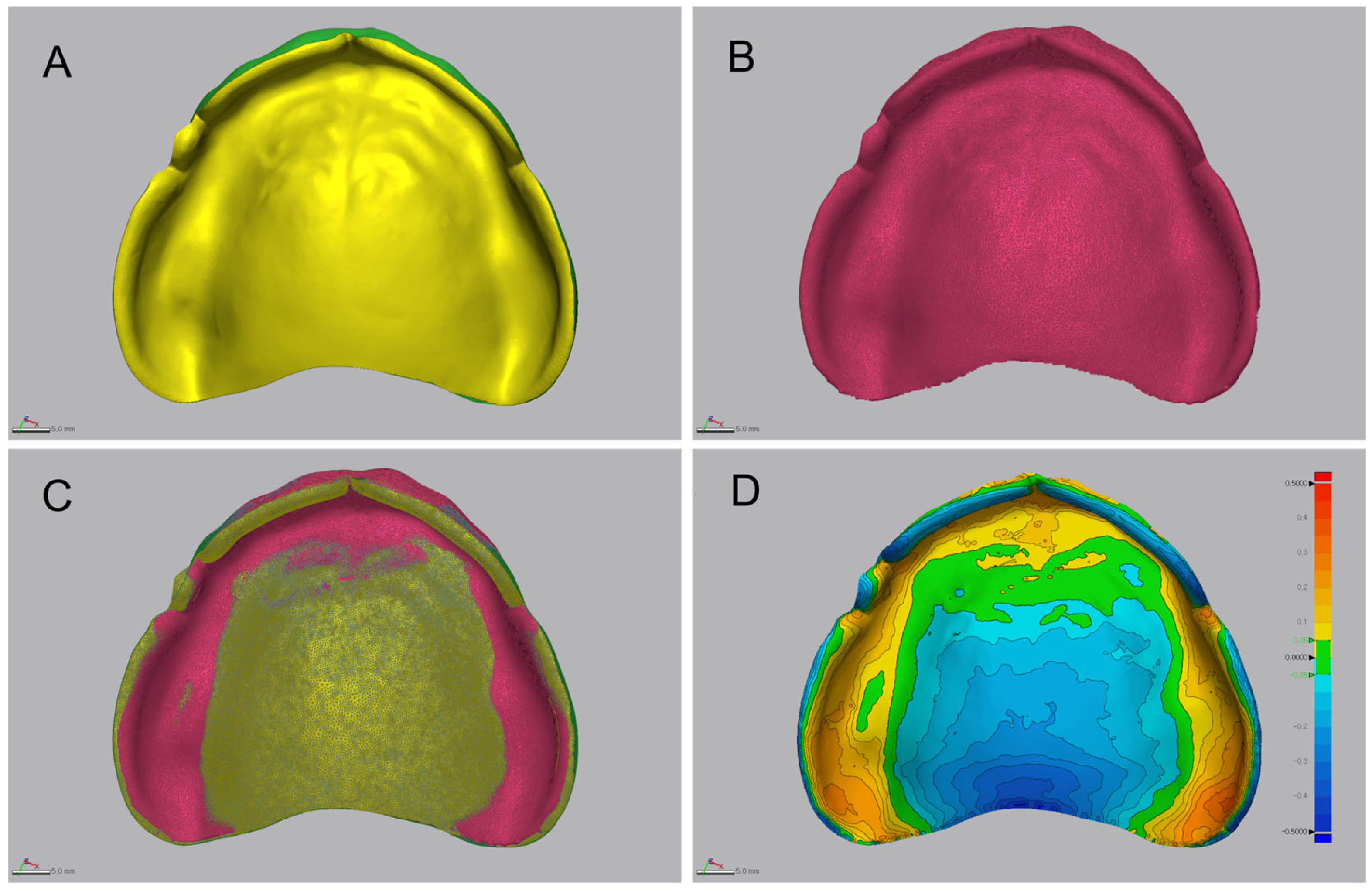
3.3. Qualitative 3D Deviation Map Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Özden, Y.; Uygun, L.A. Effects of post-curing times on the trueness of 3D printed dental inlays made with permanent resins. Clin. Oral Investig. 2025, 29, 244. [Google Scholar] [CrossRef]
- Yoon, J.Y.; Nam, Y.S.; Kim, H.Y.; Lee, S.J.; Huh, J.B.; Lee, K.D. Evaluation of dimensional changes during post-curing of 3D-printed denture bases. Appl. Sci. 2021, 11, 10000. [Google Scholar]
- Nulty, A.B.; Zeitounlouian, A.; Zeltner, M.; Wismeijer, D. A comparison of trueness and precision of 12 3D printers used in dentistry: Build-angle recommendations. BDJ Open 2022, 8, 7. [Google Scholar] [CrossRef]
- Temizci, T.; Kölüş, T. Effects of printing angle and post-curing time on the color and translucency of 3D-printed temporary restoration. Biomimetics 2024, 9, 420. [Google Scholar] [CrossRef]
- Dawood, A.; Marti Marti, B.; Sauret-Jackson, V.; Darwood, A. 3D printing in dentistry. Br. Dent. J. 2015, 219, 521–529. [Google Scholar] [CrossRef]
- Bidra, A.S.; Taylor, T.D.; Agar, J.R. Computer-aided technology for fabricating complete dentures: Systematic review. J. Prosthet. Dent. 2013, 109, 361–366. [Google Scholar] [CrossRef]
- Alhallak, K.; Hagi-Pavli, E.; Nankali, A. A review on clinical use of CAD/CAM and 3D printed dentures. Br. Dent. J. 2023, 235, 215–222. [Google Scholar] [CrossRef]
- Alotaibi, H.N. Patient satisfaction with CAD/CAM 3D-printed complete dentures: A systematic analysis. Healthcare 2025, 13, 388. [Google Scholar] [CrossRef]
- Anadioti, E.; Musharbash, L.; Blatz, M.B.; Papavasiliou, G.; Kamposiora, P. 3D printed complete removable dental prostheses: A narrative review. BMC Oral Health 2020, 20, 343. [Google Scholar] [CrossRef]
- Baba, N.Z.; Goodacre, B.J.; Goodacre, C.J.; Müller, F.; Wagner, S. CAD/CAM complete denture systems and physical properties: A review of the literature. J. Prosthodont. 2021, 30, 113–124. [Google Scholar] [CrossRef]
- Unkovskiy, A.; Schmidt, F.; Beuer, F.; Spintzyk, S.; Kraemer-Fernandez, P. Stereolithography vs. direct light processing for rapid manufacturing of complete denture bases: An in vitro accuracy analysis. J. Clin. Med. 2021, 10, 1070. [Google Scholar] [CrossRef]
- Alqutaibi, A.Y.; Aljohani, R.; Almuzaini, S.; Alghauli, M.A. Physical–mechanical properties and accuracy of additively manufactured resin denture bases: Impact of printing orientation. J. Prosthodont. Res. 2025, in press. [Google Scholar] [CrossRef]
- Kim, K.W.; Kim, S.Y.; Kim, S.-A.; Jang, H.-W.; Lee, K.-W.; Lee, Y.-S. Four different build angles in 3D-printed complete denture bases: A comparative in vitro study. Appl. Sci. 2024, 14, 8504. [Google Scholar] [CrossRef]
- Shan, Y.; Zhou, J.-L.; Zhang, R.-J.; Tan, F.-B. Evaluation of the influence of different build angles on the surface characteristics, accuracy, and dimensional stability of the complete denture base printed by digital light processing. Heliyon 2024, 10, e24095. [Google Scholar]
- ISO 5725-1; Accuracy (Trueness and Precision) of Measurement Methods and Results—Part 1: General Principles and Definitions. International standard ISO: Geneva, Switzerland, 1994.
- Park, G.S.; Kim, S.K.; Heo, S.J.; Koak, J.Y.; Seo, D.G. Effects of printing parameters on the fit of implant-supported 3D resin prosthetics. Materials 2019, 12, 2533. [Google Scholar] [CrossRef]
- García, N.; Gómez-Polo, M.; Fernández, M.; Antonaya-Martín, J.L.; Ortega, R.; Gómez-Polo, C.; Revilla-León, M.; Cascos, R. Influence of printing angulation on the accuracy (trueness and precision) of the position of implant analogs in 3D models: An in vitro pilot study. Appl. Sci. 2024, 14, 2966. [Google Scholar] [CrossRef]
- Hada, T.; Kanazawa, M.; Iwaki, M.; Arakida, T.; Soeda, Y.; Katheng, A.; Otake, R.; Minakuchi, S. Effect of printing direction on accuracy of SLA-printed dentures. Materials 2020, 13, 3405. [Google Scholar] [CrossRef]
- Yoshidome, K.; Torii, M.; Kawamura, N.; Shimpo, H.; Ohkubo, C. Trueness and fitting accuracy of maxillary 3D-printed complete dentures. J. Prosthodont. Res. 2021, 65, 559–564. [Google Scholar] [CrossRef]
- Ibrahim, I.A.; Najm, H.; Alharbi, N. Comparison of trueness and precision of 3D-printed dental crowns using LCD and DLP technologies. J. Prosthodont. 2022, 31, 123–130. [Google Scholar]
- Demirel, M.; Türksayar, A.A.; Donmez, M.B.; Yilmaz, B. Effects of post-curing time on trueness of 3D-printed dental inlays. Dent. Mater. J. 2025, 44, 132–140. [Google Scholar]
- Chaiamornsup, P.; Katheng, A.; Ha, R.; Tsuchida, Y.; Kanazawa, M.; Uo, M.; Minakuchi, S.; Suzuki, T.; Takahashi, H. Effects of build orientation and bar addition on accuracy of complete denture base fabricated with digital light projection: An in vitro study. J. Prosthodont. Res. 2023, 67, 641–646. [Google Scholar] [CrossRef]
- Ko, J.; Bloomstein, R.D.; Briss, D.; Holland, J.N.; Morsy, H.M.; Kasper, F.K.; Huang, W. Effect of build angle and layer height on the accuracy of 3-dimensional printed dental models. Am. J. Orthod. Dentofac. Orthop. 2021, 160, 451–458. [Google Scholar] [CrossRef]
- Lohfeld, S.; Belnap, B.; Retrouvey, J.-M.; Walker, M.P. Effect of model body type and print angle on the accuracy of 3D-printed orthodontic models. Biomimetics 2024, 9, 217. [Google Scholar] [CrossRef]
- Khorsandi, D.; Fahimipour, A.; Abasian, P.; Saber, S.S.; Seyedi, M.; Ghanavati, S.; Ahmad, A.; de Stephanis, A.A.; Taghavinezhaddilami, F.; Leonova, A.; et al. 3D and 4D printing in dentistry and maxillofacial surgery: Printing techniques, materials, and applications. Acta Biomater. 2021, 122, 26–49. [Google Scholar] [CrossRef]
- Alghauli, M.; Alqutaibi, A.Y.; Wille, S.; Kern, M. Clinical outcomes and influence of material parameters on the behavior and survival rate of thin and ultrathin occlusal veneers: A systematic review. J. Prosthodont. Res. 2023, 67, 45–54. [Google Scholar] [CrossRef]
- Faggion, C.M., Jr. Guidelines for reporting pre-clinical in vitro studies on dental materials. J. Evid. Based Dent. Pract. 2012, 12, 182–189. [Google Scholar] [CrossRef]
- Lo Russo, L.; Guida, L.; Zhurakivska, K.; Troiano, G.; Chochlidakis, K.; Ercoli, C. Intaglio surface trueness of milled and 3D-printed digital maxillary and mandibular dentures: A clinical study. J. Prosthet. Dent. 2023, 129, 131–139. [Google Scholar] [CrossRef]
- Tongkitcharoen, N.; Manopattanakul, S.; Boonpratham, S.; Santiwong, P.; Viwattanatipa, N. Comparison of dimensional accuracy of 3D-printed models for clear aligners among various orientation types and hollow types. Clin. Investig. Orthod. 2023, 82, 177–193. [Google Scholar] [CrossRef]
- Subbaiah, N.K.; Chaudhari, P.K.; Duggal, R.; Samrit, V.D. Effect of print orientation on the dimensional accuracy and cost-effectiveness of rapid-prototyped dental models using a PolyJet photopolymerization printer: An in vitro study. Int. Orthod. 2024, 22, 100902. [Google Scholar] [CrossRef]
- Negm, E.E.; Aboutaleb, F.A.; Alam-Eldein, A.M. Virtual evaluation of the accuracy of fit and trueness in maxillary poly(etheretherketone) removable partial denture frameworks fabricated by direct and indirect CAD/CAM techniques. J. Prosthodont. 2019, 28, 804–810. [Google Scholar] [CrossRef]
- Song, S.; Zhang, J.; Liu, M.; Li, F.; Bai, S. Effect of build orientation and layer thickness on manufacturing accuracy, printing time, and material consumption of 3D-printed complete denture bases. J. Dent. 2023, 130, 104435. [Google Scholar] [CrossRef]
- Jin, M.C.; Yoon, H.I.; Yeo, I.S.; Kim, S.H.; Han, J.S. The effect of build angle on the tissue surface adaptation of maxillary and mandibular complete denture bases manufactured by digital light processing. J. Prosthet. Dent. 2020, 123, 473–482. [Google Scholar] [CrossRef]
- You, S.M.; You, S.G.; Kang, S.Y.; Bae, S.Y.; Kim, J.H. Evaluation of the accuracy (trueness and precision) of a maxillary trial denture according to the layer thickness: An in vitro study. J. Prosthet. Dent. 2021, 125, 139–145. [Google Scholar] [CrossRef]
- Lee, W.J.; Jo, Y.H.; Yilmaz, B.; Yoon, H.I. Effect of layer thickness, build angle, and viscosity on the mechanical properties and manufacturing trueness of denture base resin for digital light processing. J. Dent. 2023, 135, 104598. [Google Scholar] [CrossRef]
- Cameron, A.B.; Evans, J.L.; Abuzar, M.A.; Tadakamadla, S.K.; Love, R.M. Trueness assessment of additively manufactured maxillary complete denture bases produced at different orientations. J. Prosthet. Dent. 2024, 131, 129–135. [Google Scholar] [CrossRef]
- Morel, L.L.; Almeida, M.V.R.; Santos, K.M.D.; Praseres, M.F.; Gonçalves Girundi, A.L.; Alexandrino, L.D.; Silva, W.J.D. Reinforcement of 3D-printed resins for denture base by adding aramid fibers: Effect on mechanical, surface, and optical properties. J. Prosthodont. 2024, 33, 324–333. [Google Scholar] [CrossRef] [PubMed]
- Benfaida, S.; Hamza, M.; Benabdelaziz, A.; Jouhadi, E.M. The impact of post-processing procedures on the characteristics of additively manufactured resins: A systematic review. Open Access Libr. J. 2024, 11, e11632. [Google Scholar] [CrossRef]
- Kim, J.; Lee, D.H. Influence of the postcuring process on dimensional accuracy and seating of 3D-printed polymeric fixed prostheses. Biomed. Res. Int. 2020, 2020, 7683121. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.H.; Lee, J.E.; Kim, H.; Dong, J.H.; Kim, Y.H. Evaluation of dimensional changes according to aging period and post-curing time of 3D-printed denture base prostheses: An in vitro study. Materials 2021, 14, 6185. [Google Scholar] [CrossRef]
- ISO 12836:2015; Dentistry—Digitizing devices for CAD/CAM systems for indirect dental restorations—Test methods for assessing accuracy. International Organization for Standardization (ISO): Geneva, Switzerland, 2015.
- Charoenphol, K.; Peampring, C. Fit accuracy of complete denture base fabricated by CAD/CAM milling and 3D-printing methods. Eur. J. Dent. 2023, 17, 889–894. [Google Scholar] [CrossRef]
- Tsai, F.C.; Yang, T.C.; Wang, T.M.; Lin, L.D. Dimensional changes of complete dentures fabricated by milled and printed techniques: An in vitro study. J. Prosthet. Dent. 2023, 129, 608–615. [Google Scholar] [CrossRef] [PubMed]
- Venkatesh, S.B.; Nayak, V.M.; Sulaya, K.; Shetty, S.S. A comparative evaluation of retention of record bases fabricated digitally in various types of posterior palatal seal area. J. Oral Biol. Craniofac. Res. 2025, 15, 11–15. [Google Scholar] [CrossRef]
- Hwang, H.J.; Lee, S.J.; Park, E.J.; Yoon, H.I. Assessment of the trueness and tissue surface adaptation of CAD-CAM maxillary denture bases manufactured using digital light processing. J. Prosthet. Dent. 2019, 121, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Casey, D.M. Interim complete immediate dentures for a patient wearing removable partial dentures. J. Prosthet. Dent. 1978, 39, 466–468. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Item | Specification |
|---|---|---|
| 3D printer | Device | Lilivis Print (Huvitz) |
| Printing type | Adaptive MSLA | |
| Light source (printer) | 405 nm | |
| Pixel size (X/Y) | 50 µm | |
| Curing unit | Light source | 395 nm UV LED |
| LED output power | 280 W | |
| Material | Material name | Tera Harz Denture (Graphy) |
| Lot number | 1-EB07D02048/1-EE01D02065 | |
| Scanner | Model | E1 (3Shape) |
| Software | 3Shape Dental System, version 17.3.0 | |
| Printing parameters | Layer thickness | 100 µm |
| Bottom layer count | 5 | |
| Transition layer count | 10 | |
| Bottom exposure time | 10 s | |
| Bottom lift distance | 5 mm | |
| Bottom lift speed | 200 mm/min | |
| Bottom retract speed | 150 mm/min | |
| Bottom light intensity | 75% | |
| Normal exposure time | 2 s | |
| Normal lift distance | 5 mm | |
| Normal lift speed | 80 mm/min | |
| Normal retract speed | 150 mm/min | |
| Normal light intensity | 40% | |
| Rest time before lift | 0 s | |
| Rest time after lift | 0 s |
| Measurement Value | Build Angle | Mean | SD | 95% Confidence Interval | Minimum | Maximum | F | p | |
|---|---|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||||
| RMS value (mm) | 0° | 0.197 A | 0.018 | 0.1809 | 0.2146 | 0.17 | 0.23 | 11.400 | 0.001 * |
| 45° | 0.174 B | 0.012 | 0.1628 | 0.1853 | 0.15 | 0.19 | |||
| 90° | 0.163 B | 0.010 | 0.1537 | 0.1723 | 0.15 | 0.18 | |||
| Positive mean value (mm) | 0° | 0.190 A | 0.017 | 0.1749 | 0.2067 | 0.17 | 0.22 | 46.507 | <0.001 * |
| 45° | 0.142 B | 0.008 | 0.1347 | 0.1503 | 0.13 | 0.16 | |||
| 90° | 0.136 B | 0.006 | 0.1306 | 0.1417 | 0.13 | 0.14 | |||
| Negative mean value (mm) | 0° | −0.059 A | 0.005 | −0.0636 | −0.0543 | −0.06 | −0.05 | 119.162 | <0.001 * |
| 45° | −0.1258 B | 0.010 | −0.1358 | −0.1158 | −0.14 | −0.1 | |||
| 90° | −0.1343 B | 0.012 | −0.1459 | −0.1227 | −0.16 | −0.12 | |||
| Tolerance (%) | 0° | 87.291 A | 2.521 | 84.9593 | 89.6241 | 82.54 | 90.32 | 27.423 | <0.001 * |
| 45° | 89.978 A | 2.218 | 87.9263 | 92.0304 | 86.37 | 93.7 | |||
| 90° | 95.326 B | 1.235 | 94.1832 | 96.469 | 92.89 | 96.76 | |||
| Build Angle | Comparison | Measurement Value | t | p |
|---|---|---|---|---|
| 0° | Day 0 vs. day 14 | RMS value | −3.591 | 0.011 * |
| Positive mean value | −5.295 | 0.002 * | ||
| Negative mean value | 2.882 | 0.028 * | ||
| Tolerance | 0.624 | 0.556 | ||
| Day 14 vs. day 30 | RMS value | −1.873 | 0.110 | |
| Positive mean value | −4.062 | 0.007 * | ||
| Negative mean value | −1.036 | 0.340 | ||
| Tolerance | 1.713 | 0.138 | ||
| 45° | Day 0 vs. day 14 | RMS value | −3.575 | 0.012 * |
| Positive mean value | −2.705 | 0.035 * | ||
| Negative mean value | 2.092 | 0.081 | ||
| Tolerance | 3.177 | 0.019 * | ||
| Day 14 vs. day 30 | RMS value | −3.981 | 0.007 * | |
| Positive mean value | −4.251 | 0.005 * | ||
| Negative mean value | −0.327 | 0.755 | ||
| Tolerance | 2.146 | 0.076 | ||
| 90° | Day 0 vs. day 14 | RMS value | −0.404 | 0.700 |
| Positive mean value | 2.653 | 0.038 * | ||
| Negative mean value | 2.176 | 0.073 | ||
| Tolerance | 1.12 | 0.305 | ||
| Day 14 vs. day 30 | RMS value | 2.544 | 0.044 * | |
| Positive mean value | 1.995 | 0.093 | ||
| Negative mean value | −0.391 | 0.709 | ||
| Tolerance | −2.167 | 0.073 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.; Son, K.; Kim, S.-Y.; Lee, K.-B. Comparison of the Trueness of Complete Dentures Fabricated Using Liquid Crystal Display 3D Printing According to Build Angle and Natural Light Exposure. J. Funct. Biomater. 2025, 16, 277. https://doi.org/10.3390/jfb16080277
Kim H, Son K, Kim S-Y, Lee K-B. Comparison of the Trueness of Complete Dentures Fabricated Using Liquid Crystal Display 3D Printing According to Build Angle and Natural Light Exposure. Journal of Functional Biomaterials. 2025; 16(8):277. https://doi.org/10.3390/jfb16080277
Chicago/Turabian StyleKim, Haeri, KeunBaDa Son, So-Yeun Kim, and Kyu-Bok Lee. 2025. "Comparison of the Trueness of Complete Dentures Fabricated Using Liquid Crystal Display 3D Printing According to Build Angle and Natural Light Exposure" Journal of Functional Biomaterials 16, no. 8: 277. https://doi.org/10.3390/jfb16080277
APA StyleKim, H., Son, K., Kim, S.-Y., & Lee, K.-B. (2025). Comparison of the Trueness of Complete Dentures Fabricated Using Liquid Crystal Display 3D Printing According to Build Angle and Natural Light Exposure. Journal of Functional Biomaterials, 16(8), 277. https://doi.org/10.3390/jfb16080277