
Wharton’s Jelly Bioscaffolds Improve Cardiac Repair with Bone Marrow Mononuclear Stem Cells in Rats

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Animals and Treatment
2.2. Preparation of Acellular Wharton’s Jelly (WJ)
2.3. Wharton’s Jelly (WJ) Harvesting Stem Cells and Isolation of Bone Marrow Stem Cells (BMMC)
2.4. BMMC Transplantation and WJ Implantation
2.5. Tissue Microarray (TMA) and Immunohistochemistry (IHC) Flow Cytometry
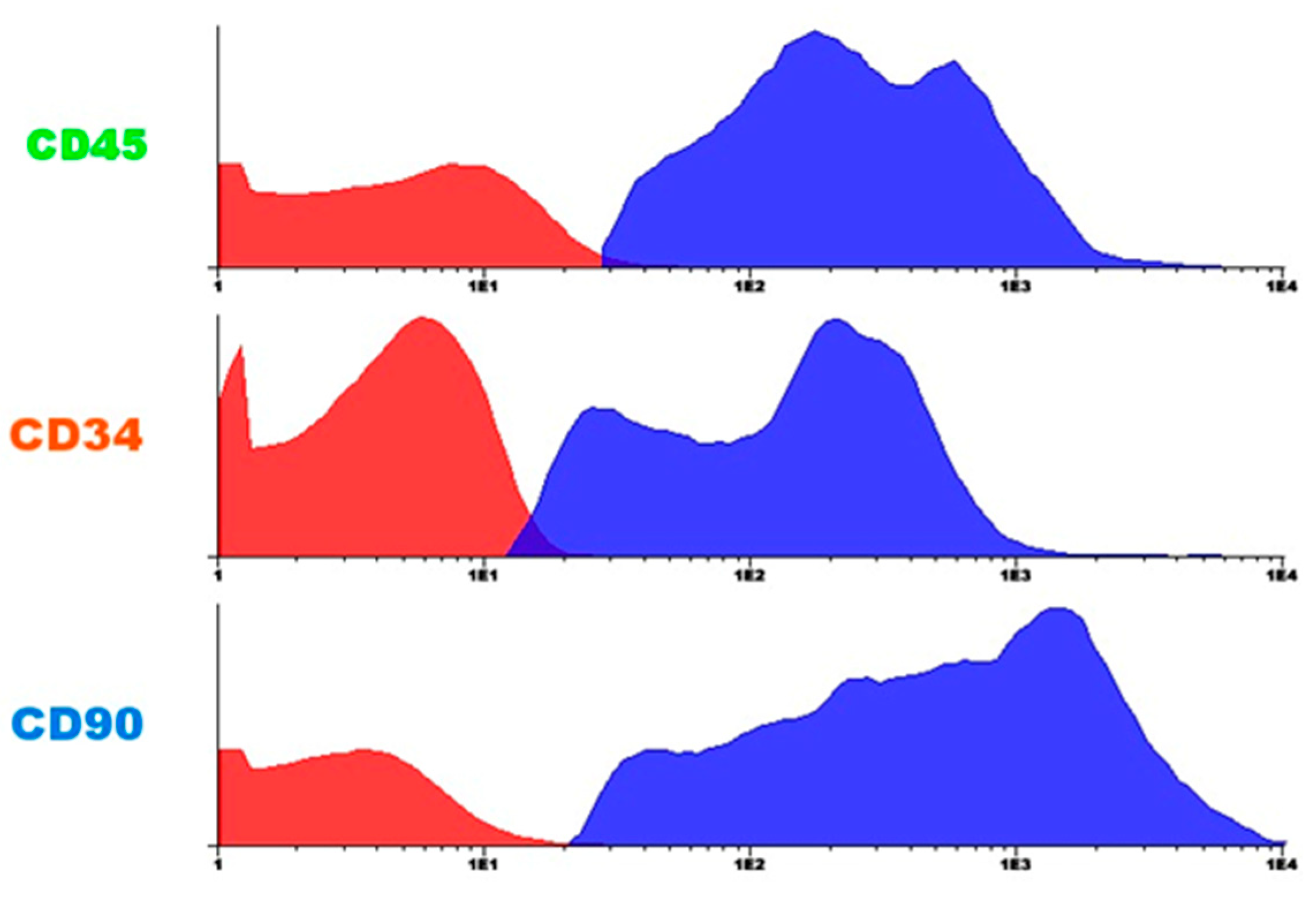
2.6. Flow Cytometry
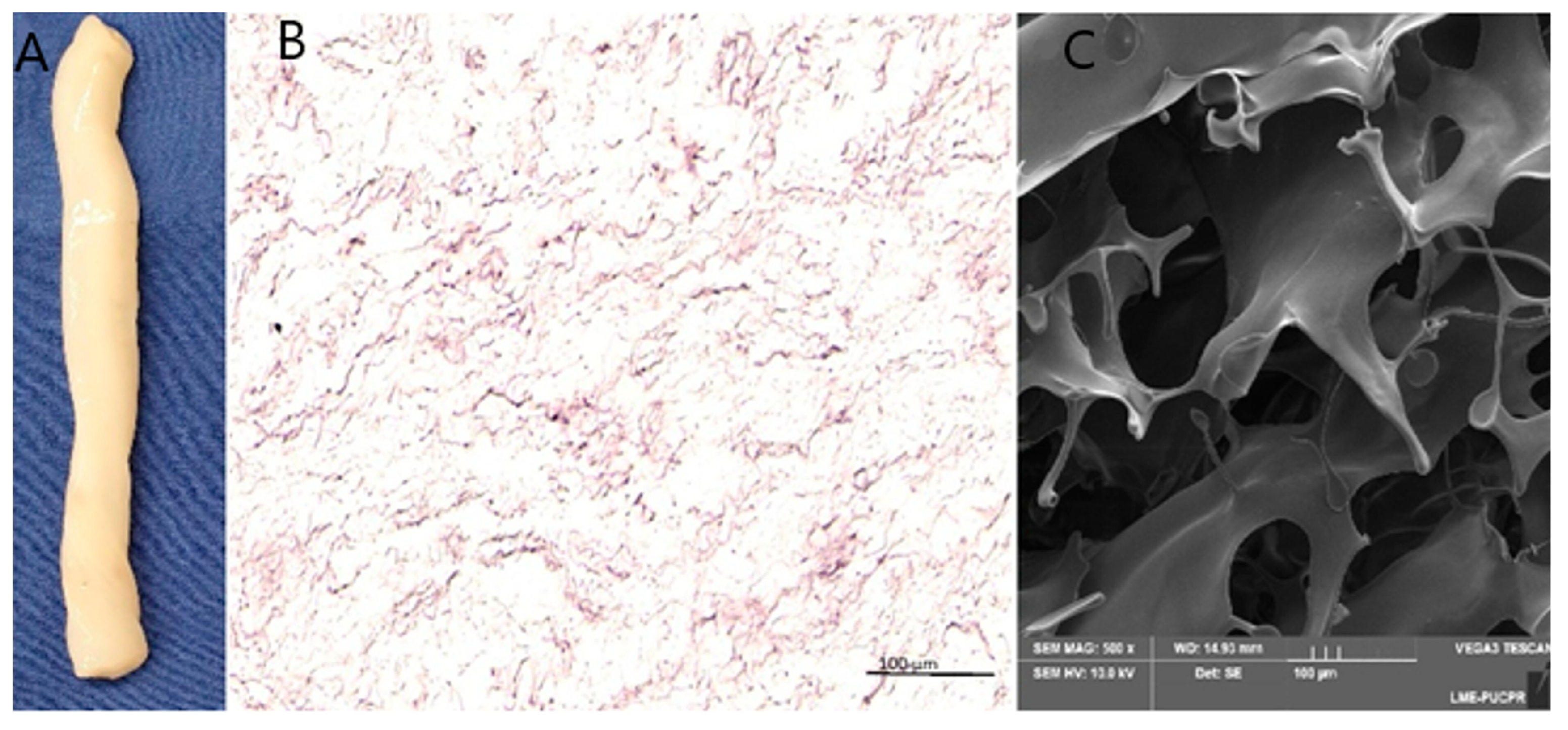
2.7. Scanning Electron Microscopy
2.8. Statistical Analysis
3. Results
3.1. Tissue Characterization
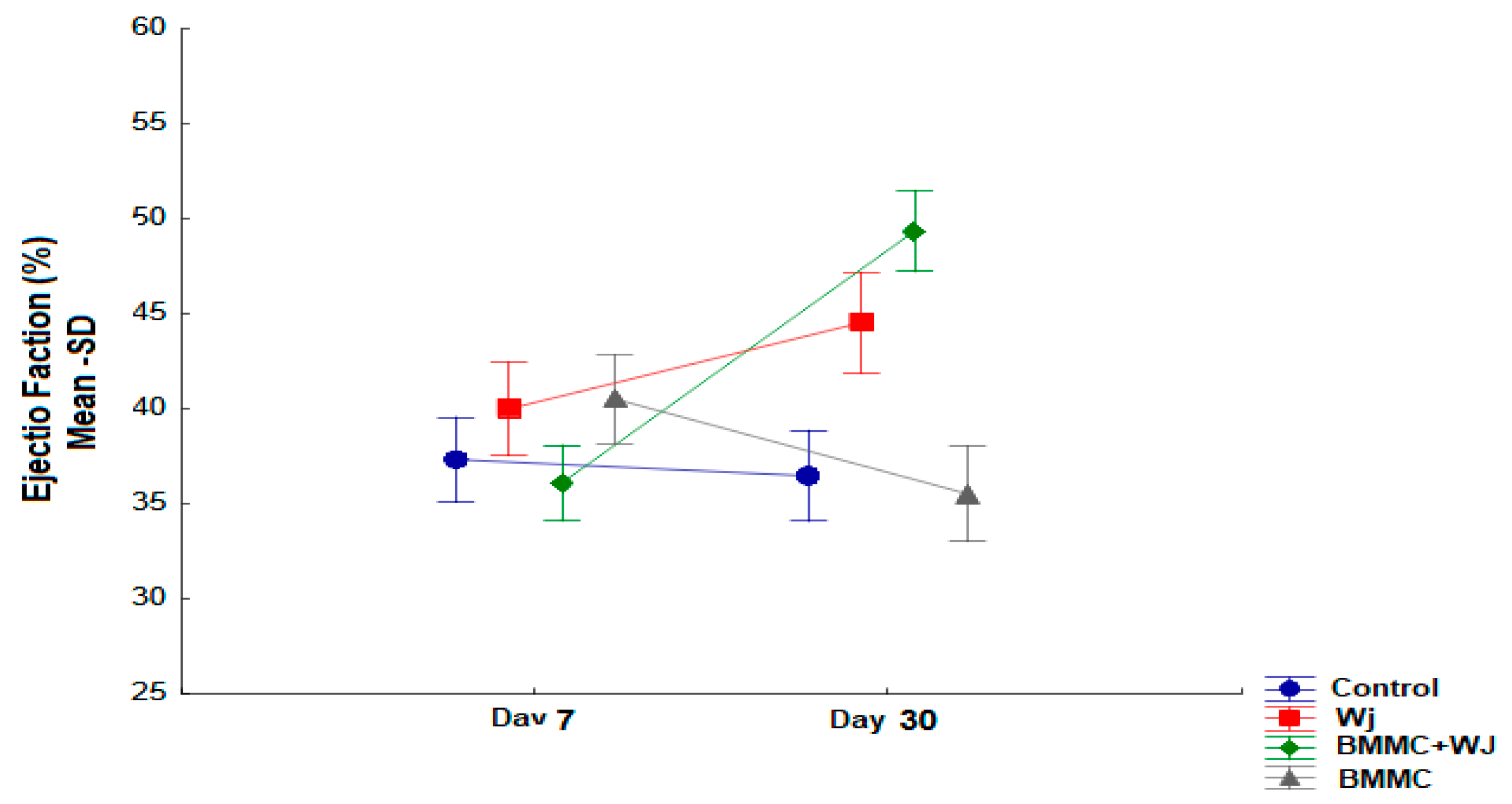
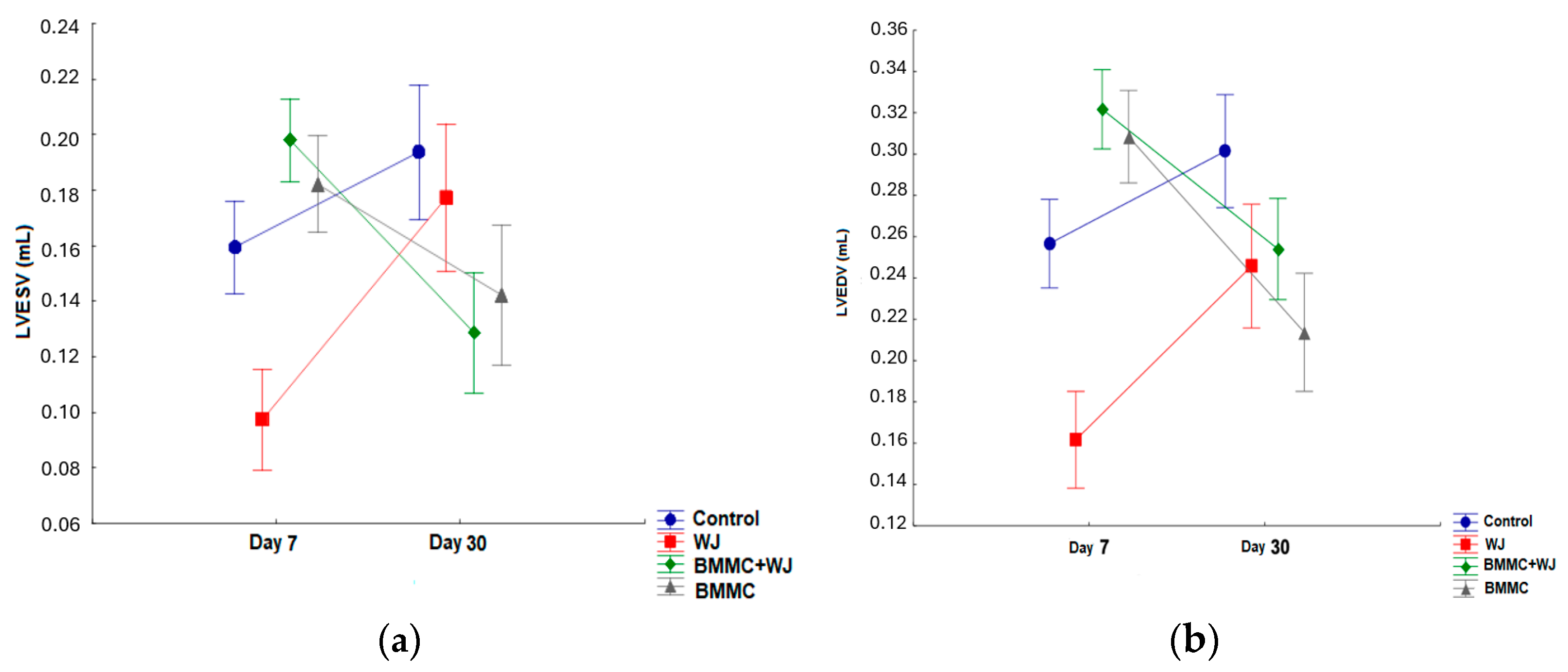
3.1.1. Results of Cardiac Function Test—Inter-Group Evaluation
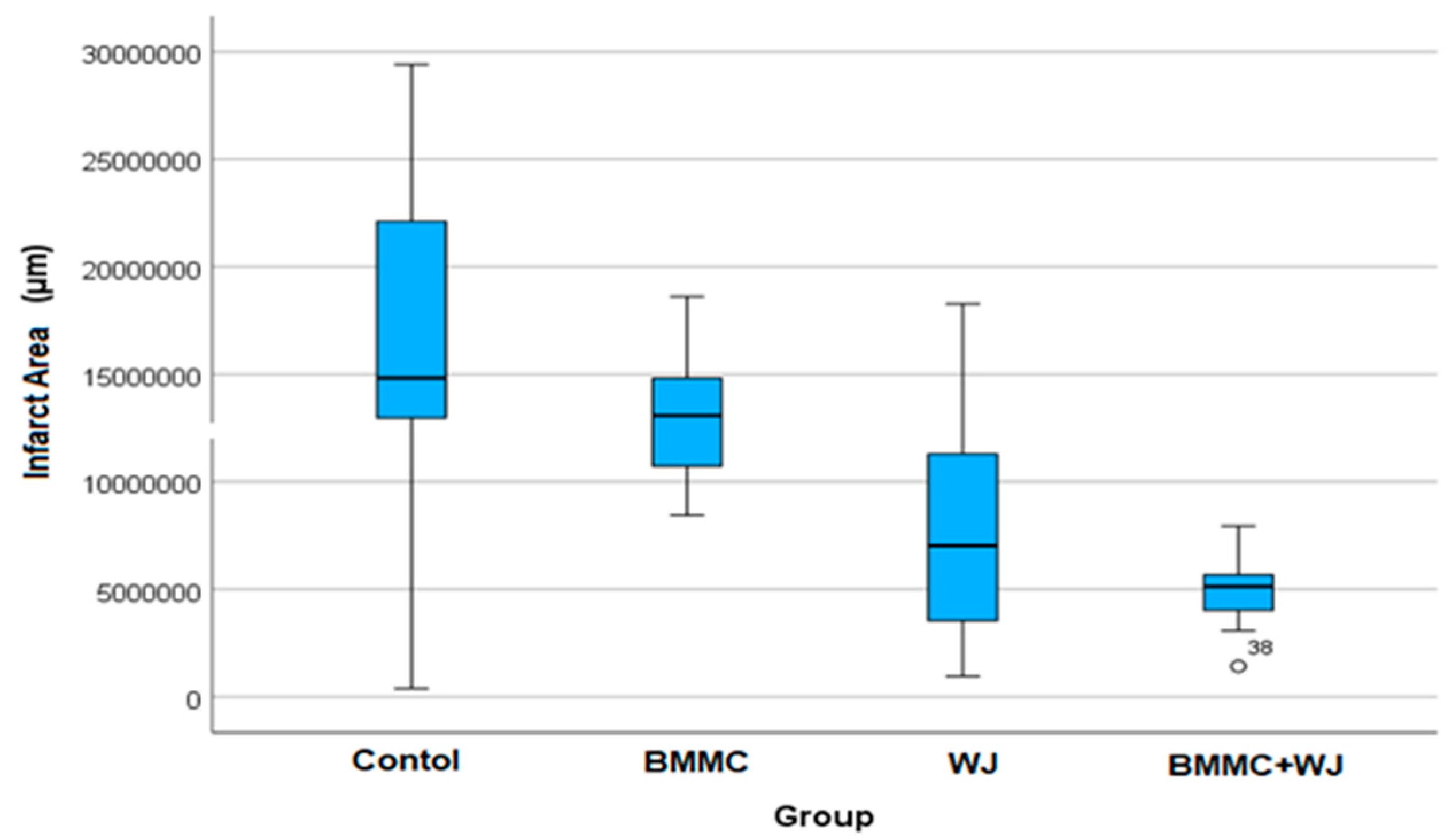
Analysis of Collagen Levels and Infarct Area
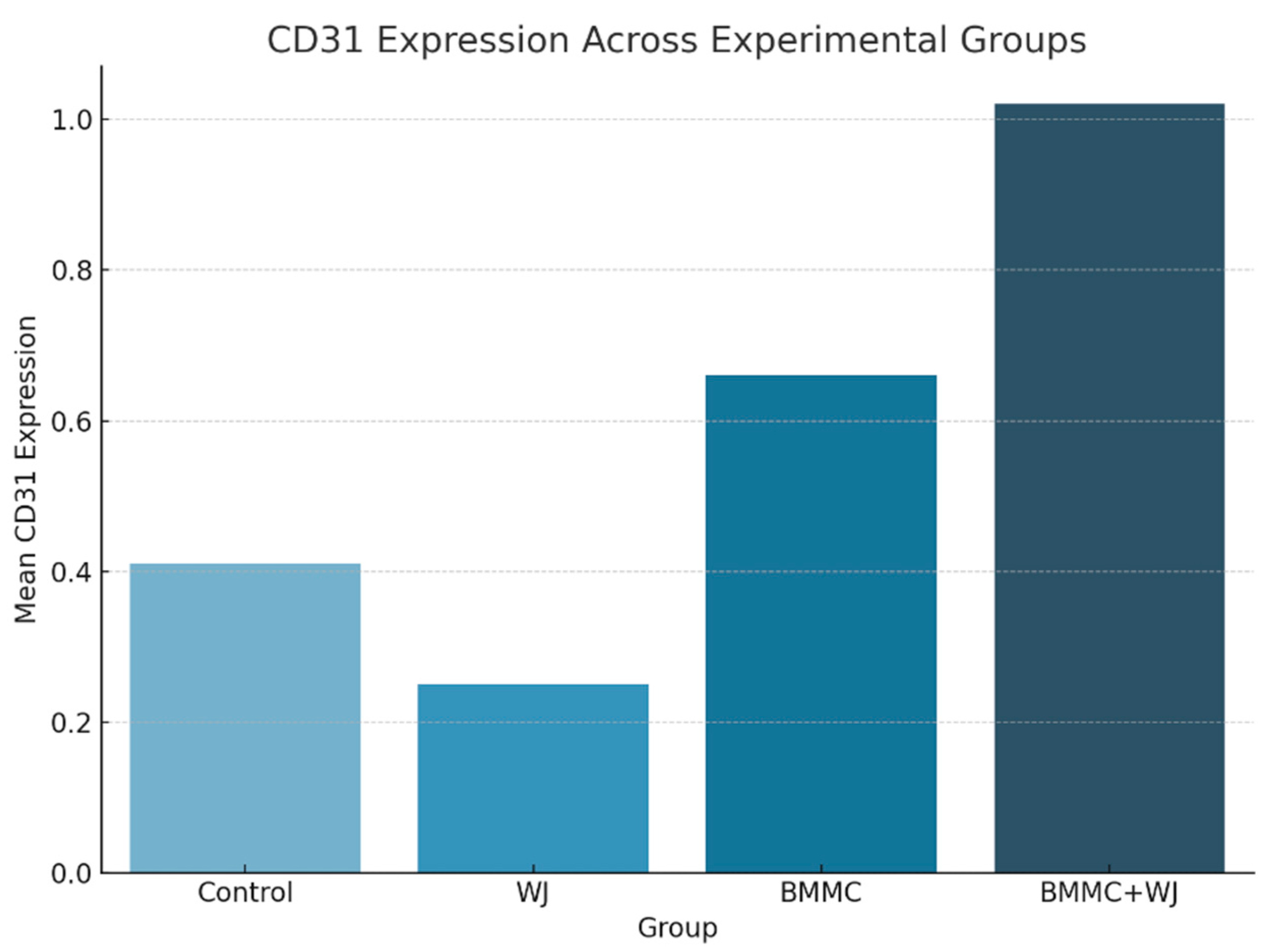
Vascularization Evaluation
4. Discussion
5. Conclusions
Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, B.; Shah, M.; Williams, L.N.; Curry, A.L.d.J.; Hong, Y.; Zhang, G.; Liao, J. Acellular Myocardial Scaffolds and Slices Fabrication, and Method for Applying Mechanical and Electrical Simulation to Tissue Construct. Methods Mol. Biol. 2022, 2485, 55–70. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Roacho-Pérez, J.A.; Garza-Treviño, E.N.; Moncada-Saucedo, N.K.; Carriquiry-Chequer, P.A.; Valencia-Gómez, L.E.; Matthews, E.R.; Gómez-Flores, V.; Simental-Mendía, M.; Delgado-Gonzalez, P.; Delgado-Gallegos, J.L.; et al. Artificial Scaffolds in Cardiac Tissue Engineering. Life 2022, 12, 1117. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pattar, S.S.; Hassanabad, A.F.; Fedak, P.W.M. Acellular Extracellular Matrix Bioscaffolds for Cardiac Repair and Regeneration. Front. Cell Dev. Biol. 2019, 7, 63. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Taylor, D.A.; Sampaio, L.C.; Ferdous, Z.; Gobin, A.S.; Taite, L.J. Decellularized matrices in regenerative medicine. Acta Biomater. 2018, 74, 74–89. [Google Scholar] [CrossRef] [PubMed]
- Penolazzi, L.; Pozzobon, M.; Bergamin, L.S.; D’agostino, S.; Francescato, R.; Bonaccorsi, G.; De Bonis, P.; Cavallo, M.; Lambertini, E.; Piva, R. Extracellular Matrix from Decellularized Wharton’s Jelly Improves the Behavior of Cells from Degenerated Intervertebral Disc. Front. Bioeng. Biotechnol. 2020, 8, 262. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Fayon, A.; Helle, D.; Francius, G.; Vincourt, J.-B.; Regnault, V.; Dumas, D.; Menu, P.; El Omar, R. Characterization of an Innovative Biomaterial Derived from Human Wharton’s Jelly as a New Promising Coating for Tissue Engineering Applications. Front. Bioeng. Biotechnol. 2022, 10, 884069. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wen, Y.; Ding, J.; Zhang, B.; Gao, Q. Bone marrow-derived mononuclear cell therapy for nonischaemic dilated cardiomyopathy-A meta-analysis. Eur. J. Clin. Investig. 2018, 48, e12894. [Google Scholar] [CrossRef] [PubMed]
- Wu, Q.; Wang, J.; Tan, W.L.W.; Jiang, Y.; Wang, S.; Li, Q.; Yu, X.; Tan, J.; Liu, S.; Zhang, P.; et al. Extracellular vesicles from human embryonic stem cell-derived cardiovascular progenitor cells promote cardiac infarct healing through reducing cardiomyocyte death and promoting angiogenesis. Cell Death Dis. 2020, 11, 354. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Uemura, L.; Simeoni, R.B.; Júnior, P.A.B.M.; Blume, G.G.; Gamba, L.K.; Tonial, M.S.; Simeoni, P.R.B.; Ribeiro, V.S.T.; Silvestre, R.; de Carvalho, K.A.T.; et al. Autologous Bone Marrow Mononuclear Cells (BMMC)-Associated Anti-Inflammatory Nanoparticles for Cardiac Repair After Myocardial Infarction. J. Funct. Biomater. 2022, 13, 59. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Blume, G.G.; Machado-Junior, P.A.B.; Simeoni, R.B.; Bertinato, G.P.; Tonial, M.S.; Nagashima, S.; Pinho, R.A.; de Noronha, L.; Olandoski, M.; de Carvalho, K.A.T.; et al. Bone-Marrow Stem Cells and Acellular Human Amniotic Membrane in a Rat Model of Heart Failure. Life 2021, 11, 958. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Foltz, K.M.; Neto, A.E.; Francisco, J.C.; Simeoni, R.B.; Miggiolaro, A.F.R.d.S.; Nascimento, T.G.D.; Mogharbel, B.F.; de Carvalho, K.A.T.; Faria-Neto, J.R.; de Noronha, L.; et al. Decellularized Wharton Jelly Implants Do Not Trigger Collagen and Cartilaginous Tissue Production in Tracheal Injury in Rabbits. Life 2022, 12, 942. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Takejima, A.L.; Francisco, J.C.; Simeoni, R.B.; de Noronha, L.; Garbers, L.A.; Foltz, K.M.; Junior, P.A.M.; Souza, I.C.; Pinho, R.A.; Carvalho, K.A.; et al. Role of mononuclear stem cells and decellularized amniotic membrane in the treatment of skin wounds in rats. Tissue Barriers. 2022, 10, 1982364. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- McInnes, A.D.; Moser, M.A.J.; Chen, X. Preparation and Use of Decellularized Extracellular Matrix for Tissue Engineering. J. Funct. Biomater. 2022, 13, 240. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Seo, M.; Kim, J.-C.; Kim, H.-K.; Choi, E.W.; Jeong, S.; Nam, K.C.; Jang, M. A Novel Secretory Vesicle from Deer Antlerogenic Mesenchymal Stem Cell-Conditioned Media (DaMSC-CM) Promotes Tissue Regeneration. Stem Cells Int. 2018, 2018, 3891404. [Google Scholar] [CrossRef]
- Bejleri, D.; Streeter, B.W.; Nachlas, A.L.Y.; Brown, M.E.; Gaetani, R.; Christman, K.L.; Davis, M.E. A Bioprinted Cardiac Patch Composed of Cardiac-Specific Extracellular Matrix and Progenitor Cells for Heart Repair. Adv. Healthc. Mater. 2018, 7, e1800672. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- de Cerio, A.L.-D.; Perez-Estenaga, I.; Inoges, S.; Abizanda, G.; Gavira, J.J.; Larequi, E.; Andreu, E.; Rodriguez, S.; Gil, A.G.; Crisostomo, V.; et al. Preclinical Evaluation of the Safety and Immunological Action of Allogeneic ADSC-Collagen Scaffolds in the Treatment of Chronic Ischemic Cardiomyopathy. Pharmaceutics 2021, 13, 1269. [Google Scholar] [CrossRef]
- Zhao, D.; Zhu, T.; Li, J.; Cui, L.; Zhang, Z.; Zhuang, X.; Ding, J. Poly(lactic-co-glycolic acid)-based composite bone-substitute materials. Bioact. Mater. 2021, 6, 346–360. [Google Scholar] [CrossRef]
- Zhu, T.; Cui, Y.; Zhang, M.; Zhao, D.; Liu, G.; Ding, J. Engineered three-dimensional scaffolds for enhanced bone regeneration in osteonecrosis. Bioact. Mater. 2020, 5, 584–601. [Google Scholar] [CrossRef]
- Das, A.; Nikhil, A.; Shiekh, P.A.; Yadav, B.; Jagavelu, K.; Kumar, A. Ameliorating impaired cardiac function in myocardial infarction using exosome-loaded gallic-acid-containing polyurethane scaffolds. Bioact. Mater. 2023, 33, 324–340. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jiang, H.; Lu, J.; Li, J.; Liu, Z.; Chen, F.; Wu, R.; Xu, X.; Liu, Y.; Jiang, Y.; Shi, D. A novel allogeneic acellular matrix scaffold for porcine cartilage regeneration. BMC Biotechnol. 2023, 23, 38. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Guarita-Souza, L.C.; Carvalho, K.A.T.D.; Rebelatto, C.; Senegaglia, A.; Hansen, P.; Furuta, M.; Miyague, N.; Francisco, J.C.; Olandoski, M.; Woitowicz, V.; et al. A comparação entre o transplante de células tronco mononucleares e mesenquimais no infarto do miocárdio. Rev. Bras. Cir. Cardiovasc. 2005, 20, 270–278. [Google Scholar] [CrossRef]
- Orlic, D.; Kajstura, J.; Chimenti, S.; Jakoniuk, I.; Anderson, S.M.; Li, B.; Pickel, J.; McKay, R.; Nadal-Ginard, B.; Bodine, D.M.; et al. Bone marrow cells regenerate infarcted myocardium. Nature 2001, 410, 701–705. [Google Scholar] [CrossRef] [PubMed]
- Hume, R.D.; Kanagalingam, S.; Deshmukh, T.; Chen, S.; Mithieux, S.M.; Rashid, F.N.; Roohani, I.; Lu, J.; Doan, T.; Graham, D.; et al. Tropoelastin Improves Post-Infarct Cardiac Function. Circ. Res. 2023, 132, 72–86. [Google Scholar] [CrossRef]
- Dubus, M.; Scomazzon, L.; Chevrier, J.; Montanede, A.; Baldit, A.; Terryn, C.; Quilès, F.; Thomachot-Schneider, C.; Gangloff, S.C.; Bouland, N.; et al. Decellularization of Wharton’s Jelly Increases Its Bioactivity and Antibacterial Properties. Front. Bioeng. Biotechnol. 2022, 10, 828424. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jiang, S.; Tian, G.; Yang, Z.; Gao, X.; Wang, F.; Li, J.; Tian, Z.; Huang, B.; Wei, F.; Sang, X.; et al. Enhancement of acellular cartilage matrix scaffold by Wharton’s jelly mesenchymal stem cell-derived exosomes to promote osteochondral regeneration. Bioact. Mater. 2021, 6, 2711–2728. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- González-Santamaría, J.; Villalba, M.; Busnadiego, O.; López-Olañeta, M.M.; Sandoval, P.; Snabel, J.; López-Cabrera, M.; Erler, J.T.; Hanemaaijer, R.; Lara-Pezzi, E.; et al. Matrix cross-linking lysyl oxidases are induced in response to myocardial infarction and promote cardiac dysfunction. Cardiovasc. Res. 2016, 109, 67–78. [Google Scholar] [CrossRef]
- Maghin, E.; Garbati, P.; Quarto, R.; Piccoli, M.; Bollini, S. Young at Heart: Combining Strategies to Rejuvenate Endogenous Mechanisms of Cardiac Repair. Front. Bioeng. Biotechnol. 2020, 8, 447. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| p * (Compared Groups) | Standard Deviation | Mean | n | Group | Variable | |
|---|---|---|---|---|---|---|
| 5.6 | 37.3 | 12 | Control | LVEF (%) D7 | ||
| 6.9 | 40.5 | 11 | BMMC | |||
| 8.1 | 40.0 | 10 | WJ | |||
| 0.434 | 9.3 | 36.1 | 15 | BMMC + WJ | ||
| 5.7 | 36.5 | 12 | Control | LVEF (%) D30 | ||
| 8.2 | 35.5 | 11 | BMMC | |||
| 10.3 | 44.5 | 10 | WJ | |||
| <0.001 | 0.051 | 8.6 | 49.4 | 15 | BMMC + WJ | |
| Dimensional Parameters | Groups | 7th | 30th | p (7 × 30 th) |
|---|---|---|---|---|
| LVESV (mL) | Control (n = 12) | 0.159 ± 0.046 | 0.194 ± 0.070 | 0.101 |
| BMMC (n = 11) | 0.182 ± 0.063 | 0.142 ± 0.074 | 0.190 | |
| WJ (n = 10) | 0.097 ± 0.052 | 0.177 ± 0.177 | 0.079 | |
| BMMC + WJ (n = 15) | 0.198 ± 0.065 | 0.129 ± 0.129 | 0.014 | |
| LVEDV (mL) | Control (n = 12) | 0.257 ± 0.065 | 0.301 ± 0.079 | 0.086 |
| BMMC (n = 11) | 0.308 ± 0.091 | 0.214 ± 0.100 | 0.065 | |
| WJ (n = 10) | 0.162 ± 0.061 | 0.246 ± 0.102 | 0.006 | |
| BMMC + WJ (n = 15) | 0.322 ± 0.076 | 0.254 ± 0.098 | 0.079 |
| Variable | Group | n | Mean | SD | p * |
|---|---|---|---|---|---|
| Collagen I (%) | Control | 11 | 95.4 | 6.8 | 20.7 |
| BMMC | 11 | 84.6 | 16.6 | 5.49 | |
| WJ | 8 | 89.3 | 12.1 | 8.3 | |
| BMMC + WJ | 13 | 88.9 | 13.3 | 0.105 | |
| Collagen III (%) | Control | 11 | 4.6 | 6.8 | |
| BMMC | 11 | 15.4 | 16.6 | ||
| WJ | 8 | 10.7 | 12.1 | ||
| BMMC + WJ | 13 | 11.1 | 13.3 | 0.105 |
| p* (Compared Groups) | SD | Mean | Group |
|---|---|---|---|
| <0.001 | 8,036,704.7 | 16,383,823 | Control (n = 12) |
| 2,949,393.4 | 13,111,745 | BMMC (n = 11) | |
| 5,496,210.3 | 7,683,479.8 | WJ (n = 10) | |
| 1,806,522.8 | 4,938,556.6 | BMMC + WJ (n = 15) |
| Groups Comparison | p * |
|---|---|
| BMMC + WJ × CONTROL | 0.0004 |
| BMMC + WJ × BMMC | 0.0027 |
| WJ × CONTROL | 0.0448 |
| Group | n | Mean | SD | p * |
|---|---|---|---|---|
| Control | 12 | 0.41 | 0.43 | |
| WJ | 11 | 0.25 | 0.23 | |
| BMMC | 10 | 0.66 | 1.38 | |
| BMMC + WJ | 15 | 1.02 | 1.11 | p = 0.420 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gamba, L.K.; Gamba, L.K.; da Costa, C.; Takejima, A.L.; Simeoni, R.B.; Rossa, I.C.M.; Silva, A.C.F.; de Bortolo, J.L.; Denk, M.A.; Nagashima, S.; et al. Wharton’s Jelly Bioscaffolds Improve Cardiac Repair with Bone Marrow Mononuclear Stem Cells in Rats. J. Funct. Biomater. 2025, 16, 175. https://doi.org/10.3390/jfb16050175
Gamba LK, Gamba LK, da Costa C, Takejima AL, Simeoni RB, Rossa ICM, Silva ACF, de Bortolo JL, Denk MA, Nagashima S, et al. Wharton’s Jelly Bioscaffolds Improve Cardiac Repair with Bone Marrow Mononuclear Stem Cells in Rats. Journal of Functional Biomaterials. 2025; 16(5):175. https://doi.org/10.3390/jfb16050175
Chicago/Turabian StyleGamba, Luize Kremer, Laiza Kremer Gamba, Camila da Costa, Aline Luri Takejima, Rossana Baggio Simeoni, Isabella Cristina Mendes Rossa, Anna Clara Faidiga Silva, Julia Letícia de Bortolo, Marcos Antônio Denk, Seigo Nagashima, and et al. 2025. "Wharton’s Jelly Bioscaffolds Improve Cardiac Repair with Bone Marrow Mononuclear Stem Cells in Rats" Journal of Functional Biomaterials 16, no. 5: 175. https://doi.org/10.3390/jfb16050175
APA StyleGamba, L. K., Gamba, L. K., da Costa, C., Takejima, A. L., Simeoni, R. B., Rossa, I. C. M., Silva, A. C. F., de Bortolo, J. L., Denk, M. A., Nagashima, S., Barbosa, C. d. A., Silveira, P. C. L., Francisco, J. C., & Guarita-Souza, L. C. (2025). Wharton’s Jelly Bioscaffolds Improve Cardiac Repair with Bone Marrow Mononuclear Stem Cells in Rats. Journal of Functional Biomaterials, 16(5), 175. https://doi.org/10.3390/jfb16050175