
Augmented Reality, Virtual Reality, and Game Technologies in Ophthalmology Training


 ,
,  ,
,  and
and
Abstract
1. Introduction
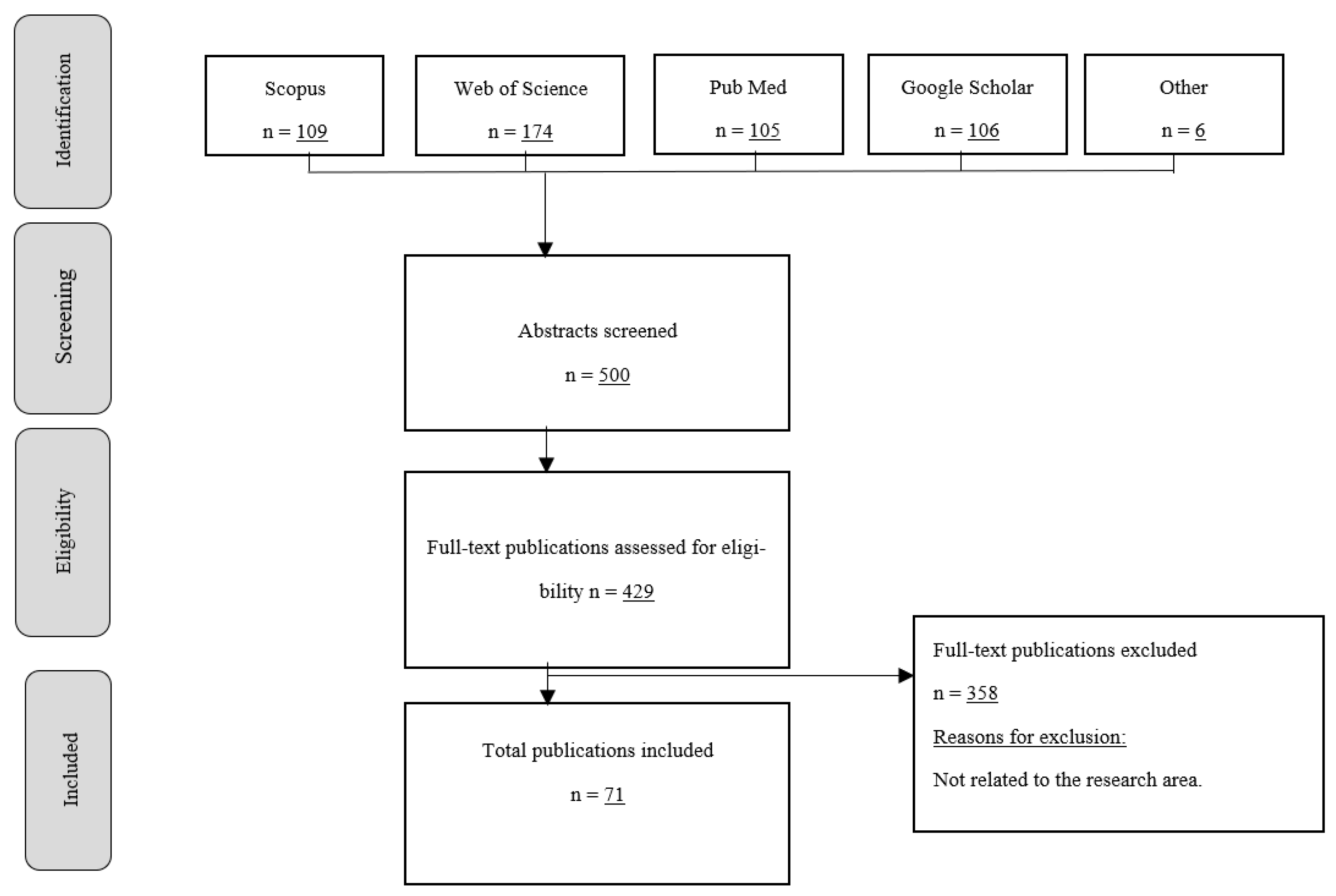
2. Search Methodology
2.1. Inclusion Criteria
2.2. Search Strategy
2.3. Exclusion Criteria
3. Review Studies Available on the Topics Related to AR in Optical Sciences Training
4. Results
4.1. RQ1: What Are the Advantages, Disadvantages, Limitations, and Challenges of AR and VR Technologies in Ophthalmology Training?
4.1.1. Advantages
4.1.2. Disadvantages and Limitations
4.1.3. Challenges
4.2. RQ2: What Hardware and Software Tools Have Been Developed for Teaching Ophthalmology?
4.2.1. HoloLens
4.2.2. Google Glass
4.2.3. VES: Virtual Eye Surgery
4.2.4. THELMA: The Human Eye Learning Model Assistant
4.2.5. The EYE Exam Simulator
4.2.6. iExaminer
4.3. RQ3: What Are the AR and VR Tools, or Frameworks Used for Developing Applications in the Field of Ophthalmology?
4.3.1. Eyesi® Surgical Simulator
4.3.2. Microvistouch
4.3.3. Eyesi® Surgical Simulator versus Microvistouch
4.3.4. PixEyes
4.3.5. Robotic Surgical Simulator (RoSSTM)
4.3.6. Mimic dV-Trainer (dV-Trainer)
4.3.7. da Vinci Skills Simulator (dVSS)
4.3.8. SimSurgery Educational Platform (SEP)
4.3.9. Other Related Technologies
4.4. RQ4: What Are the Advantages, Disadvantages, Limitations, and Challenges of Game Technologies in Ophthalmology Training?
4.5. RQ5: Can Games Technologies Be Used to Support Teaching Processes in Ophthalmology?
5. Limitations
- Methodological limitations include the lack of available data or sufficient research. There is very little research at the time in which we conducted this systematic review about ophthalmology related to new trends in teaching and learning with immersive technologies;
- Most of the analyzed articles have an adequate research method, though their samples are too small for robust data analysis;
- There are very few systematic reviews on related topics, so there are very few data that can be seen as providing a clear or consistent answer;
- Some developed VR and AR tools might not have been reported in the analyzed articles because those tools were developed by companies for commercial purposes;
- The lack of studies related to the use of gaming technologies in the field of ophthalmology is one of the most important limitations that we found.
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Avila-Garzon, C.; Bacca-Acosta, J.; Kinshuk; Duarte, J.; Betancourt, J. Augmented Reality in Education: An Overview of Twenty-Five Years of Research. Contemp. Educ. Technol. 2021, 13, ep302. [Google Scholar] [CrossRef]
- Bacca Acosta, J.L.; Fabregat Gesa, R.; Baldiris Navarro, S.M. Augmented Reality Trends in Education: A Systematic Review of Research and Applications. J. Educ. Technol. Soc. 2014, 17, 133–149. Available online: http://www.jstor.org/stable/jeductechsoci.17.4.133 (accessed on 21 April 2021).
- Khalifa, Y.M.; Bogorad, D.; Gibson, V.; Peifer, J.; Nussbaum, J. Virtual Reality in Ophthalmology Training. Surv. Ophthalmol. 2006, 51, 259–273. [Google Scholar] [CrossRef] [PubMed]
- Skarbez, R.; Smith, M.; Whitton, M.C. Revisiting Milgram and Kishino’s Reality-Virtuality Continuum. Front. Virtual Real. 2021, 2, 647997. [Google Scholar] [CrossRef]
- Bennett, C.R.; Bailin, E.S.; Gottlieb, T.K.; Bauer, C.M.; Bex, P.J.; Merabet, L.B. Virtual Reality Based Assessment of Static Object Visual Search in Ocular Compared to Cerebral Visual Impairment. In Lecture Notes in Computer Science, Universal Access in Human-Computer Interaction. Virtual, Augmented, and Intelligent Environments; Antona, M., Stephanidis, C., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 28–38. [Google Scholar]
- Sikder, S.; Luo, J.; Banerjee, P.P.; Luciano, C.; Kania, P.; Song, J.C.; Kahtani, E.S.; Edward, D.P.; Al Towerki, A.-E. The use of a virtual reality surgical simulator for cataract surgical skill assessment with 6 months of intervening operating room experience. Clin. Ophthalmol. 2015, 9, 141–149. [Google Scholar] [CrossRef]
- Thomsen, A.S.S.; Smith, P.; Subhi, Y.; de la Cour, M.D.; Tang, H.; Saleh, G.M.; Konge, L. High correlation between performance on a virtual-reality simulator and real-life cataract surgery. Acta Ophthalmol. 2016, 95, 307–311. [Google Scholar] [CrossRef] [PubMed]
- Ong, C.W.; Tan, M.C.J.; Lam, M.; Koh, V.T.C. Applications of Extended Reality in Ophthalmology: Systematic Review. J. Med. Internet Res. 2021, 23, e24152. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement (Chinese edition). J. Chin. Integr. Med. 2009, 7, 889–896. [Google Scholar] [CrossRef]
- Valencia-Hernandez, D.S.; Robledo, S.; Pinilla, R.; Duque-Méndez, N.D.; Olivar-Tost, G. SAP Algorithm for Citation Analysis: An improvement to Tree of Science. Ing. Investig. 2020, 40, 45–49. [Google Scholar] [CrossRef]
- Lee, R.; Raison, N.; Lau, W.Y.; Aydin, A.; Dasgupta, P.; Ahmed, K.; Haldar, S. A systematic review of simulation-based training tools for technical and non-technical skills in ophthalmology. Eye 2020, 34, 1737–1759. [Google Scholar] [CrossRef]
- Tang, K.S.; Cheng, D.L.; Mi, E.; Greenberg, P.B. Augmented reality in medical education: A systematic review. Can. Med. Educ. J. 2020, 11, e81–e96. [Google Scholar] [CrossRef] [PubMed]
- Newball, A.N.; Velez, J.; Satizabal, J.; Múnera, L.; Bernabe, G. Virtual surgical tele-simulations in ophthalmology. Int. Congr. Ser. 2003, 1256, 145–150. [Google Scholar] [CrossRef]
- Serna-Ojeda, J.C.; Graue-Hernández, E.O.; Guzmán-Salas, P.J.; Rodríguez-Loaiza, J.L. Simulation training in ophthalmology. Gac. Med. Mex. 2017, 153, 111–115. Available online: https://www.scopus.com/inward/record.uri?eid=2-s2.0-85017125811&partnerID=40&md5=16a3a31575972407840feca4f21ebcfe (accessed on 3 March 2021). [PubMed]
- Koch, F.; Koss, M.J.; Singh, P.; Naser, H. Virtuelle Realität in der Ophthalmologie. Klin. Mon. Fur Augenheilkd. 2009, 226, 672–676. [Google Scholar] [CrossRef] [PubMed]
- Leitritz, M.; Ziemssen, F.; Suesskind, D.; Partsch, M.; Voykov, B.; Bartz-Schmidt, K.U.; Szurman, G.B. Critical evaluation of the usability of augmented reality ophthalmoscopy for the training of inexperienced examiners. Retina 2014, 34, 785–791. [Google Scholar] [CrossRef] [PubMed]
- Pelah, A.; Koenderink, J.J. Editorial. ACM Trans. Appl. Percept. 2007, 4, 1. [Google Scholar] [CrossRef]
- Ahmed, Y.; Scott, I.U.; Greenberg, P.B. A survey of the role of virtual surgery simulators in ophthalmic graduate medical education. Graefe’s Arch. Clin. Exp. Ophthalmol. 2011, 249, 1263–1265. [Google Scholar] [CrossRef]
- Yeung, A.W.K.; Tosevska, A.; Klager, E.; Eibensteiner, F.; Laxar, D.; Stoyanov, J.; Glisic, M.; Zeiner, S.; Kulnik, S.T.; Crutzen, R.; et al. Virtual and Augmented Reality Applications in Medicine: Analysis of the Scientific Literature. J. Med. Internet Res. 2021, 23, e25499. [Google Scholar] [CrossRef]
- Lorch, A.C.; Kloek, C.E. An evidence-based approach to surgical teaching in ophthalmology. Surv. Ophthalmol. 2017, 62, 371–377. [Google Scholar] [CrossRef]
- Wei, L.; Nahavandi, S.; Weisinger, H. Optometry training simulation with augmented reality and haptics. In Proceedings of the 2013 IEEE/ACM International Conference on Advances in Social Networks Analysis and Mining, Niagara, ON, Canada, 25–28 August 2013; pp. 976–977. [Google Scholar]
- Wei, L.; Najdovski, Z.; Abdelrahman, W.; Nahavandi, S.; Weisinger, H. Augmented optometry training simulator with multi-point haptics. In Proceedings of the 2012 IEEE International Conference on Systems, Man, and Cybernetics (SMC), Seoul, Korea, 14–17 October 2012; pp. 2991–2997. [Google Scholar] [CrossRef]
- Knopf, N.A.; Boon, M.-Y.; Suaning, G.J.; Zapf, M.P.H.; Grigg, J. Initial mobility behaviors of people with visual impairment in a virtual environment using a mixed methods design. In Proceedings of the IEEE Life Sciences Conference (LSC), Sydney, Australia, 13–15 December 2017; pp. 153–156. [Google Scholar] [CrossRef]
- Garrett, B.; Taverner, T.; Gromala, D.; Tao, G.; Cordingley, E.; Sun, C. Virtual Reality Clinical Research: Promises and Challenges. JMIR Serious Games 2018, 6, e10839. [Google Scholar] [CrossRef]
- Grodin, M.H.; Johnson, T.M.; Acree, J.L.; Glaser, B.M. Ophthalmic surgical training: A curriculum to enhance surgical simulation. Retina 2008, 28, 1509–1514. [Google Scholar] [CrossRef] [PubMed]
- Roohipoor, R.; Yaseri, M.; Teymourpour, A.; Kloek, C.; Miller, J.B.; Loewenstein, J.I. Early Performance on an Eye Surgery Simulator Predicts Subsequent Resident Surgical Performance. J. Surg. Educ. 2017, 74, 1105–1115. [Google Scholar] [CrossRef]
- Li, E.; Fay, P.; Greenberg, P.B. A virtual cataract surgery course for ophthalmologists-in-training. Rhode Isl. Med. J. 2013, 96, 18–19. Available online: http://www.rimed.org/rimedicaljournal/2013/08/2013-08-18-cataract.pdf (accessed on 17 March 2021).
- de Paolis, L.T.; Mongelli, A. Augmented Reality, Virtual Reality, and Computer Graphics; Springer: Cham, Switzerland, 2016; Volume 9769. [Google Scholar] [CrossRef]
- Gros, B.; Kinshuk; Maina, M. The Future of Ubiquitous Learning: Learning Designs for Emerging Pedagogies. Lecture Notes in Educational Technology. 2016. Available online: https://eric.ed.gov/?id=ed613390 (accessed on 16 March 2021).
- Chan, M.; Uribe-Quevedo, A.; Kapralos, B.; Jenkin, M.; Jaimes, N.; Kanev, K. Virtual and Augmented Reality Direct Ophthalmoscopy Tool: A Comparison between Interactions Methods. Multimodal Technol. Interact. 2021, 5, 66. [Google Scholar] [CrossRef]
- Jiang, T.; Yu, D.; Wang, Y.; Zan, T.; Wang, S.; Li, Q. HoloLens-Based Vascular Localization System: Precision Evaluation Study With a Three-Dimensional Printed Model. J. Med. Internet Res. 2020, 22, e16852. [Google Scholar] [CrossRef] [PubMed]
- Wei, N.J.; Dougherty, B.; Myers, A.; Badawy, S.M.; Shah, N.; Cronin, R. Using Google Glass in Surgical Settings: Systematic Review. JMIR Mhealth Uhealth 2018, 6, e54. [Google Scholar] [CrossRef]
- Paul, S.K.; Clark, M.A.; Scott, I.U.; Greenberg, P.B. Virtual eye surgery training in ophthalmic graduate medical education. Can. J. Ophthalmol. 2018, 53, e218–e220. [Google Scholar] [CrossRef]
- Ricci, L.H.; Ferraz, C.A. Ophthalmoscopy simulation: Advances in training and practice for medical students and young ophthalmologists. Adv. Med. Educ. Pr. 2017, 8, 435–439. [Google Scholar] [CrossRef]
- Soto, C.; Vargas, M.; Uribe-Quevedo, A.; Jaimes, N.; Kapralos, B. AR stereoscopic 3D Human Eye Examination App. In Proceedings of the 2015 International Conference on Interactive Mobile Communication Technologies and Learning (IMCL), Thessaloniki, Greece, 19–20 November 2015; pp. 236–238. [Google Scholar] [CrossRef]
- Jaud, C.; Salleron, J.; Cisse, C.; Angioi-Duprez, K.; Berrod, J.; Conart, J. EyeSi Surgical Simulator: Validation of a proficiency-based test for assessment of vitreoretinal surgical skills. Acta Ophthalmol. 2020, 99, 390–396. [Google Scholar] [CrossRef]
- Rai, A.S.; Rai, A.S.; Mavrikakis, E.; Lam, W.C. Teaching binocular indirect ophthalmoscopy to novice residents using an augmented reality simulator. Can. J. Ophthalmol. 2017, 52, 430–434. [Google Scholar] [CrossRef]
- Saleh, G.M.; Lamparter, J.; Sullivan, P.M.; O’Sullivan, F.; Hussain, B.; Athanasiadis, I.; Litwin, A.S.; Gillan, S.N. The international forum of ophthalmic simulation: Developing a virtual reality training curriculum for ophthalmology. Br. J. Ophthalmol. 2013, 97, 789–792. [Google Scholar] [CrossRef] [PubMed]
- Wisse, R.P.; Coster, T.; Van Der Schaaf, M.; Cate, O.T. The Eyesi simulator in training ophthalmology residents: Results of a pilot study on self-efficacy, motivation and performance. BMJ Simul. Technol. Enhanc. Learn. 2017, 3, 111–115. [Google Scholar] [CrossRef]
- Saleh, G.M.; Theodoraki, K.; Gillan, S.; Sullivan, P.; O’Sullivan, F.; Hussain, B.; Bunce, C.; Athanasiadis, I. The development of a virtual reality training programme for ophthalmology: Repeatability and reproducibility (part of the International Forum for Ophthalmic Simulation Studies). Eye 2013, 27, 1269–1274. [Google Scholar] [CrossRef] [PubMed]
- McCannel, C. Continuous Curvilinear Capsulorhexis Training and Non-Rhexis Related Vitreous Loss: The Specificity of Virtual Reality Simulator Surgical Training (An American Ophthalmological Society Thesis). Trans. Am. Ophthalmol. Soc. 2017, 115, T2. Available online: https://www.aosonline.org/assets/PDF-Docs/Transactions/2017/1545-6110-v115-T2.pdf (accessed on 2 May 2021).
- Solverson, D.J.; Mazzoli, R.A.; Raymond, W.R.; Nelson, M.L.; Hansen, E.A.; Torres, M.F.; Bhandari, A.; Hartranft, C.D. Virtual Reality Simulation in Acquiring and Differentiating Basic Ophthalmic Microsurgical Skills. Simul. Health J. Soc. Simul. Health 2009, 4, 98–103. [Google Scholar] [CrossRef]
- Rouland, J.F.; Dubois, P.; Chaillou, C.; Meseuree, P.; Karpf, S.; Godin, S.; Duquenoy, F. SOPHOCLE (Simulateur Ophtalmologique de PHOtoCoagulation LaSer): Contribution de la réalité virtuelle [SOPHOCLE (Ophthalmologic Simulator of Laser PHOtocoagulation): Contribution to virtual reality]. J. Fr. D’ophtalmol. 1995, 18, 536–541. [Google Scholar]
- Staropoli, P.C.; Gregori, N.Z.; Junk, A.K.; Galor, A.; Goldhardt, R.; Goldhagen, B.E.; Shi, W.; Feuer, W. Surgical Simulation Training Reduces Intraoperative Cataract Surgery Complications Among Residents. Simul. Health J. Soc. Simul. Health 2018, 13, 11–15. [Google Scholar] [CrossRef]
- Pieramici, D.J.; Heimann, F.; Brassard, R.; Barteselli, G.; Ranade, S. Virtual Reality Becomes a Reality for Ophthalmologic Surgical Clinical Trials. Transl. Vis. Sci. Technol. 2020, 9, 1. [Google Scholar] [CrossRef]
- He, W.-M.; Deng, Y.-P. Actuality and expectation of ophthalmological teaching reform in China. Int. J. Ophthalmol. 2007, 7, 854–856. Available online: https://www.scopus.com/inward/record.uri?eid=2-s2.0-34447275468&partnerID=40&md5=7273dd6d5fdd8d112e05c0b14fc1291e (accessed on 13 May 2021).
- Ropelato, S.; Menozzi, M.; Michel, D.; Siegrist, M. Augmented Reality Microsurgery: A Tool for Training Micromanipulations in Ophthalmic Surgery Using Augmented Reality. Simul. Health J. Soc. Simul. Health 2020, 15, 122–127. [Google Scholar] [CrossRef]
- Balal, S.; Smith, P.; Bader, T.; Tang, H.L.; Sullivan, P.; Thomsen, A.S.S.; Carlson, T.; Saleh, G.M. Computer analysis of individual cataract surgery segments in the operating room. Eye 2019, 33, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Selvander, M.; Åsman, P. Virtual reality cataract surgery training: Learning curves and concurrent validity. Acta Ophthalmol. 2012, 90, 412–417. [Google Scholar] [CrossRef] [PubMed]
- Toledo, L.F.; Oliveira, J.; Haack, R.V. Haptic Surgery Simulation for Cataract. In Proceedings of the 19th Symposium on Virtual and Augmented Reality (SVR), Curitiba, Brasil, 1–4 November 2017; pp. 57–64. [Google Scholar]
- Vergmann, A.S.; Vestergaard, A.H.; Grauslund, J. Virtual vitreoretinal surgery: Validation of a training programme. Acta Ophthalmol. 2017, 95, 60–65. [Google Scholar] [CrossRef]
- Thomsen, A.S.S.; Subhi, Y.; Kiilgaard, J.F.; de la Cour, M.D.; Konge, L. Update on Simulation-Based Surgical Training and Assessment in Ophthalmology: A Systematic Review. Ophthalmology 2015, 122, 1111–1130.e1. [Google Scholar] [CrossRef] [PubMed]
- Alwadani, F.; Morsi, M.S. Pixeye virtual reality training has the potential of enhancing proficiency of laser trabeculoplasty performed by medical students: A pilot study. Middle East Afr. J. Ophthalmol. 2012, 19, 120–122. [Google Scholar] [CrossRef]
- Lin, J.C.; Yu, Z.; Scott, I.U.; Greenberg, P.B. Virtual reality training for cataract surgery operating performance in ophthalmology trainees. Cochrane Database Syst. Rev. 2021, 12, CD014953. [Google Scholar] [CrossRef] [PubMed]
- Bric, J.D.; Lumbard, D.C.; Frelich, M.J.; Gould, J.C. Current state of virtual reality simulation in robotic surgery training: A review. Surg. Endosc. 2016, 30, 2169–2178. [Google Scholar] [CrossRef]
- Bakshi, S.K.; Lin, S.R.; Ting, D.S.W.; Chiang, M.F.; Chodosh, J. The era of artificial intelligence and virtual reality: Transforming surgical education in ophthalmology. Br. J. Ophthalmol. 2020, 105, 1325–1328. [Google Scholar] [CrossRef]
- Le, T.D.; Adatia, F.A.; Lam, W.-C. Virtual reality ophthalmic surgical simulation as a feasible training and assessment tool: Results of a multicentre study. Can. J. Ophthalmol. 2011, 46, 56–60. [Google Scholar] [CrossRef]
- McCannel, C.A.; Reed, D.C.; Goldman, D.R. Ophthalmic Surgery Simulator Training Improves Resident Performance of Capsulorhexis in the Operating Room. Ophthalmology 2013, 120, 2456–2461. [Google Scholar] [CrossRef]
- Wilson, A.S.; O’Connor, J.; Taylor, L.; Carruthers, D. A 3D virtual reality ophthalmoscopy trainer. Clin. Teach. 2017, 14, 427–431. [Google Scholar] [CrossRef]
- Wilson, A.S.; O’Connor, J.; Taylor, L.; Carruthers, D. A Case Study into the Use of Virtual Reality and Gamification in Ophthalmology Training. In Lecture Notes in Computer Science, Serious Games; Alcañiz, M., Göbel, S., Ma, M., Fradinho Oliveira, M., Baalsrud Hauge, J., Marsh, T., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 158–169. [Google Scholar]
- Mårell-Olsson, E. Using gamification as an online teaching strategy to develop students’ 21st century skills. Interact. Des. Arch. 2021, 47, 69–93. Available online: http://urn.kb.se/resolve?urn=urn:nbn:se:umu:diva-182180 (accessed on 15 March 2021). [CrossRef]
- Scales, C.D.; Moin, T.; Fink, A.; Berry, S.H.; Afsar-Manesh, N.; Mangione, C.M.; Kerfoot, B.P. A randomized, controlled trial of team-based competition to increase learner participation in quality-improvement education. Int. J. Qual. Health Care 2016, 28, 227–232. [Google Scholar] [CrossRef]
- Aydındoğan, G.; Kavaklı, K.; Şahin, A.; Artal, P.; Ürey, H. Applications of augmented reality in ophthalmology [Invited]. Biomed. Opt. Express 2020, 12, 511–538. [Google Scholar] [CrossRef]
- Ståhl, A.; Boeker, M.; Ehlken, C.; Agostini, P.D.H.; Reinhard, T. Evaluation eines internetbasierten E-Learnings für den Studentenunterricht im Fach Augenheilkunde. Ophthalmol. Z. Dtsch. Ophthalmol. Ges. 2009, 106, 999–1005. [Google Scholar] [CrossRef]
- Carvalho, J.A. Oftalmologia e realidade virtual. Rev. Bras. Oftalmol. 2012, 71, 40–47. [Google Scholar] [CrossRef]
- Bull, G.; Thompson, A.D.; Schmidt-Crawford, D.; Garofalo, J.; Hodges, C.B.; Spector, J.M.; Ferdig, R.E.; Edyburn, D.; Kins-huk. Evaluating the Impact of Educational Technology. J. Digit. Learn. Teach. Educ. 2016, 32, 117–118. [Google Scholar] [CrossRef][Green Version]
- De Rooij, I.J.; Van De Port, I.G.; Meijer, J.-W.G. Effect of Virtual Reality Training on Balance and Gait Ability in Patients With Stroke: Systematic Review and Meta-Analysis. Phys. Ther. 2016, 96, 1905–1918. [Google Scholar] [CrossRef] [PubMed]
- Sayed, A.M.; Shousha, M.A.; Islam, B.; Eleiwa, T.K.; Kashem, R.; Abdel-Mottaleb, M.; Ozcan, E.; Tolba, M.; Cook, J.C.; Ii, R.K.P. Mobility improvement of patients with peripheral visual field losses using novel see-through digital spectacles. PLoS ONE 2020, 15, e0240509. [Google Scholar] [CrossRef]
- Winebrake, J.P.; McMahon, J.F.; Sun, G. The Utility of Virtual Reality Simulation in Cataract Surgery Training: A Systematic Review. J. Acad. Ophthalmol. 2020, 12, e221–e233. [Google Scholar] [CrossRef]
- Thomsen, A.S.S.; Bach-Holm, D.; Kjærbo, H.; Højgaard-Olsen, K.; Subhi, Y.; Saleh, G.M.; Park, Y.S.; la Cour, M.; Konge, L. Operating Room Performance Improves after Proficiency-Based Virtual Reality Cataract Surgery Training. Ophthalmology 2017, 124, 524–531. [Google Scholar] [CrossRef] [PubMed]
- Eckert, M.; Volmerg, J.S.; Friedrich, C.M. Augmented Reality in Medicine: Systematic and Bibliographic Review. JMIR Mhealth Uhealth 2019, 7, e10967. [Google Scholar] [CrossRef] [PubMed]
- Brigham, T.J. Reality Check: Basics of Augmented, Virtual, and Mixed Reality. Med. Ref. Serv. Q. 2017, 36, 171–178. [Google Scholar] [CrossRef]
- Kyaw, B.M.; Saxena, N.; Posadzki, P.; Vseteckova, J.; Nikolaou, C.K.; George, P.P.; Divakar, U.; Masiello, I.; A Kononowicz, A.; Zary, N.; et al. Virtual Reality for Health Professions Education: Systematic Review and Meta-Analysis by the Digital Health Education Collaboration. J. Med. Internet Res. 2019, 21, e12959. [Google Scholar] [CrossRef] [PubMed]
- Parsons, T.D.; Riva, G.; Parsons, S.; Mantovani, F.; Newbutt, N.; Lin, L.; Venturini, E.; Hall, T. Virtual Reality in Pediatric Psychology. Pediatrics 2017, 140, S86–S91. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Database | Search String |
|---|---|
| Scopus | Title-abs-key (((game and based and learning) or (serious and Games) or (gamification) or (augmented and reality) or (virtual and reality)) and (ophthalmology* or optometrist*) and (training* or learn*)) and (limit-to (doctype, “ar”) or limit-to (doctype, “cp”)) and (limit-to (subjarea, “comp”) or limit-to (subjarea, “medi”) or limit-to (subjarea, “engi”)) |
| Web of Science | ts = (((game and based and learning) or (serious and games) or (gamification) or (augmented and reality) or (virtual and reality)) and (ophthalmology* or optometrist*) and (training* or learn*)) or ti = (((game and based and learning) or (serious and games) or (gamification) or (augmented and reality) or (virtual and reality)) and (ophthalmology* or optometrist*) and (training* or learn*)) |
| PubMed | (((game and based and learning) or (serious and games) or (gamification) or (augmented and reality) or (virtual and reality)) and (ophthalmology* or optometrist*) and (training* or learn*)) or ts = (((game and based and learning) or (serious and games) or (gamification) or (augmented and reality) or (virtual and reality)) and (ophthalmology* or optometrist*) and (training* or learn*)) |
| Google Scholar | (((game and based and learning) or (serious and games) or (gamification) or (augmented and reality) or (virtual and reality)) and (ophthalmology* or optometrist*) and (training* or learn*)) or ts = (((game and based and learning) or (serious and games) or (gamification) or (augmented and reality) or (virtual and reality)) and (ophthalmology* or optometrist*) and (training* or learn*)) |
| Study (Papers Reviewed) | Summary of Findings | Analysis |
|---|---|---|
| 131 | A total of 131 studies were included in this review, with 93 different simulators described. Of these 131, 53 were virtual reality studies, 47 were wet laboratory models, 26 were dry laboratory models, and 5 were on electronic learning. Of all the analyses carried out, only two of the studies provided any evidence. The models with the greatest validity evidence were Eyesi Surgical, Eyesi Direct Ophthalmoscope, and Eye Surgical Skills Assessment Test [11]. | A wide range of models have been described, but only the Eyesi has undergone comprehensive investigation. |
| 73 | The authors introduce an analytical model to evaluate AR applications for teaching in medical education. Moreover, there is an increasing interest in the use of AR for medical education [12]. | There is a lack of research on medical training with AR and, therefore, there is insufficient evidence for recommending adoption in the curriculum. |
| Challenges | Description |
|---|---|
| Interaction with virtual world | The development of new technologies will help to replicate images with greater clarity and reality. |
| Need to generate more studies | There are very few published studies on VR and AR, so more studies should be generated to demonstrate their efficiency in ophthalmological surgery. |
| Lack of metrics | The research community has not established a standard metric, and the search for a realistic and inexpensive VR method has led to experimentation with various technologies. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muñoz, E.G.; Fabregat, R.; Bacca-Acosta, J.; Duque-Méndez, N.; Avila-Garzon, C. Augmented Reality, Virtual Reality, and Game Technologies in Ophthalmology Training. Information 2022, 13, 222. https://doi.org/10.3390/info13050222
Muñoz EG, Fabregat R, Bacca-Acosta J, Duque-Méndez N, Avila-Garzon C. Augmented Reality, Virtual Reality, and Game Technologies in Ophthalmology Training. Information. 2022; 13(5):222. https://doi.org/10.3390/info13050222
Chicago/Turabian StyleMuñoz, Eduardo Gross, Ramon Fabregat, Jorge Bacca-Acosta, Néstor Duque-Méndez, and Cecilia Avila-Garzon. 2022. "Augmented Reality, Virtual Reality, and Game Technologies in Ophthalmology Training" Information 13, no. 5: 222. https://doi.org/10.3390/info13050222
APA StyleMuñoz, E. G., Fabregat, R., Bacca-Acosta, J., Duque-Méndez, N., & Avila-Garzon, C. (2022). Augmented Reality, Virtual Reality, and Game Technologies in Ophthalmology Training. Information, 13(5), 222. https://doi.org/10.3390/info13050222