Bilateral Subthalamic Nucleus Deep Brain Stimulation under General Anesthesia: Literature Review and Single Center Experience

 , , , , and
, , , , and
Abstract
1. Introduction
2. STN DBS Using Intraoperative Imaging or Microelectrode Recording Under GA
2.1. Using Intraoperative Imaging
2.1.1. Intraoperative CT
2.1.2. Intraoperative MRI
2.1.3. Targeting Accuracy
2.2. Using Microelectrode Recording
2.2.1. Is MER Mandatory for STN DBS Surgery?
2.2.2. Is MER Possible Under GA?
2.2.3. Clinical Experiences of STN DBS Using MER under GA
2.3. Intraoperative Imaging vs. MER in STN DBS under GA

{kind=link}
{kind=link}
| Author | Year | Study Type | Number of Patients | Age (yrs) | Disease Duration (yrs) | Follow-Up (Months) | |||
|---|---|---|---|---|---|---|---|---|---|
| GA | LA | GA | LA | GA | LA | ||||
| Maltete et al. [58] | 2004 | Clinical | 15 | 15 | 59.8 8.0 | 58.0 6.1 | 13.4 3.7 | 13.5 2.6 | 6 |
| Yamada et al. [54] | 2007 | Clinical | 15 | 10 | 65.2 7.0 | 65.6 8.6 | 11.1 5.0 | 6.8 2.4 | 3 |
| Saleh et al. [26] | 2015 | Clinical | 14 | 23 | 64.0 ± 11.9 | 60.6 ± 7.0 | 10.9 ± 3.8 | 11.3 ± 4.9 | 6 |
| Tsai et al. [52] | 2016 | Clinical | 8 | 8 | 49.6 ± 7.1 * | 41.1 ± 10.2 * | 9.3 ± 2.4 | 12.4 ± 9.2 | 6 |
| Brodsky et al. [59] | 2017 | Clinical | 27 (20 GPi, 7 STN) | 34 (20 GPi, 14 STN) | 63.7 ± 9.79 | 63.1 ± 7.61 | NR | NR | 6 |
| Lefranc et al. [112] | 2017 | Clinical | 13 | 10 | 62.80 ± 7.1 | 63.1 ± 10 | 12.60 ± 3.6 | 12.10 ± 3.5 | 12 |
| Blasberg et al. [87] | 2018 | Clinical | 48 | 48 | 65.75 ± 1.18 | 65.52 ± 1.13 | 11.65 ± 0.81 | 10.87 ± 0.78 | 6 |
| Chen et al. [42] | 2018 | Clinical | 41 | 14 | 64.6 ± 8.25 | 63.1 ± 10.1 | 7.5 ± 3.4 | 8.6 ± 4.6 | 6 |
| Ho et al. [16] | 2018 | Meta-analysis | 663 | 6441 | 58.3 ± 6.8 | 59.4 ± 5.2 | 11.0 ± 1.5 | 12.3 ± 2.1 | 12 |
| Liu et al. [113] | 2019 | Meta-analysis | 967 | 556 | NR | NR | NR | NR | NR |
| Tsai et al. [108] | 2019 | Clinical | 22 | 9 | 57.7 ± 7.4 | 49.4 ± 12.2 | 57.7 ± 7.4 | 49.4 ± 12.2 | 60 |
| This study | 2020 | Clinical | 90 | 56 | 57.43 ± 7.85 | 58.91 ± 8.65 | 11.67 ± 4.75 | 10.55 ± 4.89 | 6 |
| Baseline UPDRS III | Follow-Up UPDRS III * | %UPDRS III Change | Baseline LEDD | Follow-Up LEDD | %LEDD reduction | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Author | GA | LA | GA | LA | GA | LA | p Value | GA | LA | GA | LA | GA | LA | p Value |
| Maltete et al. | 47.1 ± 15.4 | 39.9 ± 13.9 | 17.0 ± 8.6 | 10.9 ± 7.2 | 63.9% | 72.7% | 0.07 | 1449 ± 398 | 1507 ± 465 | 310 ± 350 | 392 ± 440 | 78.6% | 74.0% | 0.06 |
| Yamada et al. | 52.4 ± 19.0 | 45.9 ± 17.7 | 14.3 ± 15.4 | 7.1 ± 7.0 | 72.7% | 82.5% | No significant difference | 375.7 ± 195.6 | 425.0 ± 171.8 | 303.3 ± 164.7 | 261.1 ± 164.0 | 16.6% | 38.2% | NR |
| Saleh et al. | NR | NR | NR | NR | NR | NR | NR | 2134.9 ± 1175.8 | 1702.7 ± 876.0 | NR | NR | 49.27% | 38.27% | 0.4447 |
| Tsai et al. | 41.7 ± 29.4 | 39.9 ± 16.3 | NR | NR | 65.7% | 45.8 ± 26.2% | NR | NR | NR | NR | NR | NR | NR | NR |
| Brodsky et al. | 42.2 ± 10.6 | 41.7 ± 12.5 | 14.8 ± 8.9 ** | 17.6 ± 12.26 ** | 35%% | 42.2%% | 0.19 | NR | NR | NR | NR | NR | NR | NR |
| Lefranc et al. | 35.92 ± 11.15 | 33.10 ± 5.38 | 18.0 ± 7.2 | 20.0 ± 10.47 | 49% | 40.30% | 0.336 | 1585.10 ± 496.40 | 1247.70 ± 579.80 | 519.17 ± 282.71 | 716.80 ± 320.14 | Significantly greater in the GA than in the LA | 0.03 | |
| Blasberg et al. | 38.47 ± 1.94 | 34.79 ± 1.61 | NR | NR | NR | NR | 0.18 | 1070.72 ± 49.67 | 972.23 ± 55.15 | NR | NR | NR | NR | 0.008 |
| Chen et al. | 53.8 ± 16.4 | 53.7 ± 17.0 | 26.1 ± 12.0 | 21.6 ± 7.3 | 48.8% | 40.3% | 0.20 | NR | NR | NR | NR | NR | NR | 0.49 |
| Ho et al. | NR | NR | NR | NR | 51.1 ± 16.6% (n = 510) | 46.7 ± 27.4 ± (n = 4931) | 0.494 | NR | NR | NR | NR | 45 ± 12.8% (n = 444) | 47 ± 26.6% (n = 3893) | 0.752 |
| Liu et al. | NR | NR | NR | NR | NR | NR | 0.60 | NR | NR | NR | NR | NR | NR | 0.23 |
| Tsai et al. | 46.3 ± 14.4 | 28.6 ± 9.3 | 42.9 ± 17.4 | 24.6 ± 7.8 | 43.2 ± 14.1% | 46.8 ± 13.8% | 0.45 | NR | NR | NR | NR | 47.56 ± 18.98% | 51.37 ± 31.73% | 0.51 |
| This study | 38.11 ± 13.96 | 40.42 ± 15.30 | 21.48 ± 12.33 | 24.68 ± 12.51 | 43.6% | 38.9% | 0.136 | 1448.0 ± 546.93 | 1031.63 ± 451.08 | 483.99 ± 330.42 | 461.3 ± 284.65 | 66.6% | 55.3% | <0.0001 |
| Author | Number of MER Tracks | Overall Adverse Effects | Hemorrhage | Infection | Operation Time |
|---|---|---|---|---|---|
| Maltete et al. | NR | No adverse reaction to the use of propofol, 1 pulmonary atelectasia | NR | NR | NR |
| Yamada et al. | NR | NR | NR | NR | NR |
| Saleh et al. | NR | No significant differences | NR | NR | GA 424 ± 12 vs LA 307 ± 80 p = 0.0026 |
| Tsai et al. | NR | No significant differences | NR | NR | NR |
| Brodsky et al. | NR | NR | 1 small venous hemorrhage in LA, 1 small nonhemorrhagic infarct in GA | 1 in GA | NR |
| Lefranc et al. | NR | No significant differences p = 0.39 | NR | NR | NR |
| Blasberg et al. | NR | No significant differences | 1.00 | 1.00 | 0.31 |
| Chen et al. | NR | NR | NR | NR | GA 266.0 ± 60.6 vs LA 260.9 ± 57.6 p = 0.78 |
| Ho et al. | GA 1.4 ± 0.44 vs LA 2.1 ± 0.69 p = 0.006 | NR | %ICH/lead: GA 0.3 ± 0.0 vs LA 1.1 ± 0.3, p < 0.001 | %infection/lead GA 0.7 ± 0.0 vs LA 1.4 ± 0.0, p < 0.001 | GA 253.7 ± 82.3 vs LA 272.4 ± 92.5 p = 0.748 |
| Liu et al. | NR | 0.94 | 0.64 | NR | 0.47 |
| Tsai et al. | Significantly less in GA p = 0.04 | Similar adverse effects | NR | NR | NR |
| This study | 1 required revision due to inappropriate lead position in LA | 1 IPG site infection treated by antibiotics in LA |
3. SNUH Experience
4. Future Direction
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Han, M.; Nagele, E.; DeMarshall, C.; Acharya, N.; Nagele, R. Diagnosis of Parkinson’s disease based on disease-specific autoantibody profiles in human sera. PLoS ONE 2012, 7, e32383. [Google Scholar] [CrossRef] [PubMed]
- Benabid, A.-L.; Pollak, P.; Louveau, A.; Henry, S.; De Rougemont, J. Combined (thalamotomy and stimulation) stereotactic surgery of the VIM thalamic nucleus for bilateral Parkinson disease. Ster. Funct. Neurosurg. 1987, 50, 344–346. [Google Scholar] [CrossRef] [PubMed]
- Fasano, A.; Daniele, A.; Albanese, A. Treatment of motor and non-motor features of Parkinson’s disease with deep brain stimulation. Lancet Neurol. 2012, 11, 429–442. [Google Scholar] [CrossRef]
- Kleiner-Fisman, G.; Herzog, J.; Fisman, D.N.; Tamma, F.; Lyons, K.E.; Pahwa, R.; Lang, A.E.; Deuschl, G. Subthalamic nucleus deep brain stimulation: Summary and meta-analysis of outcomes. Mov. Disord. 2006, 21, S290–S304. [Google Scholar] [CrossRef]
- Kim, H.-J.; Jeon, B.S.; Paek, S.H. Nonmotor symptoms and subthalamic deep brain stimulation in Parkinson’s disease. J. Mov. Disord. 2015, 8, 83. [Google Scholar] [CrossRef] [PubMed]
- Rezai, A.R.; Kopell, B.H.; Gross, R.E.; Vitek, J.L.; Sharan, A.D.; Limousin, P.; Benabid, A.L. Deep brain stimulation for Parkinson’s disease: Surgical issues. Mov. Disord. 2006, 21 (Suppl. 14), S197–S218. [Google Scholar] [CrossRef]
- Lyons, M.K.; Ziemba, K.; Evidente, V. Multichannel microelectrode recording influences final electrode placement in pallidal deep brain stimulation for Parkinson’s disease: Report of twenty consecutive cases. Turk. Neurosurg. 2011, 21, 555–558. [Google Scholar] [CrossRef]
- Kinfe, T.M.; Vesper, J. The impact of multichannel microelectrode recording (MER) in deep brain stimulation of the basal ganglia. In Stereotactic and Functional Neurosurgery; Springer: Berlin/Heidelberg, Germany, 2013; pp. 27–33. [Google Scholar]
- Chen, S.-Y.; Lee, C.-C.; Lin, S.-H.; Hsin, Y.-L.; Lee, T.-W.; Yen, P.-S.; Chou, Y.-C.; Lee, C.-W.; Hsieh, W.A.; Su, C.-F. Microelectrode recording can be a good adjunct in magnetic resonance image–directed subthalamic nucleus deep brain stimulation for parkinsonism. Surg. Neurol. 2006, 65, 253–260. [Google Scholar] [CrossRef]
- Chang, W.S.; Kim, H.Y.; Kim, J.P.; Park, Y.S.; Chung, S.S.; Chang, J.W. Bilateral subthalamic deep brain stimulation using single track microelectrode recording. Acta Neurochir. 2011, 153, 1087–1095. [Google Scholar] [CrossRef]
- Tsai, S.-T.; Hung, H.-Y.; Lee, C.-H.; Chen, S.-Y. Letter to the Editor: Deep brain stimulation and microelectrode recording. J. Neurosurg. 2014, 120, 580. [Google Scholar] [CrossRef]
- Machado, A.; Rezai, A.R.; Kopell, B.H.; Gross, R.E.; Sharan, A.D.; Benabid, A.L. Deep brain stimulation for Parkinson’s disease: Surgical technique and perioperative management. Mov. Disord. 2006, 21 (Suppl. 14), S247–S258. [Google Scholar] [CrossRef] [PubMed]
- Priori, A.; Egidi, M.; Pesenti, A.; Rohr, M. Do intraoperative microrecordings improve subthalamic nucleus targeting in stereotactic neurosurgery for Parkinson’s disease? J. Neurosurg. Sci. 2003, 47, 56. [Google Scholar] [PubMed]
- Benazzouz, A.; Breit, S.; Koudsie, A.; Pollak, P.; Krack, P.; Benabid, A.L. Intraoperative microrecordings of the subthalamic nucleus in Parkinson’s disease. Mov. Disord. Off. J. Mov. Disord. Soc. 2002, 17, S145–S149. [Google Scholar] [CrossRef] [PubMed]
- Su, X.-L.; Luo, X.-G.; Lv, H.; Wang, J.; Ren, Y.; He, Z.-Y. Factors predicting the instant effect of motor function after subthalamic nucleus deep brain stimulation in Parkinson’s disease. Transl. Neurodegener. 2017, 6, 14. [Google Scholar] [CrossRef] [PubMed]
- Ho, A.L.; Ali, R.; Connolly, I.D.; Henderson, J.M.; Dhall, R.; Stein, S.C.; Halpern, C.H. Awake versus asleep deep brain stimulation for Parkinson’s disease: A critical comparison and meta-analysis. J. Neurol. Neurosurg. Psychiatry 2018, 89, 687–691. [Google Scholar] [CrossRef]
- Saint-Cyr, J.A.; Hoque, T.; Pereira, L.C.; Dostrovsky, J.O.; Hutchison, W.D.; Mikulis, D.J.; Abosch, A.; Sime, E.; Lang, A.E.; Lozano, A.M. Localization of clinically effective stimulating electrodes in the human subthalamic nucleus on magnetic resonance imaging. J. Neurosurg. 2002, 97, 1152–1166. [Google Scholar] [CrossRef]
- McClelland, S., 3rd; Ford, B.; Senatus, P.B.; Winfield, L.M.; Du, Y.E.; Pullman, S.L.; Yu, Q.; Frucht, S.J.; McKhann, G.M., 2nd; Goodman, R.R. Subthalamic stimulation for Parkinson disease: Determination of electrode location necessary for clinical efficacy. Neurosurg. Focus 2005, 19, E12. [Google Scholar] [CrossRef]
- Zonenshayn, M.; Rezai, A.R.; Mogilner, A.Y.; Beric, A.; Sterio, D.; Kelly, P.J. Comparison of anatomic and neurophysiological methods for subthalamic nucleus targeting. Neurosurgery 2000, 47, 282–292, discussion 292–284. [Google Scholar] [CrossRef]
- Lanotte, M.M.; Rizzone, M.; Bergamasco, B.; Faccani, G.; Melcarne, A.; Lopiano, L. Deep brain stimulation of the subthalamic nucleus: Anatomical, neurophysiological, and outcome correlations with the effects of stimulation. J. Neurol. Neurosurg. Psychiatry 2002, 72, 53–58. [Google Scholar] [CrossRef]
- Bus, S.; Pal, G.; Ouyang, B.; van den Munckhof, P.; Bot, M.; Sani, S.; Verhagen Metman, L. Accuracy of Microelectrode Trajectory Adjustments during DBS Assessed by Intraoperative CT. Stereotact. Funct. Neurosurg. 2018, 96, 231–238. [Google Scholar] [CrossRef]
- Starr, P.A.; Martin, A.J.; Ostrem, J.L.; Talke, P.; Levesque, N.; Larson, P.S. Subthalamic nucleus deep brain stimulator placement using high-field interventional magnetic resonance imaging and a skull-mounted aiming device: Technique and application accuracy. J. Neurosurg. 2010, 112, 479–490. [Google Scholar] [CrossRef] [PubMed]
- Foltynie, T.; Zrinzo, L.; Martinez-Torres, I.; Tripoliti, E.; Petersen, E.; Holl, E.; Aviles-Olmos, I.; Jahanshahi, M.; Hariz, M.; Limousin, P. MRI-guided STN DBS in Parkinson’s disease without microelectrode recording: Efficacy and safety. J. Neurol. Neurosurg. Psychiatry 2011, 82, 358–363. [Google Scholar] [CrossRef] [PubMed]
- Nakajima, T.; Zrinzo, L.; Foltynie, T.; Olmos, I.A.; Taylor, C.; Hariz, M.I.; Limousin, P. MRI-guided subthalamic nucleus deep brain stimulation without microelectrode recording: Can we dispense with surgery under local anaesthesia? Stereotact. Funct. Neurosurg. 2011, 89, 318–325. [Google Scholar] [CrossRef] [PubMed]
- Ostrem, J.L.; Galifianakis, N.B.; Markun, L.C.; Grace, J.K.; Martin, A.J.; Starr, P.A.; Larson, P.S. Clinical outcomes of PD patients having bilateral STN DBS using high-field interventional MR-imaging for lead placement. Clin. Neurol. Neurosurg. 2013, 115, 708–712. [Google Scholar] [CrossRef] [PubMed]
- Saleh, S.; Swanson, K.I.; Lake, W.B.; Sillay, K.A. Awake neurophysiologically guided versus asleep MRI-guided STN DBS for Parkinson disease: A comparison of outcomes using levodopa equivalents. Stereotact. Funct. Neurosurg. 2015, 93, 419–426. [Google Scholar] [CrossRef]
- Ostrem, J.L.; Ziman, N.; Galifianakis, N.B.; Starr, P.A.; San Luciano, M.; Katz, M.; Racine, C.A.; Martin, A.J.; Markun, L.C.; Larson, P.S. Clinical outcomes using ClearPoint interventional MRI for deep brain stimulation lead placement in Parkinson’s disease. J. Neurosurg. 2016, 124, 908–916. [Google Scholar] [CrossRef]
- Sidiropoulos, C.; Rammo, R.; Merker, B.; Mahajan, A.; LeWitt, P.; Kaminski, P.; Womble, M.; Zec, A.; Taylor, D.; Wall, J. Intraoperative MRI for deep brain stimulation lead placement in Parkinson’s disease: 1 year motor and neuropsychological outcomes. J. Neurol. 2016, 263, 1226–1231. [Google Scholar] [CrossRef]
- Chircop, C.; Dingli, N.; Aquilina, A.; Zrinzo, L.; Aquilina, J. MRI-verified “asleep” deep brain stimulation in Malta through cross border collaboration: Clinical outcome of the first five years. Br J. Neurosurg. 2018, 32, 365–371. [Google Scholar] [CrossRef]
- Matias, C.M.; Frizon, L.A.; Nagel, S.J.; Lobel, D.A.; Machado, A.G. Deep brain stimulation outcomes in patients implanted under general anesthesia with frame-based stereotaxy and intraoperative MRI. J. Neurosurg. 2018, 129, 1572–1578. [Google Scholar] [CrossRef]
- Mirzadeh, Z.; Chapple, K.; Lambert, M.; Evidente, V.G.; Mahant, P.; Ospina, M.C.; Samanta, J.; Moguel-Cobos, G.; Salins, N.; Lieberman, A.; et al. Parkinson’s disease outcomes after intraoperative CT-guided “asleep” deep brain stimulation in the globus pallidus internus. J. Neurosurg. 2016, 124, 902–907. [Google Scholar] [CrossRef]
- Hertel, F.; Züchner, M.; Weimar, I.; Gemmar, P.; Noll, B.; Bettag, M.; Decker, C. Implantation of electrodes fordeep brain stimulation of the subthalamic nucleus in advanced parkinson’s disease with the aid of intraoperative microrecording undergeneral anesthesia. Neurosurgery 2006, 59, E1138. [Google Scholar] [CrossRef] [PubMed]
- Lefaucheur, J.-P.; Gurruchaga, J.-M.; Pollin, B.; Von Raison, F.; Mohsen, N.; Shin, M.; Ménard-Lefaucheur, I.; Oshino, S.; Kishima, H.; Fénelon, G. Outcome of bilateral subthalamic nucleus stimulation in the treatment of Parkinson’s disease: Correlation with intra-operative multi-unit recordings but not with the type of anaesthesia. Eur. Neurol. 2008, 60, 186–199. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.H.; Chen, T.Y.; Lin, S.Z.; Shyr, M.H.; Chou, Y.C.; Hsieh, W.A.; Tsai, S.T.; Chen, S.Y. Subthalamic deep brain stimulation after anesthetic inhalation in Parkinson disease: A preliminary study. J. Neurosurg. 2008, 109, 238–244. [Google Scholar] [CrossRef] [PubMed]
- Fluchere, F.; Witjas, T.; Eusebio, A.; Bruder, N.; Giorgi, R.; Leveque, M.; Peragut, J.C.; Azulay, J.P.; Regis, J. Controlled general anaesthesia for subthalamic nucleus stimulation in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2014, 85, 1167–1173. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.K.; Heywood, P.; O’Sullivan, K.; Love, S.; Gill, S.S. MRI-directed subthalamic nucleus surgery for Parkinson’s disease. Stereotact. Funct. Neurosurg. 2002, 78, 132–145. [Google Scholar] [CrossRef] [PubMed]
- Burchiel, K.J.; McCartney, S.; Lee, A.; Raslan, A.M. Accuracy of deep brain stimulation electrode placement using intraoperative computed tomography without microelectrode recording. J. Neurosurg. 2013, 119, 301–306. [Google Scholar] [CrossRef]
- Mirzadeh, Z.; Chapple, K.; Lambert, M.; Dhall, R.; Ponce, F.A. Validation of CT-MRI fusion for intraoperative assessment of stereotactic accuracy in DBS surgery. Mov. Disord. 2014, 29, 1788–1795. [Google Scholar] [CrossRef]
- Zrinzo, L.; Foltynie, T.; Limousin, P.; Hariz, M. Image-guided and image-verified deep brain stimulation. Mov. Disord. 2013, 28, 254. [Google Scholar] [CrossRef]
- Ferroli, P.; Franzini, A.; Marras, C.; Maccagnano, E.; D’Incerti, L.; Broggi, G. A simple method to assess accuracy of deep brain stimulation electrode placement: Pre-operative stereotactic CT+ postoperative MR image fusion. Stereotact. Funct. Neurosurg. 2004, 82, 14–19. [Google Scholar] [CrossRef]
- Fiegele, T.; Feuchtner, G.; Sohm, F.; Bauer, R.; Anton, J.V.; Gotwald, T.; Twerdy, K.; Eisner, W. Accuracy of stereotactic electrode placement in deep brain stimulation by intraoperative computed tomography. Park. Relat. Disord. 2008, 14, 595–599. [Google Scholar] [CrossRef]
- Chen, T.; Mirzadeh, Z.; Chapple, K.M.; Lambert, M.; Shill, H.A.; Moguel-Cobos, G.; Troster, A.I.; Dhall, R.; Ponce, F.A. Clinical outcomes following awake and asleep deep brain stimulation for Parkinson disease. J. Neurosurg. 2018, 130, 109–120. [Google Scholar] [CrossRef]
- Ko, A.L.; Magown, P.; Ozpinar, A.; Hamzaoglu, V.; Burchiel, K.J. Asleep Deep Brain Stimulation Reduces Incidence of Intracranial Air during Electrode Implantation. Stereotact. Funct. Neurosurg. 2018, 96, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Cui, Z.; Pan, L.; Song, H.; Xu, X.; Xu, B.; Yu, X.; Ling, Z. Intraoperative MRI for optimizing electrode placement for deep brain stimulation of the subthalamic nucleus in Parkinson disease. J. Neurosurg. 2016, 124, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Mirzadeh, Z.; Ponce, F.A. "Asleep" Deep Brain Stimulation Surgery: A Critical Review of the Literature. World Neurosurg. 2017, 105, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Sheshadri, V.; Rowland, N.C.; Mehta, J.; Englesakis, M.; Manninen, P.; Venkatraghavan, L. Comparison of General and Local Anesthesia for Deep Brain Stimulator Insertion: A Systematic Review. Can. J. Neurol. Sci. 2017, 44, 697–704. [Google Scholar] [CrossRef]
- Bot, M.; van den Munckhof, P.; Bakay, R.; Stebbins, G.; Metman, L.V. Accuracy of intraoperative computed tomography during deep brain stimulation procedures: Comparison with postoperative magnetic resonance imaging. Stereotact. Funct. Neurosurg. 2017, 95, 183–188. [Google Scholar] [CrossRef]
- Kremer, N.I.; Oterdoom, D.L.M.; van Laar, P.J.; Piña-Fuentes, D.; van Laar, T.; Drost, G.; van Hulzen, A.L.J.; van Dijk, J.M.C. Accuracy of Intraoperative Computed Tomography in Deep Brain Stimulation-A Prospective Noninferiority Study. Neuromodul. Technol. Neural Interface 2019, 22, 472–477. [Google Scholar] [CrossRef]
- Harries, A.M.; Kausar, J.; Roberts, S.A.; Mocroft, A.P.; Hodson, J.A.; Pall, H.S.; Mitchell, R.D. Deep brain stimulation of the subthalamic nucleus for advanced Parkinson disease using general anesthesia: Long-term results. J. Neurosurg. 2012, 116, 107–113. [Google Scholar] [CrossRef]
- Kwon, W.K.; Kim, J.H.; Lee, J.H.; Lim, B.G.; Lee, I.O.; Koh, S.B.; Kwon, T.H. Microelectrode recording (MER) findings during sleep-awake anesthesia using dexmedetomidine in deep brain stimulation surgery for Parkinson’s disease. Clin. Neurol. Neurosurg. 2016, 143, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Warnke, P. Deep brain stimulation: Awake or asleep: It comes with a price either way. J. Neurol. Neurosurg. Psychiatry 2018, 89, 672. [Google Scholar] [CrossRef] [PubMed]
- Tsai, S.-T.; Kuo, C.-C.; Chen, T.-Y.; Chen, S.-Y. Neurophysiological comparisons of subthalamic deep-brain stimulation for Parkinson’s disease between patients receiving general and local anesthesia. Tzu Chi Med. J. 2016, 28, 63–67. [Google Scholar] [CrossRef] [PubMed]
- LaHue, S.C.; Ostrem, J.L.; Galifianakis, N.B.; San Luciano, M.; Ziman, N.; Wang, S.; Racine, C.A.; Starr, P.A.; Larson, P.S.; Katz, M. Parkinson’s disease patient preference and experience with various methods of DBS lead placement. Park. Relat. Disord. 2017, 41, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Yamada, K.; Goto, S.; Kuratsu, J.; Matsuzaki, K.; Tamura, T.; Nagahiro, S.; Murase, N.; Shimazu, H.; Kaji, R. Stereotactic surgery for subthalamic nucleus stimulation under general anesthesia: A retrospective evaluation of Japanese patients with Parkinson’s disease. Park. Relat. Disord. 2007, 13, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.Y.; Tsai, S.T.; Lin, S.H.; Chen, T.Y.; Hung, H.Y.; Lee, C.W.; Wang, W.H.; Chen, S.P.; Lin, S.Z. Subthalamic deep brain stimulation in Parkinson’s disease under different anesthetic modalities: A comparative cohort study. Stereotact. Funct. Neurosurg. 2011, 89, 372–380. [Google Scholar] [CrossRef] [PubMed]
- Asha, M.J.; Fisher, B.; Kausar, J.; Garratt, H.; Krovvidi, H.; Shirley, C.; White, A.; Chelvarajah, R.; Ughratdar, I.; Hodson, J.A. Subthalamic deep brain stimulation under general anesthesia and neurophysiological guidance while on dopaminergic medication: Comparative cohort study. Acta Neurochir. 2018, 160, 823–829. [Google Scholar] [CrossRef] [PubMed]
- Lettieri, C.; Rinaldo, S.; Devigili, G.; Pauletto, G.; Verriello, L.; Budai, R.; Fadiga, L.; Oliynyk, A.; Mondani, M.; D’Auria, S.; et al. Deep brain stimulation: Subthalamic nucleus electrophysiological activity in awake and anesthetized patients. Clin. Neurophysiol. Off. J. Int. Fed. Clin. Neurophysiol. 2012, 123, 2406–2413. [Google Scholar] [CrossRef] [PubMed]
- Maltête, D.; Navarro, S.; Welter, M.-L.; Roche, S.; Bonnet, A.-M.; Houeto, J.-L.; Mesnage, V.; Pidoux, B.; Dormont, D.; Cornu, P. Subthalamic stimulation in Parkinson disease: With or without anesthesia? Arch. Neurol. 2004, 61, 390–392. [Google Scholar] [CrossRef]
- Brodsky, M.A.; Anderson, S.; Murchison, C.; Seier, M.; Wilhelm, J.; Vederman, A.; Burchiel, K.J. Clinical outcomes of asleep vs awake deep brain stimulation for Parkinson disease. Neurology 2017, 89, 1944–1950. [Google Scholar] [CrossRef]
- Sharma, M.; Deogaonkar, M. Accuracy and safety of targeting using intraoperative “O-arm” during placement of deep brain stimulation electrodes without electrophysiological recordings. J. Clin. Neurosci. Off. J. Neurosurg. Soc. Australas 2016, 27, 80–86. [Google Scholar] [CrossRef]
- Carlson, J.D.; McLeod, K.E.; McLeod, P.S.; Mark, J.B. Stereotactic Accuracy and Surgical Utility of the O-Arm in Deep Brain Stimulation Surgery. Oper. Neurosurg. (Hagerstown) 2017, 13, 96–107. [Google Scholar] [CrossRef]
- Sillay, K.A.; Rusy, D.; Buyan-Dent, L.; Ninman, N.L.; Vigen, K.K. Wide-bore 1.5 T MRI-guided deep brain stimulation surgery: Initial experience and technique comparison. Clin. Neurol. Neurosurg. 2014, 127, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Aviles-Olmos, I.; Kefalopoulou, Z.; Tripoliti, E.; Candelario, J.; Akram, H.; Martinez-Torres, I.; Jahanshahi, M.; Foltynie, T.; Hariz, M.; Zrinzo, L. Long-term outcome of subthalamic nucleus deep brain stimulation for Parkinson’s disease using an MRI-guided and MRI-verified approach. J. Neurol. Neurosurg. Psychiatry 2014, 85, 1419–1425. [Google Scholar] [CrossRef] [PubMed]
- Chabardes, S.; Isnard, S.; Castrioto, A.; Oddoux, M.; Fraix, V.; Carlucci, L.; Payen, J.F.; Krainik, A.; Krack, P.; Larson, P. Surgical implantation of STN-DBS leads using intraoperative MRI guidance: Technique, accuracy, and clinical benefit at 1-year follow-up. Acta Neurochir. 2015, 157, 729–737. [Google Scholar] [CrossRef] [PubMed]
- Spiegelmann, R.; Nissim, O.; Daniels, D.; Ocherashvilli, A.; Mardor, Y. Stereotactic targeting of the ventrointermediate nucleus of the thalamus by direct visualization with high-field MRI. Stereotact. Funct. Neurosurg. 2006, 84, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.S.; Richardson, R.M. Interventional MRI-Guided Deep Brain Stimulation Lead Implantation. Neurosurg. Clin. N. Am. 2017, 28, 535–544. [Google Scholar] [CrossRef]
- Min, H.K.; Ross, E.K.; Lee, K.H.; Dennis, K.; Han, S.R.; Jeong, J.H.; Marsh, M.P.; Striemer, B.; Felmlee, J.P.; Lujan, J.L.; et al. Subthalamic nucleus deep brain stimulation induces motor network BOLD activation: Use of a high precision MRI guided stereotactic system for nonhuman primates. Brain Stimul. 2014, 7, 603–607. [Google Scholar] [CrossRef]
- Kochanski, R.B.; Sani, S. Awake versus Asleep Deep Brain Stimulation Surgery: Technical Considerations and Critical Review of the Literature. Brain Sci. 2018, 8, 17. [Google Scholar] [CrossRef]
- Kamiryo, T.; Laws, E.R., Jr. Stereotactic frame-based error in magnetic-resonance-guided stereotactic procedures: A method for measurement of error and standardization of technique. Stereotact. Funct. Neurosurg. 1996, 67, 198–209. [Google Scholar] [CrossRef]
- Ko, A.L.; Ibrahim, A.; Magown, P.; Macallum, R.; Burchiel, K.J. Factors affecting stereotactic accuracy in image-guided deep brain stimulator electrode placement. Stereotact. Funct. Neurosurg. 2017, 95, 315–324. [Google Scholar] [CrossRef]
- Chen, T.; Mirzadeh, Z.; Chapple, K.; Lambert, M.; Dhall, R.; Ponce, F.A. “Asleep” deep brain stimulation for essential tremor. J. Neurosurg. 2016, 124, 1842–1849. [Google Scholar] [CrossRef]
- Holloway, K.; Docef, A. A quantitative assessment of the accuracy and reliability of O-arm images for deep brain stimulation surgery. Neurosurgery 2013, 72, 47–57. [Google Scholar] [CrossRef] [PubMed]
- Geevarghese, R.; O’Gorman Tuura, R.; Lumsden, D.E.; Samuel, M.; Ashkan, K. Registration Accuracy of CT/MRI Fusion for Localisation of Deep Brain Stimulation Electrode Position: An Imaging Study and Systematic Review. Stereotact. Funct. Neurosurg. 2016, 94, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Ivan, M.E.; Yarlagadda, J.; Saxena, A.P.; Martin, A.J.; Starr, P.A.; Sootsman, W.K.; Larson, P.S. Brain shift during bur hole-based procedures using interventional MRI. J. Neurosurg. 2014, 121, 149–160. [Google Scholar] [CrossRef] [PubMed]
- Deuschl, G.; Schade-Brittinger, C.; Krack, P.; Volkmann, J.; Schäfer, H.; Bötzel, K.; Daniels, C.; Deutschländer, A.; Dillmann, U.; Eisner, W. A randomized trial of deep-brain stimulation for Parkinson’s disease. N. Engl. J. Med. 2006, 355, 896–908. [Google Scholar] [CrossRef]
- Erickson, K.M.; Cole, D.J. Anesthetic considerations for awake craniotomy for epilepsy. Anesthesiol. Clin. 2007, 25, 535–555, ix. [Google Scholar] [CrossRef]
- Grant, R.; Gruenbaum, S.E.; Gerrard, J. Anaesthesia for deep brain stimulation: A review. Curr. Opin. Anaesthesiol. 2015, 28, 505. [Google Scholar] [CrossRef]
- Khan, M.F.; Mewes, K.; Gross, R.E.; Skrinjar, O. Assessment of brain shift related to deep brain stimulation surgery. Stereotact. Funct. Neurosurg. 2008, 86, 44–53. [Google Scholar] [CrossRef]
- Pallavaram, S.; Dawant, B.M.; Remple, M.S.; Neimat, J.S.; Kao, C.; Konrad, P.E.; D’Haese, P.F. Effect of brain shift on the creation of functional atlases for deep brain stimulation surgery. Int. J. Comput. Assist. Radiol. Surg. 2010, 5, 221–228. [Google Scholar] [CrossRef]
- Elias, W.J.; Durieux, M.E.; Huss, D.; Frysinger, R.C. Dexmedetomidine and arousal affect subthalamic neurons. Mov. Disord. 2008, 23, 1317–1320. [Google Scholar] [CrossRef]
- Pollak, P.; Krack, P.; Fraix, V.; Mendes, A.; Moro, E.; Chabardes, S.; Benabid, A.L. Intraoperative micro- and macrostimulation of the subthalamic nucleus in Parkinson’s disease. Mov. Disord. 2002, 17 (Suppl. 3), S155–S161. [Google Scholar] [CrossRef]
- Gorgulho, A.; De Salles, A.A.; Frighetto, L.; Behnke, E. Incidence of hemorrhage associated with electrophysiological studies performed using macroelectrodes and microelectrodes in functional neurosurgery. J. Neurosurg. 2005, 102, 888–896. [Google Scholar] [CrossRef] [PubMed]
- Binder, D.K.; Rau, G.M.; Starr, P.A. Risk factors for hemorrhage during microelectrode-guided deep brain stimulator implantation for movement disorders. Neurosurgery 2005, 56, 722–732. [Google Scholar] [CrossRef] [PubMed]
- Vesper, J.; Haak, S.; Ostertag, C.; Nikkhah, G. Subthalamic nucleus deep brain stimulation in elderly patients--analysis of outcome and complications. BMC Neurol. 2007, 7, 7. [Google Scholar] [CrossRef] [PubMed]
- Guridi, J.; Rodriguez-Oroz, M.C.; Lozano, A.M.; Moro, E.; Albanese, A.; Nuttin, B.; Gybels, J.; Ramos, E.; Obeso, J.A. Targeting the basal ganglia for deep brain stimulation in Parkinson’s disease. Neurology 2000, 55, S21–S28. [Google Scholar]
- Houeto, J.-L.; Welter, M.-L.; Bejjani, P.-B.; du Montcel, S.T.; Bonnet, A.-M.; Mesnage, V.; Navarro, S.; Pidoux, B.; Dormont, D.; Cornu, P. Subthalamic stimulation in Parkinson disease: Intraoperative predictive factors. Arch. Neurol. 2003, 60, 690–694. [Google Scholar] [CrossRef][Green Version]
- Blasberg, F.; Wojtecki, L.; Elben, S.; Slotty, P.J.; Vesper, J.; Schnitzler, A.; Groiss, S.J. Comparison of Awake vs. Asleep Surgery for Subthalamic Deep Brain Stimulation in Parkinson’s Disease. Neuromodulation 2018, 21, 541–547. [Google Scholar] [CrossRef]
- Castrioto, A.; Marmor, O.; Deffains, M.; Willner, D.; Linetsky, E.; Bergman, H.; Israel, Z.; Eitan, R.; Arkadir, D. Anesthesia reduces discharge rates in the human pallidum without changing the discharge rate ratio between pallidal segments. Eur. J. Neurosci. 2016, 44, 2909–2913. [Google Scholar] [CrossRef]
- Moll, C.K.; Payer, S.; Gulberti, A.; Sharrott, A.; Zittel, S.; Boelmans, K.; Köppen, J.; Gerloff, C.; Westphal, M.; Engel, A.K. STN stimulation in general anaesthesia: Evidence beyond ‘evidence-based medicine’. In Stereotactic and Functional Neurosurgery; Springer: Berlin/Heidelberg, Germany, 2013; pp. 19–25. [Google Scholar]
- Sanghera, M.K.; Grossman, R.G.; Kalhorn, C.G.; Hamilton, W.J.; Ondo, W.G.; Jankovic, J. Basal ganglia neuronal discharge in primary and secondary dystonia in patients undergoing pallidotomy. Neurosurgery 2003, 52, 1358–1373. [Google Scholar] [CrossRef]
- Tsai, S.T.; Chuang, W.Y.; Kuo, C.C.; Chao, P.C.; Chen, T.Y.; Hung, H.Y.; Chen, S.Y. Dorsolateral subthalamic neuronal activity enhanced by median nerve stimulation characterizes Parkinson’s disease during deep brain stimulation with general anesthesia. J. Neurosurg. 2015, 123, 1394–1400. [Google Scholar] [CrossRef]
- Kim, W.; Song, I.H.; Lim, Y.H.; Kim, M.-R.; Kim, Y.E.; Hwang, J.H.; Kim, I.K.; Song, S.W.; Kim, J.W.; Lee, W.-W. Influence of propofol and fentanyl on deep brain stimulation of the subthalamic nucleus. J. Korean Med. Sci. 2014, 29, 1278–1286. [Google Scholar] [CrossRef]
- Lee, W.-W.; Ehm, G.; Yang, H.-J.; Song, I.H.; Lim, Y.H.; Kim, M.-R.; Kim, Y.E.; Hwang, J.H.; Park, H.R.; Lee, J.M. Bilateral deep brain stimulation of the subthalamic nucleus under sedation with propofol and fentanyl. PLoS ONE 2016, 11, e0152619. [Google Scholar] [CrossRef] [PubMed]
- Galvan, A.; Wichmann, T. GABAergic circuits in the basal ganglia and movement disorders. Prog. Brain Res. 2007, 160, 287–312. [Google Scholar] [PubMed]
- Raz, A.; Eimerl, D.; Zaidel, A.; Bergman, H.; Israel, Z. Propofol decreases neuronal population spiking activity in the subthalamic nucleus of Parkinsonian patients. Anesth. Analg. 2010, 111, 1285–1289. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.H.; Lai, H.Y.; Lo, Y.C.; Chou, C.; Chou, Y.T.; Yang, S.H.; Sun, I.; Chen, B.W.; Wang, C.F.; Liu, G.T.; et al. Decreased Power but Preserved Bursting Features of Subthalamic Neuronal Signals in Advanced Parkinson’s Patients under Controlled Desflurane Inhalation Anesthesia. Front. Neurosci. 2017, 11, 701. [Google Scholar] [CrossRef] [PubMed]
- Kouvaras, E.; Asprodini, E.K.; Asouchidou, I.; Vasilaki, A.; Kilindris, T.; Michaloudis, D.; Koukoutianou, I.; Papatheodoropoulos, C.; Kostopoulos, G. Fentanyl treatment reduces GABAergic inhibition in the CA1 area of the hippocampus 24 h after acute exposure to the drug. Neuropharmacology 2008, 55, 1172–1182. [Google Scholar] [CrossRef]
- Hutchison, W.D.; Lang, A.E.; Dostrovsky, J.O.; Lozano, A.M. Pallidal neuronal activity: Implications for models of dystonia. Ann. Neurol. 2003, 53, 480–488. [Google Scholar] [CrossRef]
- Khatib, R.; Ebrahim, Z.; Rezai, A.; Cata, J.P.; Boulis, N.M.; John Doyle, D.; Schurigyn, T.; Farag, E. Perioperative events during deep brain stimulation: The experience at cleveland clinic. J. Neurosurg. Anesthesiol. 2008, 20, 36–40. [Google Scholar] [CrossRef]
- Duque, P.; Mateo, O.; Ruiz, F.; de Viloria, J.G.; Contreras, A.; Grandas, F. Intraoperative microrecording under general anaesthesia with bispectral analysis monitoring in a case of deep brain stimulation surgery for Parkinson’s disease. Eur. J. Neurol. 2008, 15, e76–e77. [Google Scholar] [CrossRef]
- Lee, J.Y.; Deogaonkar, M.; Rezai, A. Deep brain stimulation of globus pallidus internus for dystonia. Park. Relat. Disord. 2007, 13, 261–265. [Google Scholar] [CrossRef]
- Morace, R.; De Angelis, M.; Aglialoro, E.; Maucione, G.; Cavallo, L.; Solari, D.; Modugno, N.; Santilli, M.; Esposito, V.; Aloj, F. Sedation with α2 Agonist Dexmedetomidine During Unilateral Subthalamic Nucleus Deep Brain Stimulation: A Preliminary Report. World Neurosurg. 2016, 89, 320–328. [Google Scholar] [CrossRef]
- Rozet, I. Anesthesia for functional neurosurgery: The role of dexmedetomidine. Curr. Opin. Anaesthesiol. 2008, 21, 537–543. [Google Scholar] [CrossRef] [PubMed]
- Sassi, M.; Zekaj, E.; Grotta, A.; Pollini, A.; Pellanda, A.; Borroni, M.; Pacchetti, C.; Menghetti, C.; Porta, M.; Servello, D. Safety in the use of dexmedetomidine (precedex) for deep brain stimulation surgery: Our experience in 23 randomized patients. Neuromodulation 2013, 16, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Hans, P.; Bonhomme, V.; Born, J.D.; Maertens de Noordhoudt, A.; Brichant, J.F.; Dewandre, P.Y. Target-controlled infusion of propofol and remifentanil combined with bispectral index monitoring for awake craniotomy. Anaesthesia 2000, 55, 255–259. [Google Scholar] [CrossRef] [PubMed]
- Johansen, J.W.; Sebel, P.S. Development and clinical application of electroencephalographic bispectrum monitoring. Anesthesiology 2000, 93, 1336–1344. [Google Scholar] [CrossRef] [PubMed]
- Sutcliffe, A.; Mitchell, R.; Gan, Y.; Mocroft, A.; Nightingale, P. General anaesthesia for deep brain stimulator electrode insertion in Parkinson’s disease. Acta Neurochir. 2011, 153, 621–627. [Google Scholar] [CrossRef]
- Tsai, S.-T.; Chen, T.-Y.; Lin, S.-H.; Chen, S.-Y. Five-year clinical outcomes of local versus general anesthesia deep brain stimulation for Parkinson’s disease. Parkinson’s Dis. 2019, 2019, 5676345. [Google Scholar] [CrossRef]
- Martin, A.J.; Larson, P.S.; Ziman, N.; Levesque, N.; Volz, M.; Ostrem, J.L.; Starr, P.A. Deep brain stimulator implantation in a diagnostic MRI suite: Infection history over a 10-year period. J. Neurosurg. 2017, 126, 108–113. [Google Scholar] [CrossRef]
- Chen, T.; Mirzadeh, Z.; Chapple, K.; Lambert, M.; Ponce, F.A. Complication rates, lengths of stay, and readmission rates in “awake” and “asleep” deep brain simulation. J. Neurosurg. 2017, 127, 360–369. [Google Scholar] [CrossRef]
- Jacob, R.L.; Geddes, J.; McCartney, S.; Burchiel, K.J. Cost analysis of awake versus asleep deep brain stimulation: A single academic health center experience. J. Neurosurg. 2016, 124, 1517–1523. [Google Scholar] [CrossRef]
- Lefranc, M.; Zouitina, Y.; Tir, M.; Merle, P.; Ouendo, M.; Constans, J.M.; Godefroy, O.; Peltier, J.; Krystkowiak, P. Asleep Robot-Assisted Surgery for the Implantation of Subthalamic Electrodes Provides the Same Clinical Improvement and Therapeutic Window as Awake Surgery. World Neurosurg. 2017, 106, 602–608. [Google Scholar] [CrossRef]
- Liu, Z.; He, S.; Li, L. General Anesthesia versus Local Anesthesia for Deep Brain Stimulation in Parkinson’s Disease: A Meta-Analysis. Stereotact. Funct. Neurosurg. 2019, 97, 381–390. [Google Scholar] [CrossRef] [PubMed]
- Paek, S.H.; Han, J.H.; Lee, J.Y.; Kim, C.; Jeon, B.S.; Kim, D.G. Electrode position determined by fused images of preoperative and postoperative magnetic resonance imaging and surgical outcome after subthalamic nucleus deep brain stimulation. Neurosurgery 2008, 63, 925–936, discussion 936–927. [Google Scholar] [CrossRef] [PubMed]
- Paek, S.H.; Yun, J.Y.; Song, S.W.; Kim, I.K.; Hwang, J.H.; Kim, J.W.; Kim, H.J.; Kim, H.J.; Kim, Y.E.; Lim, Y.H.; et al. The clinical impact of precise electrode positioning in STN DBS on three-year outcomes. J. Neurol. Sci. 2013, 327, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Ryu, S.I.; Romanelli, P.; Heit, G. Asymptomatic transient MRI signal changes after unilateral deep brain stimulation electrode implantation for movement disorder. Stereotact. Funct. Neurosurg. 2004, 82, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Englot, D.J.; Glastonbury, C.M.; Larson, P.S. Abnormal T2-weighted MRI signal surrounding leads in a subset of deep brain stimulation patients. Stereotact. Funct. Neurosurg. 2011, 89, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Fenoy, A.J.; Villarreal, S.J.; Schiess, M.C. Acute and subacute presentations of cerebral edema following deep brain stimulation lead implantation. Stereotact. Funct. Neurosurg. 2017, 95, 86–92. [Google Scholar] [CrossRef]
- Deogaonkar, M.; Nazzaro, J.M.; Machado, A.; Rezai, A. Transient, symptomatic, post-operative, non-infectious hypodensity around the deep brain stimulation (DBS) electrode. J. Clin. Neurosci. 2011, 18, 910–915. [Google Scholar] [CrossRef]
- Holewijn, R.A.; Verbaan, D.; de Bie, R.M.A.; Schuurman, P.R. General Anesthesia versus Local Anesthesia in StereotaXY (GALAXY) for Parkinson’s disease: Study protocol for a randomized controlled trial. Trials 2017, 18, 417. [Google Scholar] [CrossRef]
- Little, S.; Pogosyan, A.; Neal, S.; Zavala, B.; Zrinzo, L.; Hariz, M.; Foltynie, T.; Limousin, P.; Ashkan, K.; FitzGerald, J. Adaptive deep brain stimulation in advanced Parkinson disease. Ann. Neurol. 2013, 74, 449–457. [Google Scholar] [CrossRef]
- Little, S.; Beudel, M.; Zrinzo, L.; Foltynie, T.; Limousin, P.; Hariz, M.; Neal, S.; Cheeran, B.; Cagnan, H.; Gratwicke, J. Bilateral adaptive deep brain stimulation is effective in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2016, 87, 717–721. [Google Scholar] [CrossRef]
- Higuchi, Y.; Matsuda, S.; Serizawa, T. Gamma knife radiosurgery in movement disorders: Indications and limitations. Mov. Disord. 2017, 32, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Friedman, J.H.; Epstein, M.; Sanes, J.N.; Lieberman, P.; Cullen, K.; Lindquist, C.; Daamen, M. Gamma knife pallidotomy in advanced Parkinson’s disease. Ann. Neurol. 1996, 39, 535–538. [Google Scholar] [CrossRef] [PubMed]
- Magara, A.; Bühler, R.; Moser, D.; Kowalski, M.; Pourtehrani, P.; Jeanmonod, D. First experience with MR-guided focused ultrasound in the treatment of Parkinson’s disease. J. Ther. Ultrasound 2014, 2, 11. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Fernández, R.; Rodríguez-Rojas, R.; Del Álamo, M.; Hernández-Fernández, F.; Pineda-Pardo, J.A.; Dileone, M.; Alonso-Frech, F.; Foffani, G.; Obeso, I.; Gasca-Salas, C. Focused ultrasound subthalamotomy in patients with asymmetric Parkinson’s disease: A pilot study. Lancet Neurol. 2018, 17, 54–63. [Google Scholar] [CrossRef]


| Author | Year | No. of Patients | Age (yrs) | Disease Duration (yrs) | Follow-Up Months | UPDRS III Medication Off | LEDD | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Follow-Up * | % Change | p-Value | Baseline | Follow-Up * | % Change | p-Value | ||||||
| Intraoperative imaging | |||||||||||||
| Interventional MRI | |||||||||||||
| Starr et al. [22] | 2010 | 29 | 58 ± 8.1 | NR | 9 | 49 ± 13 | 19 ±14 | 60% | 0.0001 | NR | NR | NR | NR |
| Foltynie et al. [23] | 2011 | 79 | 58.9± 7.7 | 11.5 ± 7 | 14 | 51.5 ± 14.9 | 23.8 ± 11.2 | 52% | 0.0001 | NR | NR | NR | NR |
| Nakajima et al. [24] | 2011 | 14 | 56.1 ± 6.5 | 13.8 ± 8.1 | 12 ± 6.1 | 57.9 ± 16.6 | 27.3 ± 11.8 | 53% | 0.0001 | 1505 ± 764 | 764 ± 435 | 49.20% | <0.01 |
| Ostrem et al. [25] | 2013 | 17 | 59.8 | 11.1 | 6 | 44.5 ± NA | 22.5 | 49.44% | 0.001 | 1337 ± 482 | NR | 24.70% | 0.003 |
| Saleh et al. [26] | 2015 | 14 | 64 ± 11.9 | 10.9 ± 3.8 | 5.86 ± 1.15 | NR | NR | NR | NR | NR | NR | 49.27% | 0.0031 |
| Ostrem et al. [27] | 2016 | 20 | 63.2 ± 6.8 | 10.8 ± 2.9 | 12 | 40.75 ± 10.9 | 24.35 ± 8.8 | 40.20% | 0.001 | 1072.5 ± 382 | 828.25 ± 492 | 21.13% | 0.046 |
| Sidiropoulous et al. [28] | 2016 | 12 | 64.7 ± 5.9 | 11.9 ± 3.7 | 13.5 ± 3.7 | 37.2 | 20.2 | 46.2% | 0.03 | 1458 ± 653 | 1337 ± 733 | 8.3% | 0.7 |
| Chircop et al. [29] | 2018 | 26 | 60.2 ± 9.3 | 8.8 ± 2.7 | 12 | 45.9 ± 14.3 | 26.7 ± 11.5 | 41.70% | <0.001 | 863 ± 211 | 599 ± 273 | 30.60% | <0.001 |
| Matias et al. [30] | 2018 | 33 | 67.2 ± 6.4 | 12.7 ± 6.9 | 9.1 | 52.8 ± 14.9 | 28.6 ± 11.9 | 45.8% | <0.001 | NR | NR | NR | NR |
| Intraoperative CT | |||||||||||||
| Mirzadeh et al. [31] | 2016 | 35 | 61.1 | 10.7 | 6 | 48.4 ± 13.8 | 28.9 ± 12.5 | 40.30% | <0.0001 | 1207 ± 733 | 1035 ± 478 | 14% | 0.004 |
| Microelectrode recording | |||||||||||||
| Hertel et al. [32] | 2006 | 9 | 70.7 ± 3.6 | 13.6 ± 6.0 | 3 | 43.0 ± NR | 19 ± NR | 55.80% | NR | NR | NR | NR | NR |
| Lefaucheur et al. [33] | 2008 | 30 | 57.7 ± 11.1 | 14.0 ± 4.0 | 12 | 47.9 ± 13.6 | 48.6 ± 19.0 | 69.10% | 0.87 | 1470.8 ± 729.5 | NR | 66.4 ± 17.2 | NR |
| Lin et al. [34] | 2008 | 10 | 58.9 ± 9.9 | 8.8 ± 3.7 | 6 | 50.2 ± 12.9 | 25.6 ± 11.68 | 48.85% | <0.05 | NR | NR | NR | NR |
| Fluchere et al. [35] | 2014 | 188 | 61 ± 7 | 12 ± 4 | 12 | 33.6 ± 13.3 | 13.2 ± 9.1 | 61.00% | <0.001 | 1173 ± 495 | 636 ± 376 | 46.00% | <0.001 |
| This study | 2020 | 90 | 57.43 ± 7.85 | 11.67 ± 4.75 | 6 | 38.11 ± 13.96 | 21.48 ± 12.33 | 43.60% | <0.001 | 1448.0 ± 546.93 | 483.99 ± 330.42 | 66.60% | <0.001 |
| Medication | General Anesthesia (n = 90) | Local Anesthesia (n = 56) | p Value | |
|---|---|---|---|---|
| Patient characteristics | ||||
| Age | 57.43 ± 7.85 | 58.91 ± 8.65 | 0.2893 | |
| Sex | 0.8110 | |||
| Male | 42(46.67%) | 25(44.64%) | ||
| Female | 48(53.33%) | 31(55.36%) | ||
| Symptom duration | 11.67 ± 4.75 | 10.55 ± 4.89 | 0.1753 | |
| Medication duration | 9.82 ± 3.89 | 8.98 ± 3.81 | 0.2027 | |
| Baseline measurement | ||||
| Total UPDRS | On | 31.86 ± 16.96 | 32.87 ± 17.76 | 0.7315 |
| Off | 65.93 ± 20.42 | 68.53 ± 20.34 | 0.4569 | |
| UPDRS Part III | On | 20.83 ± 10.96 | 21.40 ± 12.90 | 0.7764 |
| Off | 38.11 ± 13.96 | 40.42 ± 15.30 | 0.3521 | |
| H & Y | On | 2.36 ± 0.63 | 2.30 ± 0.63 | 0.6280 |
| Off | 3.05 ± 0.82 | 3.24 ± 0.91 | 0.1918 | |
| ADL | On | 82.89 ± 16.86 | 80.27 ± 15.45 | 0.3474 |
| Off | 47.44 ± 23.54 | 50.00 ± 22.18 | 0.5154 | |
| Dyskinesia Disability | 2.72 ± 1.31 | 2.21 ± 1.39 | 0.0294 * | |
| LEDD (mg/day) | 1448.00 ± 546.93 | 1031.63 ± 451.08 | <0.0001 * | |
| MMSE | 27.61 ± 2.52 | 26.53 ± 2.76 | 0.0273 * | |
| BDI | 17.72 ± 10.28 | 19.00 ± 10.82 | 0.4931 | |
| SF-36 Physical health | 156.25 ± 72.58 | 132.86 ± 61.09 | 0.0493 * | |
| SF-36 Mental health | 177.62 ± 80.37 | 150.39 ± 72.59 | 0.0433 * |
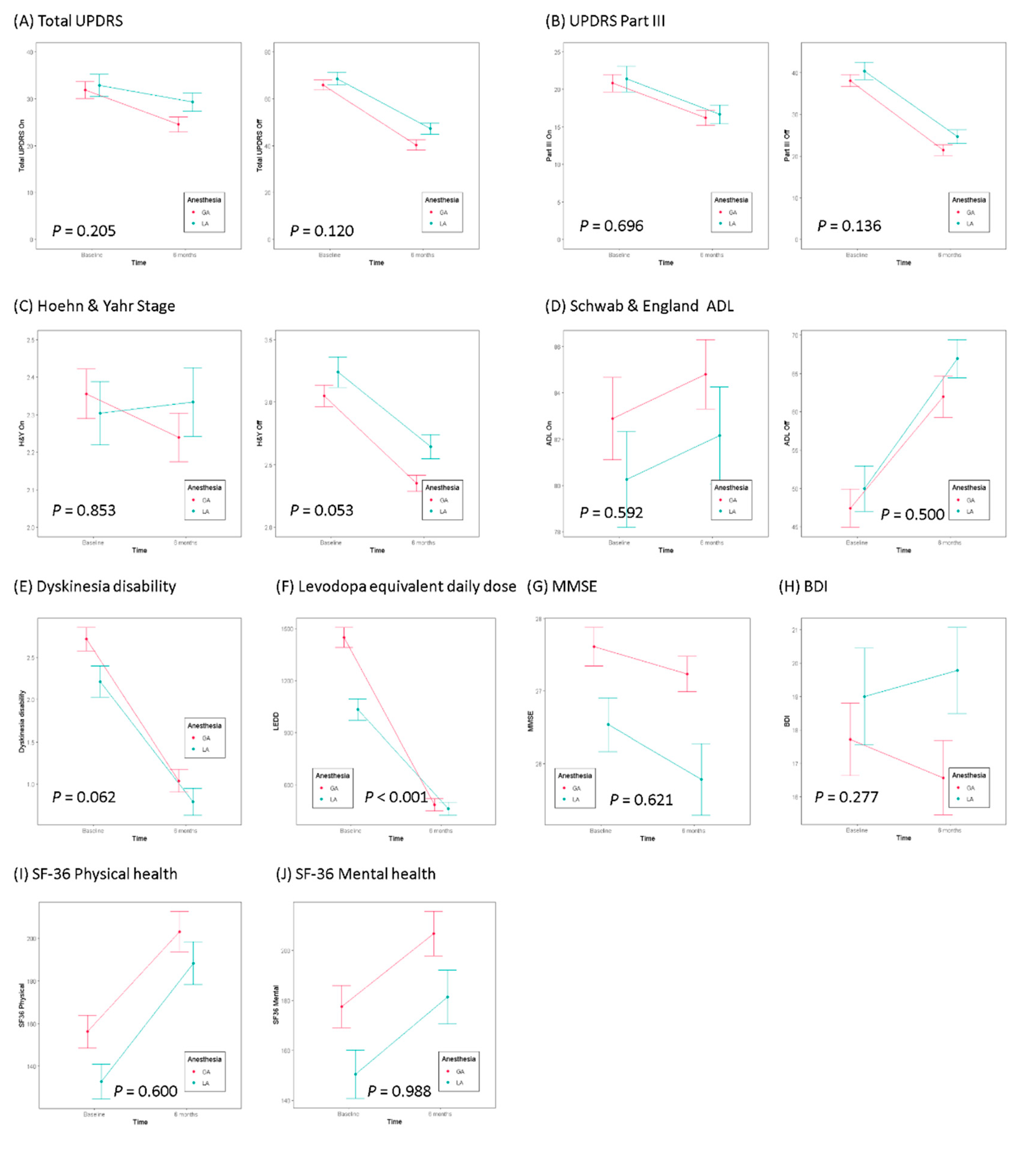
| Medication | Anesthesia | Baseline | 6 Month * | p Value ** | p Value *** | |
|---|---|---|---|---|---|---|
| Total UPDRS | On | General | 31.86 ± 16.96 | 24.53 ± 14.95 | 0.004 | 0.205 |
| Local | 32.87 ± 17.76 | 29.29 ± 14.19 | 0.429 | |||
| Off | General | 65.93 ± 20.42 | 40.32 ± 21.42 | <0.001 | 0.120 | |
| Local | 68.53 ± 20.34 | 47.26 ± 17.85 | <0.001 | |||
| UPDRS Part III | On | General | 20.83 ± 10.96 | 16.20 ± 9.46 | 0.005 | 0.696 |
| Local | 21.40 ± 12.90 | 16.67 ± 9.35 | 0.063 | |||
| Off | General | 38.11 ± 13.96 | 21.48 ± 12.33 | <0.001 | 0.136 | |
| Local | 40.42 ± 15.30 | 24.68 ± 12.51 | <0.001 | |||
| H & Y | On | General | 2.36 ± 0.63 | 2.24 ± 0.61 | 0.238 | 0.853 |
| Local | 2.3 ± 0.63 | 2.33 ± 0.68 | 0.959 | |||
| Off | General | 3.05 ± 0.82 | 2.35 ± 0.61 | <0.001 | 0.053 | |
| Local | 3.24 ± 0.91 | 2.64 ± 0.72 | 0.002 | |||
| ADL | On | General | 82.89 ± 16.86 | 84.80 ± 14.22 | 0.435 | 0.592 |
| Local | 80.27 ± 15.45 | 82.16 ± 15.66 | 0.247 | |||
| Off | General | 47.44 ± 23.54 | 61.98 ± 25.58 | <0.001 | 0.500 | |
| Local | 50 ± 22.18 | 66.92 ± 18.53 | <0.001 | |||
| Dyskinesia Disability | General | 2.72 ± 1.31 | 1.04 ± 1.27 | <0.001 | 0.062 | |
| Local | 2.21 ± 1.39 | 0.79 ± 1.21 | <0.001 | |||
| LEDD (mg/day) | General | 1448.00 ± 546.93 | 483.99 ± 330.42 | <0.001 | 0.000 | |
| Local | 1031.63 ± 451.08 | 461.3 ± 284.65 | <0.001 | |||
| MMSE | General | 27.61 ± 2.52 | 27.23 ± 2.33 | 0.314 | 0.621 | |
| Local | 26.53 ± 2.76 | 25.78 ± 3.71 | 0.493 | |||
| BDI | General | 17.72 ± 10.28 | 16.57 ± 10.56 | 0.473 | 0.277 | |
| Local | 19 ± 10.82 | 19.78 ± 9.68 | 0.524 | |||
| SF-36 Physical health | General | 156.25 ± 72.58 | 203.14 ± 90.03 | <0.001 | 0.600 | |
| Local | 132.86 ± 61.09 | 188.34 ± 74.5 | <0.001 | |||
| SF-36 Mental health | General | 177.62 ± 80.37 | 206.88 ± 84.62 | 0.021 | 0.988 | |
| Local | 150.39 ± 72.59 | 181.44 ± 80.95 | 0.076 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, H.R.; Lim, Y.H.; Song, E.J.; Lee, J.M.; Park, K.; Park, K.H.; Lee, W.-W.; Kim, H.-J.; Jeon, B.; Paek, S.H. Bilateral Subthalamic Nucleus Deep Brain Stimulation under General Anesthesia: Literature Review and Single Center Experience. J. Clin. Med. 2020, 9, 3044. https://doi.org/10.3390/jcm9093044
Park HR, Lim YH, Song EJ, Lee JM, Park K, Park KH, Lee W-W, Kim H-J, Jeon B, Paek SH. Bilateral Subthalamic Nucleus Deep Brain Stimulation under General Anesthesia: Literature Review and Single Center Experience. Journal of Clinical Medicine. 2020; 9(9):3044. https://doi.org/10.3390/jcm9093044
Chicago/Turabian StylePark, Hye Ran, Yong Hoon Lim, Eun Jin Song, Jae Meen Lee, Kawngwoo Park, Kwang Hyon Park, Woong-Woo Lee, Han-Joon Kim, Beomseok Jeon, and Sun Ha Paek. 2020. "Bilateral Subthalamic Nucleus Deep Brain Stimulation under General Anesthesia: Literature Review and Single Center Experience" Journal of Clinical Medicine 9, no. 9: 3044. https://doi.org/10.3390/jcm9093044
APA StylePark, H. R., Lim, Y. H., Song, E. J., Lee, J. M., Park, K., Park, K. H., Lee, W.-W., Kim, H.-J., Jeon, B., & Paek, S. H. (2020). Bilateral Subthalamic Nucleus Deep Brain Stimulation under General Anesthesia: Literature Review and Single Center Experience. Journal of Clinical Medicine, 9(9), 3044. https://doi.org/10.3390/jcm9093044