Neural Networks to Predict Radiographic Brain Injury in Pediatric Patients Treated with Extracorporeal Membrane Oxygenation

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Oversight
2.2. Patients
2.3. Brain Injury and Neuroimaging
2.4. Data Collection and Sources
2.5. Data Organization
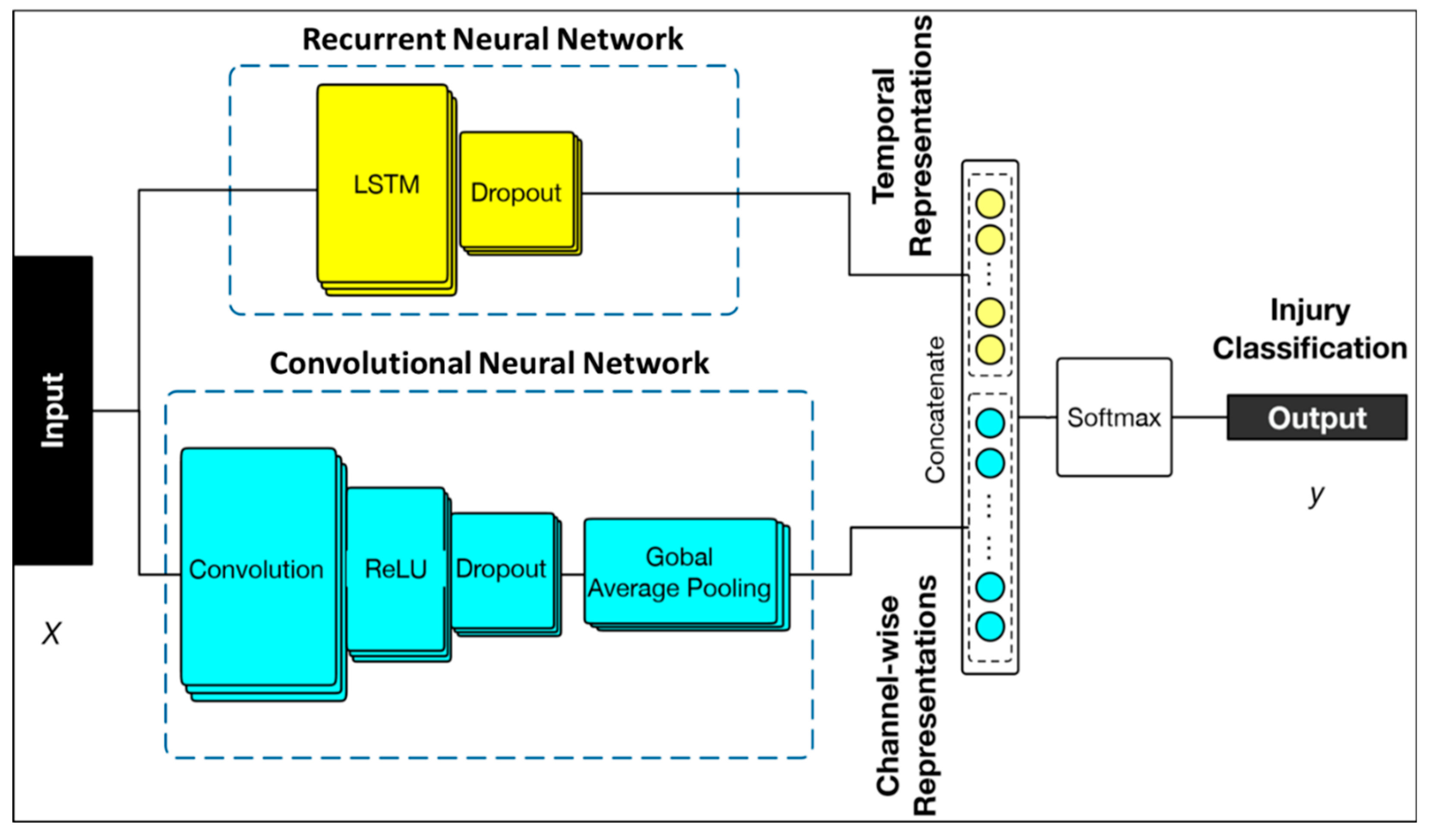
2.6. Machine Learning Methods
2.7. Clinician Suspicion for Injury
2.8. Logistic Regression
3. Results
3.1. Patients
3.2. Injury Prediction Based on Neural Networks
3.3. Clinician Suspicion for Injury
3.4. Injury Prediction Based on Conventional Methods
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable Group | Included Variables | ||||||
|---|---|---|---|---|---|---|---|
| Acid-Base | Arterial pH | Arterial CO2 (pCO2) | Arterial Oxygen (pO2) | Base Excess | |||
| Coagulation | International Normalized Ratio (INR) | Prothrombin time (PTT) | Platelet count | Fibrinogen | Hemoglobin | Free Hemoglobin | Heparin drip infusion rate (units/kg/h) |
| Machine Factors | Pre-oxygenator pressure | Post-oxygenator pressure | Pressure at Volume sensor | Measured flow (mL/kg/h) | Oxygenator FiO2 | Sweep (L/min) | |
| Markers of End-Organ Perfusion | Alanine aminotransferase (ALT) | Aspartate aminotransferase (AST) | Creatinine | Lactate | Bilirubin | * Glucose | |
| Vasoactive Medications | Epinephrine (mcg/kg/min) | Dopamine (mcg/kg/min) | Norepinephrine (mcg/kg/min) | Milrinone (mcg/kg/min) | Vasopressin (units/kg/h) | Vasoactive Infusion Score (VIS) | |
| Physiological Data | Systolic blood pressure | Diastolic blood pressure | Mean blood pressure | SpO2 | Heart Rate | Temp (°C) | |
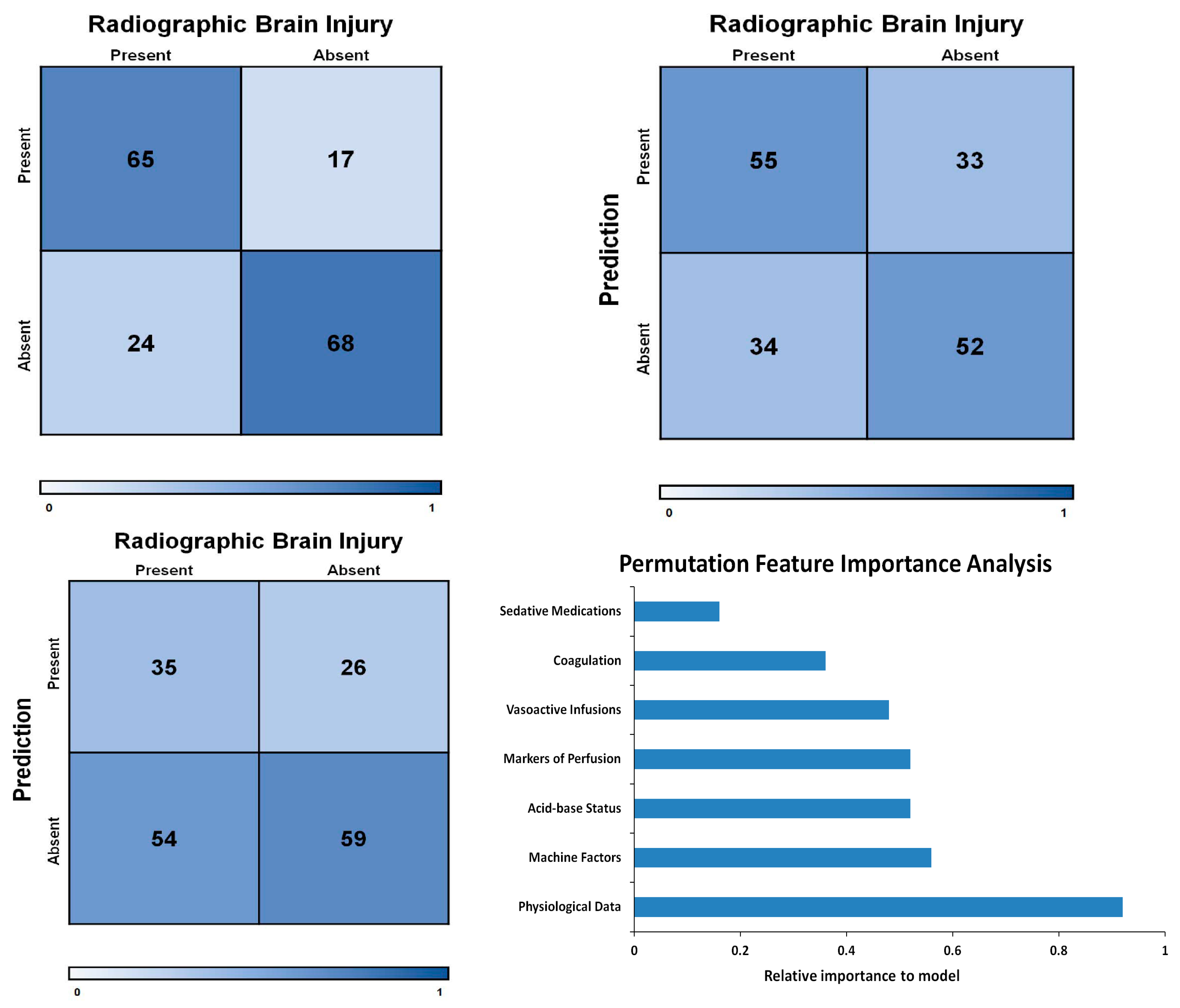
| Data Group | Magnitude of Importance |
|---|---|
| Acid-base | 0.52 |
| Coagulation | 0.36 |
| Machine factors | 0.56 |
| Markers of perfusion | 0.52 |
| Vasoactives | 0.48 |
| Physiological data | 0.92 |
| Model | Sensitivity | Specificity | PPV | NPV | +LR | −LR | AUC |
|---|---|---|---|---|---|---|---|
| Complete Model | 73% | 80% | 78% | 75% | 3.65 | 0.38 | 0.76 |
| Alternate assessments: | |||||||
| Clinician suspicion | 39% | 69% | 57% | 52% | 1.29 | 0.87 | 0.54 |
| Logistic Regression | 62% | 61% | 63% | 60% | 1.59 | 0.62 | 0.61 |
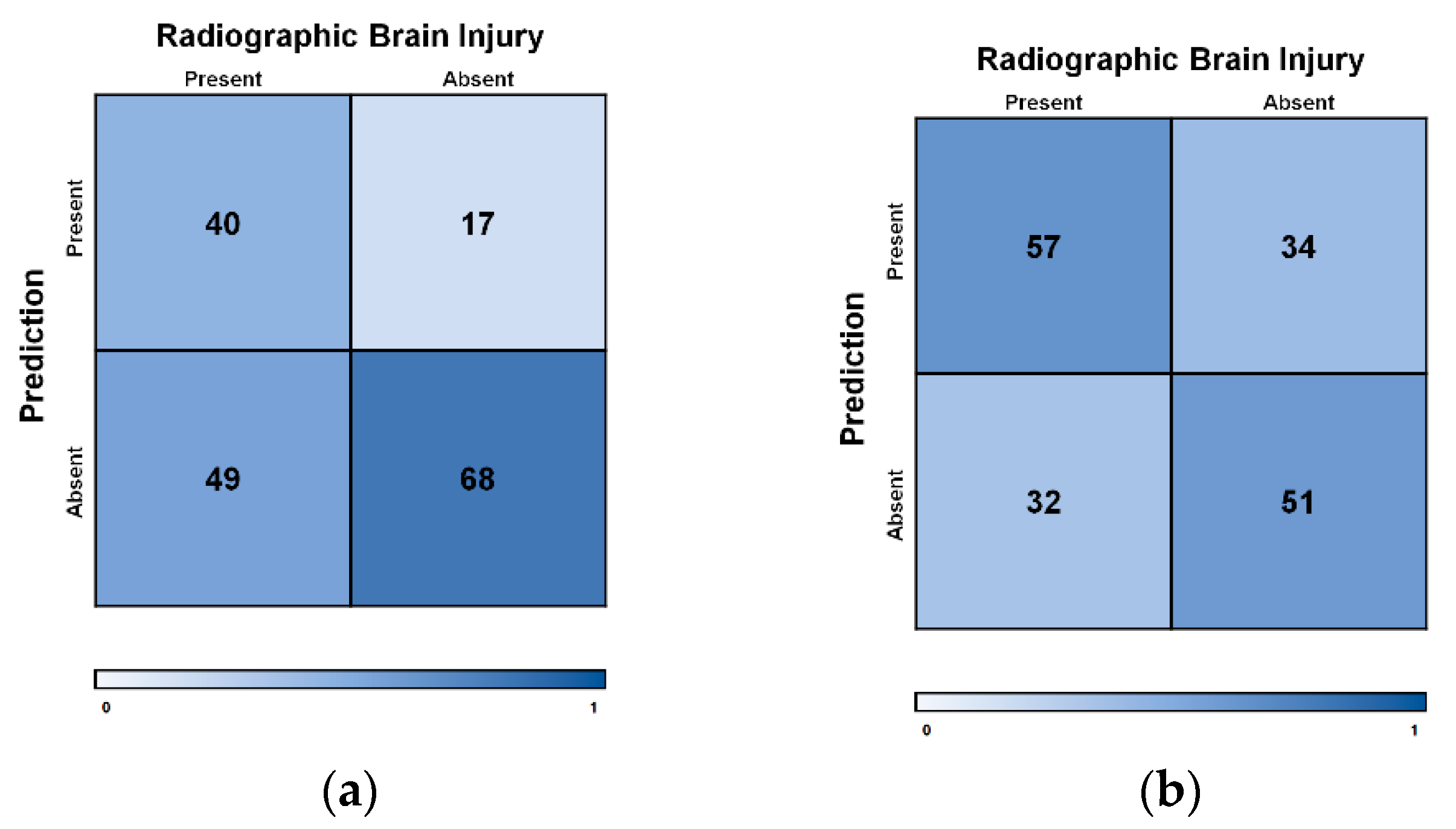
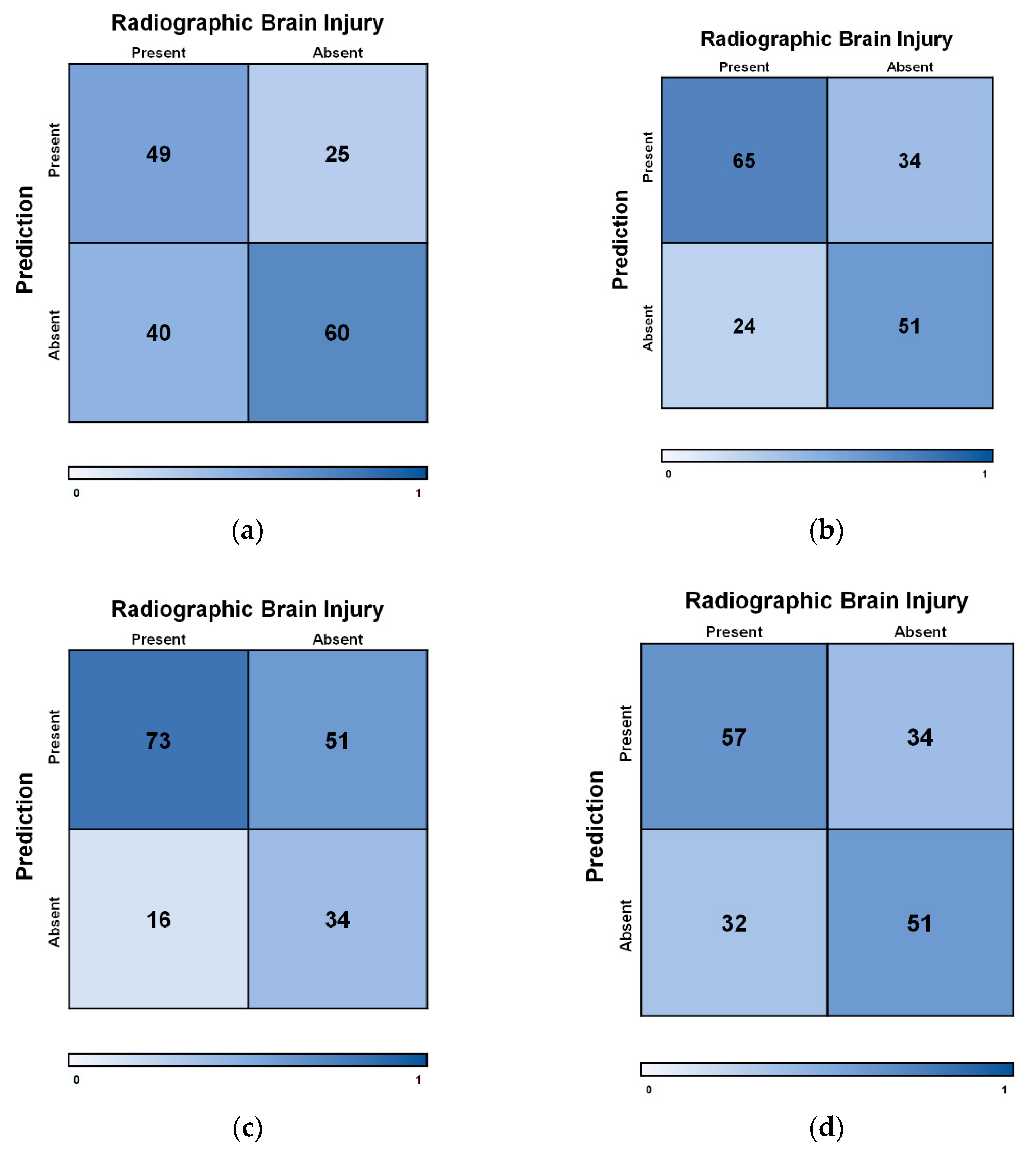
| Permutation feature importance and data-groups excluded: | |||||||
| Acid-base | 55% | 71% | 66% | 60% | 1.87 | 0.64 | 0.62 |
| Coagulation | 73% | 60% | 66% | 68% | 1.83 | 0.45 | 0.67 |
| Machine factors | 82% | 40% | 59% | 68% | 1.37 | 0.45 | 0.61 |
| Markers of perfusion | 64% | 60% | 63% | 62% | 1.60 | 0.60 | 0.62 |
| Vasoactives | 55% | 70% | 66% | 60% | 1.87 | 0.64 | 0.63 |
| Physiological data | 55% | 51% | 54% | 52% | 1.11 | 0.90 | 0.53 |



References
- Extracorporeal Life Support Organization-ECMO and ECLS > Registry > Statistics > International Summary. Available online: https://www.elso.org/Registry/Statistics/InternationalSummary.aspx (accessed on 13 July 2020).
- Jenks, C.L.; Raman, L.; Dalton, H.J. Pediatric Extracorporeal Membrane Oxygenation. Crit. Care Clin. 2017, 33, 825–841. [Google Scholar] [CrossRef] [PubMed]
- Lorusso, R.; Gelsomino, S.; Parise, O.; Di Mauro, M.; Barili, F.; Geskes, G.; Vizzardi, E.; Rycus, P.T.; Muellenbach, R.; Muellenbach, R.; et al. Neurologic Injury in Adults Supported With Veno-venous Extracorporeal Membrane Oxygenation for Respiratory Failure: Findings From the Extracorporeal Life Support Organization Database. Crit. Care Med. 2017, 45, 1389–1397. [Google Scholar] [CrossRef] [PubMed]
- Polito, A.; Barrett, C.S.; Wypij, D.; Rycus, P.T.; Netto, R.; Cogo, P.E.; Thiagarajan, R.R. Neurologic complications in neonates supported with extracorporeal membrane oxygenation. An analysis of ELSO registry data. Intensive Care Med. 2013, 39, 1594–1601. [Google Scholar] [CrossRef] [PubMed]
- Madderom, M.J.; Reuser, J.J.C.M.; Utens, E.M.W.J.; van Rosmalen, J.; Raets, M.; Govaert, P.; Steiner, K.; Gischler, S.J.; Tibboel, D.; van Heijst, A.F.J.; et al. Neurodevelopmental, educational and behavioral outcome at 8 years after neonatal ECMO: A nationwide multicenter study. Intensive Care Med. 2013, 39, 1584–1593. [Google Scholar] [CrossRef]
- Boyle, K.; Felling, R.; Yiu, A.; Battarjee, W.; Schwartz, J.M.; Salorio, C.; Bembea, M.M. Neurologic Outcomes After Extracorporeal Membrane Oxygenation: A Systematic Review. Pediatr. Crit. Care Med. 2018, 19, 760–766. [Google Scholar] [CrossRef]
- Bembea, M.M.; Felling, R.J.; Caprarola, S.D.; Ng, D.K.; Tekes, A.; Boyle, K.; Yiu, A.; Rizkalla, N.; Schwartz, J.; Everett, A.D.; et al. Neurologic Outcomes in a Two-Center Cohort of Neonatal and Pediatric Patients Supported on Extracorporeal Membrane Oxygenation. ASAIO J. 2020, 66, 79–88. [Google Scholar] [CrossRef]
- Waitzer, E.; Riley, S.P.; Perreault, T.; Shevell, M.I. Neurologic Outcome at School Entry for Newborns Treated With Extracorporeal Membrane Oxygenation for Noncardiac Indications. J. Child Neurol. 2009, 24, 801–806. [Google Scholar] [CrossRef]
- Barbaro, R.P.; Bartlett, R.H.; Chapman, R.L.; Paden, M.L.; Roberts, L.A.; Gebremariam, A.; Annich, G.M.; Davis, M.M. Development and validation of the neonatal risk estimate score for children using extracorporeal respiratory support. J. Pediatr. 2016, 173, 56.e3–61.e3. [Google Scholar] [CrossRef]
- Anton-Martin, P.; Raman, L.; Thatte, N.; Tweed, J.; Modem, V.; Journeycake, J. Pre-ECMO Coagulopathy does not Increase the Occurrence of Hemorrhage during Extracorporeal Support. Int. J. Artif. Organs 2017, 40, 250–255. [Google Scholar] [CrossRef]
- Park, S.J.; Kim, S.; Kim, J.B.; Jung, S.-H.; Choo, S.J.; Chung, C.H.; Lee, J.W. Blood lactate level during extracorporeal life support as a surrogate marker for survival. J. Thorac. Cardiovasc. Surg. 2014, 148, 714–720. [Google Scholar] [CrossRef]
- Kolodziej, A.; Burchett, A.; Tribble, T.; Grigorian, A.Y.; Guglin, M. Lactic Acid Is the Most Important Factor Predicting Survival on VA ECMO. J. Heart Lung Transplant. 2017, 36, S347. [Google Scholar] [CrossRef]
- Akin, S.; Caliskan, K.; Soliman, O.; Muslem, R.; Guven, G.; van Thiel, R.J.; Struijs, A.; Gommers, D.; Zijlstra, F.; Bakker, J. A novel mortality risk score predicting intensive care mortality in cardiogenic shock patients treated with veno-arterial extracorporeal membrane oxygenation. J. Crit. Care 2020, 55, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Bailly, D.K.; Reeder, R.W.; Zabrocki, L.A.; Hubbard, A.M.; Wilkes, J.; Bratton, S.L.; Thiagarajan, R.R. Development and Validation of a Score to Predict Mortality in Children Undergoing Extracorporeal Membrane Oxygenation for Respiratory Failure: Pediatric Pulmonary Rescue With Extracorporeal Membrane Oxygenation Prediction Score. Crit. Care Med. 2017, 45, e58–e66. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Majewicz Fey, A. Deep learning with convolutional neural network for objective skill evaluation in robot-assisted surgery. Int. J. Comput. Assist. Radiol. Surg. 2018, 13, 1959–1970. [Google Scholar] [CrossRef]
- Kidwell, C.S.; Chalela, J.A.; Saver, J.L.; Starkman, S.; Hill, M.D.; Demchuk, A.M.; Butman, J.A.; Patronas, N.; Alger, J.R.; Latour, L.L.; et al. Comparison of MRI and CT for Detection of Acute Intracerebral Hemorrhage. JAMA 2004, 292, 1823–1830. [Google Scholar] [CrossRef]
- Lidegran, M.K.; Mosskin, M.; Ringertz, H.G.; Frenckner, B.P.; Lindén, V.B. Cranial CT for diagnosis of intracranial complications in adult and pediatric patients during ECMO: Clinical benefits in diagnosis and treatment. Acad. Radiol. 2007, 14, 62–71. [Google Scholar] [CrossRef]
- Chalela, J.A.; Kidwell, C.S.; Nentwich, L.M.; Luby, M.; Butman, J.A.; Demchuk, A.M.; Hill, M.D.; Patronas, N.; Latour, L.; Warach, S. Magnetic resonance imaging and computed tomography in emergency assessment of patients with suspected acute stroke: A prospective comparison. Lancet 2007, 369, 293–298. [Google Scholar] [CrossRef]
- Parikh, N.A. Advanced neuroimaging and its role in predicting neurodevelopmental outcomes in very preterm infants. Semin. Perinatol. 2016, 40, 530–541. [Google Scholar] [CrossRef]
- Jose, A.; Matthai, J.; Paul, S. Correlation of EEG, CT, and MRI Brain with Neurological Outcome at 12 Months in Term Newborns with Hypoxic Ischemic Encephalopathy. J. Clin. Neonatol. 2013, 2, 125–130. [Google Scholar] [CrossRef]
- Slaughter, L.A.; Bonfante-Mejia, E.; Hintz, S.R.; Dvorchik, I.; Parikh, N.A. Early Conventional MRI for Prediction of Neurodevelopmental Impairment in Extremely-Low-Birth-Weight Infants. Neonatology 2016, 110, 47–54. [Google Scholar] [CrossRef]
- McIntosh, A.M.; Tong, S.; Deakyne, S.J.; Davidson, J.A.; Scott, H.F. Validation of the Vasoactive-Inotropic Score in Pediatric Sepsis. Pediatr. Crit. Care Med. 2017, 18, 750–757. [Google Scholar] [CrossRef] [PubMed]
- Abadi, M.; Barham, P.; Chen, J.; Chen, Z.; Davis, A.; Dean, J.; Devin, M.; Ghemawat, S.; Irving, G.; Isard, M.; et al. TensorFlow: A System for Large-Scale Machine Learning. Available online: https://www.usenix.org/system/files/conference/osdi16/osdi16-abadi.pdf (accessed on 13 July 2020).
- Bock, S.; Goppold, J.; Weiß, M. An Improvement of the Convergence Proof of the ADAM-Optimizer. Available online: https://arxiv.org/abs/1804.10587 (accessed on 13 July 2020).
- McWilliams, C.J.; Lawson, D.J.; Santos-Rodriguez, R.; Gilchrist, I.D.; Champneys, A.; Gould, T.H.; Thomas, M.J.; Bourdeaux, C.P. Towards a decision support tool for intensive care discharge: Machine learning algorithm development using electronic healthcare data from MIMIC-III and Bristol, UK. BMJ Open 2019, 9. [Google Scholar] [CrossRef] [PubMed]
- Leray, P.; Gallinari, P. Feature Selection with Neural Networks. Behaviormetrika 1999, 26, 145–166. [Google Scholar] [CrossRef]
- Khemphila, A.; Boonjing, V. Heart Disease Classification Using Neural Network and Feature Selection. In Proceedings of the 2011 21st International Conference on Systems Engineering, Las Vegas, NV, USA, 16–18 August 2011. [Google Scholar] [CrossRef]
- Aczon, M.; Ledbetter, D.; Ho, L.; Gunny, A.; Flynn, A.; Williams, J.; Wetzel, R. Dynamic Mortality Risk Predictions in Pediatric Critical Care Using Recurrent Neural Networks. arXiv 2017, arXiv:170106675. [Google Scholar]
- Perng, J.-W.; Kao, I.-H.; Kung, C.-T.; Hung, S.-C.; Lai, Y.-H.; Su, C.-M. Mortality Prediction of Septic Patients in the Emergency Department Based on Machine Learning. J. Clin. Med. 2019, 8, 1906. [Google Scholar] [CrossRef]
- Le, S.; Hoffman, J.; Barton, C.; Fitzgerald, J.C.; Allen, A.; Pellegrini, E.; Calvert, J.; Das, R. Pediatric Severe Sepsis Prediction Using Machine Learning. Front. Pediatr. 2019, 7. [Google Scholar] [CrossRef]
- Yee, C.R.; Narain, N.R.; Akmaev, V.R.; Vemulapalli, V. A Data-Driven Approach to Predicting Septic Shock in the Intensive Care Unit. Biomed. Inform. Insights 2019, 11. [Google Scholar] [CrossRef]
- Peiffer-Smadja, N.; Rawson, T.M.; Ahmad, R.; Buchard, A.; Georgiou, P.; Lescure, F.-X.; Birgand, G.; Holmes, A.H. Machine learning for clinical decision support in infectious diseases: A narrative review of current applications. Clin. Microbiol. Infect. 2020, 26, 584–595. [Google Scholar] [CrossRef]
- Jaimes, F.; Farbiarz, J.; Alvarez, D.; Martínez, C. Comparison between logistic regression and neural networks to predict death in patients with suspected sepsis in the emergency room. Crit. Care 2005, 9, R150–R156. [Google Scholar] [CrossRef]



| Demographics of Patients in Database | ||
|---|---|---|
| Age | Range | 0–18 years |
| Median (IQR) | 10 months (6 years) | |
| Gender | Male | 92 (53%) |
| Female | 82 (47%) | |
| Weight (kg) | Range | 1.9–132 |
| Median (IQR) | 5.9 (14.2) | |
| ECMO Type | Venoarterial | 106 (61%) |
| Venovenous | 68 (39%) | |
| ECMO Primary Indication | Cardiac | 49 (28%) |
| Non-cardiac | 125 (72%) | |
| ECMO Run Length (hours) | Range | 14–985 |
| Median (IQR) | 129 (165) | |
| Injury Status | Injury | 89 (51%) |
| No injury | 85 (49%) | |
| Patient Characteristics | |||
|---|---|---|---|
| Neurological Injury | No Neurological injury | p | |
| Primary ECMO indication (total n: 174) | |||
| Non-cardiac | 64 | 61 | 0.85 |
| Cardiac | 25 | 24 | 0.50 |
| Initial mode of ECMO (total n: 174) | |||
| Venoarterial | 61 | 45 | 0.12 |
| Venovenous | 28 | 40 | 0.15 |
| Gender (total n: 174) | |||
| Male | 49 | 43 | 0.53 |
| Female | 40 | 42 | 0.83 |
| Age (total n: 174) | |||
| Neonate (0–30 days) | 38 | 32 | 0.47 |
| Infant (1–12 months) | 8 | 21 | 0.02 * |
| Child (1–12 years) | 35 | 19 | 0.03 * |
| Adolescent (>12 years) | 8 | 13 | 0.28 |
| Survived to hospital discharge | 76% | 72% | 0.74 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shah, N.; Farhat, A.; Tweed, J.; Wang, Z.; Lee, J.; McBeth, R.; Skinner, M.; Tian, F.; Thiagarajan, R.; Raman, L. Neural Networks to Predict Radiographic Brain Injury in Pediatric Patients Treated with Extracorporeal Membrane Oxygenation. J. Clin. Med. 2020, 9, 2718. https://doi.org/10.3390/jcm9092718
Shah N, Farhat A, Tweed J, Wang Z, Lee J, McBeth R, Skinner M, Tian F, Thiagarajan R, Raman L. Neural Networks to Predict Radiographic Brain Injury in Pediatric Patients Treated with Extracorporeal Membrane Oxygenation. Journal of Clinical Medicine. 2020; 9(9):2718. https://doi.org/10.3390/jcm9092718
Chicago/Turabian StyleShah, Neel, Abdelaziz Farhat, Jefferson Tweed, Ziheng Wang, Jeon Lee, Rafe McBeth, Michael Skinner, Fenghua Tian, Ravi Thiagarajan, and Lakshmi Raman. 2020. "Neural Networks to Predict Radiographic Brain Injury in Pediatric Patients Treated with Extracorporeal Membrane Oxygenation" Journal of Clinical Medicine 9, no. 9: 2718. https://doi.org/10.3390/jcm9092718
APA StyleShah, N., Farhat, A., Tweed, J., Wang, Z., Lee, J., McBeth, R., Skinner, M., Tian, F., Thiagarajan, R., & Raman, L. (2020). Neural Networks to Predict Radiographic Brain Injury in Pediatric Patients Treated with Extracorporeal Membrane Oxygenation. Journal of Clinical Medicine, 9(9), 2718. https://doi.org/10.3390/jcm9092718