Increased First Pass Success with C-MAC Videolaryngoscopy in Prehospital Endotracheal Intubation—A Randomized Controlled Trial

 ,
,
Abstract
1. Introduction
2. Experimental Section
2.1. Primary Outcome
2.2. Secondary Outcome
2.3. Intubation and Staff
2.3.1. Physician
2.3.2. HEMS Paramedic
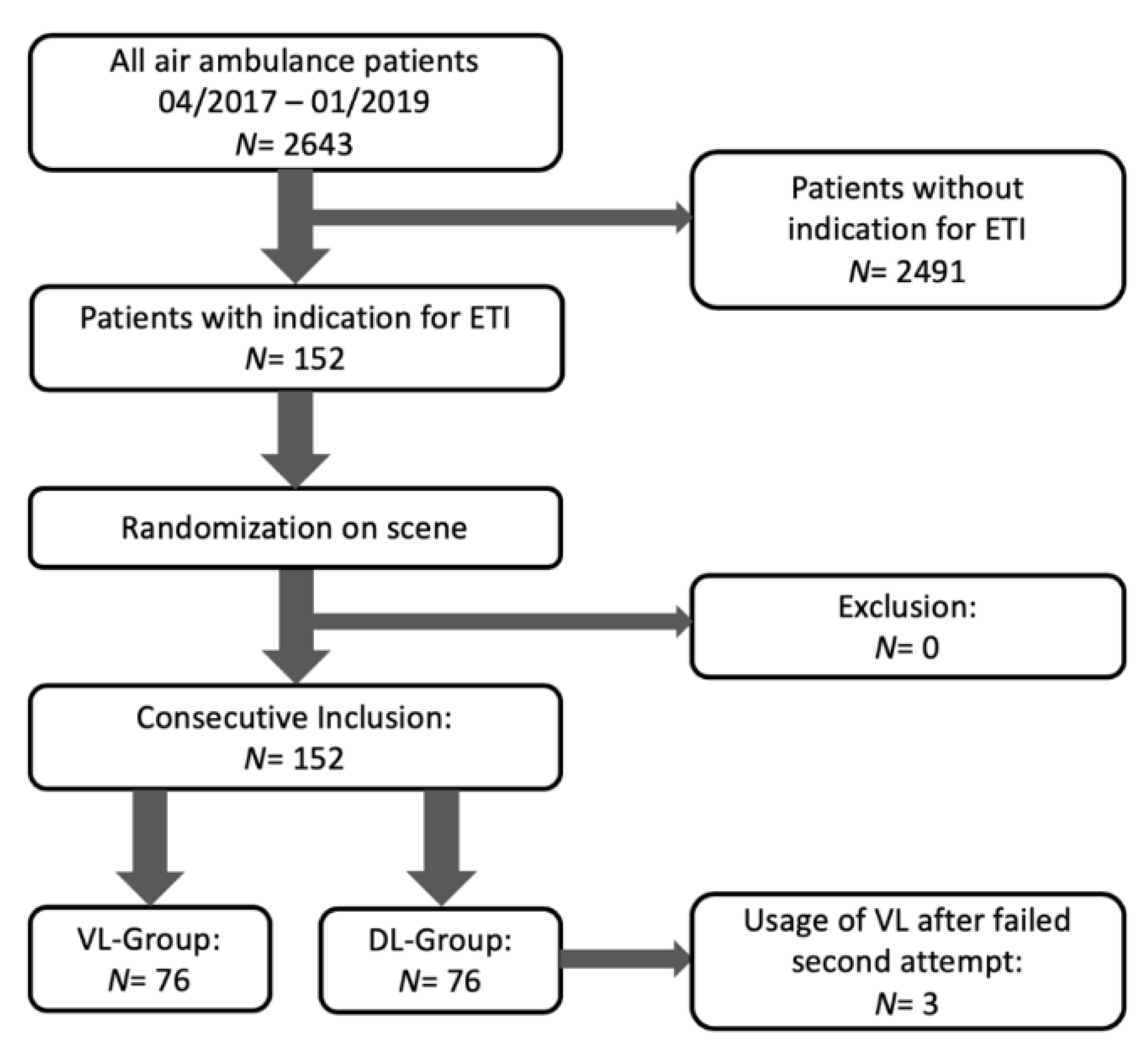
2.4. Randomization
2.5. Airway Management Problems
2.6. Laryngoscope
2.7. Measured Parameters
- Assumed intubation problems (facial trauma, limited mouth opening (<2.5 cm), no neck, rigid collar during intubation, fluid in pharynx (vomit/blood)).
- Indication (resuscitation/CPR (cardiopulmonary resuscitation), trauma-resuscitation/trauma-CPR, musculoskeletal trauma, neurologic, burns, pulmonary, drowning).
- Site (floor, ambulance stretcher, sitting position, inside helicopter, other).
- Lighting conditions (poor, good, too bright).
- Necessary or applied relaxation with induction.
- Oxygen saturation before, during and after intubation.
- Best sight of glottis with percentage of glottis opening (POGO-Score) and Cormack-Lehane Score (CL) I–IV.
- Time for intubation measured by the HEMS paramedic with a stopwatch from taking off the mask to either tube blocking and detectable end-tidal CO2 or putting back the mask.
- In case of videolaryngoscopy usage: whether the monitor or direct laryngoscopy was used. In all cases the monitor was used.
- Number of attempts with video- or direct view laryngoscopy.
- Blade size and type (Macintosh II-IV, D-Blade).
- Correctness of intubation proofed by auscultation and capnography.
- Necessity of alternative airway management.
2.8. Statistical Analysis
3. Results
3.1. General Patient Data
3.2. Experienced vs. Less Experienced Physicians
3.3. First Pass Success Rate
3.4. ETI Time and Glottic View
4. Discussion
4.1. Limitations, Strength, and Generalizability
4.2. Summary
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lavery, G.; McCloskey, B.V. The difficult airway in adult critical care. Crit. Care Med. 2008, 36, 2163–2173. [Google Scholar] [CrossRef] [PubMed]
- Adnet, F.; Racine, S.; Borron, S.W.; Clemessy, J.L.; Fournier, J.L.; Lapostolle, F.; Cupa, M. A survey of tracheal intubation difficulty in the operating room: A prospective observational study. Acta Anaesth. Scand. 2001, 45, 327–332. [Google Scholar] [CrossRef]
- Timmermann, A.; Russo, S.G.; Eich, C.; Roessler, M.; Braun, U.; Rosenblatt, W.H.; Quintel, M. The Out-Of-Hospital Esophageal and Endobronchial Intubations Performed by Emergency Physicians. Anesth. Analg. 2007, 104, 619–623. [Google Scholar] [CrossRef]
- Aziz, M.F.; Brambrink, A.M.; Healy, D.W.; Willett, A.W.; Shanks, A.; Tremper, T.; Jameson, L.; Ragheb, J.; Biggs, D.A.; Paganelli, W.C.; et al. Success of Intubation Rescue Techniques after Failed Direct Laryngoscopy in Adults: A Retrospective Comparative Analysis from the Multicenter Perioperative Outcomes Group. Anesthesiology 2016, 125, 656–666. [Google Scholar] [CrossRef]
- Bernhard, M.; Bax, S.N.; Hartwig, T.; Yahiaoui-Doktor, M.; Petros, S.; Bercker, S.; Ramshorn-Zimmer, A.; Gries, A. Airway Management in the Emergency Department (The OcEAN-Study)-A prospective single centre observational cohort study. Scand. J. Trauma Resusc. Emerg. Med. 2019, 27, 20. [Google Scholar] [CrossRef]
- Loughnan, A.; Deng, C.; Dominick, F.; Pencheva, L.; Campbell, D. A single-centre, randomised controlled feasibility pilot trial comparing performance of direct laryngoscopy versus videolaryngoscopy for endotracheal intubation in surgical patients. Pilot Feasibility Stud. 2019, 5, 50. [Google Scholar] [CrossRef]
- Lewis, S.R.; Butler, A.; Parker, J.; Cook, T.; Schofield-Robinson, O.; Smith, A. Videolaryngoscopy versus direct laryngoscopy for adult patients requiring tracheal intubation: A Cochrane Systematic Review. Br. J. Anaesth. 2017, 119, 369–383. [Google Scholar] [CrossRef]
- Pieters, B.M.A.; Maas, E.H.A.; Knape, J.T.A.; Van Zundert, A.A.J. Videolaryngoscopy vs. direct laryngoscopy use by experienced anaesthetists in patients with known difficult airways: A systematic review and meta-analysis. Anaesthesia 2017, 72, 1532–1541. [Google Scholar] [CrossRef]
- Trimmel, H.; Kreutziger, J.; Fitzka, R.; Szuts, S.; Derdak, C.; Koch, E.; Erwied, B.; Voelckel, W.G. Use of the glidescope ranger video laryngoscope for emergency intubation in the prehospital setting: A Randomized Control Trial. Crit. Care Med. 2016, 44, e470–e476. [Google Scholar] [CrossRef] [PubMed]
- Kreutziger, J.; Hornung, S.; Harrer, C.; Urschl, W.; Doppler, R.; Voelckel, W.G.; Trimmel, H. Comparing the McGrath Mac Video Laryngoscope and Direct Laryngoscopy for Prehospital Emergency Intubation in Air Rescue Patients. Crit. Care Med. 2019, 47, 1362–1370. [Google Scholar] [CrossRef] [PubMed]
- Cavus, E.; Janssen, S.; Reifferscheid, F.; Caliebe, A.; Callies, A.; von der Heyden, M.; Knacke, P.G.; Doerges, V. Faculty Opinions recommendation of Videolaryngoscopy for Physician-Based, Prehospital Emergency Intubation: A Prospective, Randomized, Multicenter Comparison of Different Blade Types Using A.P. Advance, C-MAC System, and KingVision. Anesth. Analg. 2018, 126, 1565–1574. [Google Scholar] [CrossRef] [PubMed]
- Luckscheiter, A.; Lohs, T.; Fischer, M.; Zink, W. Preclinical emergency anesthesia: A current state analysis from 2015–2017. Anaesthesist 2019, 68, 270–281. [Google Scholar] [CrossRef] [PubMed]
- Cook, T.M.; Boniface, N.; Seller, C.; Hughes, J.; Damen, C.; Macdonald, L.; Kelly, F.E. Universal videolaryngoscopy: A structured approach to conversion to videolaryngoscopy for all intubations in an anaesthetic and intensive care department. Br. J. Anaesth. 2018, 120, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.-Y. Education: The last mile to universal videolaryngoscopy. Br. J. Anaesth. 2018, 120, 1431–1432. [Google Scholar] [CrossRef]
- Park, L.; Zeng, I.; Brainard, A.H. Systematic review and meta-analysis of first-pass success rates in emergency department intubation: Creating a benchmark for emergency airway care. Emerg. Med. Australas. 2016, 29, 40–47. [Google Scholar] [CrossRef]
- Aziz, M.; Healy, D.; Kheterpal, S.; Fu, R.F.; Dillman, D.; Brambrink, A.M. Routine Clinical Practice Effectiveness of the Glidescope in Difficult Airway Management. Anesthesiology 2011, 114, 34–41. [Google Scholar] [CrossRef]
- Sakles, J.C.; Chiu, S.; Mosier, J.; Walker, C.; Stolz, U. The importance of first pass success when performing orotracheal intubation in the emergency department. Acad. Emerg. Med. 2013, 20, 71–78. [Google Scholar] [CrossRef]
- Powell, E.K.; Hinckley, W.R.; Stolz, U.; Golden, A.J.; Ventura, A.; McMullan, J.T. Abstract 4: Predictors of Definitive Airway sans Hypoxia/Hypotension on First Attempt (DASH 1A) Success in Traumatically Injured Patients Undergoing Prehospital Intubation. Prehosp. Emerg. Care 2019, 7, 1–8. [Google Scholar] [CrossRef]
- Guihard, B.; Chollet-Xémard, C.; Lakhnati, P.; Vivien, B.; Broche, C.; Savary, D.; Ricard-Hibon, A.; Cassou, P.-J.M.D.; Adnet, F.; Wiel, E.; et al. Effect of Rocuronium vs Succinylcholine on Endotracheal Intubation Success Rate Among Patients Undergoing Out-of-Hospital Rapid Sequence Intubation: A Randomized Clinical Trial. JAMA 2019, 322, 2303–2312. [Google Scholar] [CrossRef]
- Min, B.C.; Park, J.E.; Lee, G.T.; Kim, T.; Yoon, H.; Cha, W.C.; Shin, T.G.; Song, K.J.; Park, M.; Han, H.; et al. C-MAC Video Laryngoscope versus Conventional Direct Laryngoscopy for Endotracheal Intubation During Cardiopulmonary Resuscitation. Medicina 2019, 55, 225. [Google Scholar] [CrossRef]
- Eberlein, C.M.; Luther, I.S.; Carpenter, T.A.; Ramirez, L.D. First-Pass Success Intubations Using Video Laryngoscopy Versus Direct Laryngoscopy: A Retrospective Prehospital Ambulance Service Study. Air Med. J. 2019, 38, 356–358. [Google Scholar] [CrossRef] [PubMed]
- Mackie, S.; Moy, F.; Kamona, S.; Jones, P. Effect of the introduction of C-MAC videolaryngoscopy on first-pass intubation success rates for emergency medicine registrars. Emerg. Med. Australas. 2019, 32, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Wilson, P.M.E.; Spiegelhalter, P.D.; Robertson, F.J.A.; Lesser, F.P. Predicting Difficult Intubation. Br. J. Anaesth. 1988, 61, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Piepho, T.; Fortmueller, K.; Heid, F.M.; Schmidtmann, I.; Werner, C.; Noppens, R.R. Performance of the C-MAC video laryngoscope in patients after a limited glottic view using Macintosh laryngoscopy. Anaesthesia 2011, 66, 1101–1105. [Google Scholar] [CrossRef] [PubMed]
- Sulser, S.; Ubmann, D.; Schlaepfer, M.; Brueesch, M.; Goliasch, G.; Seifert, B.; Spahn, D.R.; Ruetzler, K. C-MAC videolaryngoscope compared with direct laryngoscopy for rapid sequence intubation in an emergency department. Eur. J. Anaesth. 2016, 33, 943–948. [Google Scholar] [CrossRef] [PubMed]
- Bodily, J.B.; Webb, H.R.; Weiss, S.J.; Braude, D.A. Incidence and Duration of Continuously Measured Oxygen Desaturation During Emergency Department Intubation. Ann. Emerg. Med. 2016, 67, 389–395. [Google Scholar] [CrossRef]
- Ruetzler, K.; Imach, S.; Weiss, M.; Haas, T.; Schmidt, A.R. Comparison of five video laryngoscopes and conventional direct laryngoscopy: Investigations on simple and simulated difficult airways on the intubation trainer. Anaesthesist 2015, 64, 513–519. [Google Scholar] [CrossRef]


{kind=link}
| Indication | Number (n (%)) Total | Number (n (%)) VL | Number (n (%)) DL |
|---|---|---|---|
| Resuscitation/CPR | 70 (46.1%) | 29 (38.2%) | 41 (53.9%) |
| Trauma-resuscitation/Trauma-CPR | 14 (9.2%) | 10 (13.2%) | 4 (5.3%) |
| Musculoskeletal trauma | 47 (30.9%) | 27 (35.5%) | 20 (26.3%) |
| Neurologic | 11 (7.2%) | 6 (7.9%) | 5 (6.6%) |
| Burns | 5 (3.3%) | 1 (1.3%) | 4 (5.3%) |
| Pulmonary | 4 (2.6%) | 2 (2.6%) | 2 (2.6%) |
| Drowning | 1 (0.7%) | 1 (1.3%) | 0 (0.0%) |
| VL (n (%; 95%-CI)) | DL (n (%; 95%-CI)) | p-Value | |
|---|---|---|---|
| Number | 76 | 76 | - |
| Rigid collar during ETI | 19 (25%; 15–35) | 11 (14%; 6–23) | 0.15 |
| No neck patient | 12 (16%; 7–24) | 8 (11%; 3–18) | 0.47 |
| Mid facial trauma | 10 (13%; 5–21) | 8 (11%; 3–18) | 0.80 |
| Bleeding/aspiration | 10 (13%; 5–21) | 12 (16%; 7–24) | 0.82 |
| Limited mouth opening | 6 (8%; 2–14) | 3 (4%; −1–8) | 0.49 |
| Assumed intubation problems | 42 (55%; 44–67) | 39 (51%; 49–63) | 0.75 |
| Attempts | VL (n, (%; 95%-CI)) | DL (n, (%; 95%-CI)) | p-Value |
|---|---|---|---|
| 1st attempt successful | 72 (95%; 90–100) | 60 (79%; 70–88) | 0.007 |
| 2nd attempt successful | 4 (100%; 100) | 13 (81%; 60–103) | 1.0 |
| 3rd attempt successful | 0 (0%) | 2 (67%; −77–210) | not applicable |
| 4th attempt successful | 0 (0%) | 1 (100%; 100) | not applicable |
| Attempts | VL (s) as Median (Q1:Q3) | DL (s) as Median (Q1:Q3) | p-Value |
|---|---|---|---|
| 1st attempt | 15.5 (10:20) | 18.5 (12.5:24.5) | 0.01 |
| 2nd attempt | 15 (9.0:25.0) | 15 (10:20) | 0.89 |
| 3rd attempt | n. a. | 12 (10.5:18.5) | n. a. |
| 4th attempt | n. a. | 30 | n. a. |
| Dependence on 1st Attempt | VL | DL | p-Value |
| POGO-Score (%), median (Q1:Q3) | 100 (90:100) | 65 (30:90) | <0.001 |
| Cormack & Lehane, median (Q1:Q3) | 1 (1:2) | 2 (2:2) | <0.001 |
| Dependence on 2nd Attempt | VL | DL | p-Value |
| POGO-Score (%), median (Q1:Q3) | 72.5 (51.25:90) | 20 (0:62.5) | 0.04 |
| Cormack & Lehane, median (Q1:Q3) | 2 (2:2) | 2 (2:3.75) | 0.29 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Macke, C.; Gralla, F.; Winkelmann, M.; Clausen, J.-D.; Haertle, M.; Krettek, C.; Omar, M. Increased First Pass Success with C-MAC Videolaryngoscopy in Prehospital Endotracheal Intubation—A Randomized Controlled Trial. J. Clin. Med. 2020, 9, 2719. https://doi.org/10.3390/jcm9092719
Macke C, Gralla F, Winkelmann M, Clausen J-D, Haertle M, Krettek C, Omar M. Increased First Pass Success with C-MAC Videolaryngoscopy in Prehospital Endotracheal Intubation—A Randomized Controlled Trial. Journal of Clinical Medicine. 2020; 9(9):2719. https://doi.org/10.3390/jcm9092719
Chicago/Turabian StyleMacke, Christian, Felix Gralla, Marcel Winkelmann, Jan-Dierk Clausen, Marco Haertle, Christian Krettek, and Mohamed Omar. 2020. "Increased First Pass Success with C-MAC Videolaryngoscopy in Prehospital Endotracheal Intubation—A Randomized Controlled Trial" Journal of Clinical Medicine 9, no. 9: 2719. https://doi.org/10.3390/jcm9092719
APA StyleMacke, C., Gralla, F., Winkelmann, M., Clausen, J.-D., Haertle, M., Krettek, C., & Omar, M. (2020). Increased First Pass Success with C-MAC Videolaryngoscopy in Prehospital Endotracheal Intubation—A Randomized Controlled Trial. Journal of Clinical Medicine, 9(9), 2719. https://doi.org/10.3390/jcm9092719