Additional Mosapride to Proton Pump Inhibitor for Gastroesophageal Reflux Disease: A Meta-Analysis

 and
and 
Abstract
1. Introduction
2. Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Outcome Measures
2.4. Data Extraction
2.5. Assessment of Methodological Quality
2.6. Statistical Analysis
3. Results
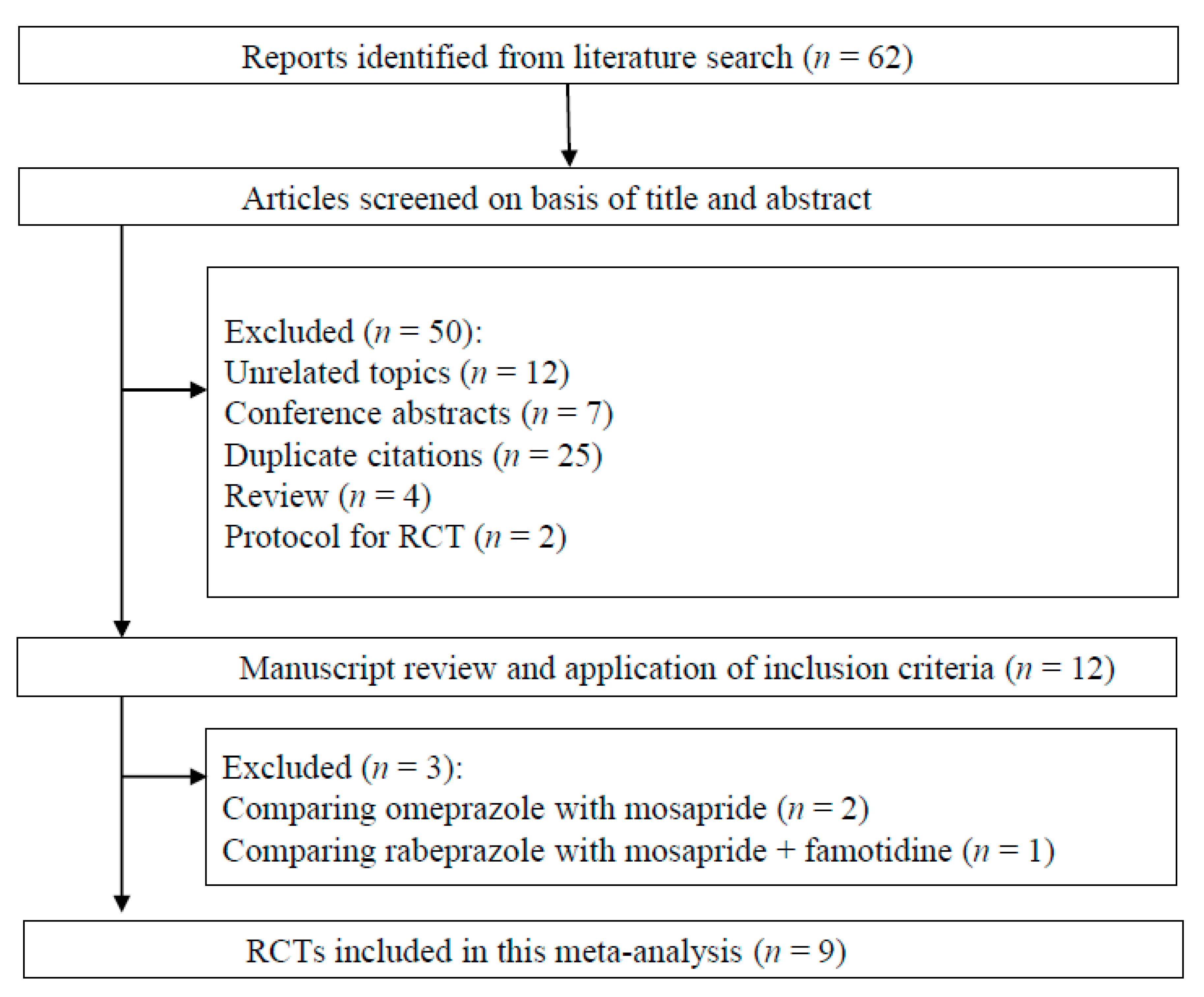
3.1. Search Results
3.2. Quality Assessment
3.3. Meta-Analysis Results
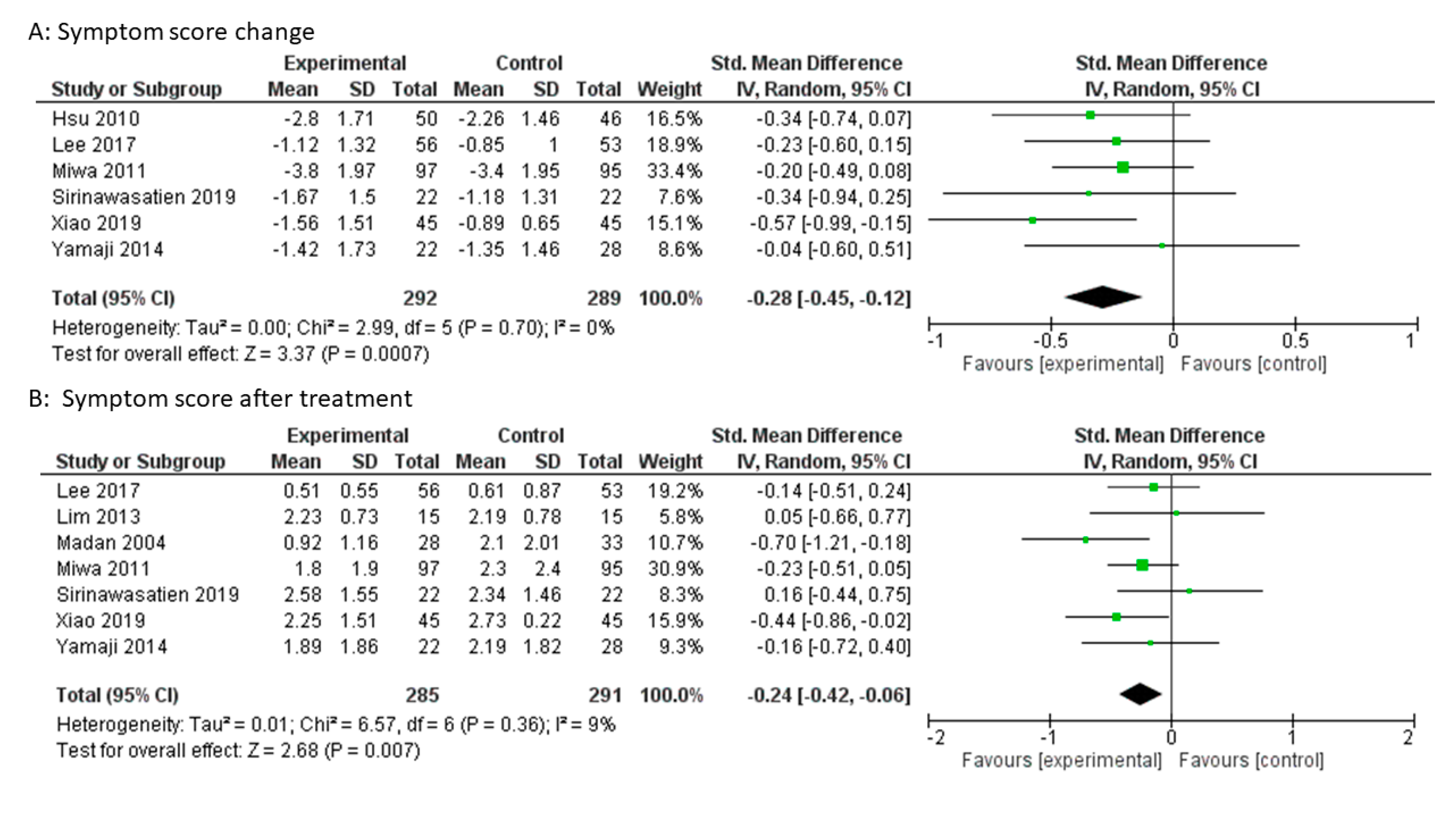
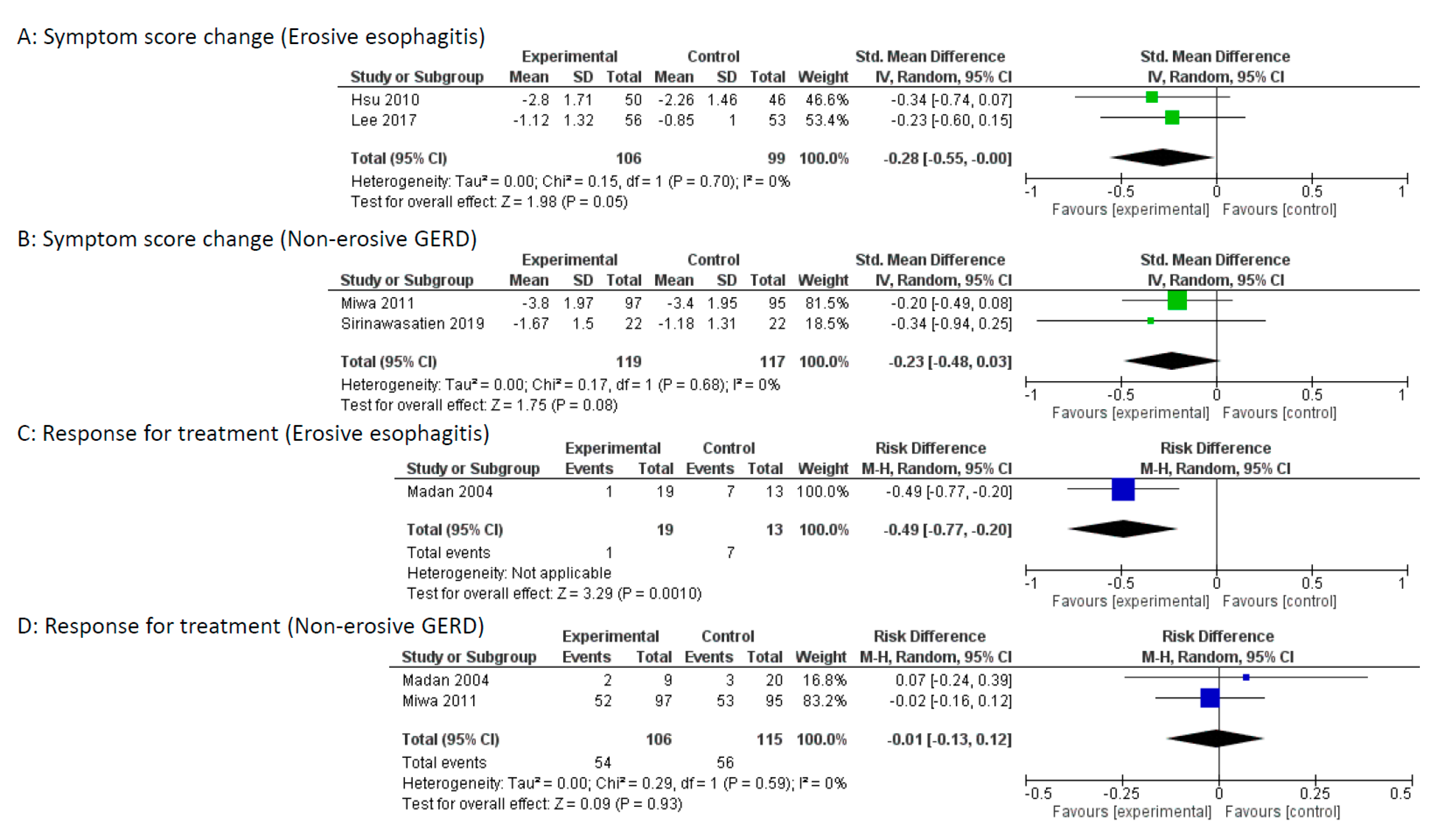
3.3.1. Improvement in Symptom Scores
3.3.2. Symptom Scores after Treatment
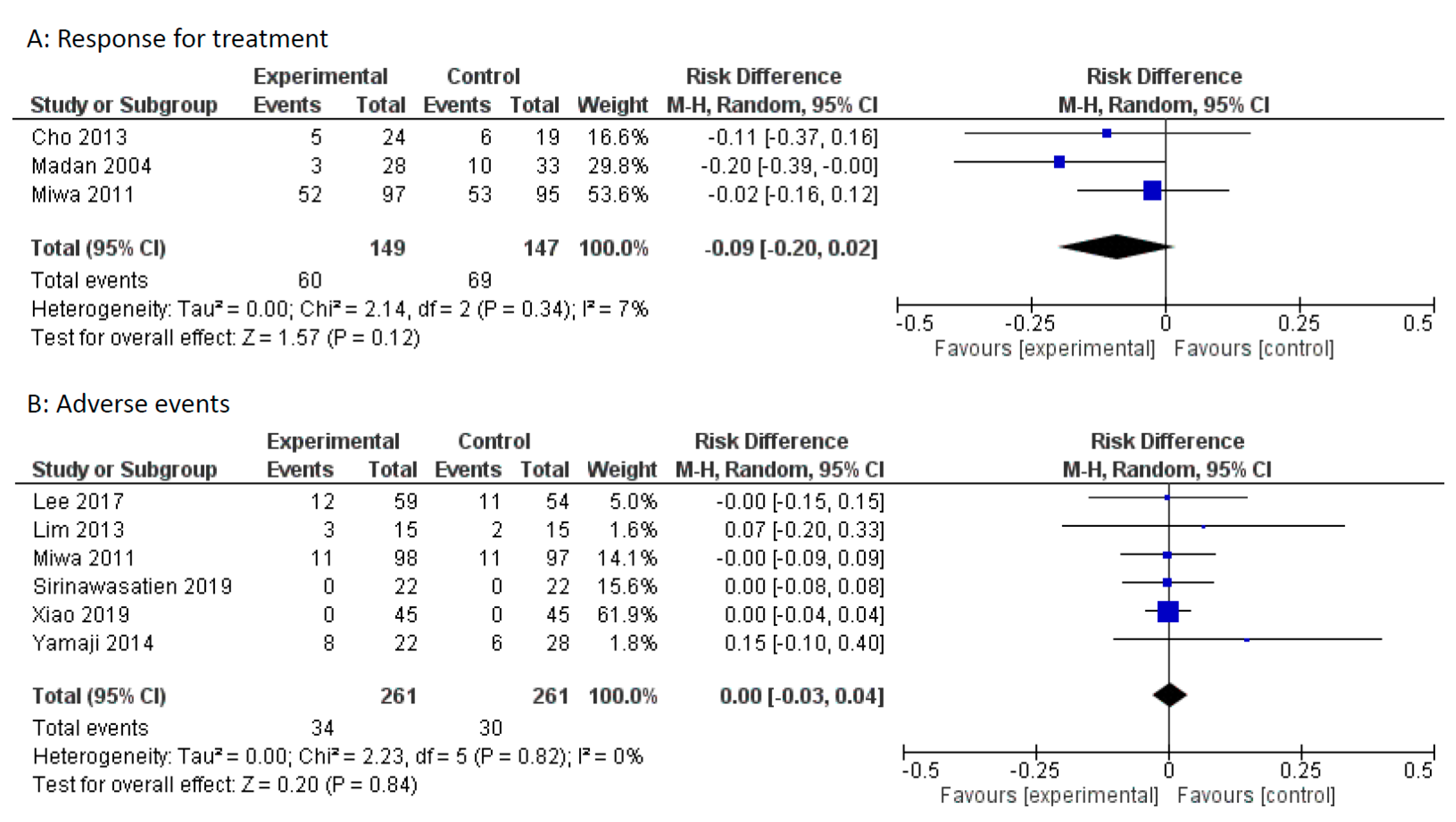
3.3.3. Response to Treatment
3.3.4. Adverse Events
3.3.5. Subgroup Analysis
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Boeckxstaens, G.; El-Serag, H.B.; Smout, A.J.; Kahrilas, P.J. Symptomatic reflux disease: The present, the past and the future. Gut 2014, 63, 1185–1193. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, E.; Suzuki, H.; Sugino, Y.; Iida, T.; Nishizawa, T.; Masaoka, T.; Hosoda, H.; Kangawa, K.; Hibi, T. Decreased levels of adiponectin in obese patients with gastroesophageal reflux evaluated by videoesophagography: Possible relationship between gastroesophageal reflux and metabolic syndrome. J. Gastroenterol. Hepatol. 2008, 23, 216–221. [Google Scholar] [CrossRef]
- Suzuki, H.; Matsuzaki, J.; Okada, S.; Hirata, K.; Fukuhara, S.; Hibi, T. Validation of the GerdQ questionnaire for the management of gastro-oesophageal reflux disease in Japan. United Eur. Gastroenterol. J. 2013, 1, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Eguaras, N.; Rodriguez-Lopez, E.S.; Lopez-Dicastillo, O.; Franco-Sierra, M.A.; Ricard, F.; Oliva-Pascual-Vaca, A. Effects of osteopathic visceral treatment in patients with gastroesophageal reflux: a randomized controlled trial. J. Clin. Med. 2019, 8, 1738. [Google Scholar] [CrossRef] [PubMed]
- Futagami, S.; Iwakiri, K.; Shindo, T.; Kawagoe, T.; Horie, A.; Shimpuku, M.; Tanaka, Y.; Kawami, N.; Gudis, K.; Sakamoto, C. The prokinetic effect of mosapride citrate combined with omeprazole therapy improves clinical symptoms and gastric emptying in PPI-resistant NERD patients with delayed gastric emptying. J. Gastroenterol. 2010, 45, 413–421. [Google Scholar] [CrossRef]
- Matsuzaki, J.; Suzuki, H.; Kobayakawa, M.; Inadomi, J.M.; Takayama, M.; Makino, K.; Iwao, Y.; Sugino, Y.; Kanai, T. Association of visceral fat area, smoking, and alcohol consumption with reflux esophagitis and barrett’s esophagus in Japan. PLoS ONE 2015, 10, e0133865. [Google Scholar] [CrossRef]
- Kinoshita, Y.; Hongo, M.; Kusano, M.; Furuhata, Y.; Miyagishi, H.; Ikeuchi, S. Therapeutic response to twice-daily rabeprazole on health-related quality of life and symptoms in patients with refractory reflux esophagitis: a multicenter observational study. Intern. Med. 2017, 56, 1131–1139. [Google Scholar] [CrossRef]
- Kwon, Y.S.; Choi, J.W.; Lee, H.S.; Kim, J.H.; Kim, Y.; Lee, J.J. Effect of a preoperative proton pump inhibitor and gastroesophageal reflux disease on postoperative nausea and vomiting. J. Clin. Med. 2020, 9, 825. [Google Scholar] [CrossRef]
- Hirata, K.; Suzuki, H.; Matsuzaki, J.; Masaoka, T.; Saito, Y.; Nishizawa, T.; Iwasaki, E.; Fukuhara, S.; Okada, S.; Hibi, T. Improvement of reflux symptom related quality of life after Helicobacter pylori eradication therapy. J. Clin. Biochem. Nutr. 2013, 52, 172–178. [Google Scholar] [CrossRef]
- Miwa, H.; Igarashi, A.; Teng, L.; Uda, A.; Deguchi, H.; Tango, T. Systematic review with network meta-analysis: Indirect comparison of the efficacy of vonoprazan and proton-pump inhibitors for maintenance treatment of gastroesophageal reflux disease. J. Gastroenterol. 2019, 54, 718–729. [Google Scholar] [CrossRef]
- Ren, L.H.; Chen, W.X.; Qian, L.J.; Li, S.; Gu, M.; Shi, R.H. Addition of prokinetics to PPI therapy in gastroesophageal reflux disease: A meta-analysis. World J. Gastroenterol. 2014, 20, 2412–2419. [Google Scholar] [CrossRef] [PubMed]
- Madan, K.; Ahuja, V.; Kashyap, P.C.; Sharma, M.P. Comparison of efficacy of pantoprazole alone versus pantoprazole plus mosapride in therapy of gastroesophageal reflux disease: A randomized trial. Dis. Esophagus 2004, 17, 274–278. [Google Scholar] [CrossRef] [PubMed]
- Hsu, Y.C.; Yang, T.H.; Hsu, W.L.; Wu, H.T.; Cheng, Y.C.; Chiang, M.F.; Wang, C.S.; Lin, H.J. Mosapride as an adjunct to lansoprazole for symptom relief of reflux oesophagitis. Br. J. Clin. Pharm. 2010, 70, 171–179. [Google Scholar] [CrossRef]
- Miwa, H.; Inoue, K.; Ashida, K.; Kogawa, T.; Nagahara, A.; Yoshida, S.; Tano, N.; Yamazaki, Y.; Wada, T.; Asaoka, D.; et al. Randomised clinical trial: Efficacy of the addition of a prokinetic, mosapride citrate, to omeprazole in the treatment of patients with non-erosive reflux disease-a double-blind, placebo-controlled study. Aliment. Pharm. Ther. 2011, 33, 323–332. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.K.; Choi, M.G.; Park, E.Y.; Lim, C.H.; Kim, J.S.; Park, J.M.; Lee, I.S.; Kim, S.W.; Choi, K.Y. Effect of mosapride combined with esomeprazole improves esophageal peristaltic function in patients with gastroesophageal reflux disease: A study using high resolution manometry. Dig. Dis. Sci. 2013, 58, 1035–1041. [Google Scholar] [CrossRef]
- Liu, Q.; Feng, C.C.; Wang, E.M.; Yan, X.J.; Chen, S.L. Efficacy of mosapride plus proton pump inhibitors for treatment of gastroesophageal reflux disease: A systematic review. World J. Gastroenterol. 2013, 19, 9111–9118. [Google Scholar] [CrossRef]
- Lim, H.C.; Kim, J.H.; Youn, Y.H.; Lee, E.H.; Lee, B.K.; Park, H. Effects of the addition of mosapride to gastroesophageal reflux disease patients on proton pump inhibitor: A prospective randomized, double-blind study. J. Neurogastroenterol. Motil. 2013, 19, 495–502. [Google Scholar] [CrossRef][Green Version]
- Sirinawasatien, A.; Kantathavorn, N. Efficacy of the four weeks treatment of omeprazole plus mosapride combination therapy compared with that of omeprazole monotherapy in patients with proton pump inhibitor-refractory gastroesophageal reflux disease: A randomized controlled trial. Clin. Exp. Gastroenterol. 2019, 12, 337–347. [Google Scholar] [CrossRef]
- Yamaji, Y.; Isomura, Y.; Yoshida, S.; Yamada, A.; Hirata, Y.; Koike, K. Randomized controlled trial comparing the efficacy of mosapride plus omeprazole combination therapy to omeprazole monotherapy in gastroesophageal reflux disease. J. Dig. Dis. 2014, 15, 469–476. [Google Scholar] [CrossRef]
- Lee, J.Y.; Kim, S.K.; Cho, K.B.; Park, K.S.; Kwon, J.G.; Jung, J.T.; Kim, E.Y.; Jang, B.I.; Lee, S.H.A. Double-blind, randomized, multicenter clinical trial investigating the efficacy and safety of esomeprazole single therapy versus mosapride and esomeprazole combined therapy in patients with esophageal reflux disease. J. Neurogastroenterol. Motil. 2017, 23, 218–228. [Google Scholar] [CrossRef]
- Xiao, F.; Mao, J. Treatment of gastoesophageal reflux-related cough with proton pump inhibitors and prokinetic agents. Acta. Med. Mediterr. 2019, 35, 3131–3137. [Google Scholar]
- Nishizawa, T.; Suzuki, H.; Akimoto, T.; Maehata, T.; Morizane, T.; Kanai, T.; Yahagi, N. Effects of preoperative proton pump inhibitor administration on bleeding after gastric endoscopic submucosal dissection: A systematic review and meta-analysis. United Eur. Gastroenterol. J. 2016, 4, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions, Version 5.1.0 [updated March 2011]; The Cochrane Collaboration: Hoboken, NJ, USA, 2011; Available online: www.cochrane-handbook.org. (accessed on 20 March 2011).
- Murata, M.; Sugimoto, M.; Mizuno, H.; Kanno, T.; Satoh, K. Clarithromycin versus metronidazole in first-line helicobacter pylori triple eradication therapy based on resistance to antimicrobial agents: meta-analysis. J. Clin. Med. 2020, 9, 543. [Google Scholar] [CrossRef] [PubMed]
- Horibe, M.; Nishizawa, T.; Suzuki, H.; Minami, K.; Yahagi, N.; Iwasaki, E.; Kanai, T. Timing of oral refeeding in acute pancreatitis: A systematic review and meta-analysis. United Eur. Gastroenterol. J. 2016, 4, 725–732. [Google Scholar] [CrossRef] [PubMed]
- Nishizawa, T.; Suzuki, H.; Higuchi, H.; Ebinuma, H.; Toyoshima, O. Effects of encircled abdominal compression device in colonoscopy: A meta-analysis. J. Clin. Med. 2019, 9, 11. [Google Scholar] [CrossRef]
- Nishizawa, T.; Suzuki, H.; Sagara, S.; Kanai, T.; Yahagi, N. Dexmedetomidine versus midazolam for gastrointestinal endoscopy: A meta-analysis. Dig. Endosc. 2015, 27, 8–15. [Google Scholar] [CrossRef]
- Nishizawa, T.; Suzuki, H.; Goto, O.; Ogata, H.; Kanai, T.; Yahagi, N. Effect of prophylactic clipping in colorectal endoscopic resection: A meta-analysis of randomized controlled studies. United Eur. Gastroenterol. J. 2017, 5, 859–867. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. B.M.J. 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Ng, Q.X.; Soh, A.Y.S.; Loke, W.; Venkatanarayanan, N.; Lim, D.Y.; Yeo, W.S. A meta-analysis of the clinical use of curcumin for irritable bowel syndrome (IBS). J. Clin. Med. 2018, 7, 298. [Google Scholar] [CrossRef]
- Nishizawa, T.; Suzuki, H.; Fujimoto, A.; Ochiai, Y.; Kanai, T.; Naohisa, Y. Effects of carbon dioxide insufflation in balloon-assisted enteroscopy: A systematic review and meta-analysis. United Eur. Gastroenterol. J. 2016, 4, 11–17. [Google Scholar] [CrossRef]
- Sakurai, K.; Nagahara, A.; Inoue, K.; Akiyama, J.; Mabe, K.; Suzuki, J.; Habu, Y.; Araki, A.; Suzuki, T.; Satoh, K.; et al. Efficacy of omeprazole, famotidine, mosapride and teprenone in patients with upper gastrointestinal symptoms: An omeprazole-controlled randomized study (J-FOCUS). BMC Gastroenterol. 2012, 12, 42. [Google Scholar] [CrossRef] [PubMed]
- Sakaguchi, M.; Takao, M.; Hashimoto, T.; Muroya, M.; Muroya, M.; Mashima, K.; Kiyota, K.; Shiomi, M. Efficacy of acid secretion inhibitors for FD symptoms: Multicenter study. Dig. Med. 2009, 48, 430–438. [Google Scholar]
- Konda, Y.; Iwano, M.; Chiba, T. Comparison of PPI and prokinetics for patients with non erosive reflux disease. Dign. Treat. 2007, 95, 149–152. [Google Scholar]
- Tack, J.; Camilleri, M.; Chang, L.; Chey, W.D.; Galligan, J.J.; Lacy, B.E.; Muller-Lissner, S.; Quigley, E.M.; Schuurkes, J.; De Maeyer, J.H.; et al. Systematic review: Cardiovascular safety profile of 5-HT(4) agonists developed for gastrointestinal disorders. Aliment. Pharm. 2012, 35, 745–767. [Google Scholar] [CrossRef]
- Carlsson, L.; Amos, G.J.; Andersson, B.; Drews, L.; Duker, G.; Wadstedt, G. Electrophysiological characterization of the prokinetic agents cisapride and mosapride in vivo and in vitro: Implications for proarrhythmic potential? J. Pharm. Exp. 1997, 282, 220–227. [Google Scholar]
- Katoh, T.; Saitoh, H.; Ohno, N.; Tateno, M.; Nakamura, T.; Dendo, I.; Kobayashi, S.; Nagasawa, K. Drug interaction between mosapride and erythromycin without electrocardiographic changes. Jpn. Heart J. 2003, 44, 225–234. [Google Scholar] [CrossRef]
- Endo, J.; Nomura, M.; Morishita, S.; Uemura, N.; Inoue, S.; Kishi, S.; Kawaguchi, R.; Iga, A.; Ito, S.; Nakaya, Y. Influence of mosapride citrate on gastric motility and autonomic nervous function: Evaluation by spectral analyses of heart rate and blood pressure variabilities, and by electrogastrography. J. Gastroenterol. 2002, 37, 888–895. [Google Scholar] [CrossRef]
- Arai, K.; Takeuchi, Y.; Watanabe, H.; Tsukurimichi, A.; Uchida, N.; Imawari, M. Prokinetics influence the pharmacokinetics of rabeprazole. Digestion 2008, 78, 67–71. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Country | Diagnosis of GERD | Assessment of | Range of | Duration | PPI | Allocation | Patients | Age | Gender |
|---|---|---|---|---|---|---|---|---|---|---|
| Year | reflux symptoms | symptom score | (weeks) | (dose/day) | number | ±SD | M/F | |||
| Madan | India | GERD symptoms >2/week | Multiplying the scores for severity | 0–18 | 8 | Pantoprazole | PPI | 33 | 34.7 ± 10.8 | 19/14 |
| 2004 | Screening endoscopy | (0–3) and frequency (0–3) for 2 items | 80 mg | PPI + Mosapride | 28 | 36.5 ± 12.8 | 21/7 | |||
| Hsu | Taiwan | GERD symptoms | FSSG; sum of | 0–48 | 4 | Lansoprazole | PPI | 46 | 47 ± 8.9 | 25/21 |
| 2010 | Esophagitis at endoscopy | frequency (0–4) for 12 items | 30 mg | PPI + Mosapride | 50 | 47 ± 14.8 | 23/27 | |||
| Miwa | Japan | GERD symptoms >2/week | Reflux symptoms using 10-cm | 0–10 | 4 | Omeprazole | PPI | 95 | 52.2 ± 15.8 | 35/60 |
| 2011 | No esophagitis at endoscopy | visual analogue scale (VAS) | 10 mg | PPI + Mosapride | 97 | 52.1 ± 16.1 | 37/60 | |||
| Lim | Korea | Typical GERD symptoms | Severity; none (0), mild (1), | 0–3 | 8 | Pantoprazole | PPI | 15 | 55.3 (25–66) * | 10/5 |
| 2013 | Normal gastric emptying scan | moderate (2) or severe (3) | 40 mg | PPI + Mosapride | 15 | 48.5 (20–70) * | 6/9 | |||
| Cho | Korea | GERD symptoms >2/week | Severity; none, mild, moderate, | 1–5 | 4 | Esomeprazole | PPI | 19 | 43 ± 15 | 9/10 |
| 2013 | Endoscopy, 48 h pH monitoring | severe, or very severe | 40 mg | PPI + Mosapride | 24 | 49 ± 16 | 15/9 | |||
| Yamaji | Japan | GERD symptoms >2/week | FSSG; sum of | 0–48 | 4 | Omeprazole | PPI | 28 | 61.7 ± 11.9 | 9/19 |
| 2014 | Screening endoscopy | frequency (0–4) for 12 items | 10 mg | PPI + Mosapride | 22 | 65.0 ± 11.6 | 4/18 | |||
| Lee | Korea | GERD symptoms >2/week | Multiplying the scores for severity | 0–120 | 8 | Esomeprazole | PPI | 53 | 55.8 ± 8.4 | 37/16 |
| 2017 | Esophagitis at endoscopy | (0–4) and frequency (0–5) for 6 items | 40 mg | PPI + Mosapride | 56 | 54.9 ± 11.1 | 34/22 | |||
| Sirina | Thailand | GERD symptoms >2/week | FSSG; sum of | 0–48 | 4 | Omeprazole | PPI | 22 | 53.1 ± 11.9 | 6/16 |
| wasatien | 2019 | Screening endoscopy | frequency (0–4) for 12 items | 20 mg | PPI + Mosapride | 22 | 49.2 ± 13.8 | 7/15 | ||
| Xiao | China | GERD symptoms and cough | RDQ; sum of frequency (0–5) | 0–40 | 12 | Omeprazole | PPI | 45 | 39.9 ± 10.1 | 29/16 |
| 2019 | Screening endoscopy | and severity (0–5) for 4 items | 40 mg | PPI + Mosapride | 45 | 40.6 ± 6.0 | 24/21 |
| First | Random Sequence | Allocation | Blinding of Participants | Blinding of Outcome | Adequate Assessment | Selective Reporting | No Other |
|---|---|---|---|---|---|---|---|
| author | generation | concealment | and personnel | assessment | of incomplete outcome | avoided | bias |
| Madan | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Hsu | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Miwa | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Lim | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Cho | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Yamaji | Yes | Yes | No | No | Yes | Yes | Yes |
| Lee | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Sirinawasatien | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Xiao | Yes | Unclear | No | No | Yes | Yes | Yes |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nishizawa, T.; Mori, K.; Yoshida, S.; Ebinuma, H.; Toyoshima, O.; Suzuki, H. Additional Mosapride to Proton Pump Inhibitor for Gastroesophageal Reflux Disease: A Meta-Analysis. J. Clin. Med. 2020, 9, 2705. https://doi.org/10.3390/jcm9092705
Nishizawa T, Mori K, Yoshida S, Ebinuma H, Toyoshima O, Suzuki H. Additional Mosapride to Proton Pump Inhibitor for Gastroesophageal Reflux Disease: A Meta-Analysis. Journal of Clinical Medicine. 2020; 9(9):2705. https://doi.org/10.3390/jcm9092705
Chicago/Turabian StyleNishizawa, Toshihiro, Kiyoto Mori, Shuntaro Yoshida, Hirotoshi Ebinuma, Osamu Toyoshima, and Hidekazu Suzuki. 2020. "Additional Mosapride to Proton Pump Inhibitor for Gastroesophageal Reflux Disease: A Meta-Analysis" Journal of Clinical Medicine 9, no. 9: 2705. https://doi.org/10.3390/jcm9092705
APA StyleNishizawa, T., Mori, K., Yoshida, S., Ebinuma, H., Toyoshima, O., & Suzuki, H. (2020). Additional Mosapride to Proton Pump Inhibitor for Gastroesophageal Reflux Disease: A Meta-Analysis. Journal of Clinical Medicine, 9(9), 2705. https://doi.org/10.3390/jcm9092705