Contour Changes Following Immediate Placement of Ultra-Wide Implants in Molar Extraction Sockets without Bone Grafting

 ,
,
Abstract
1. Introduction
2. Experimental Section
2.1. Clinical Procedure
2.2. Data Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Schropp, L.; Wenzel, A.; Kostopoulos, L.; Karring, T. Bone healing and soft tissue contour changes following single-tooth extraction: A clinical and radiographic 12-month prospective study. Int. J. Periodontics Restor. Dent. 2003, 23, 313–323. [Google Scholar]
- Trombelli, L.; Farina, R.; Marzola, A.; Bozzi, L.; Liljenberg, B.; Lindhe, J. Modeling and remodeling of human extraction sockets. J. Clin. Periodontol. 2008, 35, 630–639. [Google Scholar] [CrossRef] [PubMed]
- Araujo, M.G.; Lindhe, J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J. Clin. Periodontol. 2005, 32, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Bartee, B.K. Extraction site reconstruction for alveolar ridge preservation. Part 2: Membrane-assisted surgical technique. J. Oral Implantol. 2001, 27, 194–197. [Google Scholar] [CrossRef]
- Farina, R.; Pramstraller, M.; Franceschetti, G.; Pramstraller, C.; Trombelli, L. Alveolar ridge dimensions in maxillary posterior sextants: A retrospective comparative study of dentate and edentulous sites using computerized tomography data. Clin. Oral Implants Res. 2011, 22, 1138–1144. [Google Scholar] [CrossRef] [PubMed]
- Jahangiri, L.; Devlin, H.; Ting, K.; Nishimura, I. Current perspectives in residual ridge remodeling and its clinical implications: A review. J. Prosthet. Dent. 1998, 80, 224–237. [Google Scholar] [CrossRef]
- Jeffcoat, M.K. Bone loss in the oral cavity. J. Bone Miner. Res. 1993, 8 (Suppl. S2), S467–S473. [Google Scholar] [CrossRef]
- Tallgren, A. The continuing reduction of the residual alveolar ridges in complete denture wearers: A mixed-longitudinal study covering 25 years. J. Prosthet. Dent. 1972, 27, 120–132. [Google Scholar] [CrossRef]
- Lekovic, V.; Camargo, P.M.; Klokkevold, P.R.; Weinlaender, M.; Kenney, E.B.; Dimitrijevic, B.; Nedic, M. Preservation of alveolar bone in extraction sockets using bioabsorbable membranes. J. Periodontol. 1998, 69, 1044–1049. [Google Scholar] [CrossRef]
- Lekovic, V.; Kenney, E.B.; Weinlaender, M.; Han, T.; Klokkevold, P.; Nedic, M.; Orsini, M. A bone regenerative approach to alveolar ridge maintenance following tooth extraction. Report of 10 cases. J. Periodontol. 1997, 68, 563–570. [Google Scholar] [CrossRef]
- Bressan, E.; Ferrarese, N.; Pramstraller, M.; Lops, D.; Farina, R.; Tomasi, C. Ridge Dimensions of the Edentulous Mandible in Posterior Sextants: An Observational Study on Cone Beam Computed Tomography Radiographs. Implant. Dent. 2017, 26, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Pinho, M.N.; Roriz, V.L.; Novaes, A.B., Jr.; Taba, M., Jr.; Grisi, M.F.; de Souza, S.L.; Palioto, D.B. Titanium membranes in prevention of alveolar collapse after tooth extraction. Implant. Dent. 2006, 15, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Van der Weijden, F.; Dell’Acqua, F.; Slot, D.E. Alveolar bone dimensional changes of post-extraction sockets in humans: A systematic review. J. Clin. Periodontol. 2009, 36, 1048–1058. [Google Scholar] [CrossRef] [PubMed]
- Bodic, F.; Hamel, L.; Lerouxel, E.; Basle, M.F.; Chappard, D. Bone loss and teeth. Jt. Bone Spine 2005, 72, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, J.; Zhao, D.; Wu, Y.; Xu, C. Evaluation of Outcomes of Dental Implants Inserted by Flapless or Flapped Procedure: A Meta-Analysis. Implant. Dent. 2018, 27, 588–598. [Google Scholar] [CrossRef] [PubMed]
- Yaffe, A.; Fine, N.; Binderman, I. Regional accelerated phenomenon in the mandible following mucoperiosteal flap surgery. J. Periodontol. 1994, 65, 79–83. [Google Scholar] [CrossRef]
- Fickl, S.; Zuhr, O.; Wachtel, H.; Bolz, W.; Huerzeler, M. Tissue alterations after tooth extraction with and without surgical trauma: A volumetric study in the beagle dog. J. Clin. Periodontol. 2008, 35, 356–363. [Google Scholar] [CrossRef]
- Blanco, J.; Nunez, V.; Aracil, L.; Munoz, F.; Ramos, I. Ridge alterations following immediate implant placement in the dog: Flap versus flapless surgery. J. Clin. Periodontol. 2008, 35, 640–648. [Google Scholar] [CrossRef]
- O’Neill, J.E.; Yeung, S.C. Do dental implants preserve and maintain alveolar bone? J. Investig. Clin. Dent. 2011, 2, 229–235. [Google Scholar] [CrossRef]
- Van Nimwegen, W.G.; Goene, R.J.; Van Daelen, A.C.; Stellingsma, K.; Raghoebar, G.M.; Meijer, H.J. Immediate implant placement and provisionalisation in the aesthetic zone. J. Oral Rehabil. 2016, 43, 745–752. [Google Scholar] [CrossRef]
- Arora, H.; Khzam, N.; Roberts, D.; Bruce, W.L.; Ivanovski, S. Immediate implant placement and restoration in the anterior maxilla: Tissue dimensional changes after 2-5 year follow up. Clin. Implant Dent. Relat. Res. 2017, 19, 694–702. [Google Scholar] [CrossRef]
- Covani, U.; Bortolaia, C.; Barone, A.; Sbordone, L. Bucco-lingual crestal bone changes after immediate and delayed implant placement. J. Periodontol. 2004, 75, 1605–1612. [Google Scholar] [CrossRef]
- Paolantonio, M.; Dolci, M.; Scarano, A.; d’Archivio, D.; di Placido, G.; Tumini, V.; Piattelli, A. Immediate implantation in fresh extraction sockets. A controlled clinical and histological study in man. J. Periodontol. 2001, 72, 1560–1571. [Google Scholar] [CrossRef]
- Schultz, A.J. Guided tissue regeneration (GTR) of nonsubmerged implants in immediate extraction sites. Pract. Periodontics Aesthet. Dent. 1993, 5, 59–65, quiz 66. [Google Scholar]
- Werbitt, M.J.; Goldberg, P.V. The immediate implant: Bone preservation and bone regeneration. Int. J. Periodontics Restor. Dent. 1992, 12, 206–217. [Google Scholar]
- Denissen, H.W.; Kalk, W.; Veldhuis, H.A.; van Waas, M.A. Anatomic consideration for preventive implantation. Int. J. Oral Maxillofac. Implant. 1993, 8, 191–196. [Google Scholar]
- Watzek, G.; Haider, R.; Mensdorff-Pouilly, N.; Haas, R. Immediate and delayed implantation for complete restoration of the jaw following extraction of all residual teeth: A retrospective study comparing different types of serial immediate implantation. Int. J. Oral Maxillofac. Implant. 1995, 10, 561–567. [Google Scholar]
- Esposito, M.; Grusovin, M.G.; Polyzos, I.P.; Felice, P.; Worthington, H.V. Timing of implant placement after tooth extraction: Immediate, immediate-delayed or delayed implants? A Cochrane systematic review. Eur. J. Oral Implantol. 2010, 3, 189–205. [Google Scholar]
- Tonetti, M.S.; Cortellini, P.; Graziani, F.; Cairo, F.; Lang, N.P.; Abundo, R.; Conforti, G.P.; Marquardt, S.; Rasperini, G.; Silvestri, M.; et al. Immediate versus delayed implant placement after anterior single tooth extraction: The timing randomized controlled clinical trial. J. Clin. Periodontol. 2017, 44, 215–224. [Google Scholar] [CrossRef]
- Maiorana, C.; Poli, P.P.; Deflorian, M.; Testori, T.; Mandelli, F.; Nagursky, H.; Vinci, R. Alveolar socket preservation with demineralised bovine bone mineral and a collagen matrix. J. Periodontal Implant. Sci 2017, 47, 194–210. [Google Scholar] [CrossRef]
- Mozzati, M.; Gallesio, G.; Staiti, G.; Iezzi, G.; Piattelli, A.; Mortellaro, C. Socket Preservation Using a Biomimetic Nanostructured Matrix and Atraumatic Surgical Extraction Technique. J. Craniofac. Surg. 2017, 28, 1042–1045. [Google Scholar] [CrossRef]
- Amato, F.; Polara, G.; Spedicato, G.A. Tissue Dimensional Changes in Single-Tooth Immediate Extraction Implant Placement in the Esthetic Zone: A Retrospective Clinical Study. Int. J. Oral Maxillofac Implant. 2018, 33, 439–447. [Google Scholar] [CrossRef]
- Ramaglia, L.; Sbordone, C.; Saviano, R.; Martuscelli, R.; Sbordone, L. Marginal masticatory mucosa dimensional changes in immediate post-extractive implants: A 2 year prospective cohort study. Clin. Oral Implant. Res. 2015, 26, 1495–1502. [Google Scholar] [CrossRef]
- Arora, H.; Ivanovski, S. Immediate and early implant placement in single-tooth gaps in the anterior maxilla: A prospective study on ridge dimensional, clinical, and aesthetic changes. Clin. Oral Implant. Res. 2018. [Google Scholar] [CrossRef]
- Vandeweghe, S.; Hattingh, A.; Wennerberg, A.; Bruyn, H.D. Surgical protocol and short-term clinical outcome of immediate placement in molar extraction sockets using a wide body implant. J. Oral Maxillofac. Res. 2011, 2, e1. [Google Scholar] [CrossRef]
- Vandeweghe, S.; Ackermann, A.; Bronner, J.; Hattingh, A.; Tschakaloff, A.; De Bruyn, H. A retrospective, multicenter study on a novo wide-body implant for posterior regions. Clin. Implant Dent. Relat. Res. 2012, 14, 281–292. [Google Scholar] [CrossRef]
- Hattingh, A.; Hommez, G.; De Bruyn, H.; Huyghe, M.; Vandeweghe, S. A prospective study on ultra-wide diameter dental implants for immediate molar replacement. Clin. Implant Dent. Relat. Res. 2018, 20, 1009–1015. [Google Scholar] [CrossRef]
- Chen, S.T.; Darby, I.B.; Reynolds, E.C. A prospective clinical study of non-submerged immediate implants: Clinical outcomes and esthetic results. Clin. Oral Implant. Res. 2007, 18, 552–562. [Google Scholar] [CrossRef]
- Evans, C.D.; Chen, S.T. Esthetic outcomes of immediate implant placements. Clin. Oral Implant. Res. 2008, 19, 73–80. [Google Scholar] [CrossRef]
- Hattingh, A.C.; De Bruyn, H.; Ackermann, A.; Vandeweghe, S. Immediate Placement of Ultrawide-Diameter Implants in Molar Sockets: Description of a Recommended Technique. Int. J. Periodontics Restor. Dent. 2018, 38, 17–23. [Google Scholar] [CrossRef]
- Alqahtani, S.; Alsheraimi, A.; Alshareef, A.; Alsaban, R.; Alqahtani, A.; Almgran, M.; Eldesouky, M.; Al-Omar, A. Maxillary Sinus Pneumatization Following Extractions in Riyadh, Saudi Arabia: A Cross-sectional Study. Cureus 2020, 12, e6611. [Google Scholar] [CrossRef]
- Cavalcanti, M.C.; Guirado, T.E.; Sapata, V.M.; Costa, C.; Pannuti, C.M.; Jung, R.E.; Cesar Neto, J.B. Maxillary sinus floor pneumatization and alveolar ridge resorption after tooth loss: A cross-sectional study. Braz. Oral Res. 2018, 32, e64. [Google Scholar] [CrossRef]
- Pramstraller, M.; Schincaglia, G.P.; Vecchiatini, R.; Farina, R.; Trombelli, L. Alveolar ridge dimensions in mandibular posterior regions: A retrospective comparative study of dentate and edentulous sites using computerized tomography data. Surg. Radiol. Anat. 2018, 40, 1419–1428. [Google Scholar] [CrossRef]
- Smith, R.B.; Tarnow, D.P. Classification of molar extraction sites for immediate dental implant placement: Technical note. Int.. J. Oral Maxillofac. Implant. 2013, 28, 911–916. [Google Scholar] [CrossRef]
- Tallarico, M.; Xhanari, E.; Pisano, M.; Gatti, F.; Meloni, S.M. Molar replacement with 7 mm-wide diameter implants: To place the implant immediately or to wait 4 months after socket preservation? 1 year after loading results from a randomised controlled trial. Eur. J. Oral Implantol. 2017, 10, 169–178. [Google Scholar]
- Cosyn, J.; Hooghe, N.; De Bruyn, H. A systematic review on the frequency of advanced recession following single immediate implant treatment. J. Clin. Periodontol. 2012, 39, 582–589. [Google Scholar] [CrossRef]
- Lops, D.; Chiapasco, M.; Rossi, A.; Bressan, E.; Romeo, E. Incidence of inter-proximal papilla between a tooth and an adjacent immediate implant placed into a fresh extraction socket: 1-year prospective study. Clin. Oral Implant. Res. 2008, 19, 1135–1140. [Google Scholar] [CrossRef]
- Romeo, E.; Lops, D.; Rossi, A.; Storelli, S.; Rozza, R.; Chiapasco, M. Surgical and prosthetic management of interproximal region with single-implant restorations: 1-year prospective study. J. Periodontol. 2008, 79, 1048–1055. [Google Scholar] [CrossRef]
- Slagter, K.W.; den Hartog, L.; Bakker, N.A.; Vissink, A.; Meijer, H.J.; Raghoebar, G.M. Immediate placement of dental implants in the esthetic zone: A systematic review and pooled analysis. J. Periodontol. 2014, 85, e241–e250. [Google Scholar] [CrossRef]
- Cordaro, L.; Torsello, F.; Roccuzzo, M. Clinical outcome of submerged vs. non-submerged implants placed in fresh extraction sockets. Clin. Oral Implant. Res. 2009, 20, 1307–1313. [Google Scholar] [CrossRef]
- Kan, J.Y.; Rungcharassaeng, K.; Lozada, J.L.; Zimmerman, G. Facial gingival tissue stability following immediate placement and provisionalization of maxillary anterior single implants: A 2- to 8-year follow-up. Int. J. Oral Maxillofac. Implant. 2011, 26, 179–187. [Google Scholar]
- Chappuis, V.; Engel, O.; Shahim, K.; Reyes, M.; Katsaros, C.; Buser, D. Soft Tissue Alterations in Esthetic Postextraction Sites: A 3-Dimensional Analysis. J. Dent. Res. 2015, 94, 187S–193S. [Google Scholar] [CrossRef]
- Chappuis, V.; Engel, O.; Reyes, M.; Shahim, K.; Nolte, L.P.; Buser, D. Ridge alterations post-extraction in the esthetic zone: A 3D analysis with CBCT. J. Dent. Res. 2013, 92, 195S–201S. [Google Scholar] [CrossRef]
- Cardaropoli, D.; Gaveglio, L.; Gherlone, E.; Cardaropoli, G. Soft tissue contour changes at immediate implants: A randomized controlled clinical study. Int. J. Periodontics Restor. Dent. 2014, 34, 631–637. [Google Scholar] [CrossRef]
- Tian, J.; Wei, D.; Zhao, Y.; Di, P.; Jiang, X.; Lin, Y. Labial soft tissue contour dynamics following immediate implants and immediate provisionalization of single maxillary incisors: A 1-year prospective study. Clin. Implant Dent. Relat. Res. 2019, 21, 492–502. [Google Scholar] [CrossRef]
- Theye, C.E.G.; Hattingh, A.; Cracknell, T.J.; Oettle, A.C.; Steyn, M.; Vandeweghe, S. Dento-alveolar measurements and histomorphometric parameters of maxillary and mandibular first molars, using micro-CT. Clin. Implant Dent. Relat. Res. 2018, 20, 550–561. [Google Scholar] [CrossRef]
- Chen, S.T.; Buser, D. Esthetic outcomes following immediate and early implant placement in the anterior maxilla--a systematic review. Int. J. Oral Maxillofac Implant. 2014, 29, 186–215. [Google Scholar] [CrossRef]
- De Bruyn, H.; Raes, F.; Cooper, L.F.; Reside, G.; Garriga, J.S.; Tarrida, L.G.; Wiltfang, J.; Kern, M. Three-years clinical outcome of immediate provisionalization of single Osseospeed() implants in extraction sockets and healed ridges. Clin. Oral Implant. Res. 2013, 24, 217–223. [Google Scholar] [CrossRef]
- Kinaia, B.M.; Ambrosio, F.; Lamble, M.; Hope, K.; Shah, M.; Neely, A.L. Soft Tissue Changes Around Immediately Placed Implants: A Systematic Review and Meta-Analyses With at Least 12 Months of Follow-Up After Functional Loading. J. Periodontol. 2017, 88, 876–886. [Google Scholar] [CrossRef]
- Hof, M.; Pommer, B.; Ambros, H.; Jesch, P.; Vogl, S.; Zechner, W. Does Timing of Implant Placement Affect Implant Therapy Outcome in the Aesthetic Zone? A Clinical, Radiological, Aesthetic, and Patient-Based Evaluation. Clin. Implant Dent. Relat. Res. 2015, 17, 1188–1199. [Google Scholar] [CrossRef]
- Checchi, V.; Felice, P.; Zucchelli, G.; Barausse, C.; Piattelli, M.; Pistilli, R.; Grandi, G.; Esposito, M. Wide diameter immediate post-extractive implants vs delayed placement of normal-diameter implants in preserved sockets in the molar region: 1-year post-loading outcome of a randomised controlled trial. Eur. J. Oral Implantol. 2017, 10, 263–278. [Google Scholar] [PubMed]
- Cecchinato, D.; Lops, D.; Salvi, G.E.; Sanz, M. A prospective, randomized, controlled study using OsseoSpeed implants placed in maxillary fresh extraction socket: Soft tissues response. Clin. Oral Implant. Res. 2015, 26, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Sanz, M.; Cecchinato, D.; Ferrus, J.; Salvi, G.E.; Ramseier, C.; Lang, N.P.; Lindhe, J. Implants placed in fresh extraction sockets in the maxilla: Clinical and radiographic outcomes from a 3-year follow-up examination. Clin. Oral Implant. Res. 2014, 25, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Farmer, M.; Darby, I. Ridge dimensional changes following single-tooth extraction in the aesthetic zone. Clin. Oral Implant. Res. 2014, 25, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Iasella, J.M.; Greenwell, H.; Miller, R.L.; Hill, M.; Drisko, C.; Bohra, A.A.; Scheetz, J.P. Ridge preservation with freeze-dried bone allograft and a collagen membrane compared to extraction alone for implant site development: A clinical and histologic study in humans. J. Periodontol. 2003, 74, 990–999. [Google Scholar] [CrossRef]
- Murugesan, A.; Sivakumar, A. Comparison of accuracy of mesiodistal tooth measurements made in conventional study models and digital models obtained from intraoral scan and desktop scan of study models. J. Orthod. 2020. [Google Scholar] [CrossRef]
- Tomita, Y.; Uechi, J.; Konno, M.; Sasamoto, S.; Iijima, M.; Mizoguchi, I. Accuracy of digital models generated by conventional impression/plaster-model methods and intraoral scanning. Dent. Mater. J. 2018, 37, 628–633. [Google Scholar] [CrossRef]
- Osnes, C.A.; Wu, J.H.; Venezia, P.; Ferrari, M.; Keeling, A.J. Full arch precision of six intraoral scanners in vitro. J. Prosthodont. Res. 2020, 64, 6–11. [Google Scholar] [CrossRef]
- Schmidt, A.; Klussmann, L.; Wostmann, B.; Schlenz, M.A. Accuracy of Digital and Conventional Full-Arch Impressions in Patients: An Update. J. Clin. Med. 2020, 9, 688. [Google Scholar] [CrossRef]
- Fageeh, H.N.; Meshni, A.A.; Jamal, H.A.; Preethanath, R.S.; Halboub, E. The accuracy and reliability of digital measurements of gingival recession versus conventional methods. BMC Oral Health 2019, 19, 154. [Google Scholar] [CrossRef]
- Lehmann, K.M.; Kasaj, A.; Ross, A.; Kammerer, P.W.; Wagner, W.; Scheller, H. A new method for volumetric evaluation of gingival recessions: A feasibility study. J. Periodontol. 2012, 83, 50–54. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, K.M.; Kasaj, A.; Ross, A.; Willershausen, I.; Schmidtmann, I.; Staedt, H.; Scheller, H. A novel method for evaluating periodontal recession: A feasibility study. Int. J. Comput. Dent. 2011, 14, 297–307. [Google Scholar] [PubMed]
- Schneider, D.; Ender, A.; Truninger, T.; Leutert, C.; Sahrmann, P.; Roos, M.; Schmidlin, P. Comparison between clinical and digital soft tissue measurements. J. Esthet. Restor. Dent. 2014, 26, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Blanco, J.; Carral, C.; Argibay, O.; Linares, A. Implant placement in fresh extraction sockets. Periodontol. 2000 2019, 79, 151–167. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 4 Months | 12 Months | ||
|---|---|---|---|
| Buccal horizontal reduction | |||
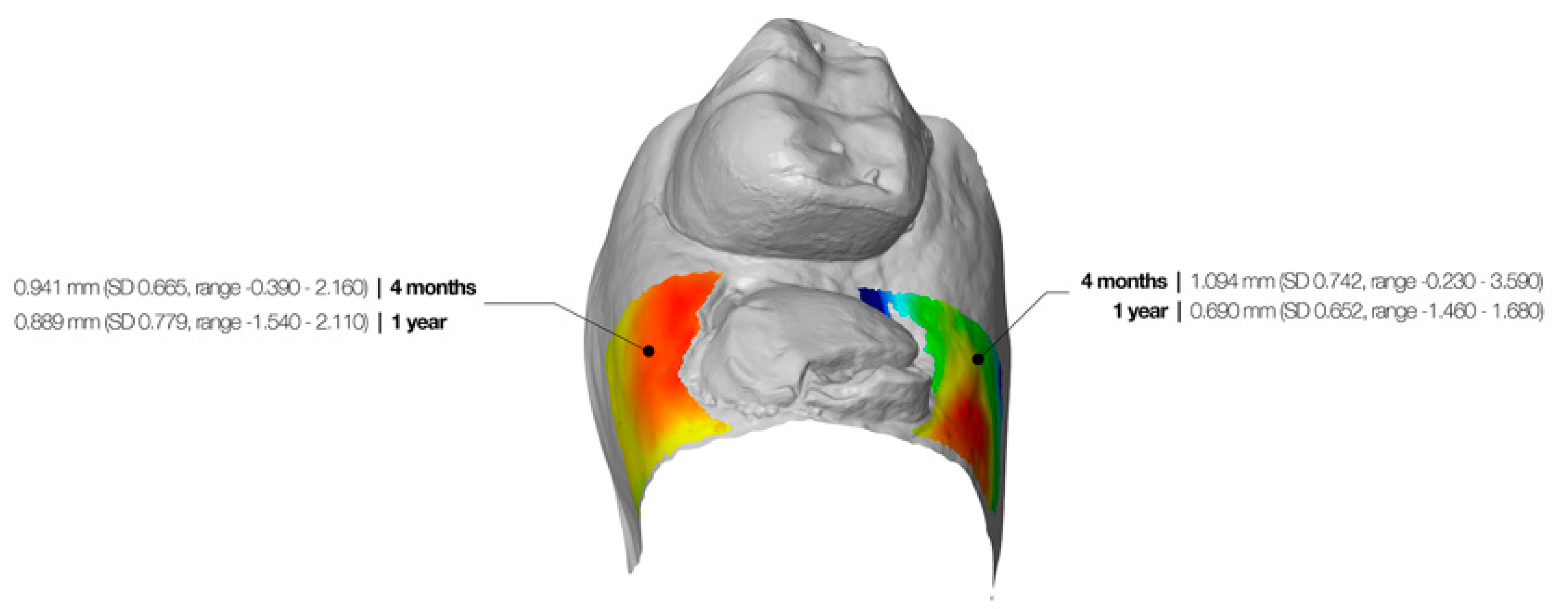
| 0.94 mm (SD 0.67, range −0.39–2.16) | 0.89 mm (SD 0.78, range −1.54–2.11) | p = 0.933 | |
| Buccal midfacial reduction | |||
| Top 2 mm ROI | 1.53 mm (SD 0.96, range −0.42–3.85) | 1.43 mm (SD 0.74, range 0.05–3.23) | p = 0.195 |
| Middle 2 mm ROI | 1.31 mm (SD 0.73, range −0.09–2.79) | 1.59 mm (SD 0.81, range 0.09–3.15) | p = 0.010 |
| Bottom 2 mm ROI | 0.86 mm (SD 0.62, range 0.10–2.78) | 1.33 mm (SD 0.76, range −0.23–2.88) | p = 0.001 |
| Overall | 1.23 mm (SD 0.71, range −0.09–3.14) | 1.45 mm (SD 0.70, range 0.18–3.09) | p = 0.013 |
| Palatal/Lingual horizontal reduction | |||
| 1.09 mm (SD 0.74, range −0.23–3.59) | 0.69 mm (SD 0.65, range −1.46–1.68) | p = 0.001 | |
| Palatal/Lingual midfacial reduction | |||
| Top 2 mm ROI | 1.68 mm (SD 0.81, range 0.48–3.62) | 1.18 mm (SD 0.81, range −0.32–2.97) | p = 0.010 |
| Middle 2 mm ROI | 1.51 mm (SD 0.73, range 0.22–3.62) | 1.35 mm (SD 0.72, range 0.30–3.32) | p = 0.186 |
| Bottom 2 mm ROI | 1.11 mm (SD 0.92, range 0.20–4.02) | 0.97 mm (SD 0.68, range 0.09–3.10) | p = 0.302 |
| Overall | 1.43 mm (SD 0.74, range 0.34–3.75) | 1.16 mm (SD 0.67, range 0.23–3.13) | p = 0.044 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hattingh, A.; De Bruyn, H.; Van Weehaeghe, M.; Hommez, G.; Vandeweghe, S. Contour Changes Following Immediate Placement of Ultra-Wide Implants in Molar Extraction Sockets without Bone Grafting. J. Clin. Med. 2020, 9, 2504. https://doi.org/10.3390/jcm9082504
Hattingh A, De Bruyn H, Van Weehaeghe M, Hommez G, Vandeweghe S. Contour Changes Following Immediate Placement of Ultra-Wide Implants in Molar Extraction Sockets without Bone Grafting. Journal of Clinical Medicine. 2020; 9(8):2504. https://doi.org/10.3390/jcm9082504
Chicago/Turabian StyleHattingh, André, Hugo De Bruyn, Manù Van Weehaeghe, Geert Hommez, and Stefan Vandeweghe. 2020. "Contour Changes Following Immediate Placement of Ultra-Wide Implants in Molar Extraction Sockets without Bone Grafting" Journal of Clinical Medicine 9, no. 8: 2504. https://doi.org/10.3390/jcm9082504
APA StyleHattingh, A., De Bruyn, H., Van Weehaeghe, M., Hommez, G., & Vandeweghe, S. (2020). Contour Changes Following Immediate Placement of Ultra-Wide Implants in Molar Extraction Sockets without Bone Grafting. Journal of Clinical Medicine, 9(8), 2504. https://doi.org/10.3390/jcm9082504