The Role of Health Literacy in Postpartum Weight, Diet, and Physical Activity

 ,
,  ,
,  and
and
Abstract
1. Introduction
2. Experimental Section
2.1. Evidence Acquisition
2.2. Data Sources and Searches
2.3. Study Selection
2.4. Data Extraction
2.5. Quality Assessment
2.6. Data Synthesis and Analysis
2.7. Evidence Synthesis
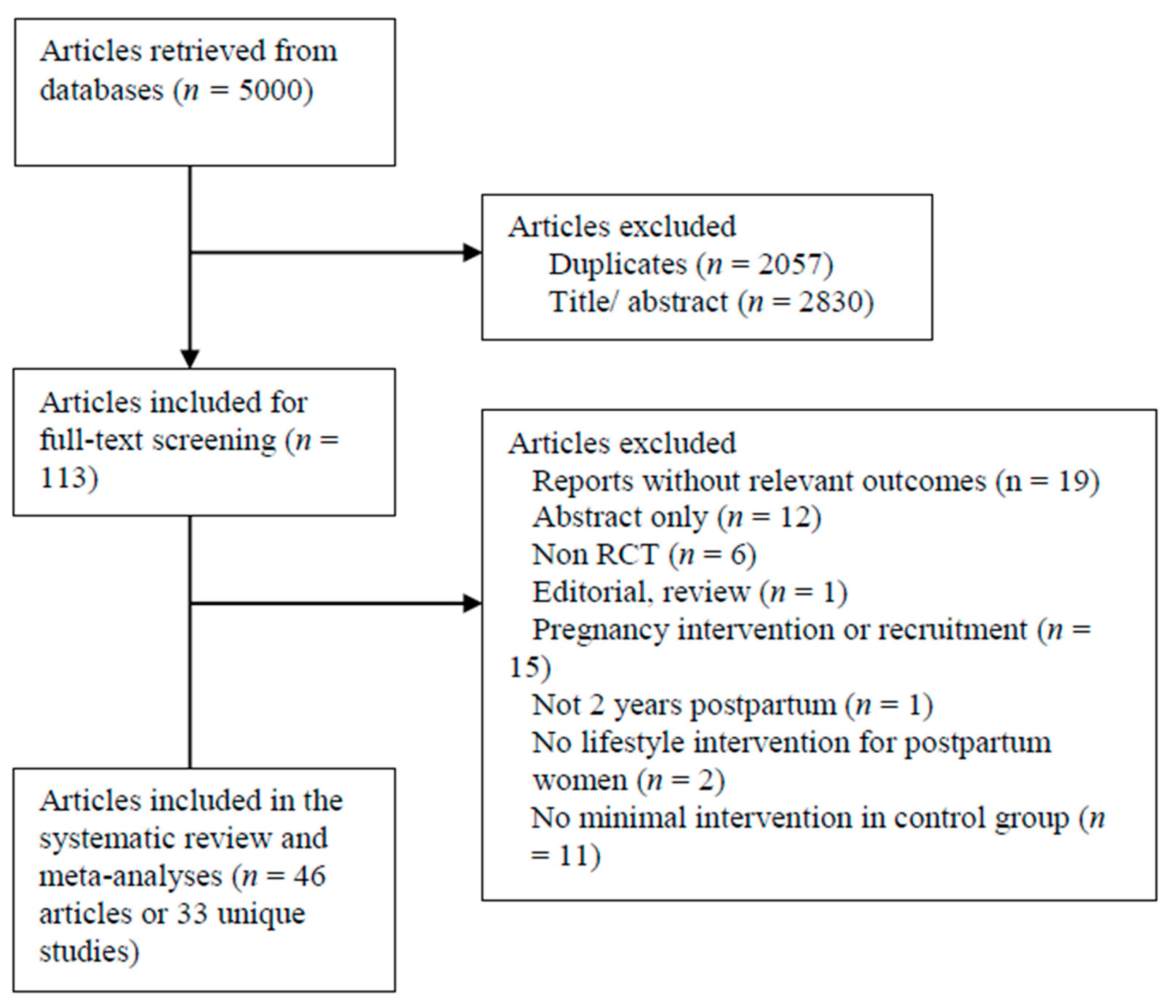
2.7.1. Identification of Studies
2.7.2. Study Characteristics
2.7.3. Quality Assessment
3. Results
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef]
- Adamson, L.; Brown, W.; Byles, J.; Chojenta, C.; Dobson, A.; Fitzgerald, D.; Hockey, R.; Loxton, D.; Powers, J.; Spallek, M.; et al. Women’s Weight: Findings from the Australian Longitudinal Study on Women’s Health; Australian Government Department of Health and Ageing: Canberra, Australia, 2007. [Google Scholar]
- Villamor, E.; Cnattingius, S. Interpregnancy weight change and risk of adverse pregnancy outcomes: A population-based study. Lancet 2006, 368, 1164–1170. [Google Scholar] [CrossRef]
- Godfrey, K.M.; Reynolds, R.M.; Prescott, S.L.; Nyirenda, M.; Jaddoe, V.W.; Eriksson, J.G.; Broekman, B.F.P. Influence of maternal obesity on the long-term health of offspring. Lancet Diabetes Endocrinol. 2017, 5, 53–64. [Google Scholar] [CrossRef]
- WHO. Health Literacy. 2016. Available online: https://www.who.int/healthpromotion/conferences/9gchp/health-literacy/en/ (accessed on 18 February 2019).
- World Health Organization. Health Promotion Glossary; WHO: Geneva, Switzerland, 1998. [Google Scholar]
- Crondahl, K.; Karlsson, L.E. The Nexus between Health Literacy and Empowerment: A Scoping Review. SAGE Open 2016, 6, 2158244016646410. [Google Scholar] [CrossRef]
- Osborne, R.H.; Beauchamp, A.; Batterham, R. Health literacy: A concept with potential to greatly impact the infectious diseases field. Int. J. Infect. Dis. 2016, 43, 101–102. [Google Scholar] [CrossRef]
- Berkman, N.D.; Sheridan, S.L.; Donahue, K.E.; Halpern, D.J.; Crotty, K. Low health literacy and health outcomes: An updated systematic review. Ann. Intern. Med. 2011, 155, 97–107. [Google Scholar] [CrossRef]
- Cheng, Y.-L.; Shu, J.-H.; Hsu, H.-C.; Liang, Y.; Chou, R.-H.; Hsu, P.-F.; Wang, Y.-J.; Ding, Y.-Z.; Liou, T.-L.; Wang, Y.-W.; et al. High health literacy is associated with less obesity and lower Framingham risk score: Sub-study of the VGH-HEALTHCARE trial. PLoS ONE 2018, 13, e0194813. [Google Scholar] [CrossRef]
- Cheong, S.M.; Nor, N.S.M.; Ahmad, M.H.; Manickam, M.; Ambak, R.; Shahrir, S.N.; Aris, T. Improvement of health literacy and intervention measurements among low socio-economic status women: Findings from the MyBFF@home study. BMC Women’s Health 2018, 18, 99. [Google Scholar] [CrossRef]
- Abdollahi, M.; Peyman, N. The Effect of an Educational Program based on Health Literacy Strategies on Physical Activity in Postpartum Women. J. Midwifery Reprod. Health 2017, 5, 1059–1065. [Google Scholar]
- McKenna, V.B.; Sixsmith, J.; Barry, M.M. The relevance of context in understanding health literacy skills: Findings from a qualitative study. Health Expect. 2017, 20, 1049–1060. [Google Scholar] [CrossRef]
- Osborne, R.H.; Batterham, R.W.; Elsworth, G.R.; Hawkins, M.; Buchbinder, R. The grounded psychometric development and initial validation of the Health Literacy Questionnaire (HLQ). BMC Public Health 2013, 13, 658. [Google Scholar] [CrossRef] [PubMed]
- Jordan, J.; Osborne, R.; Buchbinder, R. Critical appraisal of health literacy indices revealed variable underlying constructs, narrow content and psychometric weaknesses. J. Clin. Epidemiol. 2011, 64, 366–379. [Google Scholar] [CrossRef] [PubMed]
- Beauchamp, A.; Buchbinder, R.; Dodson, S.; Batterham, R.; Elsworth, G.R.; McPhee, C.; Sparkes, L.; Hawkins, M.; Osborne, R.H. Distribution of health literacy strengths and weaknesses across socio-demographic groups: A cross-sectional survey using the Health Literacy Questionnaire (HLQ). BMC Public Health 2015, 15, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Batterham, R.W.; Hawkins, M.; Collins, P.A.; Buchbinder, R.; Osborne, R.H. Health literacy: Applying current concepts to improve health services and reduce health inequalities. Public Health 2016, 132, 3–12. [Google Scholar] [CrossRef]
- Friis, K.; Lasgaard, M.; Rowlands, G.; Osborne, R.H.; Maindal, H.T. Health Literacy Mediates the Relationship between Educational Attainment and Health Behavior: A Danish Population-Based Study. J. Health Commun. 2016, 21 (Suppl. 2), 54–60. [Google Scholar] [CrossRef]
- Beauchamp, A.; Batterham, R.; Dodson, S.; Astbury, B.; Elsworth, G.R.; McPhee, C.; Jacobson, J.; Buchbinder, R.; Osborne, R.H. Systematic development and implementation of interventions to OPtimise Health Literacy and Access (Ophelia). BMC Public Health 2017, 17, 230. [Google Scholar] [CrossRef]
- Dennison, R.A.; Ward, R.J.; Griffin, S.J.; Usher-Smith, J.A. Women’s views on lifestyle changes to reduce the risk of developing Type 2 diabetes after gestational diabetes: A systematic review, qualitative synthesis and recommendations for practice. Diabet. Med. 2019, 36, 702–717. [Google Scholar] [CrossRef]
- Lim, S.S.; Liang, X.; Hill, B.; Teede, H.; Moran, L.J.; O’Reilly, S. A systematic review and meta-analysis of intervention characteristics in postpartum weight management using the TIDieR framework: A summary of evidence to inform implementation. Obes. Rev. 2019, in press. [Google Scholar] [CrossRef]
- Website: Ahpra & National Boards. Available online: https://www.ahpra.gov.au/Support/Glossary.aspx (accessed on 25 July 2020).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Murad, M.H.; Asi, N.; Alsawas, M.; Alahdab, F. New evidence pyramid. Evid.-Based Med. 2016, 21, 125–127. [Google Scholar] [CrossRef]
- Berry, D.C.; Verbiest, S.; Hall, E.G.; Dawson, I.; Norton, D.; Willis, S.; McDonald, K.; Stuebe, A. A Postpartum Community-Based Weight Management Intervention Designed for Low-Income Women: Feasibility and Initial Efficacy Testing. J. Natl. Black Nurses’ Assoc. JNBNA 2015, 26, 29–39. [Google Scholar]
- Bertz, F.; Sparud-Lundin, C.; Winkvist, A. Transformative Lifestyle Change: Key to sustainable weight loss among women in a post-partum diet and exercise intervention. Matern. Child Nutr. 2015, 11, 631–645. [Google Scholar] [CrossRef] [PubMed]
- Colleran, H.; Lovelady, C.A. Use of MyPyramid Menu Planner for Moms in a Weight-Loss Intervention during Lactation. J. Acad. Nutr. Diet. 2012, 112, 553–558. [Google Scholar] [CrossRef] [PubMed]
- Craigie, A.M.; MacLeod, M.; Barton, K.L.; Treweek, S.; Anderson, A.S.; WeighWell Team. Supporting postpartum weight loss in women living in deprived communities: Design implications for a randomised control trial. Eur. J. Clin. Nutr. 2011, 65, 952–958. [Google Scholar] [CrossRef]
- Daley, A.J.; Blamey, R.V.; Jolly, K.; Roalfe, A.K.; Turner, N.; Coleman, S.; McGuinness, M.; Jones, I.; Sharp, D.; MacArthur, C. A pragmatic randomized controlled trial to evaluate the effectiveness of a facilitated exercise intervention as a treatment for postnatal depression: The PAM-PeRS trial. Psychol. Med. 2015, 45, 2413–2425. [Google Scholar] [CrossRef] [PubMed]
- Davenport, M.H.; Giroux, I.; Sopper, M.M.; Mottola, M.F. Postpartum Exercise Regardless of Intensity Improves Chronic Disease Risk Factors. Med. Sci. Sports Exerc. 2011, 43, 951–958. [Google Scholar] [CrossRef]
- deRosset, L.; Berry, D.C.; Sanchez-Lugo, L.; Ritter, K.; Purdum, C.; Santolim, V.; Gilliland, R.; Pender, L. Mama Sana… Usted Sana: Lessons Learned from a Postpartum Weight Loss Intervention for Hispanic Women with Infants Six Months or Less. Hisp. Health Care Int. 2013, 11, 78–86. [Google Scholar] [CrossRef]
- Dritsa, M.; Dupuis, G.; Lowensteyn, I.; Da Costa, D. Effects of home-based exercise on fatigue in postpartum depressed women: Who is more likely to benefit and why? J. Psychosom. Res. 2009, 67, 159–163. [Google Scholar] [CrossRef]
- Fjeldsoe, B.S.; Miller, Y.D.; Marshall, A.L. MobileMums: A randomized controlled trial of an SMS-based physical activity intervention. Ann. Behav. Med. 2010, 39, 101–111. Available online: http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/026/CN-00753026/frame.html (accessed on 5 November 2019). [CrossRef]
- Holmes, V.A.; Draffin, C.R.; Patterson, C.C.; Francis, L.; Irwin, J.; McConnell, M.; Farrell, B.; Brennan, S.F.; McSorley, O.; Wotherspoon, A.C.; et al. Postnatal Lifestyle Intervention for Overweight Women with Previous Gestational Diabetes: A Randomized Controlled Trial. J. Clin. Endocrinol. Metab. 2018, 103, 2478–2487. [Google Scholar] [CrossRef]
- Huang, T.-T.; Yeh, C.-Y.; Tsai, Y.-C. A diet and physical activity intervention for preventing weight retention among Taiwanese childbearing women: A randomised controlled trial. Midwifery 2011, 27, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Huseinovic, E.; Bertz, F.; Leu Agelii, M.; Hellebo Johansson, E.; Winkvist, A.; Brekke, H.K. Effectiveness of a weight loss intervention in postpartum women: Results from a randomized controlled trial in primary health care. Am. J. Clin. Nutr. 2016, 104, 362–370. [Google Scholar] [CrossRef] [PubMed]
- Huseinovic, E.; Bertz, F.; Brekke, H.K.; Winkvist, A. Two-year follow-up of a postpartum weight loss intervention: Results from a randomized controlled trial. Matern. Child Nutr. 2018, 14, e12539. [Google Scholar] [CrossRef]
- Keller, C.; Ainsworth, B.; Records, K.; Todd, M.; Belyea, M.J.; Vega-López, S.; Permana, P.A.; Coonrod, D.V.; Williams, A.N. A comparison of a social support physical activity intervention in weight management among post-partum Latinas. BMC Public Health 2014, 14, 971. [Google Scholar] [CrossRef]
- Kernot, J.; Lewis, L.; Olds, T.; Maher, C. Effectiveness of a Facebook-Delivered Physical Activity Intervention for Postpartum Women: A Randomized Controlled Trial. J. Phys. Act. Health 2019, 16, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Khodabandeh, F.; Mirghafourvand, M.; Kamalifard, M.; Charandabi, S.M.-A.; Jafarabadi, M.A. Effect of educational package on lifestyle of primiparous mothers during postpartum period: A randomized controlled clinical trial. Health Educ. Res. 2017, 32, 399–411. [Google Scholar] [CrossRef]
- Krummel, D.; Semmens, E.; MacBride, A.M.; Fisher, B. Lessons Learned from the Mothers’ Overweight Management Study in 4 West Virginia WIC Offices. J. Nutr. Educ. Behav. 2010, 42 (Suppl. 3), S52–S58. [Google Scholar] [CrossRef]
- Leermakers, E.A.; Anglin, K.; Wing, R.R. Reducing postpartum weight retention through a correspondence intervention. Int. J. Obes. Relat. Metab. Disord. 1998, 22, 1103–1109. [Google Scholar] [CrossRef]
- Lioret, S.; Campbell, K.J.; Crawford, D.; Spence, A.C.; Hesketh, K.; McNaughton, S.A. A parent focused child obesity prevention intervention improves some mother obesity risk behaviors: The Melbourne inFANT program. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 100. [Google Scholar] [CrossRef] [PubMed]
- Lovelady, C.A.; Garner, K.E.; Moreno, K.L.; Williams, J.P. The effect of weight loss in overweight, lactating women on the growth of their infants. N. Engl. J. Med. 2000, 342, 449–453. [Google Scholar] [CrossRef] [PubMed]
- Lovelady, C.A.; Stephenson, K.G.; Kuppler, K.M.; Williams, J.P. The Effects of Dieting on Food and Nutrient Intake of Lactating Women. J. Am. Diet. Assoc. 2006, 106, 908–912. [Google Scholar] [CrossRef] [PubMed]
- Lovelady, C.A.; Williams, J.P.; Garner, K.E.; Moreno, K.L.; Taylor, M.L.; Leklem, J.E. Effect of energy restriction and exercise on vitamin B-6 status of women during lactation. Med. Sci. Sports Exerc. 2001, 33, 512–518. [Google Scholar] [CrossRef] [PubMed]
- Lovelady, C.A.; Nommsen-Rivers, L.A.; McCrory, M.A.; Dewey, K.G. Effects of exercise on plasma lipids and metabolism of lactating women. Med. Sci. Sports Exerc. 1995, 27, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Lovelady, C.A.; Bopp, M.J.; Colleran, H.L.; Mackie, H.K.; Wideman, L. Effect of exercise training on loss of bone mineral density during lactation. Med. Sci. Sports Exerc. 2009, 41, 1902–1907. [Google Scholar] [CrossRef] [PubMed]
- Maturi, S.M.; Afshary, P.; Abedi, P. Effect of physical activity intervention based on a pedometer on physical activity level and anthropometric measures after childbirth: A randomized controlled trial. BMC Pregnancy Childbirth 2011, 11, 103. [Google Scholar] [CrossRef]
- McCrory, M.A.; Nommsen-Rivers, A.L.; Molé, A.P.; Lönnerdal, B.; Dewey, K.G. Randomized trial of the short-term effects of dieting compared with dieting plus aerobic exercise on lactation performance. Am. J. Clin. Nutr. 1999, 69, 959–967. [Google Scholar] [CrossRef]
- McIntyre, H.D.; Peacock, A.; Miller, Y.D.; Koh, D.; Marshall, A.L. Pilot Study of an Individualised Early Postpartum Intervention to Increase Physical Activity in Women with Previous Gestational Diabetes. Int. J. Endocrinol. 2012, 2012, 1–5. [Google Scholar] [CrossRef]
- Nicklas, J.M.; Zera, C.A.; England, L.J.; Rosner, B.A.; Horton, E.; Levkoff, S.E.; Seely, E.W. A web-based lifestyle intervention for women with recent gestational diabetes mellitus: A randomized controlled trial. Obstet. Gynecol. 2014, 124, 563–570. [Google Scholar] [CrossRef]
- Ostbye, T.; Krause, K.M.; Lovelady, C.A.; Morey, M.C.; Bastian, L.A.; Peterson, B.L.; Swamy, G.K.; Brouwer, R.J.; McBride, C.M. Active Mothers Postpartum. A Randomized Controlled Weight-Loss Intervention Trial. Am. J. Prev. Med. 2009, 37, 173–180. [Google Scholar]
- O’Toole, M.L.; Sawicki, M.A.; Artal, R. Structured diet and physical activity prevent postpartum weight retention. J. Women’s Health 2003, 12, 991–998. [Google Scholar] [CrossRef]
- Parsa, P.; Alafchi, N.; Soltani, F.; Roshanaei, G. Effects of group counselling on health-promoting behaviours in mothers during postpartum period: A randomised controlled trial. J. Clin. Diagn. Res. 2017, 11, QC09–QC13. [Google Scholar] [CrossRef]
- Tripette, J.; Haruka, M.; Yuko, G.; Kawakami, R.; Azusa, S.; Satoshi, H.; Aiko, H.; Motohiko, M. Home-Based Active Video Games to Promote Weight Loss during the Postpartum Period. Med. Sci. Sports Exerc. 2014, 46, 472–478. [Google Scholar] [CrossRef] [PubMed]
- Wiltheiss, G.A.; Lovelady, C.A.; West, D.G.; Brouwer, R.J.N.; Krause, K.M.; Østbye, T. Diet Quality and Weight Change among Overweight and Obese Postpartum Women Enrolled in a Behavioral Intervention Program. J. Acad. Nutr. Diet. 2013, 113, 54–62. [Google Scholar] [CrossRef] [PubMed]
- Youngwanichsetha, S.; Phumdoung, S.; Ingkathawornwong, T. The effects of tai chi qigong exercise on plasma glucose levels and health status of postpartum Thai women with type 2 diabetes. Focus Altern. Complement. Ther. 2013, 18, 182–187. [Google Scholar] [CrossRef]
- Zourladani, A.; Zafrakas, M.; Chatzigiannis, B.; Papasozomenou, P.; Vavilis, D.; Matziari, C. The effect of physical exercise on postpartum fitness, hormone and lipid levels: A randomized controlled trial in primiparous, lactating women. Arch. Gynecol. Obstet. 2014, 291, 525–530. [Google Scholar] [CrossRef]
- Zilberman-Kravits, D.; Meyerstein, N.; Abu-Rabia, Y.; Wiznitzer, A.; Harman-Boehm, I. The Impact of a Cultural Lifestyle Intervention on Metabolic Parameters After Gestational Diabetes Mellitus A Randomized Controlled Trial. Matern. Child Health J. 2018, 22, 803–811. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savovic, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomized trials. BMJ 2019, 366, 14898. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Haire-Joshu, D.L.; Schwarz, C.D.; Peskoe, S.B.; Budd, E.L.; Brownson, R.C.; Joshu, C.E. A group randomized controlled trial integrating obesity prevention and control for postpartum adolescents in a home visiting program. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 88. [Google Scholar] [CrossRef]
- Haun, J.N.; Patel, N.R.; French, D.D.; Campbell, R.R.; Bradham, D.D.; Lapcevic, W.A. Association between health literacy and medical care costs in an integrated healthcare system: A regional population based study. BMC Health Serv. Res. 2015, 15, 1–11. [Google Scholar] [CrossRef]
- Kutner, M.; Greenburg, E.; Jin, Y.; Paulsen, C. American Institutes for Research KMD. In The Health Literacy of America’s Adults: Results from the 2003 National Assessment of Adult Literacy; National Center for Education Statistics: Washington, DC, USA, 2006. [Google Scholar]
- Faruqi, N.; Spooner, C.; Joshi, C.; Lloyd, J.; Dennis, S.; Stocks, N.; Taggart, J.; Harris, M.F. Primary health care-level interventions targeting health literacy and their effect on weight loss: A systematic review. BMC Obes. 2015, 2, 6. [Google Scholar] [CrossRef] [PubMed]
- Khan, N.N.; Vincent, A.; Boyle, J.A.; Burggraf, M.; Pillay, M.; Teede, H.J.; Gibson-Helm, M. Development of a question prompt list for women with polycystic ovary syndrome. Fertil. Steril. 2018, 110, 514–522. [Google Scholar] [CrossRef] [PubMed]
- Nutbeam, D. The evolving concept of health literacy. Soc. Sci. Med. 2008, 67, 2072–2078. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.S.; McInnes, R.J.; Hughes, A.R.; Guthrie, W.; Jepson, R. The Effect of the More Active MuMs in Stirling Trial on Body Composition and Psychological Well-Being among Postnatal Women. J. Pregnancy 2016, 2016, 4183648. [Google Scholar] [CrossRef]
- Canadian Council on Learning; Health literacy in Canada: Otawa, ON, Canada, 2007.
- ABS. Health Literacy, Australia 2006; Australian Bureau of Statistics: Canberra, Australia, 2008. [Google Scholar]
- Sentell, T.; Braun, K.L. Low Health Literacy, Limited English Proficiency, and Health Status in Asians, Latinos, and Other Racial/Ethnic Groups in California. J. Health Commun. 2012, 17, 82–99. [Google Scholar] [CrossRef]
- Yamashita, T.; Kunkel, S.R. An international comparison of the association among literacy, education, and health across the United States, Canada, Switzerland, Italy, norway, and bermuda: Implications for health disparities. J. Health Commun. 2015, 20, 406–415. [Google Scholar] [CrossRef]
- Rockwell, J.M.; Riegel, B. Predictors of self-care in persons with heart failure. Heart Lung J. Crit. Care 2001, 30, 18–25. [Google Scholar] [CrossRef]
- Newman, L.; Baum, F.; Javanparast, S.; O’Rourke, K.; Carlon, L. Addressing social determinants of health inequities through settings: A rapid review. Health Promot. Int. 2015, 30 (Suppl. 2), ii126–ii143. [Google Scholar] [CrossRef]
- Simonds, S.K. Health education as social policy. Health Educ. Monogr. 1974, 2, 1–25. [Google Scholar] [CrossRef]
- Nutbeam, D. Health literacy as a public health goal: A challenge for contemporary health education and communication strategies into the 21st century. Health Promot. Int. 2000, 15, 259–267. [Google Scholar] [CrossRef]
- Krieger, N. Epidemiology and the web of causation: Has anyone seen the spider? Soc. Sci. Med. 1994, 39, 887–903. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
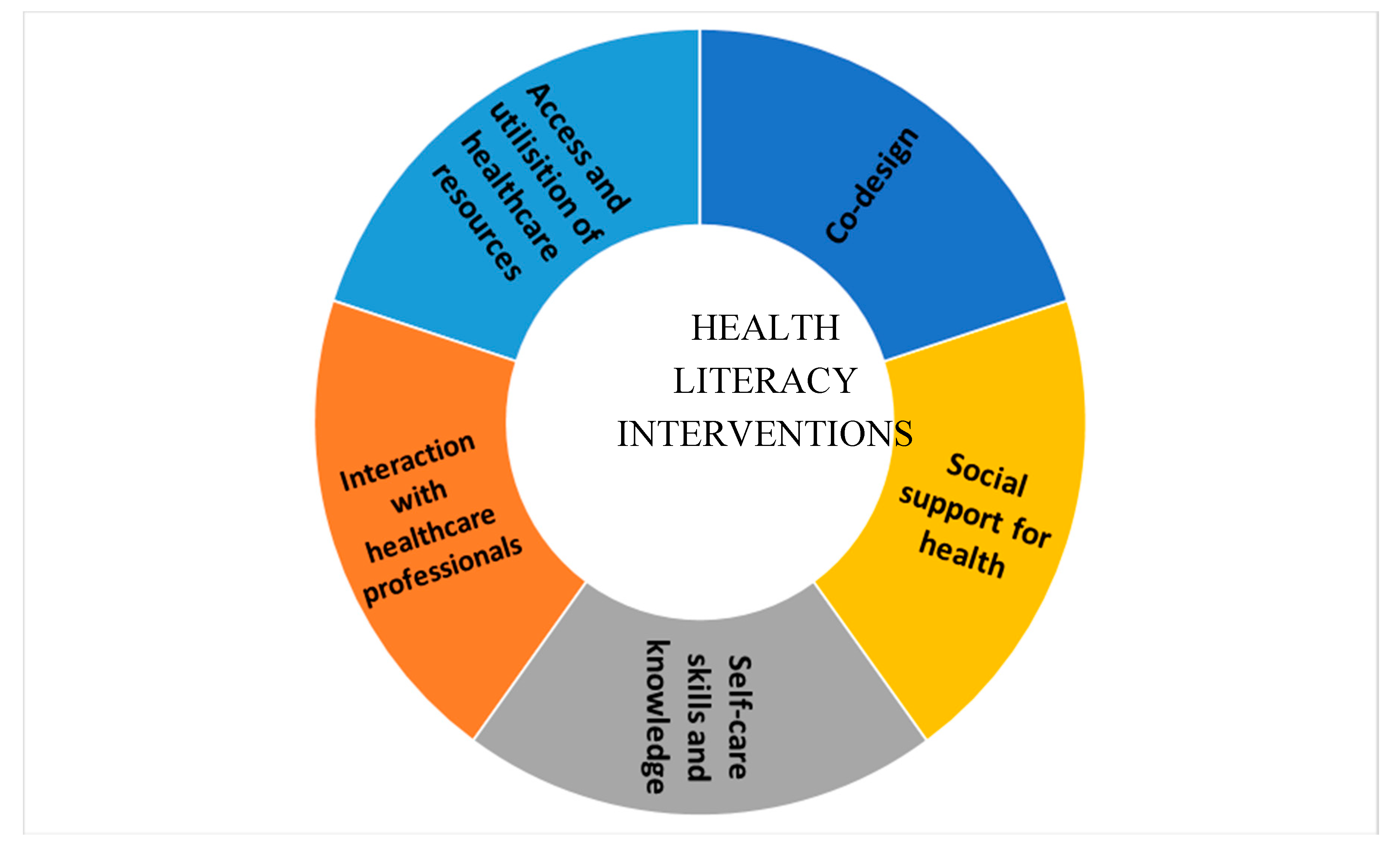
| Domain Name | Included Domains from HLQ | Example |
|---|---|---|
| Interacting with healthcare professionals (HP) * | D6—Ability to actively engage with healthcare providers (AE) | Example: a tool or intervention (practical) that augments aids communication with HP.
|
| Access and utilization of health care | D7—Navigating the healthcare system (NHS) | Example: provide advice or resource list on where to seek help to manage weight and lifestyle—can include community resources
|
| Self-care (skills and knowledge) | D3—Actively managing my health (AMH) D2—Having sufficient information to manage my health (HSI) D5—Appraisal of health information (CA) D8—Ability to find good health information (FHI) D9—Understand health information well enough to know what to do (UHI) | Example: goal setting, self-monitoring, meal or exercise plans, relapse coping, stress coping, cognitive behavioral therapy, specific time, intensity, and duration of exercise. Example: provide instruction on how to perform behavior/diet/exercise, demonstration, and onsite sessions. |
| Social support or enabler | D4—Social support for health (SS) | Example: social circle/peer natural social circle/family/partners, including leveraging social relations enabling her health/purposeful interaction.
|
| Participating in health debates and decision-making | Not in HLQ | Example: Involve in the development of implementation of the intervention/co-design |
| Study | Country | Education (Highest Level) | * Ethnicity/ Nationality | SES (Highest Income If Reported) |
|---|---|---|---|---|
| Berry et al., 2015 [25] | USA | 13% university graduates | 77% African-American; 23% Non-Hispanic White | 28% $20,000–$39,999 per year. |
| Bertz et al., 2015 [26] | Sweden | 69–80% had > 3 y beyond high school | n/a | n/a |
| Colleran et al., 2012 [27] | USA | All participants except one had at least a university education | 85% White, non-Hispanic; 11% African-American; 4% Hispanic | n/a |
| Craigie et al., 2011 [28] | UK | 28–35% degree attained | 93–96% Caucasian | 13% > £40,000 |
| Daley et al., 2015 [29] | UK | n/a | 57–68% White | 6–9% Index of Multiple Deprivation (IMD) quartile 1 (least deprived) |
| Davenport, 2011 [30] | Canada | n/a | 85–90% Caucasian | n/a |
| deRosset et al., 2013 [31] | USA | 42% completed high school | 100% Hispanic | 21% had household income from $20,000–$39,999 |
| Dritsa et al., 2009 [32] | Canada | 15–16 mean years of education | n/a | Mean 4.9–5.25 (4 = $30,000–$40,000; 5 = $40,000–$50,000) |
| Fjeldsoe et al., 2010 [33] | Australia | 16–17% had the highest education of year 10 | 2–6% identified as an Aboriginal or Torres Strait Islander | 2–6% had a weekly household income < $600 |
| Holmes et al. 2018 [34] | USA | 16–17 mean years of education | Caucasian | n/a |
| Huang et al., 2009 [35] | Taiwan | 23–28% university and above | n/a | n/a |
| Huseinovic et al., 2016, 2018 [36,37] | Sweden | 60% > 3 y beyond high school | n/a | n/a |
| Keller et al., 2014 [38] | USA | n/a | 100% Latina | 14% household income > $30,000 |
| Kernot et al., [39] | Australia | 85% tertiary education | n/a | n/a |
| Khodabandeh et al., 2017 [40] | Iran | 13–28% university degrees | 99–100% Azeri | 55–68% reported income equal to expenses |
| Krummel et al., 2010 [41] | USA | 60% had at least a high school education | 90% Caucasian | 65% stay-at-home mothers |
| Leermakers et al.,1998 [42] | USA | 12–30% graduate degree | 95–98% Caucasian | n/a |
| Lioret et al., 2012 [43] | Australia | 54% university degree or higher | 79% Australian; 21% Other | n/a |
| Lovelady et al., 2000, 2001, 2006 [44,45,46] | USA | n/a | 80–84% White; 16–19% Black | n/a |
| Lovelady et al., 1995 [47] | USA | 16–17 mean years of education | n/a | n/a |
| Lovelady et al., 2009 [48] | USA | n/a | 95% Non-Hispanic White; 5% Asian. | n/a |
| Maturi et al., 2011 [49] | Iran | 44–47% diploma; 41–48% university education | n/a | 22–24% employed |
| McCrory et al., 1999 [50] | USA | 16–17 mean years of education | 77–82% Non-Hispanic White; 9–14% Hispanic; 0–13% Black; 0–9% Asian | n/a |
| McIntyre et al., 2012 [51] | Australia | 60–62% > high school | n/a | n/a |
| Nicklas et al., 2014 [52] | USA | 20–28% some university; 56–60% university graduate | 51–64% White; 25–36% African American; 11–13% Asian; 15–25% Hispanic or Latina | 29–38% Low-income |
| Ostbye et al., 2009 [53] | USA | 24–25% some university; 54–56% university or more | 52–53% White; 45% Black; 2–3% Asian/Other | 42–43% > $60,000 |
| O’Toole et al., 2003 [54] | USA | 75% university graduates | 98% Caucasian; 3% African American | 43% full-time home-makers |
| Parsa et al., 2017 [55] | Iran | 30–32% diploma; 11% associate degree; 18% bachelor | n/a | 11% more than two million toman per month (1 USD = 3800 toman) |
| Tripette et al., 2014 [56] | Japan | n/a | 100% Japanese | n/a |
| Wiltheiss et al., 2013 [57] | USA | 20% some college or vocational, 42% college graduate, 27% graduate school | 75% White; 22% black; 4% other races; 5% Hispanic | 57% household income > $60,001 |
| Youngwanichsetha et al., 2013 [58] | Thailand | 31–38% Bachelor’s degree or higher | n/a | n/a |
| Zourladani et al., 2014 [59] | Greece | 50% university graduates | 100% Greek | n/a |
| Zilberman et al., 2018 [60] | Israel | 11 mean years of education | Jewish and Bedouin | n/a |
| Health Literacy Domains | β | 95% Confidence Interval | p-Value | Adjusted R-Squared (%) |
|---|---|---|---|---|
| Weight | ||||
| Access and utilization of health resources | 1.92 | −2.04, 5.88 | 0.33 | 0 |
| Social support or enabler | −0.47 | −3.22, 2.29 | 0.73 | 0 |
| Energy intake | ||||
| Access and utilization of health resources | 0.89 | −1.55, 3.34 | 0.44 | 0 |
| Social support or enabler | 1.02 | −0.86, 2.90 | 0.25 | 4.9 |
| Physical activity | ||||
| Access and utilization of health resources | −0.62 | −2.04, 0.81 | 0.38 | 0 |
| Social support or enabler | −0.31 | −1.19, 0.56 | 0.47 | 0 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garad, R.; McPhee, C.; Chai, T.L.; Moran, L.; O’Reilly, S.; Lim, S. The Role of Health Literacy in Postpartum Weight, Diet, and Physical Activity. J. Clin. Med. 2020, 9, 2463. https://doi.org/10.3390/jcm9082463
Garad R, McPhee C, Chai TL, Moran L, O’Reilly S, Lim S. The Role of Health Literacy in Postpartum Weight, Diet, and Physical Activity. Journal of Clinical Medicine. 2020; 9(8):2463. https://doi.org/10.3390/jcm9082463
Chicago/Turabian StyleGarad, Rhonda, Crystal McPhee, Tze Lin Chai, Lisa Moran, Sharleen O’Reilly, and Siew Lim. 2020. "The Role of Health Literacy in Postpartum Weight, Diet, and Physical Activity" Journal of Clinical Medicine 9, no. 8: 2463. https://doi.org/10.3390/jcm9082463
APA StyleGarad, R., McPhee, C., Chai, T. L., Moran, L., O’Reilly, S., & Lim, S. (2020). The Role of Health Literacy in Postpartum Weight, Diet, and Physical Activity. Journal of Clinical Medicine, 9(8), 2463. https://doi.org/10.3390/jcm9082463