Early Pregnancy Vitamin D Binding Protein Is Independently Associated with the Development of Gestational Diabetes: A Retrospective Cohort Study

 , , ,
, , ,  , and
, and 
Abstract
1. Introduction
2. Experimental Section
2.1. Study Design and Population
2.2. Ethics
2.3. Sample and Data Collection
2.4. Biochemical Analyses
2.4.1. Archived Data (Serum Glucose, Total 25(OH)D)
2.4.2. VDBP Analysis
2.4.3. Albumin Analysis
2.5. Calculation of Free and Bioavailable 25(OH)D
- = serum free 25(OH)D concentrations in mol/L;
- = serum total 25(OH)D concentration in mol/L;
- = serum bioavailable 25(OH)D concentration in mol/L;
- = serum albumin concentration in mol/L (albumin was measured in g/L and converted to mol/L using: );
- = serum vitamin D binding protein concentration in mol/L (VDBP was measured in ug/mL and converted to mol/L using: ).
2.6. Statistical Analyses
3. Results
3.1. Sample Characteristics
3.2. Univariable Analyses of Vitamin D Metabolites and Demographic and Anthropometric Variables
3.3. Univariable and Multivariable Analyses of Vitamin D Metabolites and Biochemical Variables
3.4. Univariable Analyses of Vitamin D Metabolites and Pregnancy Outcomes
3.5. Multivariable Analyses of Vitamin D Metabolites and Pregnancy Outcomes
4. Discussion
4.1. Summary of Results
4.2. Comparison with Previous Literature and Potential Mechanisms
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mousa, A.; Naderpoor, N.; Teede, H.; Scragg, R.; De Courten, B. Vitamin D supplementation for improvement of chronic low-grade inflammation in patients with type 2 diabetes: A systematic review and meta-analysis of randomized controlled trials. Nutr. Rev. 2018, 76, 380–394. [Google Scholar] [CrossRef] [PubMed]
- Mousa, A.; Abell, S.; Scragg, R.K.R.; De Courten, B. Vitamin D in Reproductive Health and Pregnancy. Semin. Reprod. Med. 2016, 34, e1–e13. [Google Scholar] [CrossRef]
- Marquina, C.; Mousa, A.; Scragg, R.; De Courten, B. Vitamin D and cardiometabolic disorders: A review of current evidence, genetic determinants and pathomechanisms. Obes. Rev. 2018, 20, 262–277. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Chen, T. Vitamin D deficiency: A worldwide problem with health consequences. Am. J. Clin. Nutr. 2008, 87, 1080S–1086S. [Google Scholar] [CrossRef]
- Ojo, O.; Weldon, S.M.; Thompson, T.; Vargo, E.J. The Effect of Vitamin D Supplementation on Glycaemic Control in Women with Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Int. J. Environ. Res. Public Health 2019, 16, 1716. [Google Scholar] [CrossRef] [PubMed]
- Karras, S.N.; Koufakis, T.; Fakhoury, H.A.; Kotsa, K. Deconvoluting the Biological Roles of Vitamin D-Binding Protein During Pregnancy: A Both Clinical and Theoretical Challenge. Front. Endocrinol. 2018, 9, 259. [Google Scholar] [CrossRef] [PubMed]
- Bikle, D.; Schwartz, J. Vitamin D Binding Protein, Total and Free Vitamin D Levels in Different Physiological and Pathophysiological Conditions. Front. Endocrinol. 2019, 10, 317. [Google Scholar] [CrossRef]
- Bouillon, R.; Schuit, F.; Antonio, L.; Rastinejad, F. Vitamin D Binding Protein: A Historic Overview. Front. Endocrinol. 2020, 10, 910. [Google Scholar] [CrossRef]
- Norman, A.W. 1α,25(OH)2 Vitamin D3Vitamin D Nuclear Receptor (VDR) and Plasma Vitamin D-Binding Protein (DBP) Structures and Ligand Shape Preferences for Genomic and Rapid Biological Responses. In Principles of Bone Biology; Elsevier BV: Amsterdam, The Netherlands, 2008; pp. 749–778. [Google Scholar]
- Fernando, M.; Ellery, S.J.; Marquina, C.; Lim, S.; Naderpoor, N.; Mousa, A. Vitamin D-Binding Protein in Pregnancy and Reproductive Health. Nutrients 2020, 12, 1489. [Google Scholar] [CrossRef]
- Laopaiboon, M.; Lumbiganon, P.; Intarut, N.; Mori, R.; Ganchimeg, T.; Vogel, J.P.; Souza, J.P.; Gülmezoglu, A. Advanced maternal age and pregnancy outcomes: A multicountry assessment. BJOG Int. J. Obstet. Gynaecol. 2014, 121, 49–56. [Google Scholar] [CrossRef]
- Mund, M.; Louwen, F.; Groneberg, D.A.; Gerber, A. Smoking and Pregnancy—A Review on the First Major Environmental Risk Factor of the Unborn. Int. J. Environ. Res. Public Health 2013, 10, 6485–6499. [Google Scholar] [CrossRef] [PubMed]
- Verma, A.; Shrimali, L. Maternal Body Mass Index and Pregnancy Outcome. J. Clin. Diagn. Res. 2012, 6, 1531–1533. [Google Scholar] [CrossRef]
- Newton, D.A.; Baatz, J.E.; Kindy, M.S.; Gattoni-Celli, S.; Shary, J.R.; Hollis, B.W.; Wagner, C.L. Vitamin D binding protein polymorphisms significantly impact vitamin D status in children. Pediatr. Res. 2019, 86, 662–669. [Google Scholar] [CrossRef] [PubMed]
- Aloia, J.F.; Mikhail, M.; Dhaliwal, R.; Shieh, A.; Usera, G.; Stolberg, A.; Ragolia, L.; Islam, S. Free 25(OH)D and the Vitamin D Paradox in African Americans. J. Clin. Endocrinol. Metab. 2015, 100, 3356–3363. [Google Scholar] [CrossRef] [PubMed]
- Daiger, S.P.; Miller, M.; Chakraborty, R. Heritability of quantitative variation at the group-specific component (Gc) locus. Am. J. Hum. Genet. 1984, 36, 663–676. [Google Scholar]
- Nielson, C.M.; Jones, K.S.; Chun, R.F.; Jacobs, J.M.; Wang, Y.; Hewison, M.; Adams, J.S.; Swanson, C.M.; Lee, C.G.; Vanderschueren, D.; et al. Free 25-Hydroxyvitamin D: Impact of Vitamin D Binding Protein Assays on Racial-Genotypic Associations. J. Clin. Endocrinol. Metab. 2016, 101, 2226–2234. [Google Scholar] [CrossRef]
- Harrison, C.L.; Lombard, C.; Strauss, B.J.; Teede, H.J. Optimizing healthy gestational weight gain in women at high risk of gestational diabetes: A randomized controlled trial. Obesity 2013, 21, 904–909. [Google Scholar] [CrossRef]
- Teede, H.J.; Harrison, C.L.; Teh, W.T.; Paul, E.; Allan, C.A. Gestational diabetes: Development of an early risk prediction tool to facilitate opportunities for prevention. Aust. N. Z. J. Obstet. Gynaecol. 2011, 51, 499–504. [Google Scholar] [CrossRef]
- De Guingand, D.L.; Ellery, S.J.; Davies-Tuck, M.L.; Dickinson, H. Creatine and pregnancy outcomes, a prospective cohort study in low-risk pregnant women: Study protocol. BMJ Open 2019, 9, e026756. [Google Scholar] [CrossRef]
- Hoffman, L.; Nolan, C.; Wilson, J.D.; Oats, J.J.N.; Simmons, D. Gestational diabetes mellitus--management guidelines. The Australasian Diabetes in Pregnancy Society. Med J. Aust. 1998, 169, 93–97. [Google Scholar] [CrossRef]
- Walker, S.; Nassar, N.; Fung, A. Screening in Early Pregnancy for Adverse Perinatal Outcomes. The Royal Australian and New Zealand College of Obstetricians and Gynaecologists. Statement C-Obs 61, July 2015. Available online: https://ranzcog.edu.au/RANZCOG_SITE/media/RANZCOG-MEDIA/Women%27s%20Health/Statement%20and%20guidelines/Clinical-Obstetrics/Screening-in-Early-Pregnancy-for-Adverse-Perinatal-Outcomes-(C-Obs-61)-New-July-2015_1.pdf?ext=.pdf (accessed on 18 June 2020).
- Bikle, D.; Bouillon, R.; Thadhani, R.; Schoenmakers, I. Vitamin D metabolites in captivity? Should we measure free or total 25(OH)D to assess vitamin D status? J. Steroid Biochem. Mol. Biol. 2017, 173, 105–116. [Google Scholar] [CrossRef]
- Holick, M.F.; Binkley, N.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, Treatment, and Prevention of Vitamin D Deficiency: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed]
- Burris, H.H.; Rifas-Shiman, S.L.; Kleinman, K.; A Litonjua, A.; Huh, S.Y.; Rich-Edwards, J.W.; Camargo, C.A.; Gillman, M.W.; Rifas-Shiman, M.S.L. Vitamin D deficiency in pregnancy and gestational diabetes mellitus. Am. J. Obstet. Gynecol. 2012, 207, e1–e8. [Google Scholar] [CrossRef]
- Zhang, Y.-B.; Gong, Y.; Xue, H.; Xiong, J.; Cheng, G. Vitamin D and gestational diabetes mellitus: A systematic review based on data free of Hawthorne effect. BJOG Int. J. Obstet. Gynaecol. 2018, 125, 784–793. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.-X.; Pan, G.-T.; Guo, J.-F.; Li, B.-Y.; Qin, L.; Zhang, Z. Vitamin D Deficiency Increases the Risk of Gestational Diabetes Mellitus: A Meta-Analysis of Observational Studies. Nutrients 2015, 7, 8366–8375. [Google Scholar] [CrossRef]
- Wei, S.Q.; Qi, H.-P.; Luo, Z.-C.; Fraser, W.D. Maternal vitamin D status and adverse pregnancy outcomes: A systematic review and meta-analysis. J. Matern. Neonatal Med. 2013, 26, 889–899. [Google Scholar] [CrossRef]
- Palomer, X.; González-Clemente, J.M.; Blanco-Vaca, F.; Mauricio, D. Role of vitamin D in the pathogenesis of type 2 diabetes mellitus. Diabetes Obes. Metab. 2008, 10, 185–197. [Google Scholar] [CrossRef]
- Farrant, H.J.; Krishnaveni, G.V.; Hill, J.C.; Boucher, B.J.; Fisher, D.J.; Noonan, K.; Osmond, C.; Veena, S.R.; Fall, C.H. Vitamin D insufficiency is common in Indian mothers but is not associated with gestational diabetes or variation in newborn size. Eur. J. Clin. Nutr. 2008, 63, 646–652. [Google Scholar] [CrossRef]
- Makgoba, M.; Nelson, S.M.; Savvidou, M.D.; Messow, C.-M.; Nicolaides, K.; Sattar, N. First-Trimester Circulating 25-Hydroxyvitamin D Levels and Development of Gestational Diabetes Mellitus. Diabetes Care 2011, 34, 1091–1093. [Google Scholar] [CrossRef]
- Park, S.; Yoon, H.-K.; Ryu, H.-M.; Han, Y.J.; Lee, S.W.; Park, B.K.; Park, S.-Y.; Yim, C.H.; Kim, S.-H. Maternal Vitamin D Deficiency in Early Pregnancy Is Not Associated with Gestational Diabetes Mellitus Development or Pregnancy Outcomes in Korean Pregnant Women in a Prospective Study. J. Nutr. Sci. Vitaminol. 2014, 60, 269–275. [Google Scholar] [CrossRef]
- Xia, J.; Song, Y.; Rawal, S.; Wu, J.; Hinkle, S.N.; Tsai, M.Y.; Zhang, C. Vitamin D status during pregnancy and the risk of gestational diabetes mellitus: A longitudinal study in a multiracial cohort. Diabetes Obes. Metab. 2019, 21, 1895–1905. [Google Scholar] [CrossRef] [PubMed]
- Sauer, C.G.; Loop, M.S.; Venkateswaran, S.; Tangpricha, V.; Ziegler, T.R.; Dhawan, A.; McCall, C.; Bonkowski, E.; Mack, D.R.; Boyle, B.; et al. Free and Bioavailable 25-Hydroxyvitamin D Concentrations are Associated With Disease Activity in Pediatric Patients With Newly Diagnosed Treatment Naïve Ulcerative Colitis. Inflamm. Bowel Dis. 2018, 24, 641–650. [Google Scholar] [CrossRef]
- Ying, H.-Q.; Sun, H.-L.; He, B.-S.; Pan, Y.-Q.; Wang, F.; Deng, Q.-W.; Chen, J.; Liu, X.; Wang, S. Circulating vitamin D binding protein, total, free and bioavailable 25-hydroxyvitamin D and risk of colorectal cancer. Sci. Rep. 2015, 5, 7956. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-J.; Ji, M.; Song, J.; Moon, H.-W.; Hur, M.; Yun, Y.-M. Clinical Utility of Measurement of Vitamin D-Binding Protein and Calculation of Bioavailable Vitamin D in Assessment of Vitamin D Status. Ann. Lab. Med. 2017, 37, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, J.B.; Lai, J.; Lizaola, B.; Kane, L.; Weyland, P.; Terrault, N.A.; Stotland, N.; Bikle, D. Variability in free 25(OH) vitamin D levels in clinical populations. J. Steroid Biochem. Mol. Biol. 2013, 144, 156–158. [Google Scholar] [CrossRef] [PubMed]
- Bouillon, R.; Van Assche, F.A.; Van Baelen, H.; Heyns, W.; De Moor, P. Influence of the Vitamin D-binding Protein on the Serum Concentration of 1,25-Dihydroxyvitamin D3. J. Clin. Investig. 1981, 67, 589–596. [Google Scholar] [CrossRef]
- Bikle, D.D.; Gee, E.; Halloran, B.; Haddad, J.G. Free 1,25-dihydroxyvitamin D levels in serum from normal subjects, pregnant subjects, and subjects with liver disease. J. Clin. Investig. 1984, 74, 1966–1971. [Google Scholar] [CrossRef]
- Gustafsson, M.K.; Romundstad, P.R.; Stafne, S.N.; Helvik, A.-S.; Stunes, A.K.; Mørkved, S.; Salvesen, K. Åsmund; Thorsby, P.M.; Syversen, U. Alterations in the vitamin D endocrine system during pregnancy: A longitudinal study of 855 healthy Norwegian women. PLoS ONE 2018, 13, e0195041. [Google Scholar] [CrossRef]
- Delanghe, J.R.; Speeckaert, R.; Speeckaert, M.M. Behind the scenes of vitamin D binding protein: More than vitamin D binding. Best Pr. Res. Clin. Endocrinol. Metab. 2015, 29, 773–786. [Google Scholar] [CrossRef]
- Kew, R.R. The Vitamin D Binding Protein and Inflammatory Injury: A Mediator or Sentinel of Tissue Damage? Front. Endocrinol. 2019, 10, 470. [Google Scholar] [CrossRef]
- Radaelli, T.; Varastehpour, A.; Catalano, P.; Mouzon, S.H.-D. Gestational diabetes induces placental genes for chronic stress and inflammatory pathways. Diabetes 2003, 52, 2951–2958. [Google Scholar] [CrossRef] [PubMed]
- Pantham, P.; Aye, I.L.; Powell, T.L. Inflammation in maternal obesity and gestational diabetes mellitus. Placenta 2015, 36, 709–715. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.Y.; Lucey, A.; Horgan, R.; Kenny, L.C.; Kiely, M.E. Impact of pregnancy on vitamin D status: A longitudinal study. Br. J. Nutr. 2014, 112, 1081–1087. [Google Scholar] [CrossRef] [PubMed]
- Sonagra, A.D.; Biradar, S.M.; K., D.; D.S., J.M. Normal Pregnancy—A State of Insulin Resistance. J. Clin. Diagn. Res. 2014, 8, CC01–CC03. [Google Scholar] [CrossRef] [PubMed]
- Nyomba, B.L.; Bouillon, R.; De Moor, P. Evidence for an interaction of insulin and sex steroids in the regulation of vitamin D metabolism in the rat. J. Endocrinol. 1987, 115, 295–301. [Google Scholar] [CrossRef]
- Kuliczkowska-Plaksej, J.; Pasquali, R.; Milewicz, A.; Lwow, F.; Jedrzejuk, D.; Bolanowski, M. Serum Vitamin D Binding Protein Level Associated with Metabolic Cardiovascular Risk Factors in Women with the Polycystic Ovary Syndrome. Horm. Metab. Res. 2018, 51, 54–61. [Google Scholar] [CrossRef]
- Shi, A.; Wen, J.; Liu, G.; Liu, H.; Fu, Z.; Zhou, J.; Zhu, Y.; Liu, Y.; Guo, X.; Xu, J. Genetic variants in vitamin D signaling pathways and risk of gestational diabetes mellitus. Oncotarget 2016, 7, 67788–67795. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wang, O.; Li, W.; Ma, L.; Ping, F.; Chen, L.; Nie, M. Variants in Vitamin D Binding Protein Gene Are Associated With Gestational Diabetes Mellitus. Medicine 2015, 94, e1693. [Google Scholar] [CrossRef] [PubMed]
- Kolialexi, A.; Tsangaris, G.T.; Sifakis, S.; Gourgiotis, D.; Katsafadou, A.; Lykoudi, A.; Marmarinos, A.; Mavreli, D.; Pergialiotis, V.; Fexi, D.; et al. Plasma biomarkers for the identification of women at risk for early-onset preeclampsia. Expert Rev. Proteom. 2017, 14, 269–276. [Google Scholar] [CrossRef]
- Tannetta, D.; Redman, C.W.; Sargent, I.L. Investigation of the actin scavenging system in pre-eclampsia. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 172, 32–35. [Google Scholar] [CrossRef]
- Bailey, L.J.; Alahari, S.; Tagliaferro, A.; Post, M.; Caniggia, I. Augmented trophoblast cell death in preeclampsia can proceed via ceramide-mediated necroptosis. Cell Death Dis. 2017, 8, e2590. [Google Scholar] [CrossRef]
- Harper, K.D.; McLeod, J.F.; A Kowalski, M.; Haddad, J.G. Vitamin D binding protein sequesters monomeric actin in the circulation of the rat. J. Clin. Investig. 1987, 79, 1365–1370. [Google Scholar] [CrossRef] [PubMed]
- Ma, R.; Gu, Y.; Zhao, S.; Sun, J.; Groome, L.J.; Wang, Y. Expressions of vitamin D metabolic components VDBP, CYP2R1, CYP27B1, CYP24A1, and VDR in placentas from normal and preeclamptic pregnancies. Am. J. Physiol. Metab. 2012, 303, E928–E935. [Google Scholar] [CrossRef] [PubMed]
- Kook, S.Y.; Park, K.H.; Jang, J.A.; Kim, Y.M.; Park, H.; Jeon, S.J. Vitamin D-binding protein in cervicovaginal fluid as a non-invasive predictor of intra-amniotic infection and impending preterm delivery in women with preterm labor or preterm premature rupture of membranes. PLoS ONE 2018, 13, e0198842. [Google Scholar] [CrossRef] [PubMed]
- Liong, S.; Di Quinzio, M.; Fleming, G.; Permezel, M.; Rice, G.; Georgiou, H.M. New biomarkers for the prediction of spontaneous preterm labour in symptomatic pregnant women: A comparison with fetal fibronectin. BJOG Int. J. Obstet. Gynaecol. 2014, 122, 370–379. [Google Scholar] [CrossRef]
- Wang, Y.; Li, H.; Zheng, M.; Wu, Y.; Zeng, T.; Fu, J.; Zeng, D. Maternal vitamin D deficiency increases the risk of adverse neonatal outcomes in the Chinese population: A prospective cohort study. PLoS ONE 2018, 13, e0195700. [Google Scholar] [CrossRef]
- Khalessi, N.; Kalani, M.; Araghi, M.; Farahani, Z. The Relationship between Maternal Vitamin D Deficiency and Low Birth Weight Neonates. J. Fam. Reprod. Health 2015, 9, 113–117. [Google Scholar]
- Chen, Y.; Zhu, B.; Wu, X.; Li, S.; Tao, F. Association between maternal vitamin D deficiency and small for gestational age: Evidence from a meta-analysis of prospective cohort studies. BMJ Open 2017, 7, e016404. [Google Scholar] [CrossRef]
- Francis, E.; Hinkle, S.N.; Song, Y.; Rawal, S.; Donnelly, S.R.; Zhu, Y.; Chen, L.; Zhang, C. Longitudinal Maternal Vitamin D Status during Pregnancy Is Associated with Neonatal Anthropometric Measures. Nutrients 2018, 10, 1631. [Google Scholar] [CrossRef]
- Merewood, A.; Mehta, S.D.; Chen, T.; Bauchner, H.; Holick, M.F. Association Between Vitamin D Deficiency and Primary Cesarean Section. Obstet. Gynecol. Surv. 2009, 64, 501–502. [Google Scholar] [CrossRef]
- Liu, N.; Hewison, M. Vitamin D, the placenta and pregnancy. Arch. Biochem. Biophys. 2012, 523, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Qin, L.-L.; Lu, F.-G.; Yang, S.-H.; Xu, H.-L.; Luo, B.-A. Does Maternal Vitamin D Deficiency Increase the Risk of Preterm Birth: A Meta-Analysis of Observational Studies. Nutrients 2016, 8, 301. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, J.B.; Lai, J.; Lizaola, B.; Kane, L.; Marková, S.; Weyland, P.; Terrault, N.A.; Stotland, N.; Bikle, D. A comparison of measured and calculated free 25(OH) vitamin D levels in clinical populations. J. Clin. Endocrinol. Metab. 2014, 99, 1631–1637. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. 2071.0-Census of Population and Housing: Reflecting Australia-Stories from the Census, 2016. Cultural Diversity in Australia, 2016. 2017. Available online: https://www.abs.gov.au/ausstats/abs@.nsf/Lookup/by%20Subject/2071.0~2016~Main%20Features~Cultural%20Diversity%20Data%20Summary~30 (accessed on 18 June 2020).
- Christensen, M.H.; Scragg, R.K.R. Consistent ethnic specific differences in diabetes risk and vitamin D status in the National Health and Nutrition Examination Surveys. J. Steroid Biochem. Mol. Biol. 2016, 164, 4–10. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria | ||
|---|---|---|---|
| HLP Cohort | CPO Cohort | HLP Cohort | CPO Cohort |
| Age ≥18 years | Age 18 ≤ 40 years | Age <18 years | Age <18 or >40 years |
| Singleton pregnancy | Multiple pregnancy | ||
| High risk of GDM (scoring ≥3 on risk prediction tool [19]) | Low-risk pregnancy (based on medical/obstetric history) | Known pre-existing diabetes diagnosis (any diabetes) | High-risk pregnancy (requiring care in high-risk clinic) |
| ≤15 weeks gestation at recruitment | 10–20 weeks gestation (±1 week) at recruitment | Other chronic medical conditions precluding participation | Models of care outside tertiary public hospital care (e.g., private, shared, or GP/midwife care) |
| English speaking | Non-English Speaking | ||
| Overweight/obese: BMI ≥25 kg/m2 (or ≥23 kg/m2 in high-risk ethnicities) or ≥30 kg/m2 | Attending Monash Health for labour | Morbidly obese (BMI ≥45 kg/m2) | Use of creatine supplements in pregnancy |
| Timepoint (Gestation) | Data Collected in Both Cohorts | Methods |
|---|---|---|
| <20 weeks | Demographic characteristics: age, ethnicity, parity, smoking status, medical history | Demographic questionnaires |
| BMI, weight, height | Weight (kg)/height (m)2 measured directly or calculated from SMR | |
| Fasting plasma glucose; serum/plasma total 25(OH)D, albumin, VDBP | Fasting venous blood samples and commercial assays for plasma glucose and total 25(OH)D; albumin and VDBP measured in bio-banked samples by Monash Pathology and Hudson laboratory (detailed below) | |
| 26–28 weeks | GDM diagnosis, fasting glucose, 1 h glucose post-OGTT, and 2 h glucose post-OGTT. | Data retrieved from routine OGTTs recorded on BOS or SMR. GDM diagnosed based on 2014 ADIPS criteria: FBG 5.1 or over and/or 2 h glucose 8.5 or over (mmol/L) |
| During pregnancy/at birth | Maternal outcomes and complications (including pre-eclampsia, pregnancy-induced hypertension, preterm birth) | Data retrieved from BOS and SMR |
| Variable | Mean ± SD or n (%) |
|---|---|
| Maternal age (years) | 31.4 ± 4.2 |
| Parity | |
| Primiparous | 133 (46.0) |
| 2 | 106 (36.7) |
| 3 | 39 (13.5) |
| 4 | 11 (3.8) |
| Ethnicity | |
| Caucasian | 174 (57.4) |
| South East and North East Asian | 37 (12.2) |
| Southern and Central Asian | 69 (22.8) |
| Other a | 23 (7.6) |
| Past history of GDM | 13 (4.3) |
| BMI (kg/m²) | 26.8 ± 5.9 |
| Gestational weight gain (kg, at 28 weeks) | 7.4 ± 3.6 |
| Vitamin D metabolites | |
| Total 25(OH)D, nmol/L (ng/mL) | 54.8 ± 20.2 (22.0 ± 8.1) |
| Free 25(OH)D (pg/mL) | 5.6 ± 4.7 |
| Bioavailable 25(OH)D (nmol/L) | 4.4 ± 3.1 |
| VDBP (µg/mL) | 364.7 ± 126.1 |
| Albumin (g/L) | 36.9 ± 4.1 |
| Glycaemic measures | |
| FBG at baseline (< 20 weeks) (mmol/L) | 4.6 ± 0.6 |
| FBG OGTT (26–28 weeks) (mmol/L) | 4.5 ± 0.5 |
| 1 h OGTT (26–28 weeks) (mmol/L) | 7.6 ± 1.9 |
| 2 h OGTT (26–28 weeks) (mmol/L) | 6.3 ± 1.5 |
| Pregnancy outcome | |
| Gestational diabetes mellitus | 55 (19.4) |
| Pre-eclampsia | 10 (3.4) |
| Placental abnormality | 102 (48.1) |
| Gestation at delivery (weeks) | 39.1 ± 2.0 |
| Preterm birth | 16 (5.4) |
| Premature rupture of membranes | 42 (20.4) |
| Caesarean section | 75 (25.5) |
| Variable | VDBP | Total 25(OH)D * | Free 25(OH)D * | Bioavailable 25(OH)D * | ||||
|---|---|---|---|---|---|---|---|---|
| r | p | r | p | r | p | r | p | |
| Maternal characteristics | ||||||||
| Age (years) | −0.24 | <0.01 | 0.11 | 0.07 | 0.22 | <0.01 | 0.24 | <0.01 |
| BMI (kg/m²) | −0.12 | 0.047 | −0.26 | <0.001 | −0.11 | 0.08 | −0.09 | 0.1 |
| Glycaemic measures | ||||||||
| FBG (<20 weeks; mmol/L) | −0.02 | 0.7 | −0.06 | 0.3 | −0.003 | 0.9 | −0.02 | 0.7 |
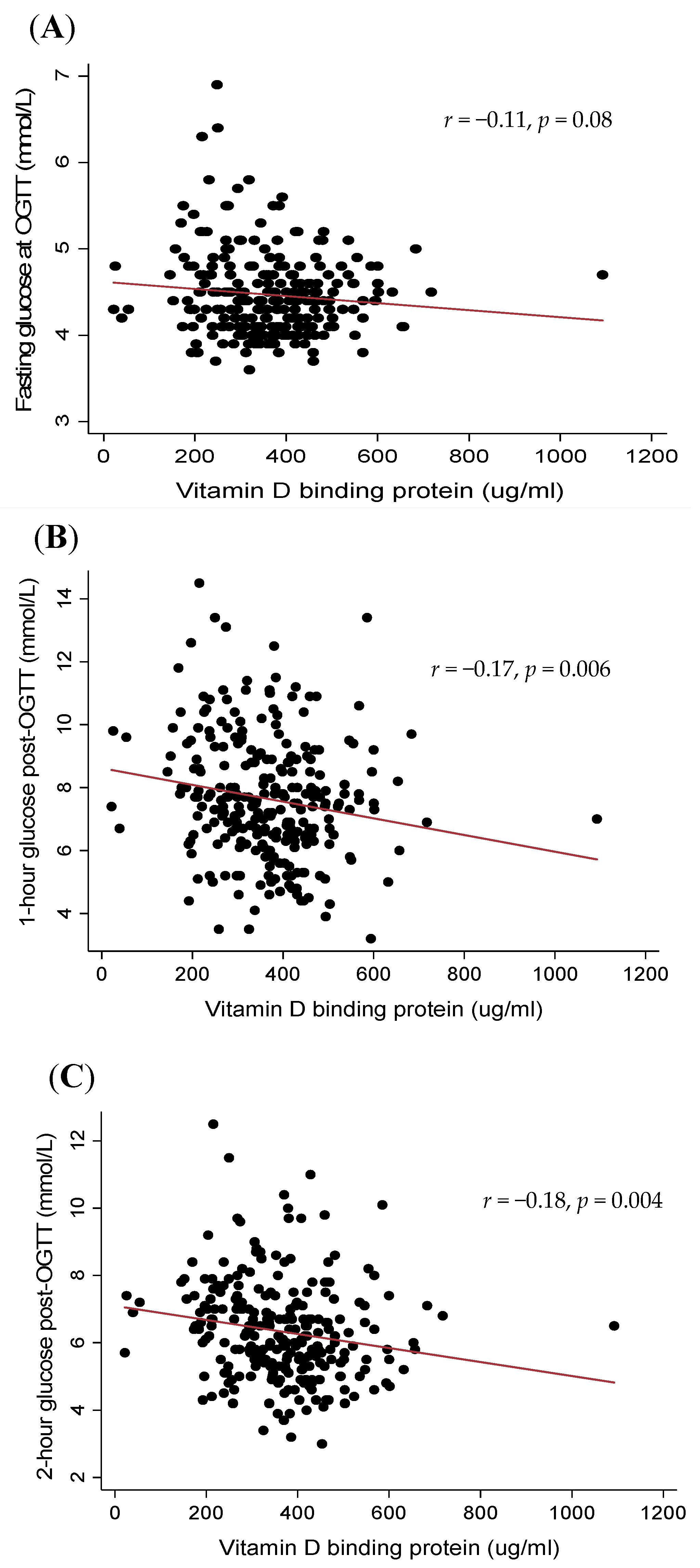
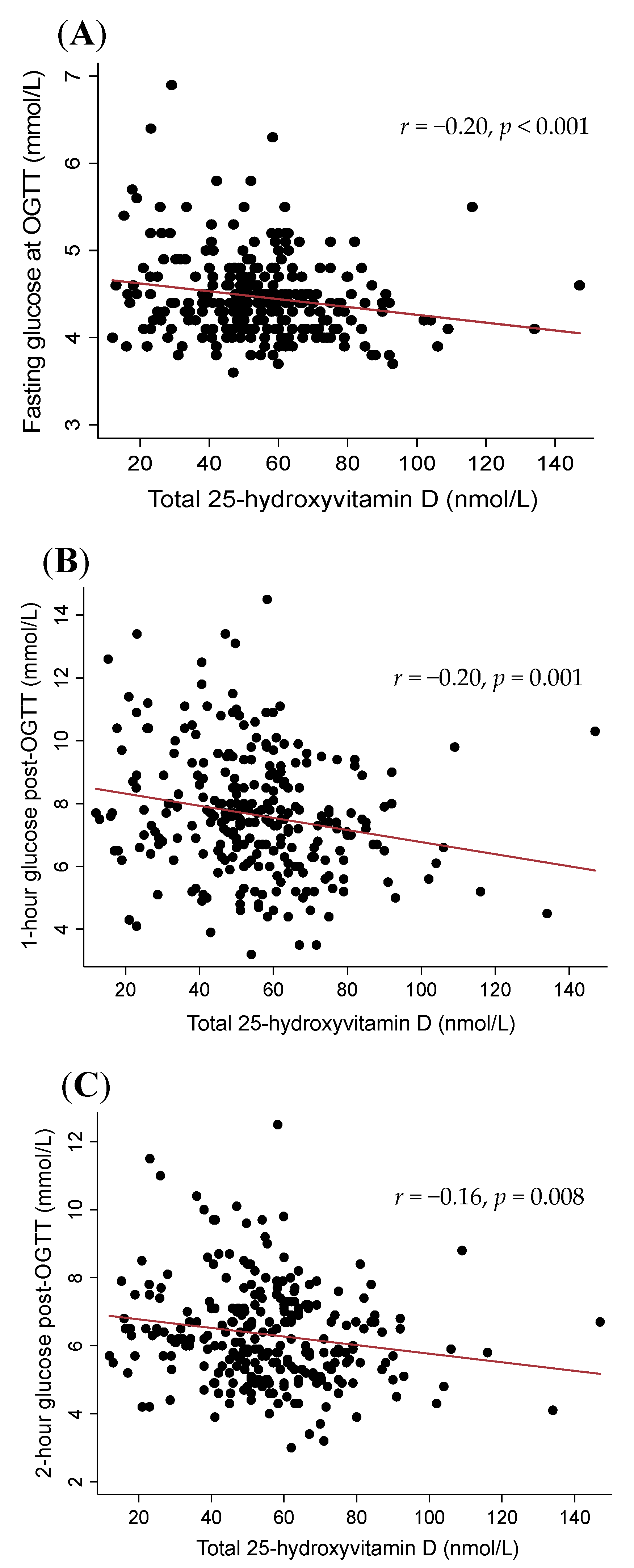
| FBG OGTT (26–28 wks; mmol/L) | −0.11 | 0.08 | −0.20 | <0.001 | −0.07 | 0.3 | −0.05 | 0.4 |
| 1 h OGTT (26–28 weeks; mmol/L) | −0.17 | 0.007 | −0.20 | 0.001 | −0.02 | 0.8 | −0.02 | 0.8 |
| 2 h OGTT (26–28 weeks; mmol/L) | −0.18 | 0.003 | −0.16 | 0.008 | 0.008 | 0.9 | 0.001 | 0.9 |
| Variable | VDBP | Total 25(OH)D | Free 25(OH)D | Bioavailable 25(OH)D | ||||
|---|---|---|---|---|---|---|---|---|
| β or OR | p | β or OR (95%CI) | p * | β or OR | p * | β or OR (95%CI) | p * | |
| (95%CI) | (95%CI) | |||||||
| GDM | 0.98 | 0.015 | 0.98 | 0.04 | 0.99 | 0.9 | 1.01 | 0.9 |
| (0.97, 0.99) | (0.97, 0.99) | (0.93, 1.06) | (0.92, 1.10) | |||||
| PIH | 1 | 0.5 | 1.03 | 0.06 | 1.02 | 0.3 | 1.04 | 0.3 |
| (0.99, 1.00) | (1.00, 1.06) | (0.91, 1.13) | (0.90, 1.22) | |||||
| Pre-eclampsia | 0.99 | 0.1 | 1 | 0.8 | 1.06 | 0.09 | 1.12 | 0.08 |
| (0.99, 1.00) | (0.97, 1.03) | (0.98, 1.14) | (0.99, 1.24) | |||||
| Placental abnormalities | 1 | 0.3 | 0.99 | 0.2 | 0.94 | 0.2 | 0.94 | 0.5 |
| (0.99, 1.00) | (0.98, 1.01) | (0.87, 1.02) | (0.85, 1.03) | |||||
| Gestation † | 0.001 † | 0.5 | 0.02 † | 0.002 | 0.02 † | 0.07 | 0.05 † | 0.07 |
| (−0.001, −0.003) | (0.004, 0.03) | (−0.03, 0.07) | (−0.02, 0.13) | |||||
| Preterm birth | 0.99 | 0.3 | 0.98 | 0.1 | 0.88 | 0.4 | 0.89 | 0.6 |
| (0.99, 1.00) | (0.95, 1.01) | (0.70, 1.10) | (0.69, 1.15) | |||||
| PROM | 1 | 0.8 | 0.99 | 0.5 | 0.94 | 0.4 | 0.94 | 0.6 |
| (0.99, 1.00) | (0.98, 1.01) | (0.84, 1.06) | (0.81, 1.08) | |||||
| Dependent Variable | Model | VDBP | Total 25(OH)D | Free 25(OH)D | Bioavailable 25(OH)D | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | SE | R2 | p | β | SE | R2 | p | β | SE | R2 | p | β | SE | R2 | p | ||
| GDM | + age | −0.003 | 0.001 | 0.05 | 0.04 | −0.02 | 0.01 | 0.05 | 0.01 | −0.02 | 0.04 | 0.03 | 0.4 | −0.03 | 0.05 | 0.03 | 0.5 |
| + BMI | −0.003 | 0.001 | 0.06 | 0.05 | −0.01 | 0.01 | 0.05 | 0.04 | −0.01 | 0.04 | 0.04 | 0.7 | −0.01 | 0.05 | 0.04 | 0.7 | |
| + ethnicity | −0.003 | 0.001 | 0.07 | 0.03 | −0.01 | −0.03 | 0.01 | 0.1 | 0.002 | 0.04 | 0.05 | 0.9 | 0.01 | 0.05 | 0.05 | 0.9 | |
| Pregnancy-induced hypertension | + age | 0.001 | 0.002 | 0.004 | 0.5 | 0.03 | 0.01 | 0.05 | 0.06 | 0.02 | 0.06 | 0.001 | 0.3 | 0.05 | 0.08 | 0.003 | 0.3 |
| + BMI | 0.001 | 0.003 | 0.002 | 0.7 | 0.02 | 0.02 | 0.01 | 0.2 | 0.001 | 0.07 | 0.0003 | 0.5 | 0.02 | 0.10 | 0.001 | 0.5 | |
| + ethnicity | 0.001 | 0.003 | 0.05 | 0.7 | 0.01 | 0.02 | 0.05 | 0.5 | −0.02 | 0.09 | 0.05 | 0.8 | −0.01 | 0.11 | 0.05 | 0.9 | |
| Pre-eclampsia | + age | −0.003 | 0.003 | 0.06 | 0.3 | 0.001 | 0.02 | 0.05 | 0.6 | 0.05 | 0.07 | 0.10 | 0.2 | 0.10 | 0.06 | 0.07 | 0.2 |
| + BMI | −0.003 | 0.003 | 0.09 | 0.4 | 0.007 | 0.02 | 0.08 | 0.5 | 0.07 | 0.04 | 0.11 | 0.2 | 0.10 | 0.06 | 0.11 | 0.1 | |
| + ethnicity | −0.003 | 0.003 | 0.09 | 0.4 | 0.007 | 0.02 | 0.08 | 0.9 | 0.07 | 0.04 | 0.11 | 0.1 | 0.10 | 0.06 | 0.11 | 0.1 | |
| Length of gestation | + age | 0.0004 | 0.001 | 0.003 | 0.7 | 0.02 | 0.01 | 0.03 | 0.001 | 0.03 | 0.03 | 0.007 | 0.039 | 0.07 | 0.04 | 0.01 | 0.03 |
| + BMI | 0.0004 | 0.001 | 0.003 | 0.7 | 0.02 | 0.01 | 0.03 | 0.001 | 0.03 | 0.03 | 0.007 | 0.03 | 0.07 | 0.04 | 0.01 | 0.03 | |
| + ethnicity | 0.0004 | 0.001 | 0.03 | 0.6 | 0.02 | 0.01 | 0.05 | 0.006 | 0.02 | 0.03 | 0.03 | 0.1 | 0.05 | 0.04 | 0.03 | 0.1 | |
| Preterm birth | + age | −0.002 | 0.002 | 0.01 | 0.3 | −0.02 | 0.01 | 0.02 | 0.1 | −0.14 | 0.12 | 0.02 | 0.4 | −0.13 | 0.13 | 0.01 | 0.6 |
| + BMI | −0.002 | 0.002 | 0.01 | 0.3 | −0.02 | 0.02 | 0.02 | 0.09 | −0.14 | 0.12 | 0.02 | 0.4 | −0.13 | 0.14 | 0.01 | 0.5 | |
| + ethnicity | −0.002 | 0.002 | 0.01 | 0.3 | −0.02 | 0.01 | 0.02 | 0.1 | −0.14 | 0.13 | 0.02 | 0.5 | −0.12 | 0.14 | 0.01 | 0.6 | |
| PROM | + age | −0.0003 | 0.002 | 0.0003 | 0.8 | −0.01 | 0.01 | 0.01 | 0.4 | −0.06 | 0.06 | 0.01 | 0.5 | −0.06 | 0.07 | 0.01 | 0.6 |
| + BMI | −0.0004 | 0.002 | 0.001 | 0.8 | −0.01 | 0.01 | 0.01 | 0.3 | −0.07 | 0.06 | 0.01 | 0.4 | −0.06 | 0.08 | 0.01 | 0.5 | |
| + ethnicity | −0.0004 | 0.002 | 0.001 | 0.8 | −0.01 | 0.01 | 0.01 | 0.3 | −0.07 | 0.07 | 0.01 | 0.4 | −0.07 | 0.08 | 0.02 | 0.6 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernando, M.; Ellery, S.J.; de Guingand, D.; Marquina, C.; Lim, S.; Harrison, C.L.; Teede, H.J.; Naderpoor, N.; Mousa, A. Early Pregnancy Vitamin D Binding Protein Is Independently Associated with the Development of Gestational Diabetes: A Retrospective Cohort Study. J. Clin. Med. 2020, 9, 2186. https://doi.org/10.3390/jcm9072186
Fernando M, Ellery SJ, de Guingand D, Marquina C, Lim S, Harrison CL, Teede HJ, Naderpoor N, Mousa A. Early Pregnancy Vitamin D Binding Protein Is Independently Associated with the Development of Gestational Diabetes: A Retrospective Cohort Study. Journal of Clinical Medicine. 2020; 9(7):2186. https://doi.org/10.3390/jcm9072186
Chicago/Turabian StyleFernando, Melinda, Stacey J. Ellery, Deborah de Guingand, Clara Marquina, Siew Lim, Cheryce L. Harrison, Helena J. Teede, Negar Naderpoor, and Aya Mousa. 2020. "Early Pregnancy Vitamin D Binding Protein Is Independently Associated with the Development of Gestational Diabetes: A Retrospective Cohort Study" Journal of Clinical Medicine 9, no. 7: 2186. https://doi.org/10.3390/jcm9072186
APA StyleFernando, M., Ellery, S. J., de Guingand, D., Marquina, C., Lim, S., Harrison, C. L., Teede, H. J., Naderpoor, N., & Mousa, A. (2020). Early Pregnancy Vitamin D Binding Protein Is Independently Associated with the Development of Gestational Diabetes: A Retrospective Cohort Study. Journal of Clinical Medicine, 9(7), 2186. https://doi.org/10.3390/jcm9072186