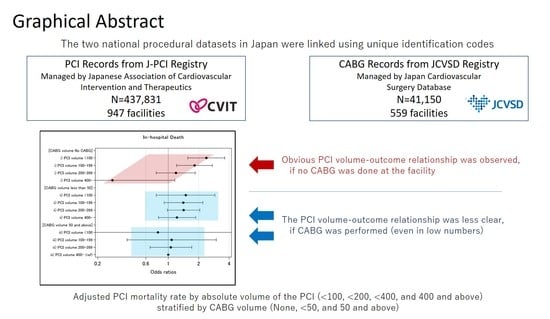
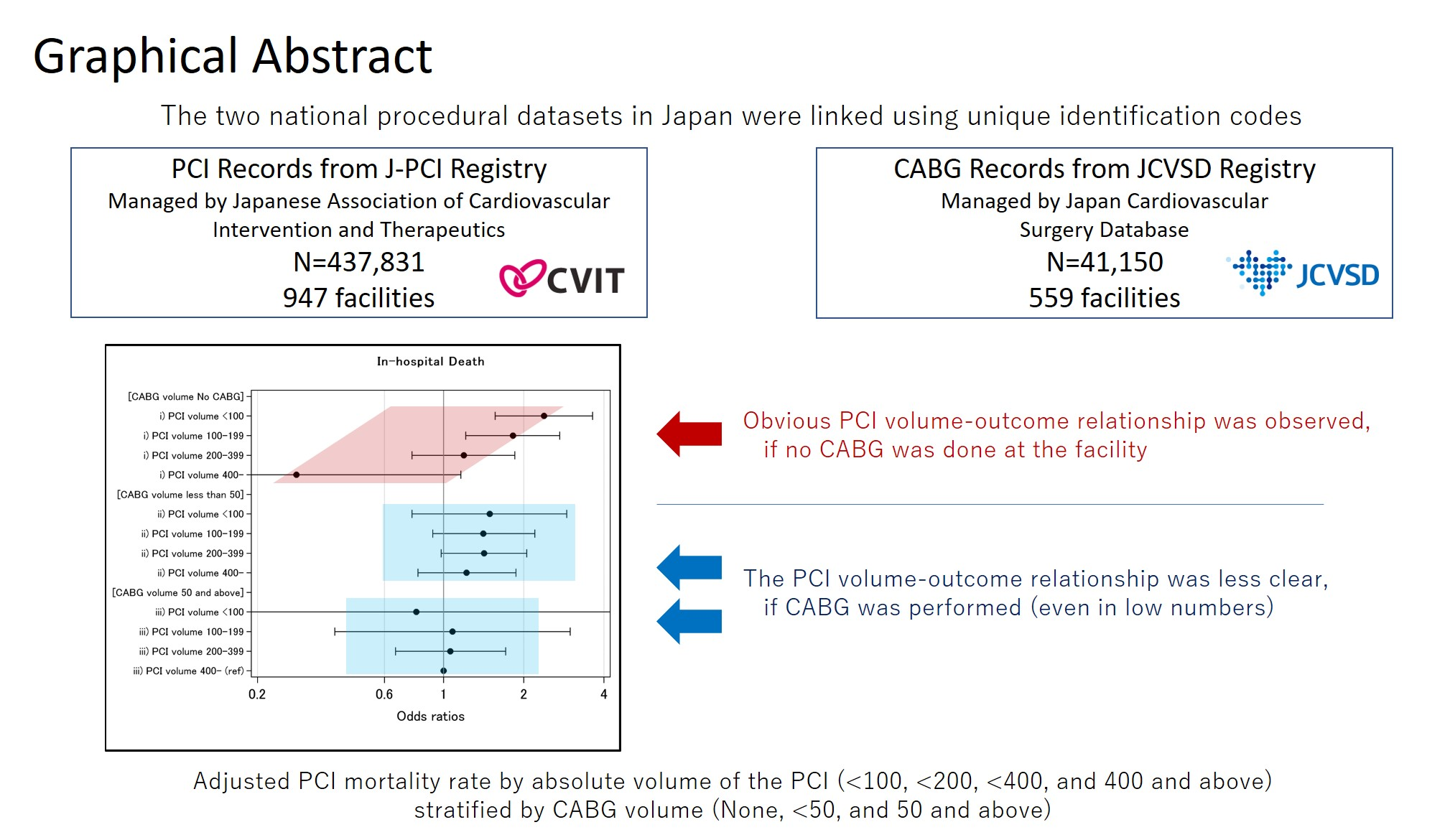
Outcome of Percutaneous Coronary Intervention in Relation to the Institutional Volume of Coronary Artery Bypass Surgery †

 ,
,
Abstract
1. Introduction
2. Methods
2.1. Data Sources
2.1.1. Japanese Cardiovascular Intervention and Therapeutics Registry: J-PCI
2.1.2. Japan Cardiovascular Surgical Database Adult Division: JCVSD Adult Division
2.1.3. Study Approval
2.2. Study Patients
2.3. Hospital Category
2.4. Study Outcomes
2.5. Statistical Analysis
3. Results
4. Outcomes
5. Discussion
6. Limitations
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
List of Abbreviations
| ACCF | American College of Cardiology Foundation |
| AHA | American Heart Association |
| CABG | coronary artery bypass grafting |
| JCVSD | Japan Cardiovascular Surgical Database |
| J-PCI | PCI Registry for Japanese Association of Cardiovascular Intervention & Therapeutics |
| PCI | percutaneous coronary intervention |
| SCAI | Society for Cardiovascular Angiography and Interventions |
References
- Rashid, M.; Sperrin, M.; Ludman, P.F.; O’Neill, D.; Nicholas, O.; de Belder, M.A.; Mamas, M.A. Impact of operator volume for percutaneous coronary intervention on clinical outcomes: What do the numbers say? Eur Heart J. Qual. Care Clin. Outcomes. 2016, 2, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Kohsaka, S.; Miyata, H.; Ueda, I.; Masoudi, F.A.; Peterson, E.D.; Maekawa, Y.; Kawamura, A.; Fukuda, K.; Roe, M.T.; Rumsfeld, J.S. JCD-KiCS and NCDR. An international comparison of patients undergoing percutaneous coronary intervention: A collaborative study of the National Cardiovascular Data Registry (NCDR) and Japan Cardiovascular Database-Keio interhospital Cardiovascular Studies (JCD-KiCS). Am. Heart J. 2015, 170, 1077–1085. [Google Scholar] [PubMed]
- Lee, J.M.; Hwang, D.; Park, J.; Kim, K.J.; Ahn, C.; Koo, B.K. Percutaneous Coronary Intervention at Centers With and Without On-Site Surgical Backup: An Updated Meta-Analysis of 23 Studies. Circulation. 2015, 132, 388–401. [Google Scholar] [CrossRef] [PubMed]
- Goel, K.; Gupta, T.; Kolte, D.; Khera, S.; Fonarow, G.C.; Bhatt, D.L.; Singh, M.; Rihal, C.S. Outcomes and Temporal Trends of Inpatient Percutaneous Coronary Intervention at Centers With and Without On-site Cardiac Surgery in the United States. JAMA Cardiol. 2017, 2, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Levine, G.N.; Bates, E.R.; Blankenship, J.C.; Bailey, S.R.; Bittl, J.A.; Cercek, B.; Chambers, C.E.; Ellis, S.G.; Guyton, R.A. 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Circulation 2011, 124, e574–e651. [Google Scholar]
- Health at a Glance 2015: OECD Indicators; OECD Publishing: Paris, France, 2015.
- Fanaroff, C.A.; Zakroysky, P.; Dai, D.; Wojdyla, D.; Sherwood, W.M.; Roe, M.T.; Wang, T.Y.; Peterson, E.D.; Gurm, H.S.; Cohen, M.G. Outcomes of PCI in Relation to Procedural Characteristics and Operator Volumes in the United States. J. Am. Coll. Cardiol. 2017, 69, 2913–2924. [Google Scholar] [CrossRef]
- Hulme, W.; Sperrin, M.; Curzen, N.; Kinnaird, T.; De Belder, M.A.; Ludman, P.; Kwok, C.S.; Gale, C.P.; Cockburn, J.; Kontopantelis, E. Operator volume is not associated with mortality following percutaneous coronary intervention: Insights from the British Cardiovascular Intervention Society registry. Eur. Heart J. 2018, 39, 1623–1634. [Google Scholar] [CrossRef]
- Inohara, T.; Kohsaka, S.; Yamaji, K.; Amano, T.; Fujii, K.; Oda, H.; Uemura, S.; Kadota, K.; Miyata, H.; Nakamura, M. Impact of Institutional and Operator Volume on Short-Term Outcomes of Percutaneous Coronary Intervention: A Report from the Japanese Nationwide Registry. JACC Cardiovasc. Interv. 2017, 10, 918–927. [Google Scholar] [CrossRef]
- The Japanese Circulation Society. Survey on the Clinical Practice Pattern of Cardiovascular Disease. Available online: http://www.j-circ.or.jp/jittai_chosa/ (accessed on 10 January 2016). (In Japanese).
- Miyata, H.; Tomotaki, A.; Motomura, N.; Takamoto, S. Operative mortality and complication risk model for all major cardiovascular operations in Japan. Ann. Thorac. Surg. 2015, 99, 130–139. [Google Scholar] [CrossRef]
- Miyata, H.; Motomura, N.; Murakami, A.; Takamoto, S.; Japan Cardiovascular Surgery Datebase. Effect of benchmarking projects on outcomes of coronary artery bypass graft surgery: Challenges and prospects regarding the quality improvement initiative. J. Thorac. Cardiovasc. Surg. 2012, 143, 1364–1369. [Google Scholar] [CrossRef]
- Inohara, T.; Kohsaka, S.; Yamaji, K.; Ishii, H.; Amano, T.; Uemura, S.; Kadota, K.; Kumamaru, H.; Miyata, H.; Nakamura, M. Risk stratification model for in-hospital death in patients undergoing percutaneous coronary intervention: A nationwide retrospective cohort study in Japan. BMJ Open 2019, 9, e026683. [Google Scholar] [CrossRef] [PubMed]
- Miyata, H.; Motomura, N.; Ueda, Y.; Matsuda, H.; Takamoto, S. Effect of procedural volume on outcome of coronary artery bypass graft surgery in Japan: Implication toward public reporting and minimal volume standards. J. Thorac. Cardiovasc. Surg. 2008, 135, 1306–1312. [Google Scholar] [CrossRef] [PubMed]
- McGrath, P.D.; Wennberg, D.E.; Dickens, J.D.; Siewers, A.E.; Lucas, F.L.; Malenka, D.J.; Kellett, M.A., Jr.; Ryan, T.J., Jr. Relation between operator and hospital volume and outcomes following percutaneous coronary interventions in the era of the coronary stent. JAMA 2000, 284, 3139–3144. [Google Scholar] [CrossRef] [PubMed]
- Wennberg, D.E.; Lucas, F.L.; Siewers, A.E.; Kellett, M.A.; Malenka, D.J. Outcomes of percutaneous coronary interventions performed at centers without and with onsite coronary artery bypass graft surgery. JAMA. 2004, 292, 1961–1968. [Google Scholar] [CrossRef]
- Singh, M.; Rihal, C.S.; Gersh, B.J.; Lennon, R.J.; Prasad, A.; Sorajja, P.; Gullerud, R.E.; Holmes, D.R., Jr. Twenty-five-year trends in in-hospital and long-term outcome after percutaneous coronary intervention: A single-institution experience. Circulation 2007, 115, 2835–2841. [Google Scholar] [CrossRef]
- Seshadri, N.; Whitlow, P.L.; Acharya, N.; Houghtaling, P.; Blackstone, E.H.; Ellis, S.G. Emergency coronary artery bypass surgery in the contemporary percutaneous coronary intervention era. Circulation 2002, 106, 2346–2350. [Google Scholar] [CrossRef]
- Carey, J.S.; Danielsen, B.; Gold, J.P.; Rossiter, S.J. Procedure rates and outcomes of coronary revascularization procedures in California and New York. J. Thorac. Cardiovasc Surg. 2005, 129, 1276–1282. [Google Scholar] [CrossRef]
- Sanchez, C.E.; Badhwar, V.; Dota, A.; Schindler, J.; Chu, D.; Smith, A.J.C.; Lee, J.S.; Khandhar, S.; Toma, C.; Marroquin, O.C. Practical implementation of the coronary revascularization heart team. Circ. Cardiovasc. Qual. Outcomes 2013, 6, 598–603. [Google Scholar] [CrossRef]
- Endo, A.; Kawamura, A.; Miyata, H.; Noma, S.; Suzuki, M.; Koyama, T.; Ishikawa, S.; Nakagawa, S.; Takagi, S.; Numasawa, Y. Angiographic Lesion Complexity Score and In-Hospital Outcomes after Percutaneous Coronary Intervention. PLoS ONE 2015, 10, e0127217. [Google Scholar] [CrossRef]
- Spertus, J.A.; Decker, C.; Gialde, E.; Jones, P.G.; McNulty, E.J.; Bach, R.; Chhatriwalla, A.K. Precision medicine to improve use of bleeding avoidance strategies and reduce bleeding in patients undergoing percutaneous coronary intervention: Prospective cohort study before and after implementation of personalized bleeding risks. BMJ 2015, 350, h1302. [Google Scholar] [CrossRef]
- Inohara, T.; Kohsaka, S.; Miyata, H.; Ueda, I.; Maekawa, Y.; Fukuda, K.; Cohen, D.J.; Kennedy, K.F.; Rumsfeld, J.S.; Spertus, J.A. Performance and Validation of the U.S. NCDR Acute Kidney Injury Prediction Model in Japan. J. Am. Coll. Cardiol. 2016, 67, 1715–1722. [Google Scholar] [CrossRef] [PubMed]
- Coronary Revascularization Writing Group; Patel, M.R.; Gregory, J.; Dehmer, G.J.; Hirshfeld, J.W.; Smith, P.K.; Spertus, J.A.; Patel, J.A. ACCF/SCAI/STS/AATS/AHA/ASNC 2009 Appropriateness Criteria for Coronary Revascularization: A report by the American College of Cardiology Foundation Appropriateness Criteria Task Force, Society for Cardiovascular Angiography and Interventions, Society of Thoracic Surgeons, American Association for Thoracic Surgery, American Heart Association, and the American Society of Nuclear Cardiology Endorsed by the American Society of Echocardiography, the Heart Failure Society of America, and the Society of Cardiovascular Computed Tomography. J. Am. Coll. Cardiol. 2009, 53, 530–553. [Google Scholar]
- Desai, N.R.; Bradley, S.M.; Parzynski, C.S.; Nallamothu, B.K.; Chan, P.S.; Spertus, J.A.; Patel, M.R.; Ader, J.; Soufer, A.; Krumholz, H.M. Appropriate Use Criteria for Coronary Revascularization and Trends in Utilization, Patient Selection, and Appropriateness of Percutaneous Coronary Intervention. JAMA 2015, 314, 2045–2053. [Google Scholar] [CrossRef] [PubMed]
- Inohara, T.; Kohsaka, S.; Miyata, H.; Ueda, I.; Noma, S.; Suzuki, M.; Negishi, K.; Endo, A.; Nishi, Y.; Hayashida, K. Appropriateness of coronary interventions in Japan by the US and Japanese standards. Am. Heart J. 2014, 168, 854–861. [Google Scholar] [CrossRef]
- Hollingsworth, J.M.; Funk, R.J.; Garrison, S.A.; Owen-Smith, J.; Kaufman, S.A.; Pagani, F.D.; Nallamothu, B.K. Association Between Physician Teamwork and Health System Outcomes After Coronary Artery Bypass Grafting. Circ. Cardiovasc. Qual. Outcomes 2016, 9, 641–648. [Google Scholar] [CrossRef]
- Sedlis, S.P.; Hartigan, P.M.; Teo, K.K.; Maron, D.J.; Spertus, J.A.; Mancini, G.J.; Kostuk, W.; Chaitman, B.R.; Berman, D.; Lorin, J.D. Effect of PCI on Long-Term Survival in Patients with Stable Ischemic Heart Disease. N. Engl. J. Med. 2015, 373, 1937–1946. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| CABG Volume Category | No CABG | 1–49 | 50 and above | p-Value |
|---|---|---|---|---|
| N (total = 220,934) | 56,580 | 110,459 | 53,895 | |
| Age category | <0.001 | |||
| 20–39 | 391 (0.7%) | 1046 (1.0%) | 450 (0.8%) | |
| 40–59 | 9058 (16.0%) | 19,529 (17.7%) | 9498 (17.6%) | |
| 50–74 | 24,885 (44.0%) | 49,934 (45.2%) | 24,677 (45.8%) | |
| 75 and above | 22,246 (39.3%) | 39,950 (36.2%) | 19,270 (35.8%) | |
| Diagnosis | <0.001 | |||
| Stable Angina | 17,688 (31.3%) | 33,706 (30.5%) | 18,654 (34.6%) | |
| Unstable Angina | 10,663 (18.9%) | 18,332 (16.6%) | 8648 (16.1%) | |
| Acute Myocardial Infarction | 17,927 (31.7%) | 33,706 (30.5%) | 18,654 (34.6%) | |
| Old Myocardial Infarction | 1572 (2.8%) | 3095 (2.8%) | 1494 (2.8%) | |
| Silent Myocardial Ischemia | 8267 (14.6%) | 12,062 (10.9%) | 6030 (11.2%) | |
| Other | 463 (0.8%) | 1070 (1.0%) | 430 (0.8%) | |
| Emergent procedure | 21,140 (37.4%) | 49,042 (44.4%) | 21,981 (40.8%) | <0.001 |
| Number of Vessels treated | <0.001 | |||
| 1 | 51,221 (90.5%) | 98,451 (89.1%) | 47,880 (88.8%) | |
| 2 | 3127 (5.5%) | 6398 (5.8%) | 3285 (6.1%) | |
| 3 or include LMT | 2232 (3.9%) | 510 (5.1%) | 2730 (5.1%) | |
| Preprocedural condition | ||||
| Cardiac Shock within 24 h of procedure | 2093 (3.7%) | 5347 (4.8%) | 1979 (3.7%) | <0.001 |
| Acute heart failure | 3032 (5.4%) | 6419 (5.8%) | 2637 (4.9%) | <0.001 |
| Cardiac Arrest within 24 h | 904 (1.6%) | 2933 (2.7%) | 1195 (2.2%) | <0.001 |
| Comorbidities | ||||
| Past Heart Failure | 4830 (8.5%) | 9647 (8.7%) | 4905 (9.1%) | <0.001 |
| COPD | 969 (1.7%) | 1960 (1.8%) | 947 (1.8%) | 0.66 |
| Hemodialysis | 2227 (3.9%) | 4715 (4.3%) | 2562 (4.8%) | <0.001 |
| Renal dysfunction | 6633 (11.7%) | 15,322 (13.9%) | 7591 (14.1%) | <0.001 |
| Diabetes | 21,395 (37.8%) | 41,911 (37.9%) | 20,167 (37.4%) | 0.12 |
| AAA/PAD | 2946 (5.2%) | 5813 (5.3%) | 3258 (6.1%) | <0.001 |
| Hypertension | 39,412 (69.7%) | 77,633 (70.3%) | 39,180 (72.7%) | <0.001 |
| Number of facilities | 437 | 389 | 117 | |
| Mean annual Case Volume | <0.001 | |||
| 1–99 | 197 (45.1%) | 35 (9.0%) | 3 (2.6%) | |
| 100–199 | 145 (33.2%) | 83 (21.3%) | 9 (7.7%) | |
| 200–399 | 87 (19.9%) | 194 (50.1%) | 53 (45.3%) | |
| 400 and above | 8 (1.8%) | 76 (19.5%) | 52 (44.4%) | |
| Outcomes | ||||
| Deaths | 535 (1.0%) | 1221 (1.1%) | 423 (0.8%) | <0.001 |
| Composite Outcome | 1426 (2.5%) | 2831 (2.6%) | 1049 (2.0%) | <0.001 |
| A. | ||||
| Yearly CABG Volume | Yearly PCI Volume | |||
| 1–99 | 100–199 | 200–399 | 400 and above | |
| None | ||||
| Number of Facilities | 200 | 145 | 87 | 8 |
| Number of Patients | 10,429 | 20,680 | 21,390 | 4081 |
| In-Hospital Death | 144 (1.4%) | 231 (1.1%) | 157 (0.7%) | 3 (0.1%) |
| In-Hospital Complications | 315 (3.0%) | 601 (2.9%) | 482 (2.3%) | 28 (0.7%) |
| Number of Registered PCI Operators, median (min-max) | 2 (1–11) | 4 (1–13) | 6 (1–12) | 8.5 (1–14) |
| Number of PCI per operator | 14 | 25 | 35 | 50.5 |
| Predicted mortality, median (p5–p95) | 0.2% (0.04–2.7) | 0.2% (0.04–2.9) | 0.2% (0.04–2.6) | 0.1% (0.04–1.5) |
| Ratio (PCI/CABG) median (p25–p75) | – | – | – | – |
| 1–49 | ||||
| Number of Facilities | 36 | 83 | 195 | 76 |
| Number of Patients | 2442 | 13,600 | 56,666 | 37,751 |
| In-Hospital Death | 25 (1.0%) | 148 (1.1%) | 663 (1.2%) | 385 (1.0%) |
| In-Hospital Complications | 85 (3.5%) | 338 (2.5%) | 1518 (2.7%) | 890 (2.4%) |
| Number of Registered PCI Operators, median (min-max) | 3 (1–10) | 5 (1–24) | 8 (1–20) | 10 (4–23) |
| Number of PCI per operator | 11 | 20 | 27 | 39 |
| Predicted mortality, median (p5–p95) | 0.2% (0.04–4.3) | 0.3% (0.04–3.8) | 0.2% (0.04–4.3) | 0.2% (0.04–2.8) |
| Ratio (PCI/CABG) median (p25–p75) | 5.2 (2.5–9.2) | 7.9 (5.0–11.6) | 11.4 (8.2–15.8) | 17.9 (12.8–26.7) |
| 50 and above | ||||
| Number of Facilities | 3 | 9 | 53 | 52 |
| Number of Patients | 194 | 1291 | 16,285 | 36,125 |
| In-Hospital Death | 2 (1.0%) | 12 (0.9%) | 154 (1.0%) | 255 (0.7%) |
| In-Hospital Complications | 4 (2.1%) | 47 (3.6%) | 382 (2.4%) | 616 (1.7%) |
| Number of Registered PCI Operators, median (min-max) | 1 (1–5) | 6 (2–24) | 10 (4–28) | 15 (6–36) |
| Number of PCI per operator | 40 | 10.5 | 19 | 32 |
| Predicted mortality, median (p5–p95) | 0.3% (0.04–12.1) | 0.2% (0.04–4.0) | 0.2% (0.04–3.5) | 0.2% (0.04–2.4) |
| Ratio (PCI/CABG) median (p25–p75) | 0.5 (0.01–1.7) | 2.0 (1.5–2.7) | 4.2 (2.9–5.1) | 7.5 (5.1–10.5) |
| B. | ||||
| Yearly CABG Volume | Yearly PCI Volume | |||
| 1–99 | 100–199 | 200–399 | 400 and above | |
| None | ||||
| OR for in-hospital death | 2.38 (1.56–3.63) | 1.82 (1.21–3.73) | 1.19 (0.76–1.85) | 0.28 (0.07–1.16) |
| OR for in-hospital complications | 1.97 (1.44–2.70) | 1.83 (1.35–2.47) | 1.42 (1.02–1.96) | 0.71 (0.33–1.53) |
| 1–49 | ||||
| OR for in-hospital death | 1.49 (0.76–2.90) | 1.41 (0.91–2.20) | 1.42 (0.98–2.05) | 1.22 (0.80–1.87) |
| OR for in-hospital complications | 2.20 (1.39–3.48) | 1.26 (0.90–1.77) | 1.35 (1.02–1.79) | 1.18 (0.85–1.63) |
| 50 and above | ||||
| OR for in-hospital death | 0.79 (0.08–7.86) | 1.08 (0.39–2.99) | 1.06 (0.66–1.71) | reference group |
| OR for in-hospital complications | 1.23 (0.25–5.91) | 2.17 (1.08–4.36) | 1.19 (0.83–1.70) | reference group |
| (A) With inclusion of ACS patients only. | ||||
| Yearly CABG Volume | Yearly PCI Volume | |||
| 1–99 | 100–199 | 200–399 | 400 and above | |
| None | ||||
| OR for in-hospital death | 2.45 (1.58–3.78) | 1.82 (1.20–2.76) | 1.28 (0.81–2.03) | 0.34 (0.08–1.46) |
| OR for in-hospital complications | 2.09 (1.47–2.97) | 2.00 (1.43–2.80) | 1.65 (1.14–2.37) | 0.85 (0.36–2.03) |
| 1–49 | ||||
| OR for in-hospital death | 1.56 (0.79–3.07) | 1.39 (0.88–2.2) | 1.42 (0.97–2.08) | 1.18 (0.76–1.82) |
| OR for in-hospital complications | 2.33 (1.40–3.87) | 1.31 (0.90–1.90) | 1.45 (1.06–1.99) | 1.21 (0.85–1.74) |
| 50 or above | ||||
| OR for in-hospital death | 0.80 (0.08–8.20) | 0.99 (0.34–2.89) | 1.01 (0.62–1.66) | reference group |
| OR for in-hospital complications | 1.68 (0.31–8.95) | 2.04 (0.93–4.45) | 1.20 (0.81–1.79) | reference group |
| (B) With exclusion of institutions with extremely low number of PCI (<50/yr) or CABG (<15/yr) volume. | ||||
| Yearly CABG Volume | Yearly PCI Volume | |||
| 50–99 | 100–199 | 200–399 | 400 and above | |
| None | ||||
| OR for in-hospital death | 2.43 (1.54–3.84) | 1.82 (1.21–2.74) | 1.19 (0.76–1.86) | 0.28 (0.07–1.17) |
| OR for in-hospital complications | 2.13 (1.53–2.96) | 1.83 (1.36–2.47) | 1.42 (1.03–1.95) | 0.71 (0.33–1.51) |
| 15–49 | ||||
| OR for in-hospital death | 0.88 (0.31–2.56) | 1.29 (0.79–2.10) | 1.39 (0.95–2.05) | 1.29 (0.83–2.00) |
| OR for in-hospital complications | 1.33 (0.66–2.68) | 1.23 (0.86–1.77) | 1.29 (0.97–1.71) | 1.22 (0.88–1.70) |
| 50 or above | ||||
| OR for in-hospital death | 1.03 (0.08–12.95) | 1.08 (0.39–3.00) | 1.06 (0.66–1.71) | reference group |
| OR for in-hospital complications | 0.44 (0.05–3.88) | 2.17 (1.09–4.31) | 1.19 (0.84–1.70) | reference group |
| Yearly CABG Volume | Yearly PCI Volume | |||
|---|---|---|---|---|
| Max 210 | Max 313.5 | Max 478.5 | Above 478.5 | |
| None | ||||
| OR for in-hospital death | 2.02 (1.34–3.05) | 1.12 (0.67–1.87) | 0.91 (0.37–2.21) | 0.13 (0.01–1.35) |
| OR for in-hospital complications | 1.82 (1.34–2.47) | 1.39 (0.96–2.02) | 0.86 (0.46–1.63) | 0.71 (0.27–1.84) |
| Max 26.5 | ||||
| OR for in-hospital death | 1.73 (1.08–2.78) | 1.50 (0.92–2.43) | 1.15 (0.68–1.94) | 0.98 (0.46–2.07) |
| OR for in-hospital complications | 1.62 (1.14–2.31) | 1.26 (0.88–1.82) | 1.09 (0.73–1.61) | 0.7 (0.39–1.24) |
| Max 49 | ||||
| OR for in-hospital death | 1.05 (0.58–1.90) | 1.32 (0.8–2.18) | 1.23 (0.75–2.03) | 1.56 (0.86–2.85) |
| OR for in-hospital complications | 1.23 (0.80–1.91) | 1.28 (0.88–1.88) | 1.13 (0.77–1.65) | 1.68 (1.06–2.65) |
| 50 and above | ||||
| OR for in-hospital death | 1.20 (0.52–2.77) | 1.05 (0.58–1.91) | 1.09 (0.62–1.90) | reference group |
| OR for in-hospital complications | 2.01 (1.12–3.62) | 1.16 (0.75–1.81) | 1.01 (0.66–1.55) | reference group |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kohsaka, S.; Kumamaru, H.; Inohara, T.; Amano, T.; Akasaka, T.; Miyata, H.; Motomura, N.; Nakamura, M. Outcome of Percutaneous Coronary Intervention in Relation to the Institutional Volume of Coronary Artery Bypass Surgery. J. Clin. Med. 2020, 9, 1267. https://doi.org/10.3390/jcm9051267
Kohsaka S, Kumamaru H, Inohara T, Amano T, Akasaka T, Miyata H, Motomura N, Nakamura M. Outcome of Percutaneous Coronary Intervention in Relation to the Institutional Volume of Coronary Artery Bypass Surgery. Journal of Clinical Medicine. 2020; 9(5):1267. https://doi.org/10.3390/jcm9051267
Chicago/Turabian StyleKohsaka, Shun, Hiraku Kumamaru, Taku Inohara, Tetsuya Amano, Takashi Akasaka, Hiroaki Miyata, Noboru Motomura, and Masato Nakamura. 2020. "Outcome of Percutaneous Coronary Intervention in Relation to the Institutional Volume of Coronary Artery Bypass Surgery" Journal of Clinical Medicine 9, no. 5: 1267. https://doi.org/10.3390/jcm9051267
APA StyleKohsaka, S., Kumamaru, H., Inohara, T., Amano, T., Akasaka, T., Miyata, H., Motomura, N., & Nakamura, M. (2020). Outcome of Percutaneous Coronary Intervention in Relation to the Institutional Volume of Coronary Artery Bypass Surgery. Journal of Clinical Medicine, 9(5), 1267. https://doi.org/10.3390/jcm9051267