Three-Dimensional Morphological Changes of the True Cleft under Passive Presurgical Orthopaedics in Unilateral Cleft Lip and Palate: A Retrospective Cohort Study

 , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Plaster Casts
2.2. Passive Plate Therapy
2.3. Three-Dimensional Analysis
2.4. Statistical Analysis
3. Results
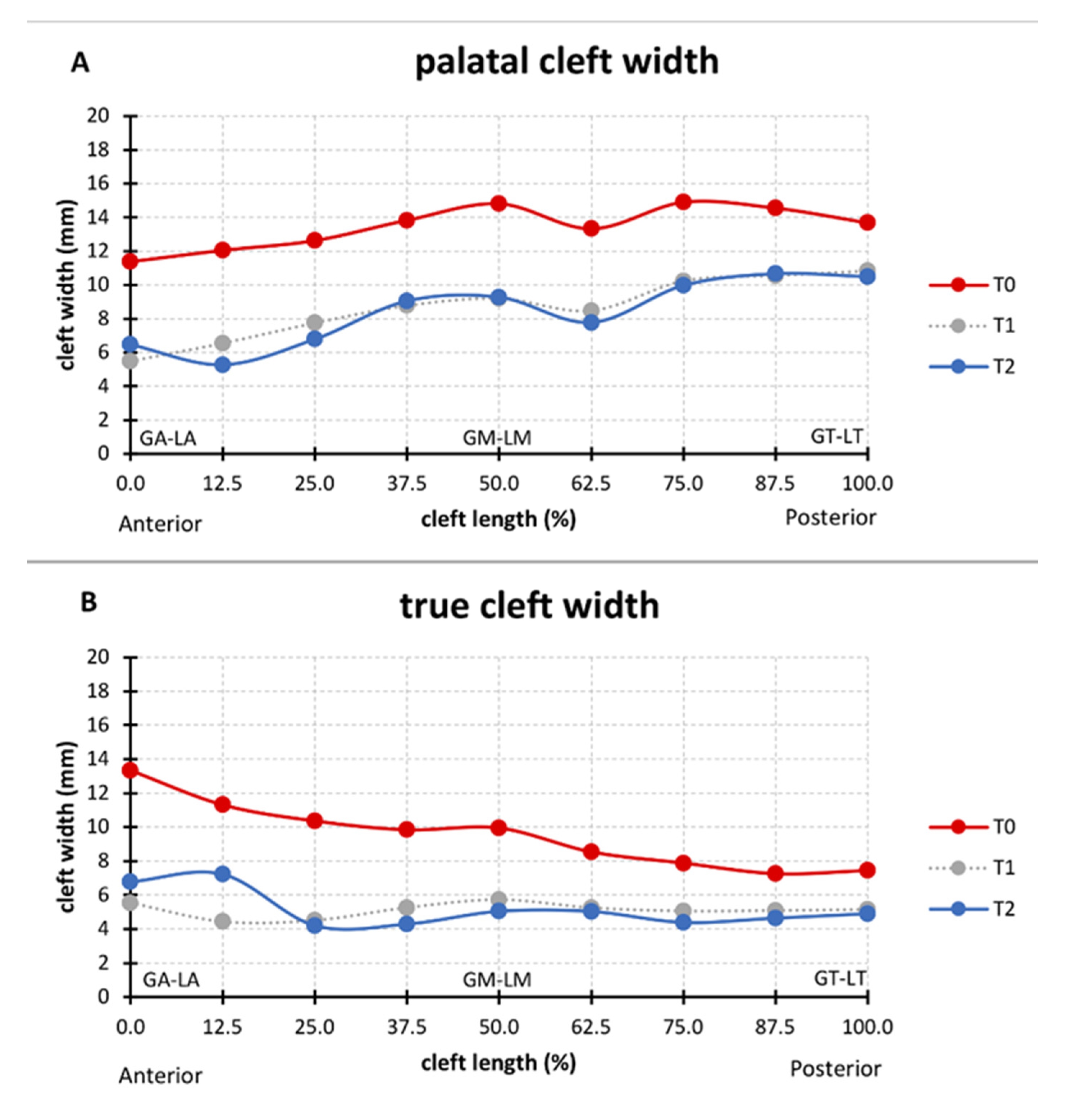
3.1. Cleft Width
3.2. Changes in Palatal and True Cleft Areas
3.3. Changes in the Height of the Palatal Surface
4. Discussion
4.1. Three-Dimensional Analysis
4.2. Cleft Width
4.3. Changes in the Palatal and True Cleft Areas
4.4. Changes in the Height of the Palatal Surface
4.5. Clinical Translation of the Findings
4.6. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Veau, V. Division Palatine. Anatomie. Chirurgie. Phonétique. Avec la Collaboration de Mlle S. Borel.; Impr. Darantière Masson et Cie éditeurs: Dijon/Paris, France, 1931. [Google Scholar]
- Stöckli, P.W. Application of a quantitative method for arch form evaluation in complete unilateral cleft lip and palate. Cleft Palate J. 1971, 8, 322–341. [Google Scholar] [PubMed]
- Grabowski, R.; Kopp, H.; Stahl, F.; Gundlach, K.K.H. Presurgical orthopaedic treatment of newborns with clefts - functional treatment with long-term effects. J. Cranio-Maxillofacial Surg. 2006, 34, 34–44. [Google Scholar] [CrossRef]
- Wada, T.; Miyazaki, T. Treatment principles for the changing arch form in children with complete unilateral cleft lips and palates. Cleft Palate J 1976, 13, 273–283. [Google Scholar]
- Peltomäki, T.; Vendittelli, B.L.; Grayson, B.H.; Cutting, C.B.; Brecht, L.E. Associations between Severity of Clefting and Maxillary Growth in Patients with Unilateral Cleft Lip and Palate Treated with Infant Orthopedics. Cleft Palate-Craniofacial J. 2001, 38, 582–586. [Google Scholar] [CrossRef] [PubMed]
- Jorge, P.K.; Gnoinski, W.; Vaz Laskos, K.; Felício Carvalho Carrara, C.; Gamba Garib, D.; Okada Ozawa, T.; Andrade Moreira Machado, M.A.; Pinelli Valarelli, F.; Oliveira, T.M. Comparison of two treatment protocols in children with unilateral complete cleft lip and palate: Tridimensional evaluation of the maxillary dental arch. J. Craniomaxillofac. Surg. 2016, 44, 1117–1122. [Google Scholar] [CrossRef] [PubMed]
- Yamanishi, T.; Nishio, J.; Kohara, H.; Hirano, Y.; Sako, M.; Yamanishi, Y.; Adachi, T.; Miya, S.; Mukai, T. Effect on Maxillary Arch Development of Early 2-Stage Palatoplasty by Modified Furlow Technique and Conventional 1-Stage Palatoplasty in Children With Complete Unilateral Cleft Lip and Palate. J. Oral Maxillofac. Surg. 2009, 67, 2210–2216. [Google Scholar] [CrossRef]
- Seckel, N.G.; Van der Tweel, I.; Elema, G.A.; Specken, T.F.J.M.C. Landmark positioning on maxilla of cleft lip and palate infant - A reality? Cleft Palate-Craniofacial J. 1995, 32, 434–441. [Google Scholar] [CrossRef]
- Shetty, V.; Agrawal, R.K.; Sailer, H.F. Long-term effect of presurgical nasoalveolar molding on growth of maxillary arch in unilateral cleft lip and palate: Randomized controlled trial. Int. J. Oral Maxillofac. Surg. 2017, 46, 977–987. [Google Scholar] [CrossRef]
- Mazaheri, M.; Harding, R.L.; Cooper, J.A.; Meier, J.A.; Jones, T.S. Changes in arch form and dimensions of cleft patients. Am. J. Orthod. 1971, 60, 19–32. [Google Scholar] [CrossRef]
- Schmidt-Flath, I.; Fränkel, R.; Grabowski, R.; Opitz, C.; Wiemann, C. Methoden zur Ausmessung des Säuglingskiefers, des Milch- und bleibenden Gebisses beim Spaltträger. Fortschr. Kieferorthop. 1972, 33, 457–476. [Google Scholar] [CrossRef]
- Berkowitz, S.; Pruzansky, S. Stereophotogrammerty of serial casts of cleft palate. Angle Orthod. 1968, 38, 136–149. [Google Scholar] [PubMed]
- Berkowitz, S.; Duncan, R.; Evans, C.; Friede, H.; Kuijpers-Jagtman, A.M.; Prahl-Anderson, B.; Rosenstein, S. Timing of cleft palate closure should be based on the ratio of the area of the cleft to that of the palatal segments and not on age alone. Plast. Reconstr. Surg. 2005, 115, 1483–1499. [Google Scholar] [CrossRef] [PubMed]
- Leighton, B.C. Morphologische Variationender Alveolarbögen beim Neugeborenen. Fortschr. Kieferorthop. 1976, 37, 8–14. [Google Scholar] [CrossRef]
- Botticelli, S.; Pedersen, T.K.; Küseler, A.; Nørholt, S.E.; Cattaneo, P.M. Novel 3-D Analysis for the Assessment of Cleft Dimensions on Digital Models of Infants With Unilateral Cleft Lip and Palate. Cleft Palate. Craniofac. J. 2019, 56, 127–133. [Google Scholar] [CrossRef]
- Malek, R. Cleft Lip and Palate: Lesions, Pathophysiology and Primary Treatment, 1st ed.; Martin, D., Ed.; CRC Press: London, UK, 27 November 2000; ISBN 978-1853174919. [Google Scholar]
- Dahlberg, G. Statistical Methods for Medical and Biological Students. Br. Med. J. 1940, 2, 358. [Google Scholar]
- Robertson, N.R.; Fish, J. Early dimensional changes in the arches of cleft palate children. Am. J. Orthod. 1975, 67, 290–303. [Google Scholar] [CrossRef]
- Long, R.E.; Daskalogiannakis, J.; Mercado, A.M.; Hathaway, R.R.; Fessler, J.; Russell, K.A. The americleft project: Plaster dental casts versus digital images for GOSLON yardstick ratings when used in intercenter comparisons. J. Craniofac. Surg. 2017, 28, 1269–1273. [Google Scholar] [CrossRef]
- Ye, B.; Ruan, C.; Hu, J.; Yang, Y.; Ghosh, A.; Jana, S.; Zhang, G. A Comparative Study on Dental-arch Morphology in Adult Unoperated and Operated Cleft Palate Patients. J. Craniofac. Surg. 2010, 21, 811–815. [Google Scholar] [CrossRef]
- Brief, J.; Behle, J.H.; Stellzig-Eisenhauer, A.; Hassfeld, S. Precision of landmark positioning on digitized models from patients with cleft lip and palate. Cleft Palate. Craniofac. J. 2006, 43, 168–173. [Google Scholar] [CrossRef]
- Oxnard, C.E. The measurement of form: Beyond biometrics. Sausages and stars, dumbbells and doughnuts: Peculiar views of anatomical structures. Cleft Palate J. 1986, 23, 110–128. [Google Scholar]
- Santiago, P.E.; Grayson, B.H.; Cutting, C.B.; Gianoutsos, M.P.; Brecht, L.E.; Kwon, S.M. Reduced Need for Alveolar Bone Grafting by Presurgical Orthopedics and Primary Gingivoperiosteoplasty. Cleft Palate-Craniofacial J. 1998, 35, 77–80. [Google Scholar] [CrossRef] [PubMed]
- Hotz, M.M.; Gnoinski, W.M.; Nussbaumer, H.; Kistler, E. Early maxillary orthopedics in CLP cases: Guidelines for surgery. Cleft Palate J. 1978, 15, 405–411. [Google Scholar] [PubMed]
- Bykowski, M.R.; Naran, S.; Winger, D.G.; Losee, J.E. The rate of oronasal fistula following primary cleft palate surgery: A meta-analysis. Cleft Palate-Craniofacial J. 2015, 52, e81–e87. [Google Scholar] [CrossRef] [PubMed]
- Isogawa, N.; Ochiai, S.; Mito, T.; Kindaichi, J.; Ishibashi, N.; Takagi, Y.; Ishikawa, M. Three-Dimensional Comparison in Palatal Forms Between Modified Presurgical Nasoalveolar Molding Plate and Hotz’s Plate Applied to the Infants with Unilateral Cleft Lip and Palate. Singapore Dent. J. 2010, 31, 36–42. [Google Scholar] [CrossRef]
- Mishima, K.; Sugahara, T.; Mori, Y.; Sakuda, M. Three-Dimensional Comparison between the Palatal Forms in Infants with Complete Unilateral Cleft Lip, Alveolus, and Palate (UCLP) with and without Hotz’s Plate. Cleft Palate-Craniofacial J. 1996, 33, 245–251. [Google Scholar] [CrossRef]
- Huddart, A.G. Presurgical changes in unilateral cleft palate subjects. Cleft Palate J. 1979, 16, 147–157. [Google Scholar]
- Gnoinski, W. Infant Orthopedics and Later Orthodontic Monitoring for Unilateral Cleft Lip and Palate Patients in Zurich; Bardach, J., Morris, H., Eds.; WB Saunders Co: Philadelphia, PA, USA, 1990. [Google Scholar]
- Prahl, C.; Kuijpers-Jagtman, A.M.; van’t Hof, M.A.; Prahl-Andersen, B. A randomised prospective clinical trial into the effect of infant orthopaedics on maxillary arch dimensions in unilateral cleft lip and palate (Dutchcleft). Eur. J. Oral Sci. 2001, 109, 297–305. [Google Scholar] [CrossRef]
- Bongaarts, C.A.M.; van ’t Hof, M.A.; Prahl-Andersen, B.; Dirks, I.V.; Kuijpers-Jagtman, A.M. Infant orthopedics has no effect on maxillary arch dimensions in the deciduous dentition of children with complete unilateral cleft lip and palate (Dutchcleft). Cleft Palate. Craniofac. J. 2006, 43, 665–672. [Google Scholar] [CrossRef]
- Noverraz, R.L.M.; Disse, M.A.; Ongkosuwito, E.M.; Kuijpers-Jagtman, A.M.; Prahl, C. Transverse dental arch relationship at 9 and 12 years in children with unilateral cleft lip and palate treated with infant orthopedics: A randomized clinical trial (DUTCHCLEFT). Clin. Oral Investig. 2015, 19, 2255–2265. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Abbreviation | Name | Definition |
|---|---|---|
| Q | Lateral sulcus vertex | Point where the lateral sulcus intersects the crest of the ridge of the greater segment [4] |
| T/T’ | Tuberosity vertex | Points where the tuberosity border intersects the crest of the ridge of the greater (T) and lesser (T’) segments [10] The base plane runs through T and T’ and is perpendicular to the plane defined by (Q, T, T’) The base line connects T–T’ within the base plane |
| g | Greater ridge | Path of the greater segment’s palatal shelf ridge, that is at the junction with the vomer [1] |
| v | Vomer edge | Path along the maximal curvature of the vomer |
| l | Lesser ridge | Path of the lesser segment’s palatal shelf ridge |
| GA (=VA) | Greater anterior (=Vomer anterior) | Most-anterior point on the ridge of the greater segment where it intersects with the vomer edge |
| GT | Greater posterior | Point where the ridge of the greater segment intersects the base plane |
| GM | Greater midpoint | Point halfway between GA and GT following the path on the ridge of the greater segment |
| LA | Lesser anterior | Most-anterior point on the ridge of the lesser segment ridge |
| LT | Lesser posterior | Point where the ridge of the lesser segment intersects the base plane |
| LM | Lesser midpoint | Point halfway between LA and LT following the path on the ridge of the lesser segment |
| VT | Vomer posterior | Point where the vomer edge intersects the base plane |
| VM | Vomer midpoint | Point halfway between VA (=GA) and VT following the path on the vomer edge |
| Abbreviation | Description |
|---|---|
| Cleft area dimensions | |
| GA/GM/GT–LA/LM/LT | Total palatal cleft area (PCA) |
| VA/VM/VT–LA/LM/LT | Total true cleft area (TCA) |
| Transverse dimensions | |
| GA–LA | Anterior palatal cleft width |
| GM–LM | Middle palatal cleft width |
| GT–LT | Posterior palatal cleft width |
| VA–LA | Anterior true cleft width |
| VM–LM | Middle true cleft width |
| VT–LT | Posterior true cleft width |
| Vertical dimensions1 | |
| g-height | Height of the palatal shelf ridge of the greater segment perpendicular to the horizontal plane |
| l-height | Height of the palatal shelf ridge of the lesser segment perpendicular to the horizontal plane |
| v-height | Height of the vomer edge perpendicular to the horizontal plane |
| Cleft Area (mm2) | Section | T0 Median (IQR) | T2 Median (IQR) | p-Value | |||
|---|---|---|---|---|---|---|---|
| PCA | Total | 0%–100% | 334 | (294.9–349.8) | 228.8 | (205–287.9) | 0.0015 |
| Anterior | 0–25% | 75.3 | (67.2–93.3) | 49.4 | (32.0–70.0) | 0.0090 | |
| Middle | 25–75% | 157.0 | (141.5–173.8) | 116.9 | (99.7–135.0) | 0.0076 | |
| Posterior | 75–100% | 91.8 | (77.5–102.6) | 75.0 | (61.5–84.2) | 0.0090 | |
| TCA | Total | 0–100% | 185.4 | (151.5–220.1) | 121.1 | (100.2–144.6) | 0.0015 |
| Anterior | 0–25% | 56.9 | (40.9–66.6) | 41.7 | (18.1–51.3) | 0.0409 | |
| Middle | 25–75% | 84.7 | (69.6–102.8) | 60.0 | (42.3–62.2) | 0.0007 | |
| Posterior | 75–100% | 41.2 | (31.5–48.5) | 24.2 | (20.3–32.35) | 0.0012 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nalabothu, P.; Benitez, B.K.; Dalstra, M.; Verna, C.; Mueller, A.A. Three-Dimensional Morphological Changes of the True Cleft under Passive Presurgical Orthopaedics in Unilateral Cleft Lip and Palate: A Retrospective Cohort Study. J. Clin. Med. 2020, 9, 962. https://doi.org/10.3390/jcm9040962
Nalabothu P, Benitez BK, Dalstra M, Verna C, Mueller AA. Three-Dimensional Morphological Changes of the True Cleft under Passive Presurgical Orthopaedics in Unilateral Cleft Lip and Palate: A Retrospective Cohort Study. Journal of Clinical Medicine. 2020; 9(4):962. https://doi.org/10.3390/jcm9040962
Chicago/Turabian StyleNalabothu, Prasad, Benito K. Benitez, Michel Dalstra, Carlalberta Verna, and Andreas A. Mueller. 2020. "Three-Dimensional Morphological Changes of the True Cleft under Passive Presurgical Orthopaedics in Unilateral Cleft Lip and Palate: A Retrospective Cohort Study" Journal of Clinical Medicine 9, no. 4: 962. https://doi.org/10.3390/jcm9040962
APA StyleNalabothu, P., Benitez, B. K., Dalstra, M., Verna, C., & Mueller, A. A. (2020). Three-Dimensional Morphological Changes of the True Cleft under Passive Presurgical Orthopaedics in Unilateral Cleft Lip and Palate: A Retrospective Cohort Study. Journal of Clinical Medicine, 9(4), 962. https://doi.org/10.3390/jcm9040962