Changes in Office Blood Pressure Control, Augmentation Index, and Liver Steatosis in Kidney Transplant Patients after Successful Hepatitis C Infection Treatment with Direct Antiviral Agents

 , ,
, ,
Abstract
1. Introduction
2. Material and Methods
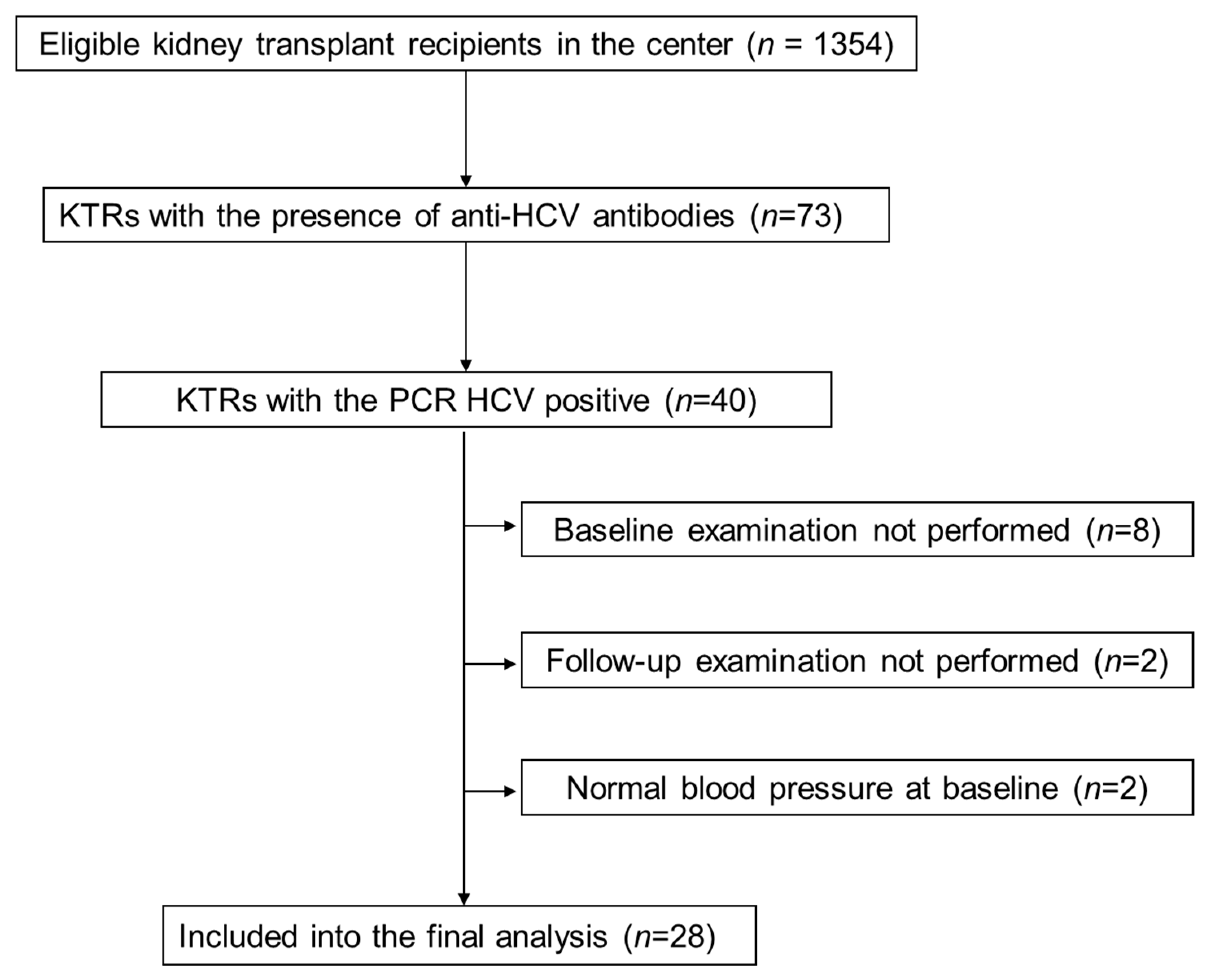
2.1. Study Group
2.2. Clinical, Anthropometric, and Laboratory Measurements
2.3. Echocardiography
2.4. Brachial Artery Flow-Mediated Dilation
2.5. Central Aortic Pressure and Arterial Stiffness Measurement
2.6. Liver Elastography
2.7. Data and Statistical Analysis
3. Results
3.1. Study Group
3.2. Study Subgroups Based on Blood Pressure Control
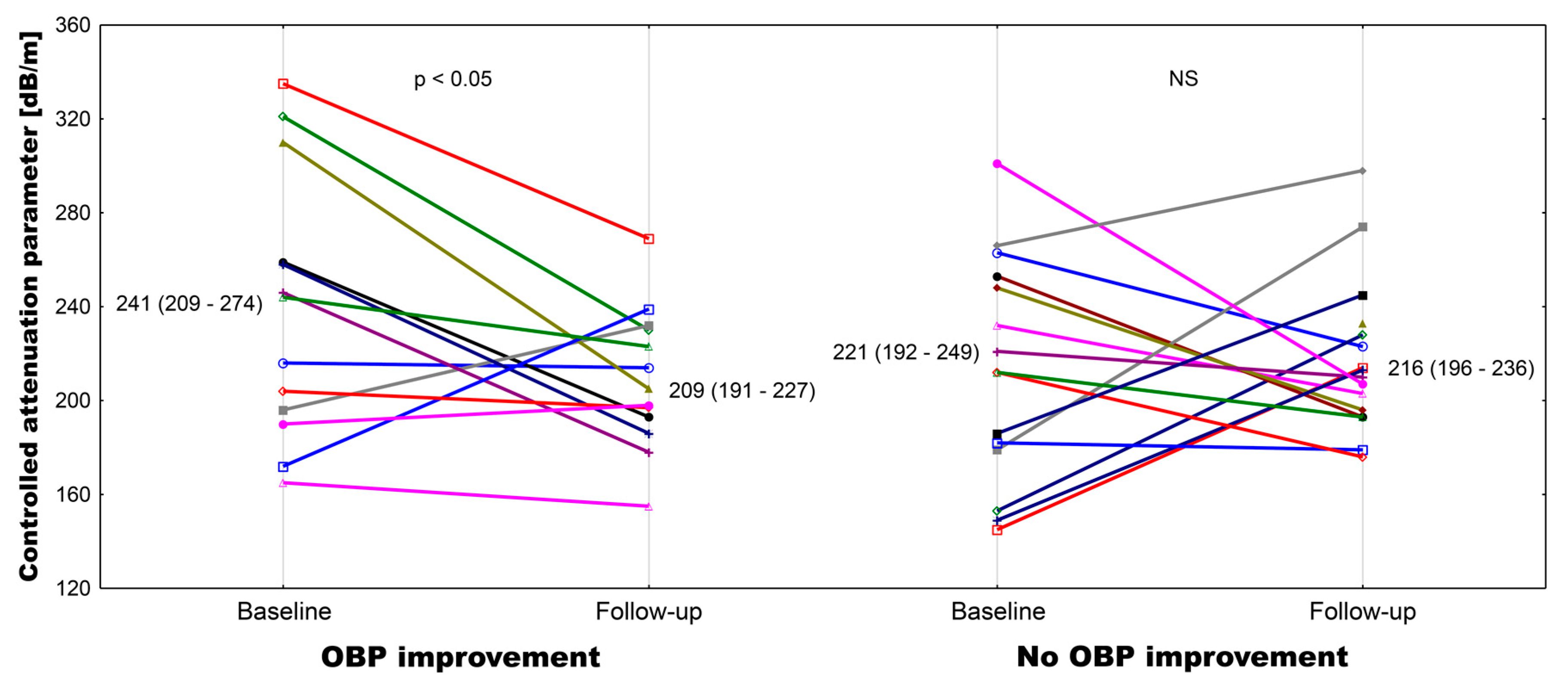
3.3. Liver Function Tests and Liver Morphologic Assessments
3.4. Central Blood Pressure Parameters
3.5. Arterial Structural and Functional Measurements
3.6. Cardiac Parameters
3.7. Inflammatory Markers
3.8. Fibroblast Growth Factor 21 Levels
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Divac, N.; Naumovic, R.; Stojanovic, R.; Prostran, M. The role of immunosuppressive medications in the pathogenesis of hypertension and efficacy of antihypertensive agents in kidney transplant recipients. Curr. Med. Chem. 2015, 23, 1941–1952. [Google Scholar] [CrossRef]
- Wadei, H.M.; Textor, S.C. Hypertension in the kidney transplant recipients. Transplant. Rev. 2010, 24, 105–120. [Google Scholar] [CrossRef]
- Arias, M.; Fernández-Fresnedo, G.; Gago, M.; Rodrigo, E.; Gómez-Alamillo, C.; Toyos, C.; Allende, N. Clinical characteristics of resistant hypertension in renal transplant recipients. Nephrol. Dial. Transplant. 2012, 27 (Suppl. 4), 36–38. [Google Scholar] [CrossRef][Green Version]
- Azancot, M.A.; Ramos, N.; Moreso, F.J.; Ibernon, M.; Espinel, E.; Torres, I.B.; Fort, J.; Seron, D. Hypertension in chronic kidney disease: The influence of renal transplantation. Transplantation 2014, 98, 537–542. [Google Scholar] [CrossRef] [PubMed]
- Opelz, G.; Wujciak, T.; Ritz, E. Association of chronic kidney graft failure with recipient blood pressure. Kidney Int. 1998, 53, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Sarnak, M.J.; Levey, A.S.; Schoolwerth, A.C.; Coresh, J.; Culleton, B.; Hamm, L.L.; McCullough, P.A.; Kasiske, B.L.; Kelepouris, E.; Klag, M.J.; et al. Kidney disease as a risk factor for development of cardiovascular disease: A statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Circulation 2002, 108, 154–169. [Google Scholar]
- Stenvinkel, P.; Carrero, J.J.; Axelsson, J.; Lindholm, B.; Heimburger, O.; Massy, Z. Emerging biomarkers for evaluating cardiovascular risk in the chronic kidney disease patient: How do new pieces fit into the uremic puzzle? Clin. J. Am. Soc. Nephrol. 2008, 3, 505–521. [Google Scholar] [CrossRef]
- Hogas, S.M.; Voroneanu, L.; Serban, D.N.; Segall, L.; Hogas, M.M.; Serban, I.L.; Covic, A. Methods and potential biomarkers for the evaluation of endothelial dysfunction in chronic kidney disease: A critical approach. J. Am. Soc. Hypertens. 2010, 4, 116–127. [Google Scholar] [CrossRef]
- Wang, M.C.; Tsai, W.C.; Chen, J.Y.; Huang, J.J. Stepwise increase in arterial stiffness corresponding with the stages of chronic kidney disease. Am. J. Kidney Dis. 2005, 45, 494–501. [Google Scholar] [CrossRef]
- Recio-Mayoral, A.; Banerjee, D.; Streather, C.; Kaski, J.C. Endothelial dysfunction, inflammation and atherosclerosis in chronic kidney disease—A cross-sectional study of predialysis, dialysis and kidney-transplantation patients. Atherosclerosis 2011, 216, 446–451. [Google Scholar] [CrossRef]
- Pedroso, S.; Martins, L.; Fonseca, I.; Dias, L.; Henriques, A.C.; Sarmento, A.M.; Cabrita, A. Impact of hepatitis C virus on renal transplantation: Association with poor survival. Transplant. Proc. 2006, 38, 1890–1894. [Google Scholar] [CrossRef] [PubMed]
- Oyake, N.; Shimada, T.; Murakami, Y.; Ishibashi, Y.; Satoh, H.; Suzuki, K.; Matsumory, A.; Oda, T. Hepatitis C virus infection as a risk factor for increased aortic stiffness and cardiovascular events in dialysis patients. J. Nephrol. 2008, 21, 345–353. [Google Scholar] [PubMed]
- Barone, M.; Viggiani, M.T.; Amoruso, A.; Schiraldi, S.; Zito, A.; Devito, F.; Cortese, F.; Gesualdo, M.; Brunetti, N.; Di Leo, A.; et al. Endothelial dysfunction correlates with liver fibrosis in chronic HCV infection. Gastroenterol. Res. Pract. 2015, 2015, 682174. [Google Scholar] [CrossRef] [PubMed]
- Osztovits, J.; Horváth, T.; Abonyi, M.; Tóth, T.; Visnyei, Z.; Bekö, G.; Csák, T.; Lakatos, P.L.; Littvay, L.; Fehér, J.; et al. Chronic hepatits C virus infection associated with autonomic dysfunction. Liver Int. 2009, 29, 1473–1478. [Google Scholar] [CrossRef] [PubMed]
- Musialik, J.; Kolonko, A.; Kwiecień, K.; Owczarek, A.J.; Więcek, A. Effectiveness and safety of sofosbuvir-based therapy against hepatitis C infection after successful kidney transplantation. Transpl. Infect. Dis. 2019, 21, e13090. [Google Scholar] [CrossRef] [PubMed]
- Babbs, C.F. The origin of Korotkoff sounds and the accuracy of auscultatory blood pressure measurements. J. Am. Soc. Hypertens. 2015, 9, 935–950. [Google Scholar] [CrossRef] [PubMed]
- Padwal, R.; Jalali, A.; McLean, D.; Anwar, S.; Smith, K.; Raggi, P.; Ringrose, J.S. Accuracy of oscillometric blood pressure algorithms in healthy adults and in adults with cardiovascular risk factors. Blood Press. Monit. 2019, 24, 33–37. [Google Scholar] [CrossRef]
- Lang, R.M.; Bierig, M.; Devereux, R.B.; Flaschkampf, F.A.; Foster, E.; Pellikka, P.A.; Picard, M.H.; Roman, M.J.; Seward, J.; Shanewise, J.S.; et al. Recommendations for Chamber Quantification: A report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing group. J. Am. Soc. Echocardiogr. 2005, 18, 1440–1463. [Google Scholar] [CrossRef]
- Devereux, R.B.; Reichek, N. Echocardiographic determination of left ventricular mass in man. Anatomic validation of the method. Circulation 1977, 55, 613–618. [Google Scholar] [CrossRef]
- Thijssen, D.H.J.; Bruno, R.M.; van Mil, A.C.C.M.; Holder, S.M.; Faita, F.; Greyling, A.; Zock, P.L.; Taddei, S.; Deanfield, J.E.; Luscher, T.; et al. Expert consensus and evidence-based recommendations for the assessment of flow-mediated dilation in humans. Eur. Heart J. 2019, 40, 2534–2547. [Google Scholar] [CrossRef]
- Jun, B.G.; Park, W.Y.; Park, E.J.; Jang, J.Y.; Jeong, S.W.; Lee, S.H.; Kim, S.G.; Cha, S.W.; Kim, Y.S.; Cho, Y.D.; et al. A prospective comparative assessment of the accuracy of the FibroScan in evaluating liver steatosis. PLoS ONE 2017, 12, e01827784. [Google Scholar] [CrossRef] [PubMed]
- Sandrin, L.; Fourquet, B.; Hasquenoph, J.M.; Yon, S.; Fournier, C.; Mal, F.; Christidis, C.; Ziol, M.; Poulet, B.; Kazemi, F.; et al. Transient elastography: A new noninvasive method for assessment of hepatic fibrosis. Ultrasound Med. Biol. 2003, 29, 1705–1713. [Google Scholar] [CrossRef] [PubMed]
- Chou, C.-H.; Ho, C.-S.; Tsai, W.-C.; Wang, M.-C.; Tsai, Y.-S.; Chen, J.-Y. Effects of chronic hepatitis C infection on arterial stiffness. J. Am. Soc. Hypertens. 2017, 11, 716–723. [Google Scholar] [CrossRef] [PubMed]
- Vasunta, R.-L.; Kesaniemi, Y.A.; Ylitalo, A.S.; Ukkola, O.H. High ambulatory blood pressure values associated with non-alcoholic fatty liver in middle-aged adults. J. Hypert. 2012, 30, 2015–2019. [Google Scholar] [CrossRef] [PubMed]
- Cheng, P.-N.; Chen, J.-Y.; Chiu, Y.-C.; Chiu, H.-C.; Tsai, L.-M. Augmenting central arterial stiffness following eradication of HCV by direct acting antivirals in advanced fibrosis patients. Sci. Rep. 2019, 9, 1426. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, F.P.; Zimmermann, T.; Wenz, T.; Schnorbus, B.; Ostad, M.A.; Feist, C.; Grambihler, A.; Schattenberg, J.M.; Sprinzl, M.F.; Münzel, T.; et al. Interferon- and ribavirin-free therapy with new direct acting antivirals (DAA) for chronic hepatitis C improves vascular endothelial function. Int. J. Cardiol. 2018, 271, 296–300. [Google Scholar] [CrossRef]
- Davis, J.S.; Young, M.; Lennox, S.; Jones, T.; Piera, K.; Pickles, R.; Oakley, S. The effect of curing hepatitis C with direct-acting antiviral treatment on endothelial function. Antivir. Ther. 2018, 23, 687–694. [Google Scholar] [CrossRef]
- Akoglu, H.; Seringec, N.; Yildirim, T.; Yilmaz, R.; Okutucu, S.; Turkmen, E.; Evranos, B.; Kaya, E.B.; Dikmenoglu, N.; Arici, M.; et al. Relationship between hemorheology and endothelial dysfunction in renal transplant patients receiving calcineurin inhibitors. J. Nephrol. 2013, 26, 931–940. [Google Scholar] [CrossRef]
- Kwak, M.S.; Chung, G.E.; Yang, J.I.; Yim, J.Y.; Chung, S.J.; Jung, S.Y.; Kim, J.S. Clinical implications of controlled attenuation parameter in a health check-up cohort. Liver Int. 2017, 38, 915–923. [Google Scholar] [CrossRef]
- Ramalho, F. Hepatitis C virus infection and liver steatosis. Antivir. Res. 2003, 60, 125–127. [Google Scholar] [CrossRef]
- Sapmaz, F.; Uzman, M.; Basyigit, S.; Ozkan, S.; Yavuz, B.; Yeniova, A.; Kefeli, A.; Asilturk, Z.; Nazligül, Y. Steatosis grade is the most important risk factor for development of endothelial dysfunction in NAFLD. Medicine 2016, 95, e3280. [Google Scholar] [CrossRef] [PubMed]
- Pacifico, L.; Anania, C.; Martino, F.; Cantisani, V.; Pascone, R.; Marcantonio, A.; Chiesa, C. Functional and morphological vascular changes in pediatric nonalcoholic fatty liver disease. Hepatology 2010, 52, 1643–1651. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zeng, Y.; Lin, C.; Chen, Z. Hypertension and non-alcoholic fatty liver disease proven by transient elastography. Hepatol. Res. 2016, 46, 1304–1310. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Pan, Q.; Wu, G.; Qian, L.; Zhang, J.; Zhang, L.; Fang, Q.; Zang, G.; Wang, Y.; Lau, G.; et al. Diverse changes of circulating fibroblast growth factor 21 levels in hepatitis B virus-related diseases. Sci. Rep. 2017, 7, 16482. [Google Scholar] [CrossRef] [PubMed]
- Iwasa, M.; Mifuji-Moroka, R.; Kobayashi, Y.; Takei, Y.; D’Alessandro-Gabazza, C.; Gabazza, E.C. Comment on serum FGF21 and RBP4 levels in patients with chronic hepatits C. Scand. J. Gastroent. 2012, 48, 252–253. [Google Scholar] [CrossRef] [PubMed]
- Tada, T.; Kumada, T.; Toyoda, H.; Sone, Y.; Takeshima, K.; Ogawa, S.; Goto, T.; Wakahata, A.; Nakashima, M.; Nakamuta, M.; et al. Viral eradication reduces both liver stiffness and steatosis in patients with chronic hepatitis C virus infection who received direct-acting anti-viral therapy. Aliment. Pharmacol. Ther. 2018, 7, 1012–1022. [Google Scholar] [CrossRef]
- Kobayashi, N.; Iijima, H.; Tada, T.; Kumada, T.; Yoshida, M.; Aoki, T.; Nishimura, T.; Nakano, C.; Takata, R.; Yoh, K.; et al. Changes in liver stiffness and steatosis among patients with hepatitis C virus infection who received direct-acting antiviral therapy and achieved sustained virological response. Eur. J. Gastroenterol. Hepatol. 2018, 5, 546–551. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| OBP Control Improvement n = 14 | No OBP Control Improvement n = 14 | p | |
|---|---|---|---|
| Age at the start of DAA therapy (years, means and 95%CI) | 49.8 (42.8–56.8) | 48.5 (42.2–54.9) | 0.78 |
| Sex (M/F) | 8/6 | 11/3 | 0.23 |
| Baseline BMI (kg/m2, means and 95%CI) | 24.9 (22.8–26.9) | 24.0 (22.3–25.7) | 0.48 |
| Follow-up BMI (kg/m2, means and 95%CI) | 25.6 (23.5–27.6) ## | 24.4 (22.6–26.3) | 0.40 |
| Baseline eGFR (mL/min/1.73 m2, means and 95%CI) | 58.1 (45.1–71.2) | 54.2 (36.3–72.1) | 0.51 |
| Follow-up eGFR (mL/min/1.73 m2, means and 95%CI) | 54.6 (39.4–69.8) | 51.7 (35.0–68.5) | 0.51 |
| Diabetes (n (%)) | 4 (28.6) | 4 (28.6) | 1.0 |
| Duration of HCV infection (years, means and 95%CI) | 11.0 (6.9–15.1) | 16.4 (12.6–20.1) | <0.05 |
| Dialysis vintage (months, median and IQR) | 30 (18–59) | 42 (20–83) | 0.37 |
| Time after KTx (months, means and 95%CI) | 121 (56–186) | 125 (80–169) | 0.92 |
| Calcineurin inhibitor (CyA/Tc) (n) | 8/6 | 7/7 | 0.70 |
| Baseline HCV viremia (IU/mL, median and IQR) | 340,258 (29,882–1,149,502) | 78,631 (14,847–330,000) | 0.40 |
| OBP Control Improvement (n = 14) | p | No OBP Control Improvement (n = 14) | p | |||||
|---|---|---|---|---|---|---|---|---|
| Baseline | Follow-up | Δ | Baseline | Follow-up | Δ | |||
| SBP (mmHg, mean and 95% CI) | 145.5 (138.3–152.7) | 125.1 (116.3–133.8) | −20.4 (−26.2–−14.6) | <0.001 | 135.6 (130.4–140.1) | 130.4 (125.1–135.6) | −5.2 (−9.7–−0.8) | <0.05 |
| DBP (mmHg, mean and 95% CI) | 84.3 (78.8–89.8) | 71.8 (67.0–76.6) | −12.5 (−16.5–−8.5) | <0.01 | 86.9 (83.6–90.1) | 82.2 (79.3–85.1) | −4.6 (−9.6–0.3) | 0.07 |
| PP (mmHg, mean and 95% CI) | 61.2 (52.7–69.7) | 53.3 (43.2–63.3) | −7.9 (−14.1–−1.8) | <0.05 | 48.7 (43.8–53.6) | 48.1 (42.1–54.2) | −0.6 (−5.3 – 4.2) | 0.86 |
| Number of antihypertensive drugs (mean and 95% CI) | 2.5 (1.3–3.7) | 1.9 (0.8–2.9) | −0.6 (−1.0- −0.3) | <0.05 | 1.9 (1.4–2.5) | 2.2 (1.5–3.0) | 0.3 (0.0–0.6) | <0.07 |
| OBP Control Improvement (n = 14) | p | No OBP Control Improvement (n = 14) | p | |||||
|---|---|---|---|---|---|---|---|---|
| Baseline | Follow-up | Δ | Baseline | Follow-up | Δ | |||
| Central blood pressure measurement | ||||||||
| AoSys (mmHg, mean and 95%CI) | 136 (124–148) | 114 (104–124) | −21.8 (−30.1–−13.5) | <0.01 | 131 (121–141) | 120 (114–127) | −10.6 (−19.4–−1.9) | 0.06 |
| AoDia (mmHg, mean and 95%CI) | 89 (81–96) | 77 71–83) | −11.6 (−19.2–−4.1) | <0.05 | 87 (81–92) | 82 (76–87) | −5.0 (−12.8–−2.8) | 0.19 |
| AoPP (mmHg, mean and 95%CI) | 47 (38–57) | 37 (29–46) | −10.1 (−14.1–−6.2) | 0.09 | 44 (37–51) | 39 (33–44) | −5.6 (−12.3–1.1) | 0.19 |
| AIx@75 (%, median and IQR) | 20.5 (8.6–25.1) | 16.9 (2.0–20.2) | −4.4 (−13.4–−1.1) | <0.05 | 15.5 (10.6–21.1) | 16.5 (8.2–21.8) | 0.0 (−8.2–7.8) | 0.85 |
| Arterial wall assessments | ||||||||
| PWV (m/s, mean and 95%CI) | 8.5 (7.4–9.7) | 8.7 (7.5–9.8) | 0.1 (−0.7–0.9) | 0.65 | 8.3 (7.1–9.5) | 8.0 (6.9–9.2) | −0.3 (−1.4–0.8) | 0.55 |
| FMD (%,median and IQR) | 9.2 (8.1–12.5) | 9.3 (4.9–17.9) | 2.1 (−6.5–3.3) | 0.88 | 9.9 (7.5–15.0) | 9.6 (5.6–12.2) | −1.6 (−2.8–0.6) | 0.36 |
| NMD (%,mean and 95%CI) | 12.9 (10.3–15.6) | 11.1 (8.4–13.8) | −1.8 (−5.5–1.8) | 0.30 | 11.8 (9.9–13.7) | 6.3 (3.7–8.9) | −5.5 (−9.1–−2.0) | <0.001 |
| NMD with double dose (%,mean and 95%CI) | 12.9 (10.3–15.6) | 13.4 (10.3–16.6) | 0.5 (−2.2–3.2) | 0.80 | 11.8 (9.9–13.7) | 10.5 (5.7–15.3) | −1.3 (−6.0–3.5) | 0.59 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kolonko, A.; Musialik, J.; Chudek, J.; Bartmańska, M.; Słabiak-Błaż, N.; Kujawa-Szewieczek, A.; Kuczera, P.; Kwiecień-Furmańczuk, K.; Więcek, A. Changes in Office Blood Pressure Control, Augmentation Index, and Liver Steatosis in Kidney Transplant Patients after Successful Hepatitis C Infection Treatment with Direct Antiviral Agents. J. Clin. Med. 2020, 9, 948. https://doi.org/10.3390/jcm9040948
Kolonko A, Musialik J, Chudek J, Bartmańska M, Słabiak-Błaż N, Kujawa-Szewieczek A, Kuczera P, Kwiecień-Furmańczuk K, Więcek A. Changes in Office Blood Pressure Control, Augmentation Index, and Liver Steatosis in Kidney Transplant Patients after Successful Hepatitis C Infection Treatment with Direct Antiviral Agents. Journal of Clinical Medicine. 2020; 9(4):948. https://doi.org/10.3390/jcm9040948
Chicago/Turabian StyleKolonko, Aureliusz, Joanna Musialik, Jerzy Chudek, Magdalena Bartmańska, Natalia Słabiak-Błaż, Agata Kujawa-Szewieczek, Piotr Kuczera, Katarzyna Kwiecień-Furmańczuk, and Andrzej Więcek. 2020. "Changes in Office Blood Pressure Control, Augmentation Index, and Liver Steatosis in Kidney Transplant Patients after Successful Hepatitis C Infection Treatment with Direct Antiviral Agents" Journal of Clinical Medicine 9, no. 4: 948. https://doi.org/10.3390/jcm9040948
APA StyleKolonko, A., Musialik, J., Chudek, J., Bartmańska, M., Słabiak-Błaż, N., Kujawa-Szewieczek, A., Kuczera, P., Kwiecień-Furmańczuk, K., & Więcek, A. (2020). Changes in Office Blood Pressure Control, Augmentation Index, and Liver Steatosis in Kidney Transplant Patients after Successful Hepatitis C Infection Treatment with Direct Antiviral Agents. Journal of Clinical Medicine, 9(4), 948. https://doi.org/10.3390/jcm9040948