Post-Traumatic Sepsis Is Associated with Increased C5a and Decreased TAFI Levels


Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Patients
2.3. Blood Processing and Analysis
2.4. Statistics
3. Results
Main Findings
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Norton, R.; Kobusingye, O. Injuries. N. Engl. J. Med. 2013, 368, 1723–1730. [Google Scholar] [CrossRef]
- Osborn, T.M.; Tracy, J.K.; Dunne, J.R.; Pasquale, M.; Napolitano, L.M. Epidemiology of sepsis in patients with traumatic injury. Crit. Care Med. 2004, 32, 2234–2240. [Google Scholar] [CrossRef]
- Relja, B.; Land, W.G. Damage-associated molecular patterns in trauma. Eur. J. Trauma Emerg. Surg. 2019, 1–25. [Google Scholar] [CrossRef] [Green Version]
- Relja, B.; Mors, K.; Marzi, I. Danger signals in trauma. Eur. J. Trauma Emerg. Surg. 2018, 44, 301–316. [Google Scholar] [CrossRef] [Green Version]
- Nast-Kolb, D.; Aufmkolk, M.; Rucholtz, S.; Obertacke, U.; Waydhas, C. Multiple organ failure still a major cause of morbidity but not mortality in blunt multiple trauma. J. Trauma 2001, 51, 835–841, discussion 41-2. [Google Scholar] [CrossRef]
- Markiewski, M.M.; DeAngelis, R.A.; Lambris, J.D. Complexity of complement activation in sepsis. J. Cell Mol. Med. 2008, 12, 2245–2254. [Google Scholar] [CrossRef]
- Ward, P.A. The harmful role of c5a on innate immunity in sepsis. J. Innate Immun. 2010, 2, 439–445. [Google Scholar] [CrossRef]
- Foley, J.H.; Kim, P.Y.; Mutch, N.J.; Gils, A. Insights into thrombin activatable fibrinolysis inhibitor function and regulation. J. Thromb. Haemost. 2013, 11 (Suppl. 1), 306–315. [Google Scholar]
- Bouma, B.N.; Mosnier, L.O. Thrombin activatable fibrinolysis inhibitor (TAFI) at the interface between coagulation and fibrinolysis. Pathophysiol. Haemost. Thromb. 2003, 33, 375–381. [Google Scholar] [CrossRef]
- Muto, Y.; Suzuki, K.; Iida, H.; Sakakibara, S.; Kato, E.; Itoh, F.; Kakui, N.; Ishii, H. EF6265, a novel inhibitor of activated thrombin-activatable fibrinolysis inhibitor, protects against sepsis-induced organ dysfunction in rats. Crit. Care Med. 2009, 37, 1744–1749. [Google Scholar] [CrossRef]
- Ravindranath, T.M.; Goto, M.; Demir, M.; Tobu, M.; Kujawski, M.F.; Hoppensteadt, D.; Samonte, V.; Iqbal, O.; Sayeed, M.M.; Fareed, J. Tissue factor pathway inhibitor and thrombin activatable fibrinolytic inhibitor plasma levels following burn and septic injuries in rats. Clin. Appl Thromb. Hemost. 2004, 10, 379–385. [Google Scholar] [CrossRef] [Green Version]
- Verbon, A.; Meijers, J.C.; Spek, C.A.; Hack, C.E.; Pribble, J.P.; Turner, T.; Dekkers, P.E.; Axtelle, T.; Levi, M.; van Deventer, S.J.; et al. Effects of IC14, an anti-CD14 antibody, on coagulation and fibrinolysis during low-grade endotoxemia in humans. J. Infect. Dis. 2003, 187, 55–61. [Google Scholar] [CrossRef]
- Watanabe, R.; Wada, H.; Watanabe, Y.; Sakakura, M.; Nakasaki, T.; Mori, Y.; Nishikawa, M.; Gabazza, E.C.; Nobori, T.; Shiku, H. Activity and antigen levels of thrombin-activatable fibrinolysis inhibitor in plasma of patients with disseminated intravascular coagulation. Thromb. Res. 2001, 104, 1–6. [Google Scholar] [CrossRef]
- Relja, B.; Lustenberger, T.; Puttkammer, B.; Jakob, H.; Morser, J.; Gabazza, E.C.; Takei, Y.; Marzi, I. Thrombin-activatable fibrinolysis inhibitor (TAFI) is enhanced in major trauma patients without infectious complications. Immunobiology 2013, 218, 470–476. [Google Scholar] [CrossRef]
- Ricklin, D.; Hajishengallis, G.; Yang, K.; Lambris, J.D. Complement: A key system for immune surveillance and homeostasis. Nat. Immunol. 2010, 11, 785–797. [Google Scholar] [CrossRef] [Green Version]
- Ajona, D.; Ortiz-Espinosa, S.; Pio, R. Complement anaphylatoxins C3a and C5a: Emerging roles in cancer progression and treatment. Semin. Cell Dev. Biol. 2019, 85, 153–163. [Google Scholar] [CrossRef]
- Blatt, A.Z.; Saggu, G.; Kulkarni, K.V.; Cortes, C.; Thurman, J.M.; Ricklin, D.; Lambris, J.D.; Valenzuela, J.G.; Ferreira, V.P. Properdin-Mediated C5a Production Enhances Stable Binding of Platelets to Granulocytes in Human Whole Blood. J. Immunol. 2016, 196, 4671–4680. [Google Scholar] [CrossRef]
- Satyam, A.; Graef, E.R.; Lapchak, P.H.; Tsokos, M.G.; Dalle Lucca, J.J.; Tsokos, G.C. Complement and coagulation cascades in trauma. Acute Med. Surg. 2019, 6, 329–335. [Google Scholar] [CrossRef]
- Guo, R.F.; Ward, P.A. Role of C5a in inflammatory responses. Ann. Rev. Immunol. 2005, 23, 821–852. [Google Scholar] [CrossRef]
- Clarke, A.R.; Christophe, B.R.; Khahera, A.; Sim, J.L.; Connolly, E.S., Jr. Therapeutic Modulation of the Complement Cascade in Stroke. Front. Immunol. 2019, 10, 1723. [Google Scholar] [CrossRef] [Green Version]
- Keshari, R.S.; Silasi, R.; Popescu, N.I.; Patel, M.M.; Chaaban, H.; Lupu, C.; Coggeshall, K.M.; Mollnes, T.E.; DeMarco, S.J.; Lupu, F. Inhibition of complement C5 protects against organ failure and reduces mortality in a baboon model of Escherichia coli sepsis. Proc. Natl. Acad. Sci. USA 2017, 114, E6390–E6399. [Google Scholar] [CrossRef] [Green Version]
- Declerck, P.J. Thrombin activatable fibrinolysis inhibitor. Hamostaseologie 2011, 31, 165–166;168–173. [Google Scholar] [CrossRef] [Green Version]
- Hugenholtz, G.C.; Meijers, J.C.; Adelmeijer, J.; Porte, R.J.; Lisman, T. TAFI deficiency promotes liver damage in murine models of liver failure through defective down-regulation of hepatic inflammation. Thromb. Haemost. 2013, 109, 948–955. [Google Scholar] [CrossRef]
- Eguchi, A.; Franz, N.; Kobayashi, Y.; Iwasa, M.; Wagner, N.; Hildebrand, F.; Takei, Y.; Marzi, I.; Relja, B. Circulating Extracellular Vesicles and Their miR “Barcode” Differentiate Alcohol Drinkers with Liver Injury and Those Without Liver Injury in Severe Trauma Patients. Front. Med. 2019, 6, 30. [Google Scholar] [CrossRef] [Green Version]
- Calandra, T.; Cohen, J. International Sepsis Forum Definition of Infection in the ICUCC. The international sepsis forum consensus conference on definitions of infection in the intensive care unit. Crit. Care Med. 2005, 33, 1538–1548. [Google Scholar] [CrossRef]
- Shankar-Hari, M.; Phillips, G.S.; Levy, M.L.; Seymour, C.W.; Liu, V.X.; Deutschman, C.S.; Angus, D.C.; Rubenfeld, G.D.; Singer, M.; Sepsis Definitions Task, F. Developing a New Definition and Assessing New Clinical Criteria for Septic Shock: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 775–787. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Levi, M.; Nieuwdorp, M.; van der Poll, T.; Stroes, E. Metabolic modulation of inflammation-induced activation of coagulation. Semin. Thromb. Hemost. 2008, 34, 26–32. [Google Scholar] [CrossRef]
- Okamoto, T.; Tanigami, H.; Suzuki, K.; Shimaoka, M. Thrombomodulin: A bifunctional modulator of inflammation and coagulation in sepsis. Crit. Care Res. Pract. 2012, 2012, 614545. [Google Scholar] [CrossRef] [Green Version]
- Myles, T.; Nishimura, T.; Yun, T.H.; Nagashima, M.; Morser, J.; Patterson, A.J.; Pearl, R.G.; Leung, L.L. Thrombin activatable fibrinolysis inhibitor, a potential regulator of vascular inflammation. J. Biol. Chem. 2003, 278, 51059–51067. [Google Scholar] [CrossRef] [Green Version]
- Chakraborty, S.; Karasu, E.; Huber-Lang, M. Complement After Trauma: Suturing Innate and Adaptive Immunity. Front. Immunol. 2018, 9, 2050. [Google Scholar] [CrossRef] [PubMed]
- Burk, A.M.; Martin, M.; Flierl, M.A.; Rittirsch, D.; Helm, M.; Lampl, L.; Bruckner, U.; Stahl, G.L.; Blom, A.M.; Perl, M.; et al. Early complementopathy after multiple injuries in humans. Shock 2012, 37, 348–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeerleder, S.; Schroeder, V.; Hack, C.E.; Kohler, H.P.; Wuillemin, W.A. TAFI and PAI-1 levels in human sepsis. Thromb. Res. 2006, 118, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Lustenberger, T.; Relja, B.; Puttkammer, B.; Gabazza, E.C.; Geiger, E.; Takei, Y.; Morser, J.; Marzi, I. Activated thrombin-activatable fibrinolysis inhibitor (TAFIa) levels are decreased in patients with trauma-induced coagulopathy. Thromb. Res. 2013, 131, e26–e30. [Google Scholar] [CrossRef]
- Naito, M.; Taguchi, O.; Kobayashi, T.; Takagi, T.; D’Alessandro-Gabazza, C.N.; Matsushima, Y.; Boveda-Ruiz, D.; Gil-Bernabe, P.; Matsumoto, T.; Chelakkot-Govindalayathil, A.L.; et al. Thrombin-activatable fibrinolysis inhibitor protects against acute lung injury by inhibiting the complement system. Am. J. Respir. Cell Mol. Biol. 2013, 49, 646–653. [Google Scholar] [CrossRef] [Green Version]
- Nishimura, T.; Myles, T.; Piliponsky, A.M.; Kao, P.N.; Berry, G.J.; Leung, L.L. Thrombin-activatable procarboxypeptidase B regulates activated complement C5a in vivo. Blood 2007, 109, 1992–1997. [Google Scholar] [CrossRef] [Green Version]
- Fujiwara, A.; Taguchi, O.; Takagi, T.; D’Alessandro-Gabazza, C.N.; Boveda-Ruiz, D.; Toda, M.; Yasukawa, A.; Matsushima, Y.; Miyake, Y.; Kobayashi, H.; et al. Role of thrombin-activatable fibrinolysis inhibitor in allergic bronchial asthma. Lung 2012, 190, 189–198. [Google Scholar] [CrossRef]
- Song, J.J.; Hwang, I.; Cho, K.H.; Garcia, M.A.; Kim, A.J.; Wang, T.H.; Lindstrom, T.M.; Lee, A.T.; Nishimura, T.; Zhao, L.; et al. Plasma carboxypeptidase B downregulates inflammatory responses in autoimmune arthritis. J. Clin. Investig. 2011, 121, 3517–3527. [Google Scholar] [CrossRef]
- Mook-Kanamori, B.B.; Valls Seron, M.; Geldhoff, M.; Havik, S.R.; van der Ende, A.; Baas, F.; van der Poll, T.; Meijers, J.C.; Morgan, B.P.; Brouwer, M.C.; et al. Thrombin-activatable fibrinolysis inhibitor influences disease severity in humans and mice with pneumococcal meningitis. J. Thromb. Haemost. 2015, 13, 2076–2086. [Google Scholar] [CrossRef] [Green Version]
- Jackson, S.P.; Darbousset, R.; Schoenwaelder, S.M. Thromboinflammation: Challenges of therapeutically targeting coagulation and other host defense mechanisms. Blood 2019, 133, 906–918. [Google Scholar] [CrossRef] [Green Version]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017, 43, 304–377. [Google Scholar] [CrossRef] [PubMed]
- Bernard, G.R.; Vincent, J.L.; Laterre, P.F.; LaRosa, S.P.; Dhainaut, J.F.; Lopez-Rodriguez, A.; Steingrub, J.S.; Garber, G.E.; Helterbrand, J.D.; Ely, E.W.; et al. Efficacy and safety of recombinant human activated protein C for severe sepsis. N. Engl. J. Med. 2001, 344, 699–709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vincent, J.L.; Ramesh, M.K.; Ernest, D.; LaRosa, S.P.; Pachl, J.; Aikawa, N.; Hoste, E.; Levy, H.; Hirman, J.; Levi, M.; et al. A randomized, double-blind, placebo-controlled, Phase 2b study to evaluate the safety and efficacy of recombinant human soluble thrombomodulin, ART-123, in patients with sepsis and suspected disseminated intravascular coagulation. Crit. Care Med. 2013, 41, 2069–2079. [Google Scholar] [CrossRef] [PubMed]
- Sadjadi, J.; Cureton, E.L.; Twomey, P.; Victorino, G.P. Transfusion, not just injury severity, leads to posttrauma infection: A matched cohort study. Am. Surg. 2009, 75, 307–312. [Google Scholar] [PubMed]
- Claridge, J.A.; Sawyer, R.G.; Schulman, A.M.; McLemore, E.C.; Young, J.S. Blood transfusions correlate with infections in trauma patients in a dose-dependent manner. Am. Surg. 2002, 68, 566–572. [Google Scholar] [PubMed]
- Taylor, R.W.; O’Brien, J.; Trottier, S.J.; Manganaro, L.; Cytron, M.; Lesko, M.F.; Arnzen, K.; Cappadoro, C.; Fu, M.; Plisco, M.S.; et al. Red blood cell transfusions and nosocomial infections in critically ill patients. Crit. Care Med. 2006, 34, 2302–2308, quiz 9. [Google Scholar] [CrossRef]
- Patel, S.V.; Kidane, B.; Klingel, M.; Parry, N. Risks associated with red blood cell transfusion in the trauma population, a meta-analysis. Injury 2014, 45, 1522–1533. [Google Scholar] [CrossRef]
- Jongerius, I.; Porcelijn, L.; van Beek, A.E.; Semple, J.W.; van der Schoot, C.E.; Vlaar, A.P.J.; Kapur, R. The Role of Complement in Transfusion-Related Acute Lung Injury. Trans. Med. Rev. 2019, 33, 236–242. [Google Scholar] [CrossRef]
- Semple, J.W.; Rebetz, J.; Kapur, R. Transfusion-associated circulatory overload and transfusion-related acute lung injury. Blood 2019, 133, 1840–1853. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subjects and Trauma Characteristics | Total (n = 48) | No Sepsis a (n = 34) | Sepsis b (n = 14) | p < 0.05 a vs. b |
|---|---|---|---|---|
| age (years), mean ± sem | 52.23 ± 2.74 | 48.45 ± 3.74 | 56,54 ± 3.68 | ns |
| gender (male, %) | 33 (68.75%) | 22 (64.71%) | 11 (78.57%) | ns |
| trauma mechanism (falls) | 23 (47.92%) | 16 (47.06%) | 7 (50.00%) | ns |
| ISS | 24.95 ± 1.75 | 25.78 ± 2.36 | 23.46 ± 2.79 | ns |
| AIS ≥ 3 (n, %) | ||||
| Head | 22 (45.83%) | 16 (47.06%) | 6 (42.86%) | ns |
| Chest | 16 (33.33%) | 11 (32.35%) | 5 (35.71%) | ns |
| Abdomen | 7 (14.58%) | 4 (11.76%) | 3 (21.43%) | ns |
| Extremity | 10 (20.83%) | 7 (20.59%) | 3 (21.43%) | ns |
| Physiologic Characteristics | Total (n = 48) | No Sepsis a (n = 34) | Sepsis b (n = 14) | p < 0.05 a vs. b |
|---|---|---|---|---|
| SBP < 90 mm Hg (ED, n, %) | 5 (10.42%) | 2 (5.71%) | 3 (21.43%) | ns |
| PRBC transfusion within 24 h (Units) | 4.84 ± 1.18 | 3.81 ± 1.53 | 7.14 ± 2.01 | ns |
| PRBC transfusion total (Units) | 6.98 ± 1.41 | 5.46 ± 21.74 | 10.50 ± 2.50 | <0.05 |
| FFP transfusion within 24 h (Units) | 2.54 ± 0.69 | 1.65 ± 0.71 | 4.31 ± 1.45 | ns |
| FFP transfusion total (Units) | 2.68 ± 0.75 | 1.73 ± 0.75 | 4.43 ± 1.56 | ns |
| INR (ED) | 1.34 ± 0.08 | 1.36 ± 0.11 | 1.31 ± 0.06 | ns |
| PTT (ED, s) | 36.13 ± 2.79 | 37.12 ± 3.88 | 33.72 ± 1.62 | ns |
| PLT count (ED, × 103/μL) | 201.40 ± 10.34 | 198.00 ± 12.44 | 210.30 ± 18.97 | ns |
| Outcome | Total (n = 48) | No Sepsis a (n = 34) | Sepsis b (n = 14) | p < 0.05 a vs. b |
|---|---|---|---|---|
| ICU stay (days) | 11.71 ± 1.82 | 7.00 ± 1.16 | 22.14 ± 4.12 | <0.0001 |
| in-hospital stay (days) | 25.67 ± 3.13 | 19.00 ± 2.90 | 41.07 ± 6.43 | <0.001 |
| in-hospital mortality (n, %) | 6 (12.5%) | 2 (5.88%) | 4 (28.57%) | <0.05 |
| Correlation Analysis | Pearson r | p-Value | Number of Pairs |
|---|---|---|---|
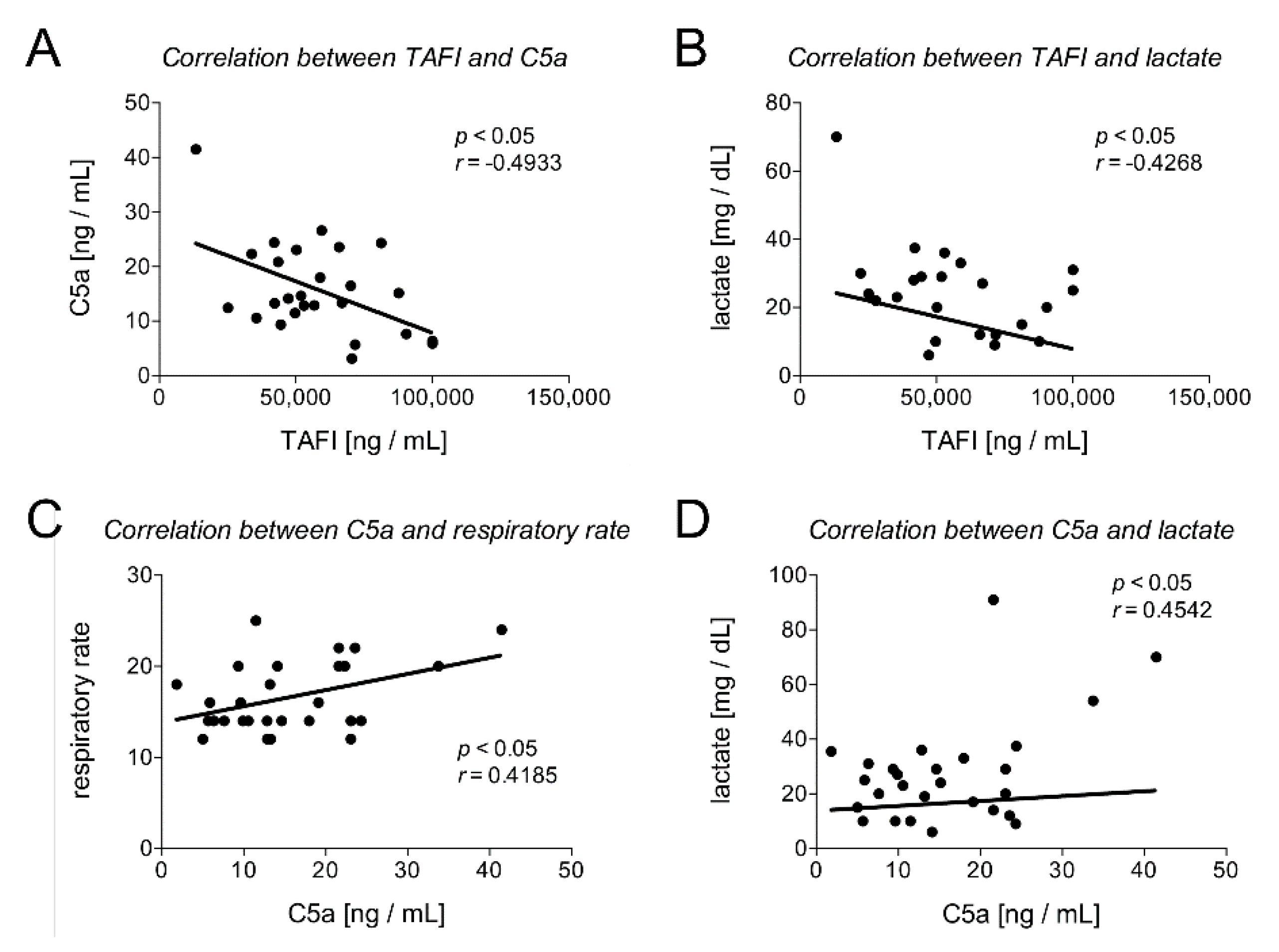
| TAFI and C5a | −0.4933 | 0.0104 | 26 |
| TAFI and leukocytes | −0.2442 | 0.1855 | 31 |
| TAFI and lactate | −0.4268 | 0.0423 | 23 |
| TAFI and pH | 0.2079 | 0.3532 | 22 |
| TAFI and heart rate | −0.2603 | 0.2304 | 23 |
| TAFI and respiratory rate | −0.3685 | 0.0915 | 22 |
| TAFI and SOFA score | −0.3865 | 0.0422 | 28 |
| TAFI and INR | −0.0499 | 0.7860 | 32 |
| TAFI and TPT | 0.0299 | 0.8750 | 30 |
| TAFI and PTT | 0.0369 | 0.8409 | 32 |
| TAFI and PLT | −0.3048 | 0.0085 | 33 |
| C5a and leukocytes | −0.2260 | 0.1918 | 35 |
| C5a and lactate | 0.4542 | 0.0173 | 27 |
| C5a and pH | −0.0805 | 0.6839 | 28 |
| C5a and heart rate | 0.2416 | 0.2068 | 29 |
| C5a and respiratory rate | 0.4185 | 0.0266 | 28 |
| C5a and SOFA score | 0.3795 | 0.0386 | 30 |
| C5a and INR | −0.0199 | 0.9055 | 38 |
| C5a and TPT | −0.2056 | 0.2291 | 36 |
| C5a and PTT | 0.0731 | 0.6629 | 38 |
| C5a and PLT | 0.0138 | 0.9353 | 37 |
| Parameter | Cut-Off Value | Sensitivity % (95% CI) | Specificity % (95% CI) | AUC (95% CI) | p-Value |
|---|---|---|---|---|---|
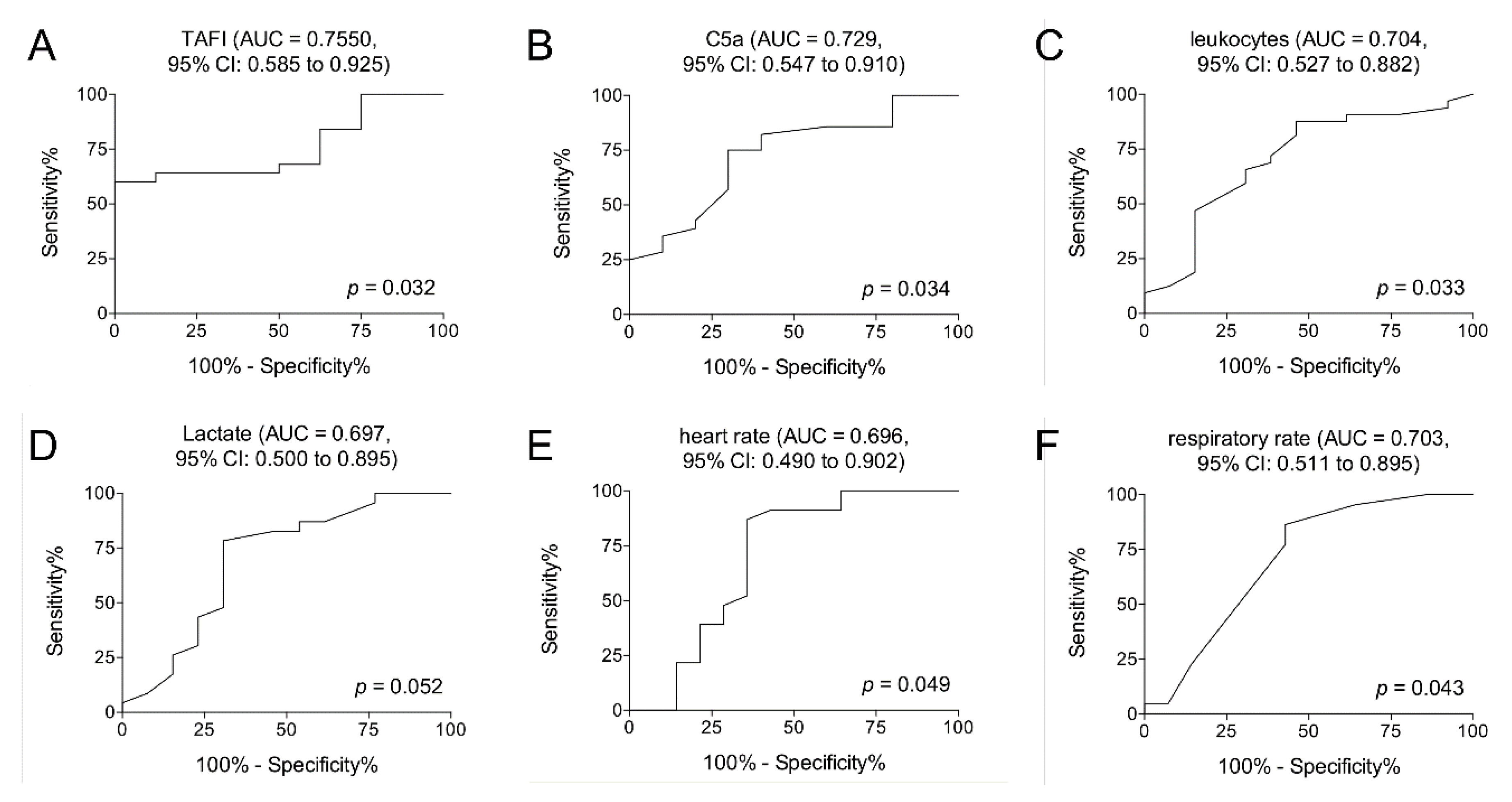
| TAFI [ng/mL] | >54857 | 64.00 (42.52 to 82.03) | 87.50 (47.35 to 99.68) | 0.7550 (0.585 to 0.925) | 0.032 |
| C5a [ng/mL] | <17.00 | 75.00 (55.13 to 89.31) | 70.00 (34.75 to 93.33) | 0.7286 (0.547 to 0.910) | 0.034 |
| leukocytes [U/nL] | <14.50 | 65.63 (46.81 to 81.43) | 69.23 (38.57 to 90.91) | 0.7043 (0.527 to 0.882) | 0.033 |
| lactate [mg/dL] | <28.50 | 78.26 (56.30 to 92.54) | 69.23 (38.57 to 90.91) | 0.6973 (0.500 to 0.895) | 0.052 |
| heart rate | <102.5 | 86.96 (66.41 to 97.22) | 64.29 (35.14 to 87.24) | 0.6957 (0.490 to 0.902) | 0.049 |
| respiratory rate | <15.00 | 63.64 (40.66 to 82.80) | 64.29 (35.14 to 87.24) | 0.7029 (0.511 to 0.895) | 0.043 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vollrath, J.T.; Marzi, I.; Herminghaus, A.; Lustenberger, T.; Relja, B. Post-Traumatic Sepsis Is Associated with Increased C5a and Decreased TAFI Levels. J. Clin. Med. 2020, 9, 1230. https://doi.org/10.3390/jcm9041230
Vollrath JT, Marzi I, Herminghaus A, Lustenberger T, Relja B. Post-Traumatic Sepsis Is Associated with Increased C5a and Decreased TAFI Levels. Journal of Clinical Medicine. 2020; 9(4):1230. https://doi.org/10.3390/jcm9041230
Chicago/Turabian StyleVollrath, Jan Tilmann, Ingo Marzi, Anna Herminghaus, Thomas Lustenberger, and Borna Relja. 2020. "Post-Traumatic Sepsis Is Associated with Increased C5a and Decreased TAFI Levels" Journal of Clinical Medicine 9, no. 4: 1230. https://doi.org/10.3390/jcm9041230
APA StyleVollrath, J. T., Marzi, I., Herminghaus, A., Lustenberger, T., & Relja, B. (2020). Post-Traumatic Sepsis Is Associated with Increased C5a and Decreased TAFI Levels. Journal of Clinical Medicine, 9(4), 1230. https://doi.org/10.3390/jcm9041230