Circulating microRNA Associated to Different Stages of Liver Steatosis in Prader–Willi Syndrome and Non-Syndromic Obesity

 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Serum Collection
2.3. Assessment of Hemolysis
2.4. RNA Extraction
2.5. qRT-PCR
2.6. Data Analysis and Statistical Methods
3. Results
3.1. Patient Characteristics
3.2. Selection of Differently Expressed miRNAs
3.3. Differently Expressed miRNAs between PWS and OB Subjects
3.4. Differently Expressed miRNAs between PWS and OB Subjects According to the Degree of Steatosis
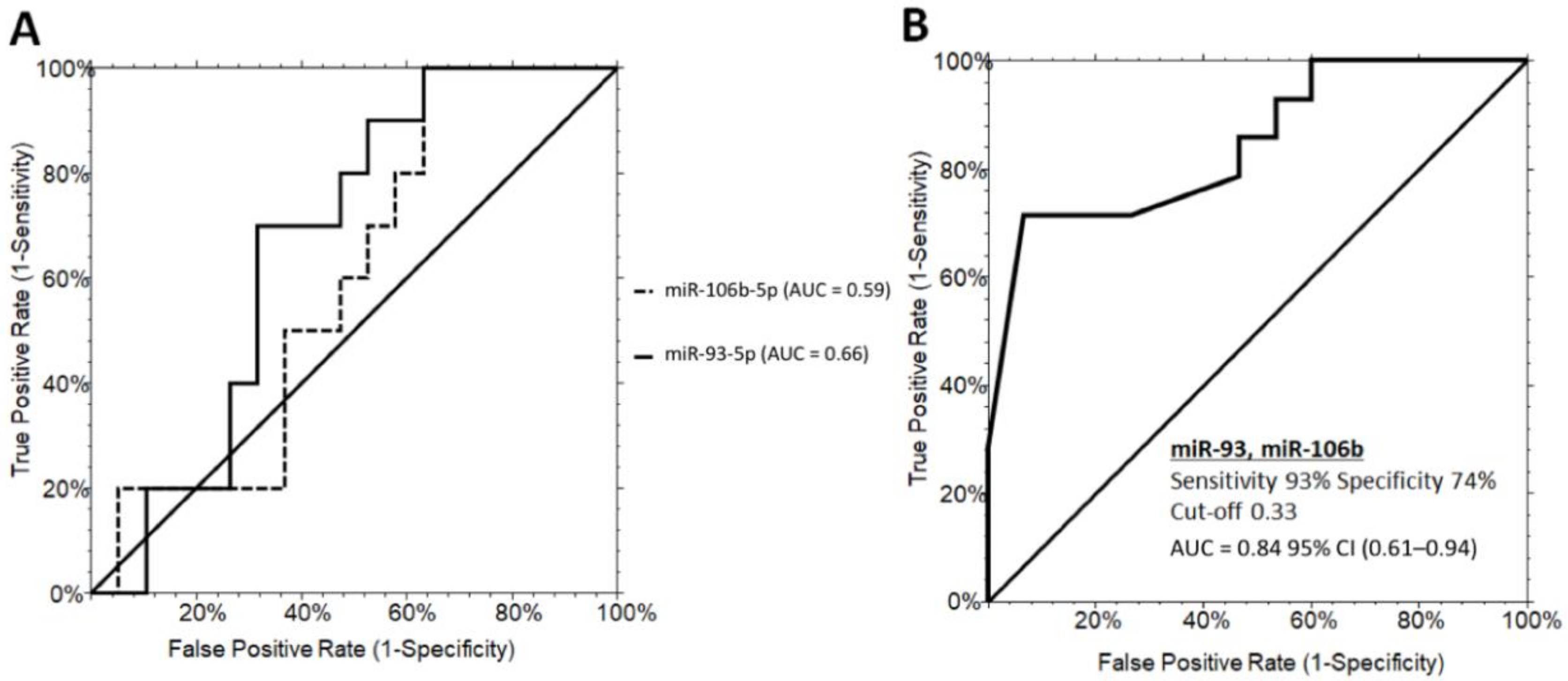
3.5. Differently Expressed miRNAs between Grade1 and Grade 2/3 Steatosis in PWS+ Group
3.6. Differently Expressed miRNAs in Relation to the Genetic Subtypes of PWS
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Butler, M.G.; Manzardo, A.M.; Forster, J.L. Prader-Willi Syndrome: Clinical Genetics and Diagnostic Aspects with Treatment Approaches. Curr. Pediatric Rev. 2016, 12, 136–166. [Google Scholar] [CrossRef] [PubMed]
- Angulo, M.A.; Butler, M.G.; Cataletto, M.E. Prader-Willi syndrome: A review of clinical, genetic, and endocrine findings. J. Endocrinol. Investig. 2015, 38, 1249–1263. [Google Scholar] [CrossRef] [PubMed]
- Grugni, G. Growth hormone in health and disease: Prader-Willi syndrome—GH therapy and bone. Nat. Rev. Endocrinol. 2013, 9, 320–321. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Choi, J.-H. Pathophysiology and clinical characteristics of hypothalamic obesity in children and adolescents. Ann. Pediatric Endocrinol. Metab. 2013, 18, 161–167. [Google Scholar] [CrossRef]
- Crinò, A.; Fintini, D.; Bocchini, S.; Grugni, G. Obesity management in Prader-Willi syndrome: Current perspectives. Diabetes Metab. Syndr. Obes. 2018, 11, 579–593. [Google Scholar] [CrossRef]
- Theodoro, M.F.; Talebizadeh, Z.; Butler, M.G. Body composition and fatness patterns in Prader-Willi syndrome: Comparison with simple obesity. Obesity (Silver Spring) 2006, 14, 1685–1690. [Google Scholar] [CrossRef]
- Reus, L.; Zwarts, M.; van Vlimmeren, L.A.; Willemsen, M.A.; Otten, B.J.; Nijhuis-van der Sanden, M.W.G. Motor problems in Prader-Willi syndrome: A systematic review on body composition and neuromuscular functioning. Neurosci. Biobehav. Rev. 2011, 35, 956–969. [Google Scholar] [CrossRef]
- Goldstone, A.P.; Thomas, E.L.; Brynes, A.E.; Bell, J.D.; Frost, G.; Saeed, N.; Hajnal, J.V.; Howard, J.K.; Holland, A.; Bloom, S.R. Visceral adipose tissue and metabolic complications of obesity are reduced in Prader-Willi syndrome female adults: Evidence for novel influences on body fat distribution. J. Clin. Endocrinol. Metab. 2001, 86, 4330–4338. [Google Scholar] [CrossRef]
- Bedogni, G.; Grugni, G.; Tringali, G.; Marazzi, N.; Sartorio, A. Does segmental body composition differ in women with Prader-Willi syndrome compared to women with essential obesity? J. Endocrinol. Investig. 2015, 38, 957–961. [Google Scholar] [CrossRef]
- Talebizadeh, Z.; Butler, M.G. Insulin resistance and obesity-related factors in Prader-Willi syndrome: Comparison with obese subjects. Clin. Genet. 2005, 67, 230–239. [Google Scholar] [CrossRef]
- Fintini, D.; Grugni, G.; Bocchini, S.; Brufani, C.; Di Candia, S.; Corrias, A.; Delvecchio, M.; Salvatoni, A.; Ragusa, L.; Greggio, N.; et al. Disorders of glucose metabolism in Prader-Willi syndrome: Results of a multicenter Italian cohort study. Nutr. Metab. Cardiovasc. Dis. 2016, 26, 842–847. [Google Scholar] [CrossRef] [PubMed]
- Grugni, G.; Crinò, A.; Bedogni, G.; Cappa, M.; Sartorio, A.; Corrias, A.; Di Candia, S.; Gargantini, L.; Iughetti, L.; Pagano, C.; et al. Metabolic syndrome in adult patients with Prader-Willi syndrome. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 1134–1140. [Google Scholar] [CrossRef] [PubMed]
- Fintini, D.; Inzaghi, E.; Colajacomo, M.; Bocchini, S.; Grugni, G.; Brufani, C.; Cappa, M.; Nobili, V.; Cianfarani, S.; Crinò, A. Non-Alcoholic Fatty Liver Disease (NAFLD) in children and adolescents with Prader-Willi Syndrome (PWS). Pediatric Obes. 2016, 11, 235–238. [Google Scholar] [CrossRef] [PubMed]
- Bedogni, G.; Grugni, G.; Nobili, V.; Agosti, F.; Saezza, A.; Sartorio, A. Is non-alcoholic fatty liver disease less frequent among women with Prader-Willi syndrome? Obes. Facts 2014, 7, 71–76. [Google Scholar] [CrossRef]
- D’Angelo, C.S.; Varela, M.C.; de Castro, C.I.E.; Otto, P.A.; Perez, A.B.A.; Lourenço, C.M.; Kim, C.A.; Bertola, D.R.; Kok, F.; Garcia-Alonso, L.; et al. Chromosomal microarray analysis in the genetic evaluation of 279 patients with syndromic obesity. Mol. Cytogenet. 2018, 11, 14. [Google Scholar] [CrossRef]
- Bittel, D.C.; Kibiryeva, N.; Sell, S.M.; Strong, T.V.; Butler, M.G. Whole Genome Microarray Analysis of Gene Expression in Prader–Willi Syndrome. Am. J. Med. Genet. A 2007, 143A, 430–442. [Google Scholar] [CrossRef]
- Pascut, D.; Tamini, S.; Bresolin, S.; Giraudi, P.; Basso, G.; Minocci, A.; Tiribelli, C.; Grugni, G.; Sartorio, A. Differences in circulating microRNA signature in Prader-Willi syndrome and non-syndromic obesity. Endocr. Connect. 2018, 7, 1262–1274. [Google Scholar] [CrossRef]
- Saadeh, S.; Younossi, Z.M.; Remer, E.M.; Gramlich, T.; Ong, J.P.; Hurley, M.; Mullen, K.D.; Cooper, J.N.; Sheridan, M.J. The utility of radiological imaging in nonalcoholic fatty liver disease. Gastroenterology 2002, 123, 745–750. [Google Scholar] [CrossRef]
- Palmentieri, B.; de Sio, I.; La Mura, V.; Masarone, M.; Vecchione, R.; Bruno, S.; Torella, R.; Persico, M. The role of bright liver echo pattern on ultrasound B-mode examination in the diagnosis of liver steatosis. Dig. Liver Dis. 2006, 38, 485–489. [Google Scholar] [CrossRef]
- Cassidy, S.B.; Schwartz, S.; Miller, J.L.; Driscoll, D.J. Prader-Willi syndrome. Genet. Med. 2012, 14, 10–26. [Google Scholar] [CrossRef]
- Harboe, M. A method for determination of hemoglobin in plasma by near-ultraviolet spectrophotometry. Scand. J. Clin. Lab. Investig. 1959, 11, 66–70. [Google Scholar] [CrossRef] [PubMed]
- Noe, D.A.; Weedn, V.; Bell, W.R. Direct spectrophotometry of serum hemoglobin: An Allen correction compared with a three-wavelength polychromatic analysis. Clin. Chem. 1984, 30, 627–630. [Google Scholar] [CrossRef] [PubMed]
- Miao, C.; Xie, Z.; Chang, J. Critical Roles of microRNAs in the Pathogenesis of Fatty Liver: New Advances, Challenges, and Potential Directions. Biochem. Genet. 2018, 56, 423–449. [Google Scholar] [CrossRef] [PubMed]
- Niculescu, L.S.; Simionescu, N.; Fuior, E.V.; Stancu, C.S.; Carnuta, M.G.; Dulceanu, M.D.; Raileanu, M.; Dragan, E.; Sima, A.V. Inhibition of miR-486 and miR-92a decreases liver and plasma cholesterol levels by modulating lipid-related genes in hyperlipidemic hamsters. Mol. Biol. Rep. 2018, 45, 497–509. [Google Scholar] [CrossRef]
- Vaughan, A.M.; Oram, J.F. ABCA1 and ABCG1 or ABCG4 act sequentially to remove cellular cholesterol and generate cholesterol-rich HDL. J. Lipid Res. 2006, 47, 2433–2443. [Google Scholar] [CrossRef]
- Hoffman, W.H.; Biade, S.; Zilfou, J.T.; Chen, J.; Murphy, M. Transcriptional repression of the anti-apoptotic survivin gene by wild type p53. J. Biol. Chem. 2002, 277, 3247–3257. [Google Scholar] [CrossRef]
- Chen, Y.; Buyel, J.J.; Hanssen, M.J.W.; Siegel, F.; Pan, R.; Naumann, J.; Schell, M.; van der Lans, A.; Schlein, C.; Froehlich, H.; et al. Exosomal microRNA miR-92a concentration in serum reflects human brown fat activity. Nat Commun 2016, 7, 1–9. [Google Scholar] [CrossRef]
- Golding, D.M.; Rees, D.J.; Davies, J.R.; Relkovic, D.; Furby, H.V.; Guschina, I.A.; Hopkins, A.L.; Davies, J.S.; Resnick, J.L.; Isles, A.R.; et al. Paradoxical leanness in the imprinting-centre deletion mouse model for Prader–Willi syndrome. J. Endocrinol. 2016, 232, 123–135. [Google Scholar] [CrossRef]
- Miao, L.; Yin, R.-X.; Pan, S.-L.; Yang, S.; Yang, D.-Z.; Lin, W.-X. Circulating miR-3659 may be a potential biomarker of dyslipidemia in patients with obesity. J. Transl. Med. 2019, 17, 25. [Google Scholar] [CrossRef]
- Yamada, H.; Suzuki, K.; Ichino, N.; Ando, Y.; Sawada, A.; Osakabe, K.; Sugimoto, K.; Ohashi, K.; Teradaira, R.; Inoue, T.; et al. Associations between circulating microRNAs (miR-21, miR-34a, miR-122 and miR-451) and non-alcoholic fatty liver. Clin. Chim. Acta 2013, 424, 99–103. [Google Scholar] [CrossRef]
- Pirola, C.J.; Gianotti, T.F.; Castaño, G.O.; Mallardi, P.; Martino, J.S.; Ledesma, M.M.G.L.; Flichman, D.; Mirshahi, F.; Sanyal, A.J.; Sookoian, S. Circulating microRNA signature in non-alcoholic fatty liver disease: From serum non-coding RNAs to liver histology and disease pathogenesis. Gut 2015, 64, 800–812. [Google Scholar] [CrossRef] [PubMed]
- Kamali, L.; Adibi, A.; Ebrahimian, S.; Jafari, F.; Sharifi, M. Diagnostic Performance of Ultrasonography in Detecting Fatty Liver Disease in Comparison with Fibroscan in People Suspected of Fatty Liver. Adv. Biomed. Res. 2019, 8, 69. [Google Scholar]
- Mottin, C.C.; Moretto, M.; Padoin, A.V.; Swarowsky, A.M.; Toneto, M.G.; Glock, L.; Repetto, G. The role of ultrasound in the diagnosis of hepatic steatosis in morbidly obese patients. Obes. Surg. 2004, 14, 635–637. [Google Scholar] [CrossRef] [PubMed]
- Rolfe, E.D.L.; Brage, S.; Sleigh, A.; Finucane, F.; Griffin, S.J.; Wareham, N.J.; Ong, K.K.; Forouhi, N.G. Validity of ultrasonography to assess hepatic steatosis compared to magnetic resonance spectroscopy as a criterion method in older adults. PLoS ONE 2018, 13, e0207923. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| MiRNA | OB Subjects Mean (Range) | PWS Subjects Mean (Range) | Fold Change |
|---|---|---|---|
| ** hsa-miR-122-5p | 0.70 (0.22–1.17) | 0.16 (0.09–0.22) | 4.38 |
| * hsa-miR-151a-5p | 0.90 (0.52–1.28) | 0.33 (0.16–0.51) | 2.72 |
| * hsa-miR-92a-3p | 0.71 (0.52–0.89) | 0.53 (0.28–0.78) | 1.34 |
| hsa-miR-425-5p | 1.39 (0.89–1.89) | 0.76 (0.46–1.07) | 1.82 |
| hsa-miR-23a-3p | 1.36 (0.83–1.89) | 1.02 (0.64–1.40) | 1.33 |
| hsa-miR-24-3p | 1.03 (0.59–1.48) | 0.78 (0.36–1.20) | 1.32 |
| hsa-miR-93-5p | 0.68 (0.38–0.98) | 0.56 (0.23–0.89) | 1.21 |
| hsa-miR-106b-5p | 0.85 (0.54–1.16) | 0.76 (0.36–1.16) | 1.11 |
| hsa-miR-191-5p | 0.77 (0.51–1.02) | 0.69 (0.34–1.04) | 1.11 |
| MiRNA | OBS+ Gr. 1 Mean (Range) | PWS+ Gr. 1 Mean (Range) | Fold Change |
|---|---|---|---|
| *** hsa-miR-151a-5p | 1.11 (0.47–1.74) | 0.38 (0.05–0.71) | 2.92 |
| ** hsa-miR-92a-3p | 0.88 (0.59–1.17) | 0.46 (0.13–0.78) | 1.91 |
| * hsa-miR-106b-5p | 0.92 (0.37–1.47) | 0.52 (0.01–1.08) | 1.76 |
| * hsa-miR-93-5p | 0.78 (0.38–1.19) | 0.49 (0.01–1.10) | 1.59 |
| hsa-miR-122-5p | 0.25 (0.06–0.45) | 0.14 (0.03–0.24) | 1.78 |
| hsa-miR-425-5p | 1.25 (0.38–2.12) | 0.74 (0.26–1.23) | 1.68 |
| hsa-miR-24-3p | 1.10 (0.42–1.78) | 0.68 (0.01–1.36) | 1.61 |
| hsa-miR-191-5p | 0.85 (0.40–1.31) | 0.67 (0.04–1.30) | 1.26 |
| hsa-miR-23a-3p | 1.37 (0.64–2.11) | 1.17 (0.52–1.83) | 1.17 |
| MiRNA | Prader–Willi Syndrome | ||
|---|---|---|---|
| Steatosis Gr. 1 Mean (Range) | Steatosis Gr. 2/3 Mean (Range) | Fold Change | |
| * hsa-miR-106b-5p | 0.29 (0.01–0.60) | 1.01 (0.40–1.61) | 3.48 |
| * hsa-miR-93-5p | 0.23 (0.21–0.44) | 0.62 (0.26–0.98) | 2.69 |
| hsa-miR-92a-3p | 0.34 (0.11–0.57) | 0.88 (0.19–1.58) | 2.58 |
| hsa-miR-425-5p | 0.59 (0.21–0.97) | 1.48 (0.28–2.68) | 2.50 |
| hsa-miR-191-5p | 0.39 (0.15–0.64) | 0.96 (0.31–1.60) | 2.46 |
| hsa-miR-151a-5p | 0.52 (0.01–1.08) | 0.92 (0.37–1.47) | 1.73 |
| hsa-miR-23a-3p | 1.06 (0.40–1.72) | 1.38 (0.20–2.56) | 1.30 |
| hsa-miR-122-5p | 0.14 (0.03–0.24) | 0.17 (0.07–0.27) | 1.21 |
| hsa-miR-24-3p | 0.38 (0.01–1.36) | 0.44 (0.08–0.81) | 1.15 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pratama, M.Y.; Pascut, D.; Tamini, S.; Minocci, A.; Tiribelli, C.; Grugni, G.; Sartorio, A. Circulating microRNA Associated to Different Stages of Liver Steatosis in Prader–Willi Syndrome and Non-Syndromic Obesity. J. Clin. Med. 2020, 9, 1123. https://doi.org/10.3390/jcm9041123
Pratama MY, Pascut D, Tamini S, Minocci A, Tiribelli C, Grugni G, Sartorio A. Circulating microRNA Associated to Different Stages of Liver Steatosis in Prader–Willi Syndrome and Non-Syndromic Obesity. Journal of Clinical Medicine. 2020; 9(4):1123. https://doi.org/10.3390/jcm9041123
Chicago/Turabian StylePratama, Muhammad Yogi, Devis Pascut, Sofia Tamini, Alessandro Minocci, Claudio Tiribelli, Graziano Grugni, and Alessandro Sartorio. 2020. "Circulating microRNA Associated to Different Stages of Liver Steatosis in Prader–Willi Syndrome and Non-Syndromic Obesity" Journal of Clinical Medicine 9, no. 4: 1123. https://doi.org/10.3390/jcm9041123
APA StylePratama, M. Y., Pascut, D., Tamini, S., Minocci, A., Tiribelli, C., Grugni, G., & Sartorio, A. (2020). Circulating microRNA Associated to Different Stages of Liver Steatosis in Prader–Willi Syndrome and Non-Syndromic Obesity. Journal of Clinical Medicine, 9(4), 1123. https://doi.org/10.3390/jcm9041123