Evaluation of Proinflammatory, NF-kappaB Dependent Cytokines: IL-1α, IL-6, IL-8, and TNF-α in Tissue Specimens and Saliva of Patients with Oral Squamous Cell Carcinoma and Oral Potentially Malignant Disorders


 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Group
2.2. Histopathology and Immunohistochemistry
2.3. Laboratory Tests
2.4. Statistical Analysis
3. Results
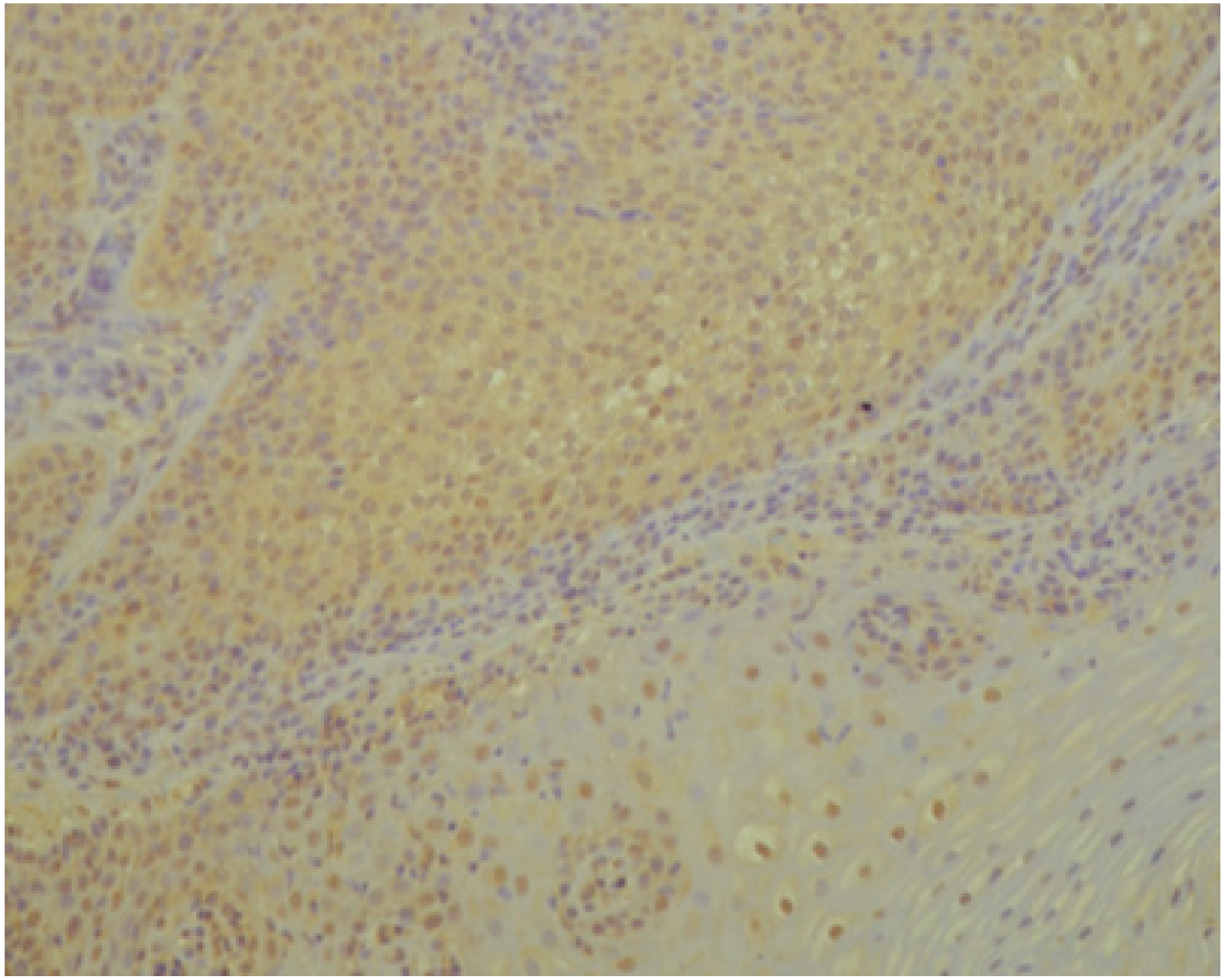
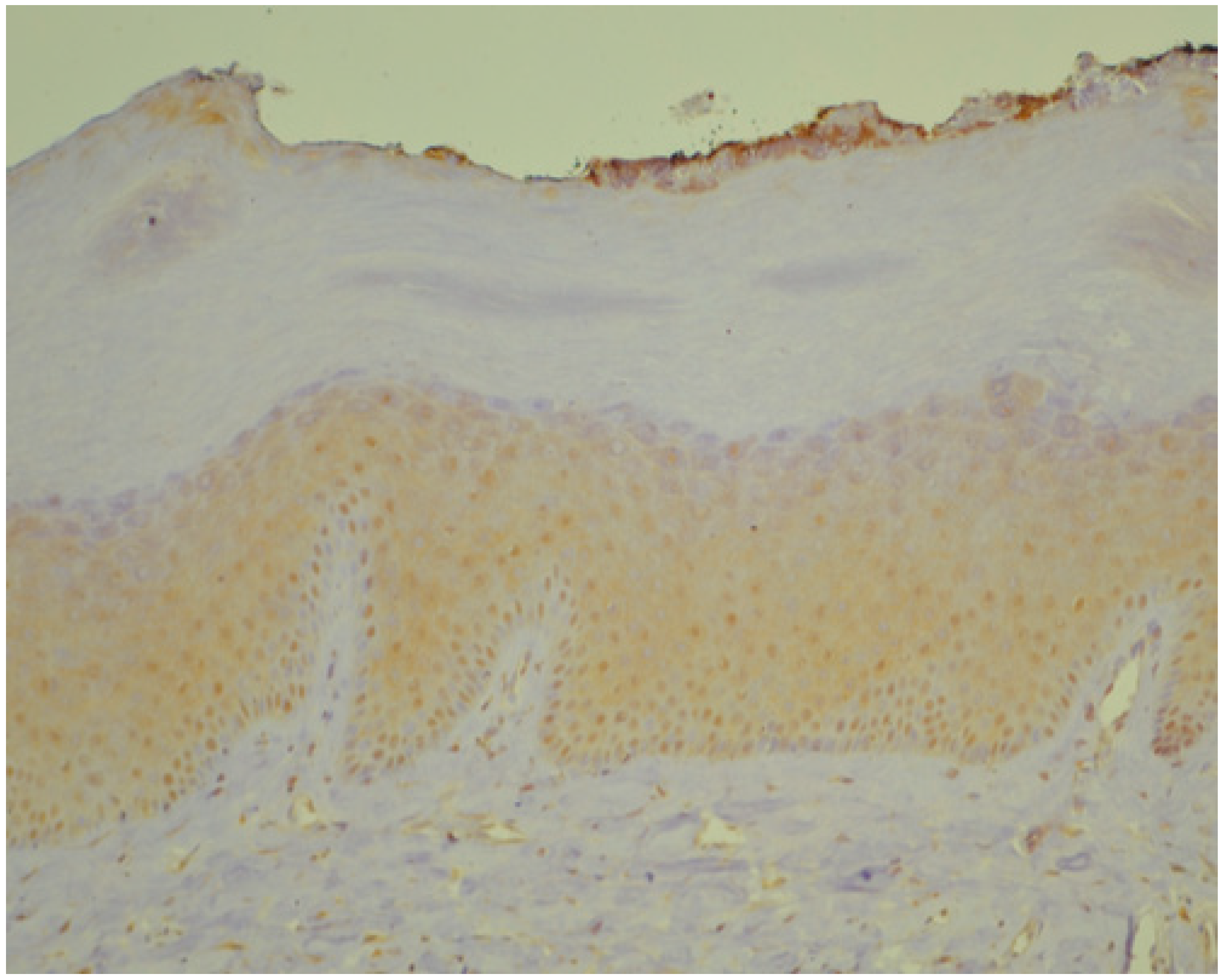
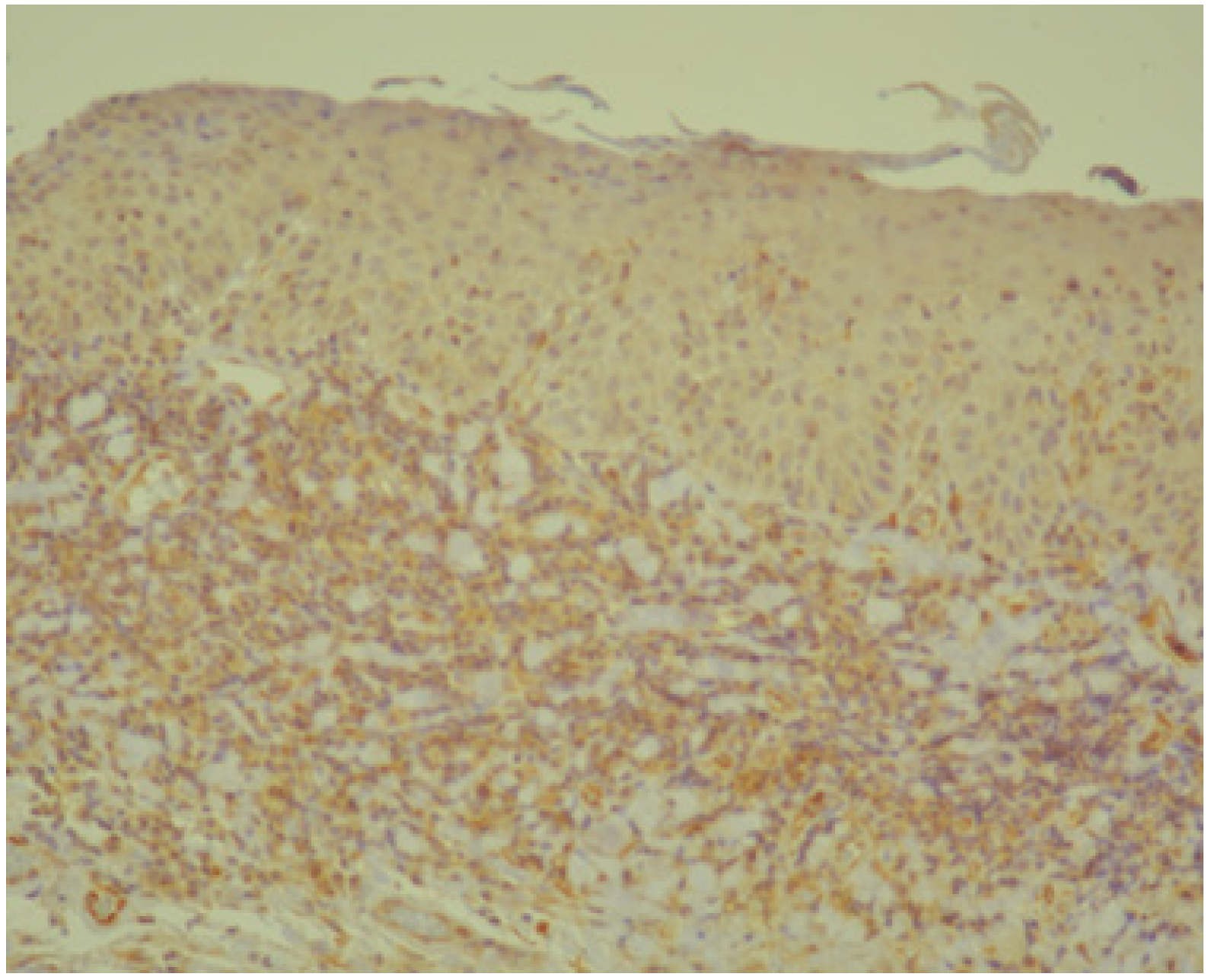
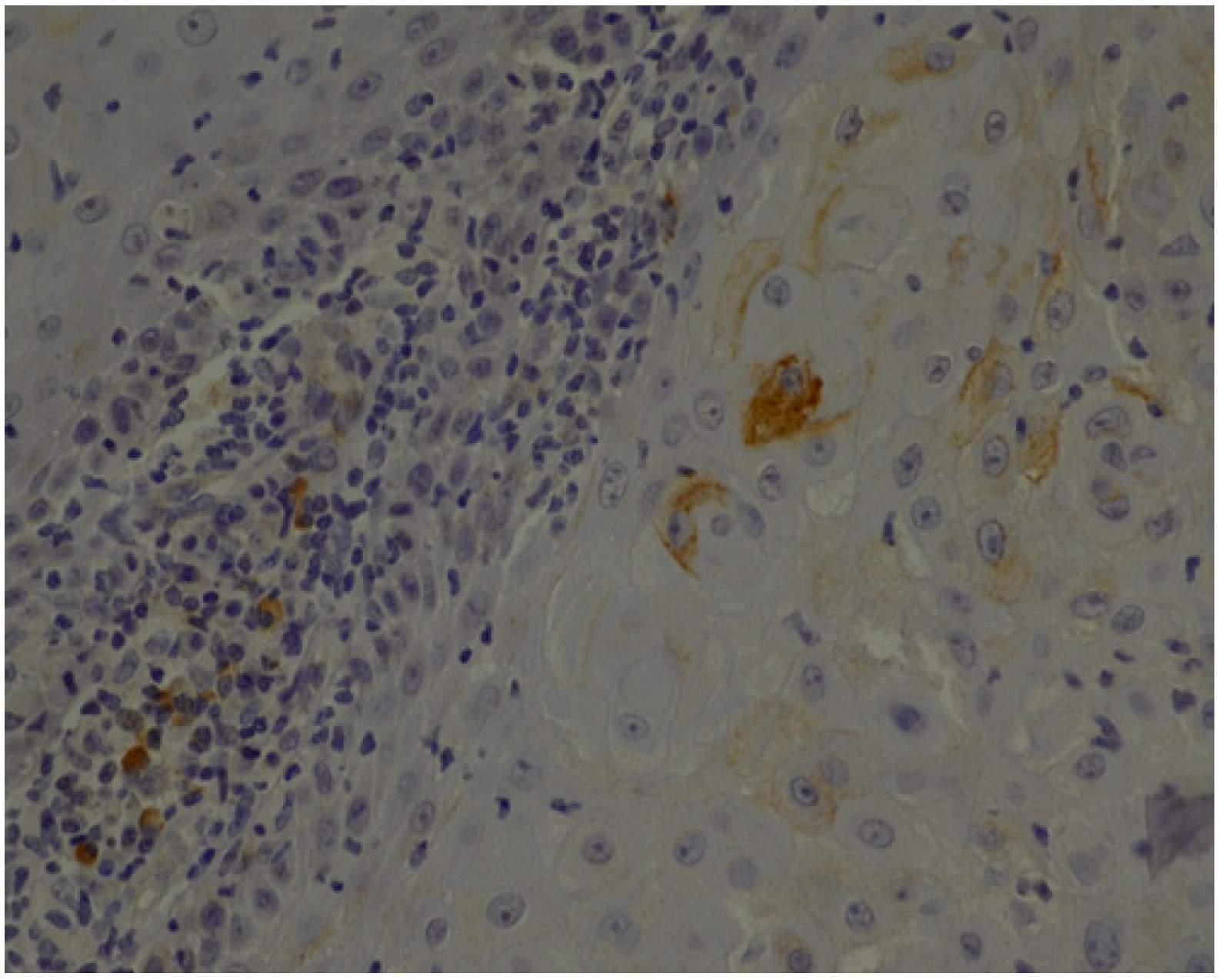
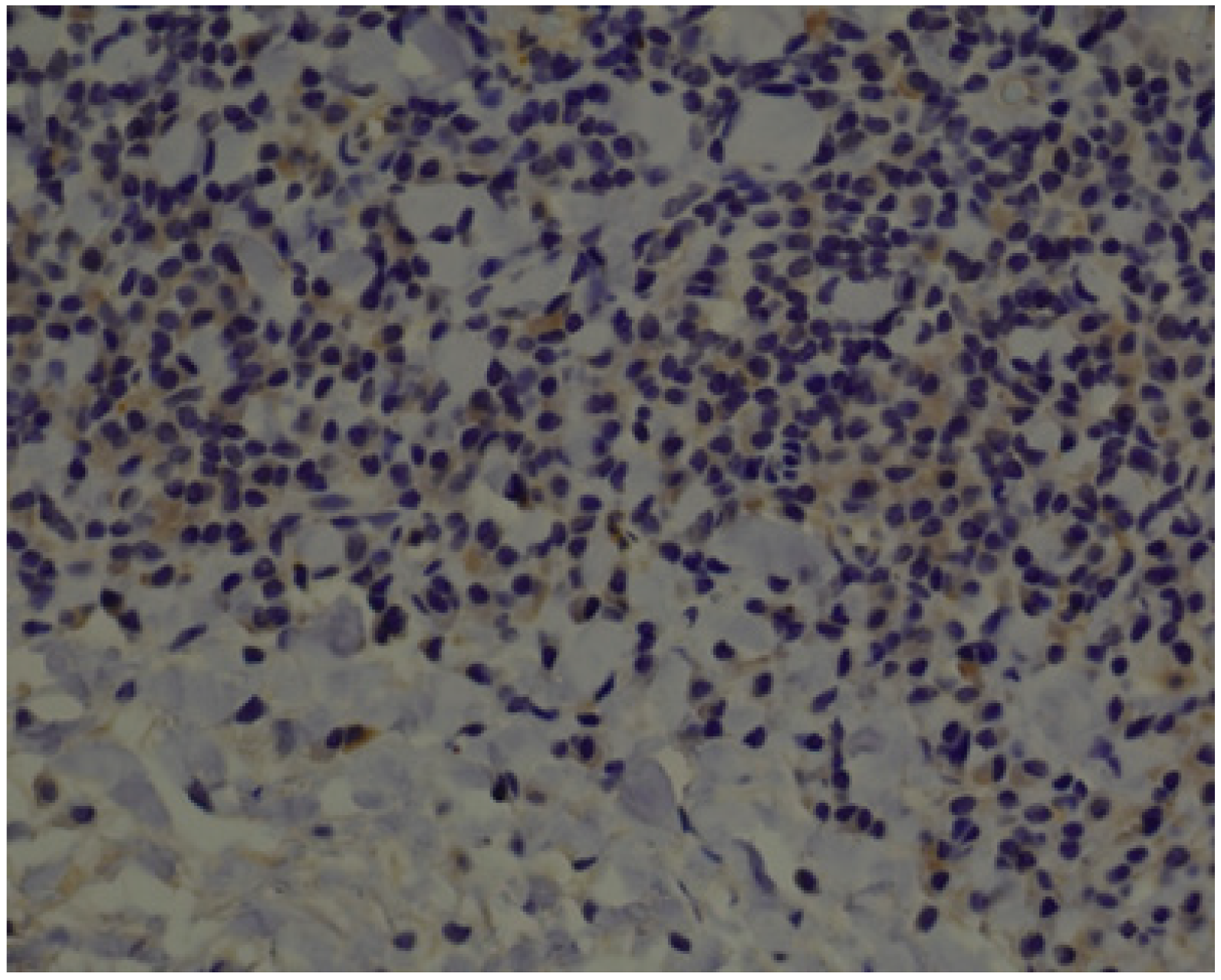
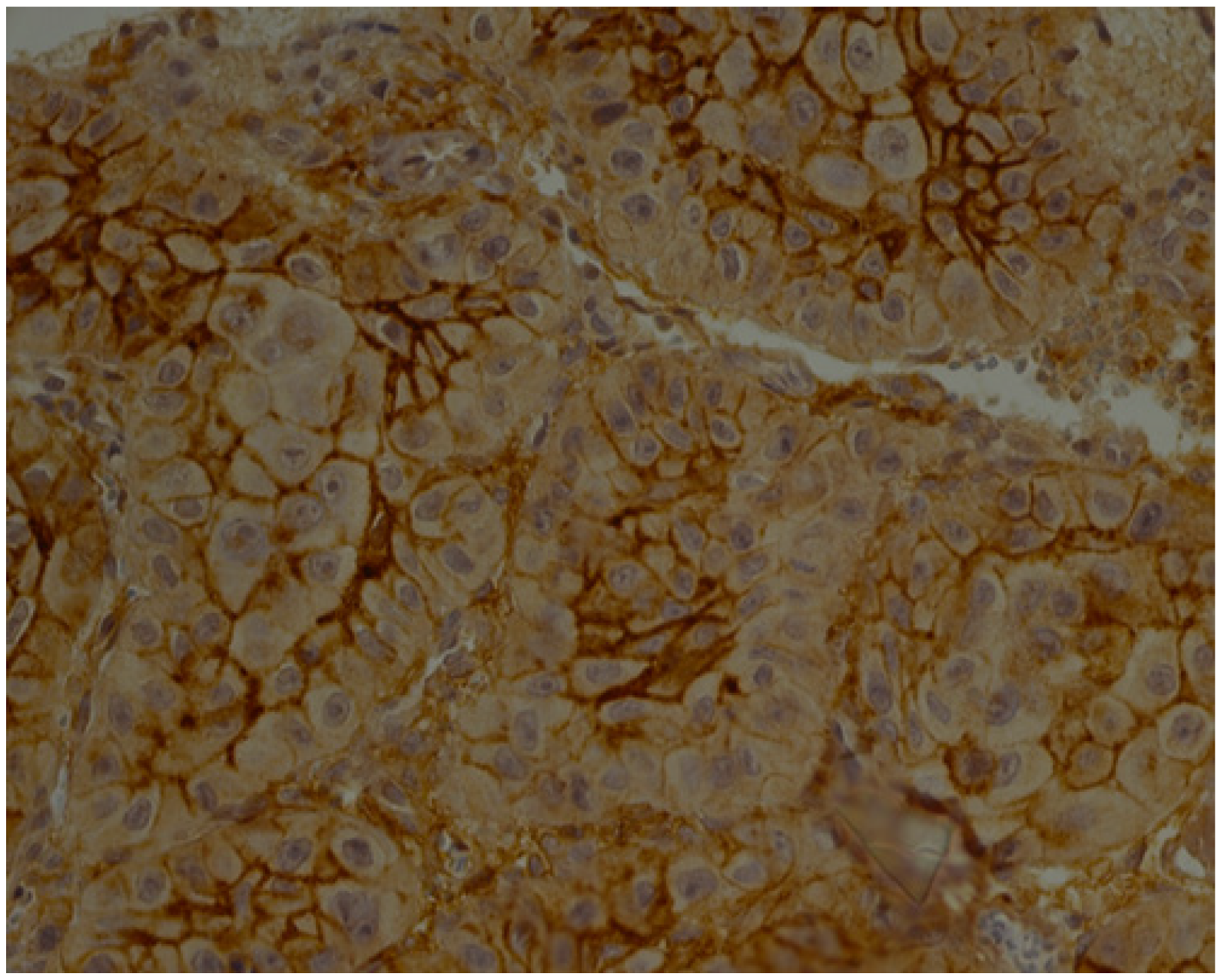
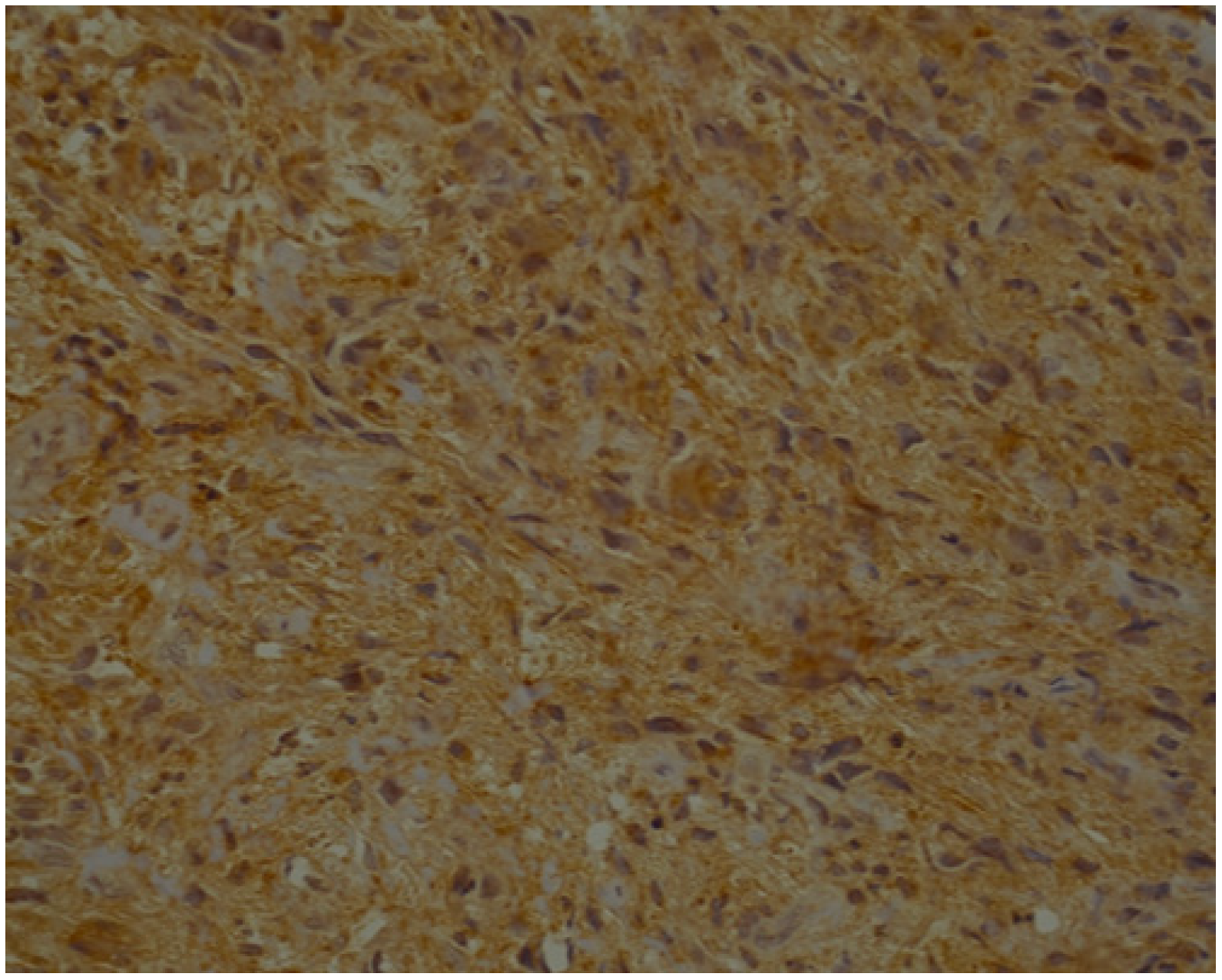
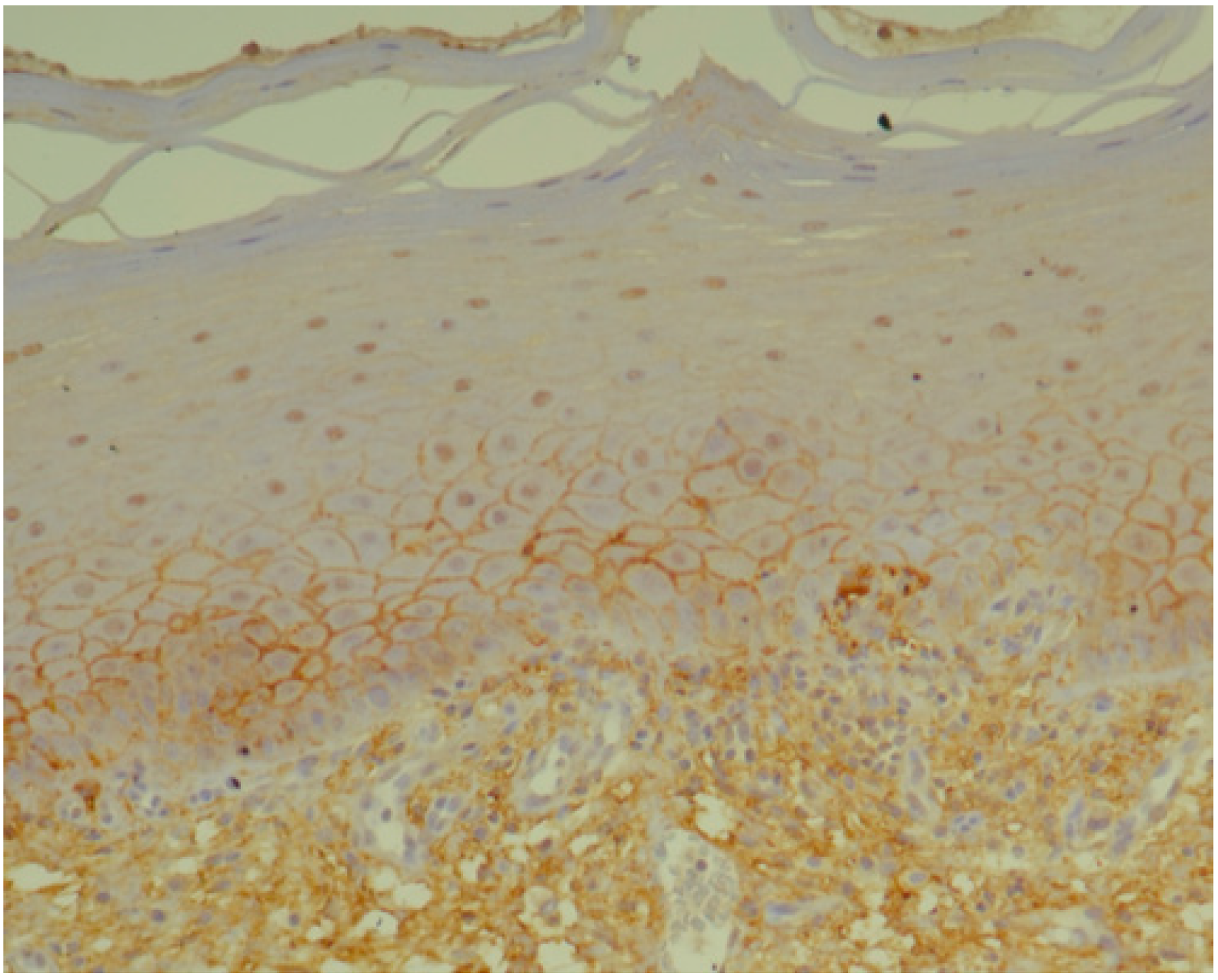
3.1. Histopathology and Immunohistochemistry
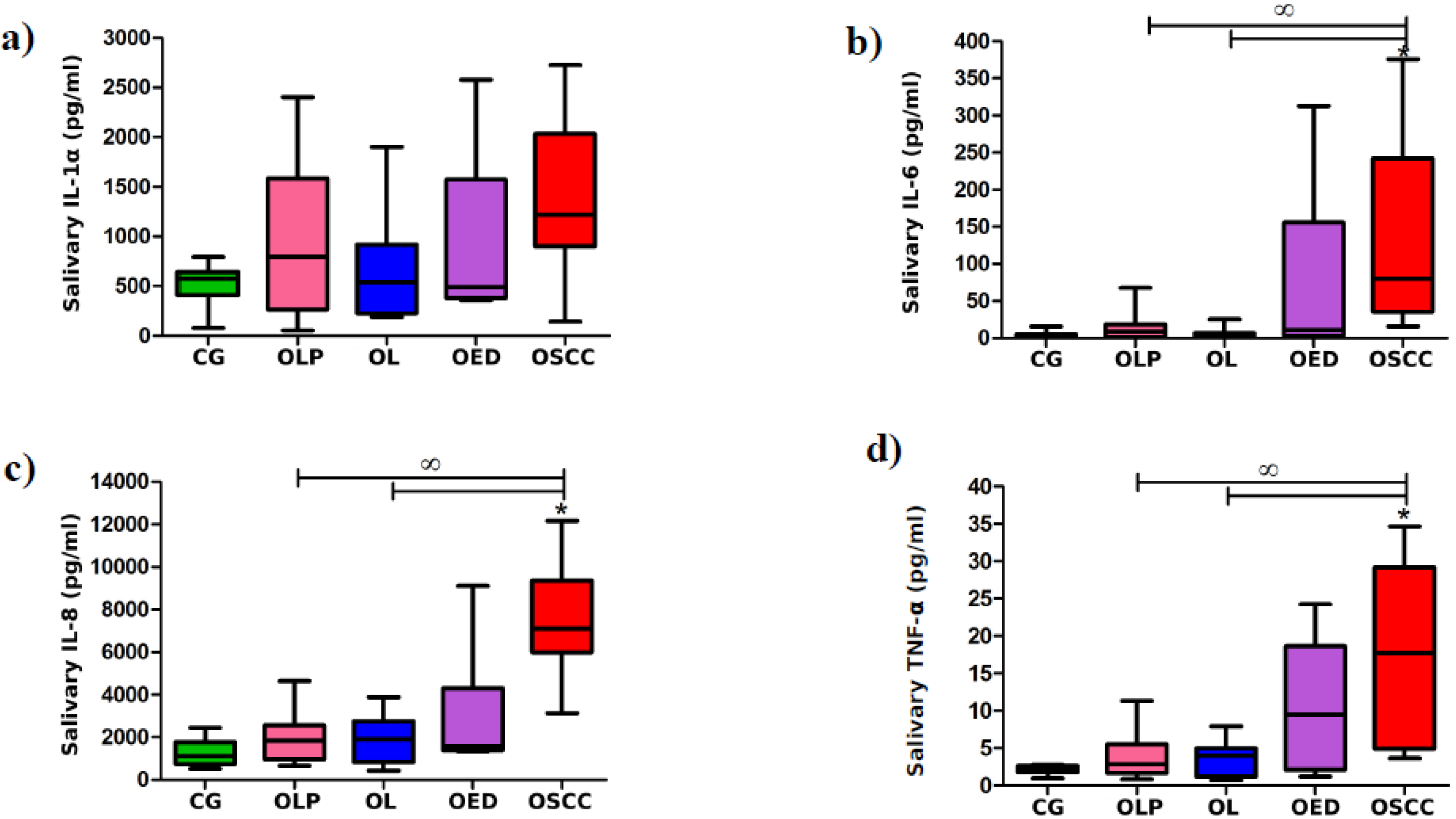
3.2. Laboratory Tests
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Du, M.; Nair, R.; Jamieson, L.; Liu, Z.; Bi, P. Incidence Trends of Lip, Oral Cavity, and Pharyngeal Cancers: Global Burden of Disease 1990–2017. J. Dent. Res. 2019, 24, 22034519894963. [Google Scholar] [CrossRef] [PubMed]
- Johnson, N.W.; Warnakulasuriya, S.; Gupta, P.C.; Dimba, E.; Chindia, M.; Otoh, S.C.; Sankaranarayaranan, R.; Califano, J.; Kowalski, L. Global oral health inequalities in incidence and outcomes for oral cancer: Causes and solutions. Adv. Dent. Res. 2011, 23, 237–246. [Google Scholar] [CrossRef] [PubMed]
- McGuire, S. World cancer report 2014. Geneva, Switzerland: World Health Organization, international agency for research on cancer, WHO Press, 2015. Adv. Nutr. 2016, 7, 418–419. [Google Scholar] [CrossRef] [PubMed]
- Petruzzi, M.N.M.R.; Cherubini, K.; Salum, F.G.; de Figueiredo, M.A.Z. Role of tumor-associated macrophages in oral squamous cells carcinoma progression: An update on current knowledge. Diagn. Pathol. 2017, 12, 32. [Google Scholar] [CrossRef] [PubMed]
- El-Naggar, A.K.; Chan, J.K.C.; Grandis, J.R.; Takata, T.; Slootweg, P.J. WHO Classification of Head and Neck Tumours, 4th ed.; International Agency for Research on Cancer: Lyon, France, 2017; pp. 105–131. [Google Scholar]
- Van der Waal, I. Potentially malignant disorders of the oral and oropharyngeal mucosa; terminology, classification and present concepts of management. Oral Oncol. 2009, 45, 317–323. [Google Scholar] [CrossRef]
- Suresh, A.; Kuriakose, M.A.; Mohanta, S.; Siddappa, G. Carcinogenesis and Field Cancerization in Oral Squamous Cell Carcinoma. In Contemporary Oral Oncology: Biology, Epidemiology, Etiology, and Prevention, 1st ed.; Kuriakose, M.A., Ed.; Springer International Publishing: Cham, Switzerland, 2017; Volume 1, pp. 1–30. [Google Scholar]
- de Oliveira, M.V.; Fraga, C.A.; Gomez, R.S.; Paula, A.M. Immunohistochemical expression of interleukin-4, -6, -8, and -12 in inflammatory cells in surrounding invasive front of oral squamous cell carcinoma. Head Neck. 2009, 31, 1439–1446. [Google Scholar] [CrossRef]
- Balkwill, F.; Mantovani, A. Inflammation and cancer: Back to Virchow? Lancet 2001, 357, 539–545. [Google Scholar] [CrossRef]
- Vallée, A.; Lecarpentier, Y. Crosstalk between peroxisome proliferator-activated receptor gamma and the canonical WNT/β-catenin pathway in chronic inflammation and oxidative stress during carcinogenesis. Front. Immunol. 2018, 9, 745. [Google Scholar] [CrossRef]
- Lu, H.; Ouyang, W.; Huang, C. Inflammation, a key event in cancer development. Mol. Cancer Res. 2006, 4, 221–233. [Google Scholar] [CrossRef]
- Korneev, K.V.; Atretkhany, K.N.; Drutskaya, M.S.; Grivennikov, S.I.; Kuprash, D.V.; Nedospasov, S.A. TLR-signaling and proinflammatory cytokines as drivers of tumorigenesis. Cytokine 2017, 89, 127–135. [Google Scholar] [CrossRef]
- Kong, H.; Wang, Y.; Zeng, X.; Wang, Z.; Wang, H.; Xie, W. Differential expression of inflammasomes in lung cancer cell lines and tissues. Tumor Biol. 2015, 36, 7501–7513. [Google Scholar] [CrossRef] [PubMed]
- Narayan, C.; Kumar, A. Constitutive over expression of IL-1β, IL-6, NF-κB, and Stat3 is a potential cause of lung tumorgenesis in urethane (ethyl carbamate) induced Balb/c mice. J. Carcinog. 2012, 11, 9. [Google Scholar] [PubMed]
- Cao, L.; Li, W.J.; Yang, J.H.; Wang, Y.; Hua, Z.J.; Liu, D.; Chen, Y.Q.; Zhang, H.M.; Zhang, R.; Zhao, J.S.; et al. Inflammatory cytokine-induced expression of MASTL is involved in hepatocarcinogenesis by regulating cell cycle progression. Oncol. Lett. 2019, 17, 3163–3172. [Google Scholar] [CrossRef] [PubMed]
- Malicki, S.; Winiarski, M.; Matlok, M.; Kostarczyk, W.; Guzdek, A.; Konturek, P.C. IL-6 and IL-8 responses of colorectal cancer in vivo and in vitro cancer cells subjected to simvastatin. J. Physiol. Pharmacol. 2009, 60, 141–146. [Google Scholar] [PubMed]
- Tang, D.; Tao, D.; Fang, Y.; Deng, C.; Xu, Q.; Zhou, J. TNF-Alpha Promotes Invasion and Metastasis via NF-Kappa B Pathway in Oral Squamous Cell Carcinoma. Med. Sci. Monit. Basic Res. 2017, 23, 141–149. [Google Scholar] [CrossRef]
- Colotta, F.; Allavena, P.; Sica, A.; Garlanda, C.; Mantovani, A. Cancer-related inflammation, the seventh hallmark of cancer: Links to genetic instability. Carcinogenesis 2009, 30, 1073–1081. [Google Scholar] [CrossRef]
- Matthews, G.M.; de Matos Simoes, R.; Dhimolea, E.; Sheffer, M.; Gandolfi, S.; Dashevsky, O.; Sorrell, J.D.; Midsiades, C.S. NF-κB dysregulation in multiple myeloma. Semin. Cancer Biol. 2018, 39, 68–76. [Google Scholar] [CrossRef]
- Rhodus, N.L.; Ho, V.; Miller, C.S.; Myers, S.; Ondrey, F. NF-kappaB dependent cytokine levels in saliva of patients with oral preneoplastic lesions and oral squamous cell carcinoma. Cancer Detect. Prev. 2005, 29, 42–45. [Google Scholar] [CrossRef]
- Sakamoto, K.; Hikiba, Y.; Nakagawa, H.; Hayakawa, Y.; Yanai, A.; Akanuma, M.; Ogura, K.; Hirata, Y.; Kaestner, K.H.; Omata, M.; et al. IkappaB kinase beta regulates gastric carcinogenesis via IL-1α expression. Gastroenterology 2010, 139, 226–238. [Google Scholar] [CrossRef]
- Bae, J.Y.; Kim, E.K.; Yang, D.H.; Zhang, X.; Park, Y.J.; Lee, D.Y.; Che, C.M.; Kim, J. Reciprocal interaction between carcinoma-associated fibroblasts and squamous carcinoma cells through interleukin-1α induces cancer progression. Neoplasia 2014, 16, 928–938. [Google Scholar] [CrossRef]
- Zarogoulidis, P.; Yarmus, L.; Darwiche, K.; Walter, R.; Huang, H.; Li, Z.; Zaric, B.; Tsakiridis, K.; Zarogoulidis, K. Interleukin-6 cytokine: A multifunctional glycoprotein for cancer. Immunome Res. 2013, 9, 16535. [Google Scholar] [CrossRef] [PubMed]
- Sahibzada, H.A.; Kurshid, D.; Khan, R.S.; Naseem, M.; Siddique, K.M.; Mali, M.; Zafar, M.S. Salivary IL-8, IL-6 and TNF-α as potential diagnostic biomarkers for oral cancer. Diagnostics (Basel) 2017, 7, 21. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, R.; Thayalan, D.K.; Padmanaban, R.; Ramadas, R.; Annasamy, R.K.; Anandan, N. Association of serum and salivary tumor necrosis factor-α with histological grading in oral cancer and its role in differentiating premalignant and malignant oral disease. Asian Pac. J. Cancer Prev. 2014, 15, 7141–7148. [Google Scholar] [CrossRef]
- Yan, B.; Wang, H.; Rabbani, Z.N.; Zhao, Y.; Li, W.; Yuan, Y.; Li, F.; Dewhirst, M.W.; Li, C.Y. Tumor necrosis factor-alpha is a potent endogenous mutagen that promotes cellular transformation. Cancer Res. 2006, 66, 11565–11570. [Google Scholar] [CrossRef] [PubMed]
- Jeng, J.H.; Wang, Y.J.; Chiang, B.L.; Lee, P.H.; Chan, C.P.; Ho, Y.S.; Wang, T.M.; Lee, J.J.; Hahn, L.J.; Chang, M.C. Roles of keratinocyte inflammation in oral cancer: Regulating the prostaglandin E2, interleukin-6 and TNF-alpfa production of oral epithelial cells by Areca nut extract and arecoline. Carcinogenesis 2003, 24, 1301–1315. [Google Scholar] [CrossRef] [PubMed]
- Feller, L.; Altini, M.; Lemmer, J. Inflammation in the context of oral cancer. Oral Oncol. 2013, 49, 887–892. [Google Scholar] [CrossRef]
- Piva, M.R.; DE Souza, L.B.; Martins-Filho, P.R.; Soares, R.C.; de Santana Santos, T.; DE Sousa Andrade, E.S. Role of inflammation in oral carcinogenesis (Part I): Histological grading of malignancy using binary system. Oncol. Lett. 2011, 2, 1225–1231. [Google Scholar] [CrossRef][Green Version]
- Gai, C.; Camussi, F.; Broccoletti, R.; Gambino, A.; Cabras, M.; Molinaro, L.; Carossa, S.; Camussi, G.; Arduino, P.G. Salivary extracellular vesicle-associated miRNAs as potential biomarkers in oral squamous cell carcinoma. BMC Cancer 2018, 18, 439. [Google Scholar] [CrossRef]
- Babiuch, K.; Bednarczyk, A.; Gawlik, K.; Pawlica-Gosiewska, D.; Kęsek, B.; Darczuk, D.; Stępień, P.; Chomyszyn-Gajewska, M.; Kaczmarzyk, T. Evaluation of enzymatic and non-enzymatic antioxidant status and biomarkers of oxidative stress in saliva of patients with oral squamous cell carcinoma and oral leukoplakia: A pilot study. Acta Odontol. Scand. 2019, 77, 408–418. [Google Scholar] [CrossRef]
- Shan, J.; Sun, Z.; Yang, J.; Xu, J.; Shi, W.; Wu, Y.; Fan, Y.; Li, H. Discovery and preclinical validation of proteomic biomarkers in saliva for early detection of oral squamous cell carcinomas. Oral Dis. 2019, 25, 97–107. [Google Scholar] [CrossRef]
- Sridharan, G.; Ramani, P.; Patankar, S.; Vijayaraghavan, R. Evaluation of salivary metabolomics in oral leukoplakia and oral squamous cell carcinoma. J. Oral Pathol. Med. 2019, 48, 299–306. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Kaczor-Urbanowicz, K.E.; Wong, D.T.W. Salivary biomarkers in cancer detection. Med. Oncol. 2017, 34, 7. [Google Scholar] [CrossRef] [PubMed]
- Brailo, V.; Vucicevic-Boras, V.; Lukac, J.; Biocina-Lukenda, D.; Zilic-Alajbeg, I.; Milenovic, A.; Balija, M. Salivary and serum interleukin 1 beta, interleukin 6 and tumor necrosis factor alpha in patients with leukoplakia and oral cancer. Med. Oral Patol. Oral Cir. Bucal 2012, 17, e10–e15. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Haq, A.; Kusnierz-Cabala, B.; Darczuk, D.; Sobuta, E.; Dumnicka, P.; Wojas-Pelc, A.; Chomyszyn-Gajewska, M. Interleukin-6 and neopterin levels in the serum and saliva of patients with Lichen planus and oral Lichen planus. J. Oral Pathol. Med. 2014, 43, 734–739. [Google Scholar] [CrossRef] [PubMed]
- Paneer Selvam, N.; Sadaksharan, J. Salivary interleukin-6 in the detection of oral cancer and precancer. Asia-Pac. J. Clin. Oncol. 2015, 11, 236–241. [Google Scholar] [CrossRef]
- Kramer, I.R.; Lucas, R.B.; Pindborg, J.J.; Sobin, L.H. Definition of leukoplakia and related lesions: An aid to studies on oral precancer. Oral Surg. Oral Med. Oral Pathol. 1978, 46, 518–539. [Google Scholar]
- Barnes, L.; Eveson, J.W.; Reichart, P.; Sidransky, D. World Health Organization Classification of Tumours. In Pathology and Genetics of Head and Neck Tumours, 3rd ed.; International Agency for Research on Cancer: Lyon, France, 2005; Volume 9, pp. 177–181. [Google Scholar]
- Sloan, P. Pathological Aspects of Oral Precancer. In Oral Precancer: Diagnosis and Management of Potentially Malignant Disorders; Thomson, P., Ed.; John Wiley & Sons: Oxford, UK, 2012. [Google Scholar]
- Nagel, H.; Laskawi, R.; Wahlers, A.; Hemmerlein, B. Expression of matrix metalloproteinases MMP-2, MMP-9 and their tissue inhibitors TIMP-1, -2, and -3 in benign and malignant tumours of the salivary gland. Histopathology 2004, 44, 222–231. [Google Scholar] [CrossRef]
- Abbas, N.F.; Labib El-Sharkawy, S.; Abbas, E.A.; Abdel Monem El-Shaer, M. Immunohistochemical study of p53 and angiogenesis in benign and preneoplastic oral lesions and oral squamous cell carcinoma. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2007, 103, 385–390. [Google Scholar] [CrossRef]
- Piva, M.R.; De Souza, L.B.; Martins-Filho, P.R.S.; Nonaka, C.F.W.; De Santana Santos, T.; De Souza Andrade, E.S.; Piva, D. Role of inflammation in oral carcinogenesis (Part II): CD8, FOXP3, TNF-alpha, TGF-beta and NF-kappaB expression. Oncol. Lett. 2013, 5, 1909–1914. [Google Scholar] [CrossRef][Green Version]
- Vissink, A.; Wolff, A.; Veerman, E.C.I. Saliva collectors. In Salivary Diagnostics; Wong, D.T., Ed.; Wiley-Blackwell: Ames, IA, USA, 2008; pp. 37–59. [Google Scholar]
- Punyani, S.R.; Sathavane, R.S. Salivary level of interleukin-8 in oral precancer and oral squamous cell carcinoma. Clin. Oral Investig. 2013, 17, 517–524. [Google Scholar] [CrossRef]
- Kaur, J.; Jacobs, R. Proinflammatory cytokine levels in oral lichen planus, oral leukoplakia, and oral submucous fibrosis. J. Korean Assoc. Oral Maxillofac. Surg. 2015, 41, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Woods, K.V.; El-Naggar, A.; Clayman, G.L.; Grimm, E.A. Variable expression of cytokines in human head and neck squamous cell carcinoma cell lines and consistent expression in surgical specimens. Cancer Res. 1998, 58, 3132–3141. [Google Scholar]
- Chen, Z.; Malhotra, P.S.; Thomas, G.R.; Ondrey, F.G.; Duffey, D.C.; Smith, C.W.; Enamorado, I.; Yeh, N.T.; Kroog, G.S.; Rudy, S.; et al. Expression of proinflammatory and proangiogenic cytokines in patients with head and neck cancer. Clin. Cancer Res. 1999, 5, 1369–1379. [Google Scholar] [PubMed]
- Haque, M.F.; Harris, M.; Meghji, S.; Barrett, A.W. Immunolocalization of cytokines and growth factors in oral submucous fibrosis. Cytokine 1998, 10, 713–719. [Google Scholar] [CrossRef]
- Sclavounou, A.; Chrysomali, E.; Scorilas, A.; Karameris, A. TNF-alpha expression and apoptosis-regulating proteins in oral lichen planus: A comparative immunohistochemical evaluation. J. Oral Pathol. Med. 2000, 29, 370–375. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.T.; Wong, Y.K.; Hsiao, H.Y.; Wang, Y.W.; Chan, M.Y.; Chang, K.W. Evaluation of saliva and plasma cytokine biomarkers in patients with oral squamous cell carcinoma. Int. J. Oral Maxillofac. Surg. 2017, 47, 699–707. [Google Scholar] [CrossRef]
- Rhodus, N.L.; Cheng, B.; Myers, S.; Miller, L.; Ho, V.; Ondrey, F. The feasibility of monitoring NF-kappaB associated cytokines: TNF-alpha, IL-1alpha, IL-6, and IL-8 in whole saliva for the malignant transformation of oral lichen planus. Mol. Carcinog. 2005, 44, 77–82. [Google Scholar] [CrossRef]
- SahebJamee, M.; Eslami, M.; AtarbashiMoghadam, F.; Sarafnejad, A. Salivary concentration of TNFalpha, IL1 alpha, IL6, and IL8 in oral squamous cell carcinoma. Med. Oral Patol. Oral Cir. Bucal. 2008, 13, E292–E295. [Google Scholar]
- Korostoff, A.; Reder, L.; Masood, R.; Sinha, U.K. The role of salivary biomarkers in tongue cancer invasion and mortality. Oral Oncol. 2011, 47, 282–287. [Google Scholar] [CrossRef]
- Sharma, M.; Bairy, I.; Pai, K.; Satyamoorthy, K.; Prasad, S.; Berkovitz, B.; Radhakrishnan, R. Salivary IL-6 levels in oral leukoplakia with dysplasia and its clinical relevance to tobacco habits and periodontitis. Clin. Oral Investig. 2011, 15, 705–714. [Google Scholar] [CrossRef]
- Rajkumar, K.; Kumar, A.R.; Ramyamalini, V.; Nandhini, G.; Kumar, T.D.; Ashwini, B.K.; Anandan, S.N. Estimation of serological and salivary biomarkers in patients with oral squamous cell carcinoma, premalignant lesions & conditions. SRM J. Res. Dent. Sci. 2010, 1, 14–19. [Google Scholar]
- Rajkumar, K.; Nandhini, G.; Ramaya, R.; Rajashree, P.; Kumar, A.R.; Anandan, S.N. Validation of the diagnostic utility of salivary interleukin 8 in the differentiation of potentially malignant oral lesions and oral squamous cell carcinoma in a region with high endemicity. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 118, 309–319. [Google Scholar] [CrossRef] [PubMed]
- Dineshkumar, T.; Ashwini, B.K.; Rameshkumar, A.; Rajashree, P.; Ramya, R.; Rajkumar, K. Salivary and Serum Interleukin-6 Levels in Oral Premalignant Disorders and Squamous Cell Carcinoma: Diagnostic Value and Clinicopathologic Correlations. Asian Pac. J. Cancer Prev. 2016, 17, 4899–4906. [Google Scholar] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Score | Percentage of Immunopositive Cells | Staining Intensity |
|---|---|---|
| 0 | 0 | Negative |
| 1 | <5 | Weak |
| 2 | 5–50 | Moderate |
| 3 | >50 | Strong |
| Interleukin | Distribution | NOM n = 7 | OLP n = 15 | OL n = 21 | OED n = 10 | OSCC n = 14 | p * |
|---|---|---|---|---|---|---|---|
| IL-1⍺ | none | 2 (28.6) | 3 (20.0) | 5 (23.8) | 1 (10.0) | 1 (7.1) | 0.011 (0.003 ′) |
| basal | 1 (14.3) | 7 (46.7) | 6 (28.6) | 6 (60.0) | 4 (28.6) | ||
| parabasal | 4 (57.1) | 4 (26.7) | 4 (19.0) | 3 (30.0) | 1 (7.1) | ||
| all layers | 0 (0.0) | 1 (6.7) | 6 (28.6) | 0 (0.0) | 8 (57.1) | ||
| IL-6 | none | 2 (28.6) | 3 (20.0) | 2 (9.5) | 3 (30.0) | 4 (28.6) | 0.117 (0.292 ′) |
| basal | 1 (14.3) | 0 (0.0) | 0 (0.0) | 2 (20.0) | 0 (0.0) | ||
| parabasal | 2 (28.6) | 1 (6.7) | 3 (14.3) | 0 (0.0) | 1 (7.1) | ||
| all layers | 2 (28.6) | 11 (73.3) | 16 (76.2) | 5 (50.0) | 9 (64.3) | ||
| IL-8 | none | 7 (100.0) | 7 (46.7) | 13 (61.9) | 6 (60.0) | 3 (21.4) | 0.101 (0.021 ′) |
| basal | 0 (0.0) | 1 (6.7) | 2 (9.5) | 0 (0.0) | 1 (7.1) | ||
| parabasal | 0 (0.0) | 3 (20.0) | 2 (9.5) | 1 (10.0) | 1 (7.1) | ||
| all layers | 0 (0.0) | 4 (26.7) | 4 (19.0) | 3 (30.0) | 9 (64.3) | ||
| TNF-α | none | 2 (28.6) | 0 (0.0) | 1 (4.8) | 1 (10.0) | 1 (7.1) | 0.011 (0.005 ′) |
| basal | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (7.1) | ||
| parabasal | 3 (42.9) | 7 (46.7) | 4 (19.0) | 0 (0.0) | 0 (0.0) | ||
| all layers | 2 (28.6) | 8 (53.3) | 16 (76.2) | 9 (90.0) | 12 (85.7) |
| Immunoreactivity (Epithelium/Cancer Cells) | NOM n = 7 | OLP n = 15 | OL n = 21 | OED n = 10 | OSCC n = 14 | p * |
|---|---|---|---|---|---|---|
| IL-1α | 0.238 (0.169 ′) | |||||
| Min | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | |
| Max | 5.00 | 5.00 | 5.00 | 6.00 | 6.00 | |
| Me | 3.00 | 4.00 | 4.00 | 4.00 | 4.00 | |
| IQR | 5.00 | 5.00 | 5.00 | 6.00 | 6.00 | |
| IL-6 | 0.176 (0.769 ′) | |||||
| Min | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | |
| Max | 5.00 | 5.00 | 6.00 | 5.00 | 6.00 | |
| Me | 4.00 | 4.00 | 5.00 | 3.00.5.00 | 4.00 | |
| IQR | 5.00 | 5.00 | 6.00 | 5.00 | 6.00 | |
| IL-8 | 0.009 (0.006 ′) | |||||
| Min | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | |
| Max | 0.00 | 5.00 | 4.00 | 4.00 | 5.00 | |
| Me | 0.00 | 3.00 | 0.00 | 0.00 | 4.00 | |
| IQR | 0.00 | 5.00 | 4.00 | 4.00 | 5.00 | |
| TNF-α | 0.001 (0.003 ′) | |||||
| Min | 0.00 | 4.00 | 0.00 | 0.00 | 0.00 | |
| Max | 4.00 | 6.00 | 6.00 | 6.00 | 6.00 | |
| Me | 3.00 | 5.00 | 5.00 | 5.00 | 5.00 | |
| IQR | 4.00 | 2.00 | 6.00 | 6.00 | 6.00 |
| Immunoreactivity (Stroma) | NOM n = 7 | OLP n =15 | OL n = 21 | OED n =1 0 | OSCC n = 14 | p * |
|---|---|---|---|---|---|---|
| IL-1α | 0.064 (0.077 ′) | |||||
| Min | 3.00 | 3.00 | 4.00 | 4.00 | 3.00 | |
| Max | 5.00 | 6.00 | 6.00 | 6.00 | 6.00 | |
| Me | 4.00 | 5.00 | 6.00 | 5.00 | 5.00 | |
| IQR | 2.00 | 3.00 | 2.00 | 2.00 | 3.00 | |
| IL-6 | 0.049 (0.150 ′) | |||||
| Min | 2.00 | 4.00 | 3.00 | 3.00 | 3.00 | |
| Max | 6.00 | 6.00 | 6.00 | 6.00 | 6.00 | |
| Me | 5.00 | 5.00 | 5.00 | 5.00 | 4.00 | |
| IQR | 4.00 | 2.00 | 3.00 | 3.00 | 3.00 | |
| IL-8 | 0.012 (0.013 ′) | |||||
| Min | 0.00 | 2.00 | 2.00 | 2.00 | 2.00 | |
| Max | 3.00 | 5.00 | 5.00 | 4.00 | 5.00 | |
| Me | 2.00 | 3.00 | 3.00 | 3.00 | 3.00.5.00 | |
| IQR | 3.00 | 3.00 | 3.00 | 2.00 | 3.00 | |
| TNF-α | 0.001 (0.002′) | |||||
| Min | 2.00 | 4.00 | 4.00 | 5.00 | 4.00 | |
| Max | 5.00 | 6.00 | 6.00 | 6.00 | 6.00 | |
| Me | 5.00 | 6.00 | 5.00 | 6.00 | 5.00 | |
| IQR | 3.00 | 2.00 | 2.00 | 1.00 | 2.00 |
| CG | OLP | OL | OED | OSCC | p | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n = 9 (%) | n = 13 (%) | n = 16 (%) | n= 7 (%) | n = 9 (%) | |||||||
| Age | 0.56 * | ||||||||||
| Me (QR) | 58.00 (29.00) | 54.00 (37.00) | 59.50 (43.00) | 61.00 (31.00) | 63.00 (49.00) | ||||||
| M (SD) | 58.11 (10.07) | 56.00 (12.32) | 60.75 (10.51) | 66.14 (11.98) | 61.00 (13.69) | ||||||
| Sex | 0.58 ** | ||||||||||
| Male | 4 | (44.4) | 6 | (46.2) | 6 | (37.5) | 2 | (28.6) | 6 | (66.7) | |
| Female | 5 | (55.6) | 7 | (53.8) | 10 | (62.5) | 5 | (71.4) | 3 | (33.3) | |
| Cigarette use | 0.6 ** | ||||||||||
| Current | 3 | (33.3) | 3 | (23.1) | 8 | (50.0) | 2 | (28.6) | 5 | (55.6) | |
| Past | 3 | (33.3) | 2 | (15.4) | 4 | (25.0) | 2 | (28.6) | 1 | (11.1) | |
| Never | 3 | (33.3) | 8 | (61.5) | 4 | (25.0) | 3 | (42.9) | 3 | (33.3) | |
| Alcohol use | 0.3 ** | ||||||||||
| Regular | 0 | (0.0) | 3 | (23.1) | 4 | (25.0) | 0 | (0.0) | 1 | (11.1) | |
| Occasional | 9 | (100.0) | 10 | (76.9) | 12 | (75.0) | 7 | (100.0) | 8 | (88.9) | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Babiuch, K.; Kuśnierz-Cabala, B.; Kęsek, B.; Okoń, K.; Darczuk, D.; Chomyszyn-Gajewska, M. Evaluation of Proinflammatory, NF-kappaB Dependent Cytokines: IL-1α, IL-6, IL-8, and TNF-α in Tissue Specimens and Saliva of Patients with Oral Squamous Cell Carcinoma and Oral Potentially Malignant Disorders. J. Clin. Med. 2020, 9, 867. https://doi.org/10.3390/jcm9030867
Babiuch K, Kuśnierz-Cabala B, Kęsek B, Okoń K, Darczuk D, Chomyszyn-Gajewska M. Evaluation of Proinflammatory, NF-kappaB Dependent Cytokines: IL-1α, IL-6, IL-8, and TNF-α in Tissue Specimens and Saliva of Patients with Oral Squamous Cell Carcinoma and Oral Potentially Malignant Disorders. Journal of Clinical Medicine. 2020; 9(3):867. https://doi.org/10.3390/jcm9030867
Chicago/Turabian StyleBabiuch, Karolina, Beata Kuśnierz-Cabala, Barbara Kęsek, Krzysztof Okoń, Dagmara Darczuk, and Maria Chomyszyn-Gajewska. 2020. "Evaluation of Proinflammatory, NF-kappaB Dependent Cytokines: IL-1α, IL-6, IL-8, and TNF-α in Tissue Specimens and Saliva of Patients with Oral Squamous Cell Carcinoma and Oral Potentially Malignant Disorders" Journal of Clinical Medicine 9, no. 3: 867. https://doi.org/10.3390/jcm9030867
APA StyleBabiuch, K., Kuśnierz-Cabala, B., Kęsek, B., Okoń, K., Darczuk, D., & Chomyszyn-Gajewska, M. (2020). Evaluation of Proinflammatory, NF-kappaB Dependent Cytokines: IL-1α, IL-6, IL-8, and TNF-α in Tissue Specimens and Saliva of Patients with Oral Squamous Cell Carcinoma and Oral Potentially Malignant Disorders. Journal of Clinical Medicine, 9(3), 867. https://doi.org/10.3390/jcm9030867