Potential Salivary mRNA Biomarkers for Early Detection of Oral Cancer


 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Saliva Collection
2.2. Total RNA Extraction
2.3. Primary Candidate Genes and Real-Time PCR (qPCR)
2.4. Comparison with NCI GEO Datasets
2.5. Statistical Analysis
3. Results
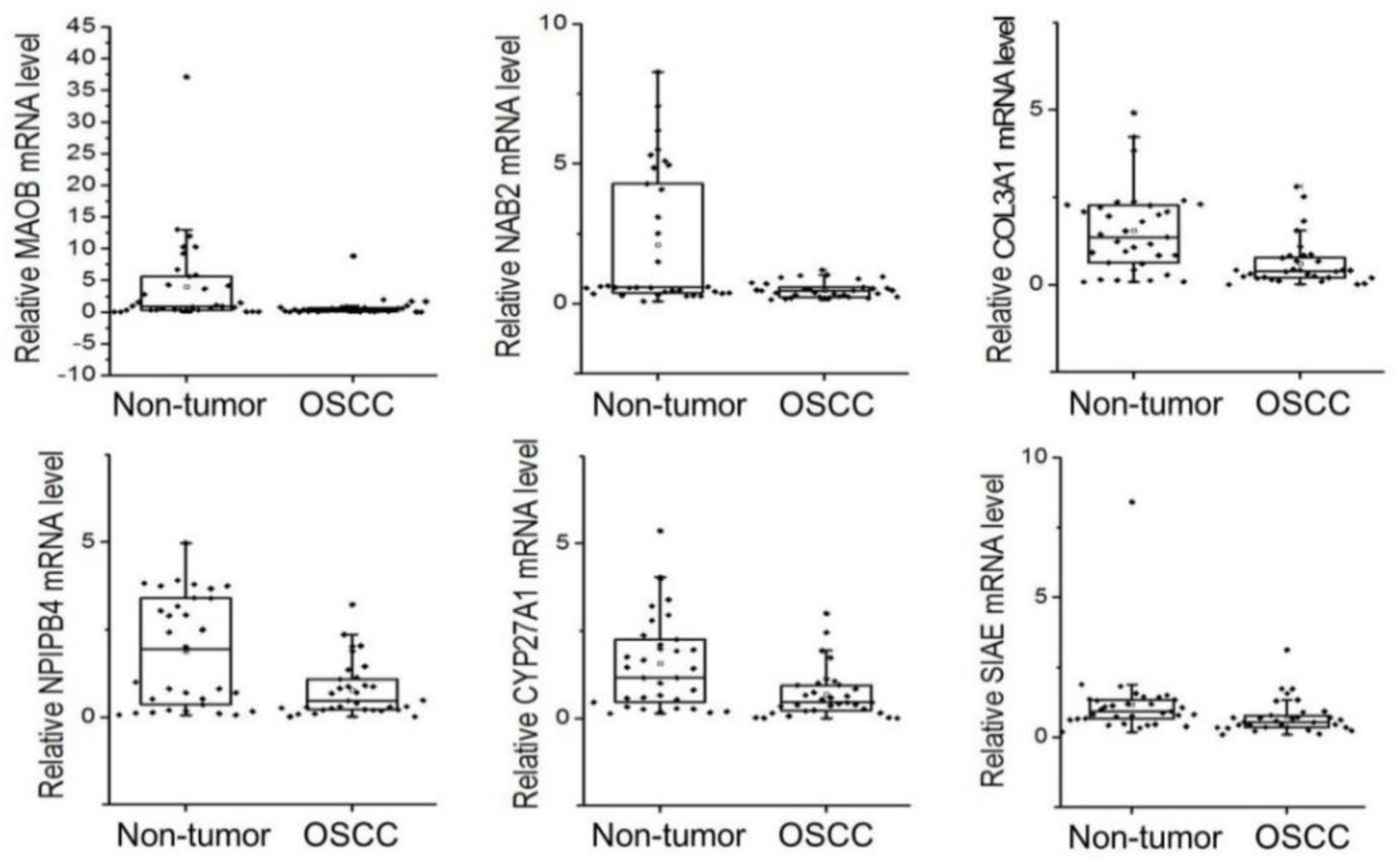
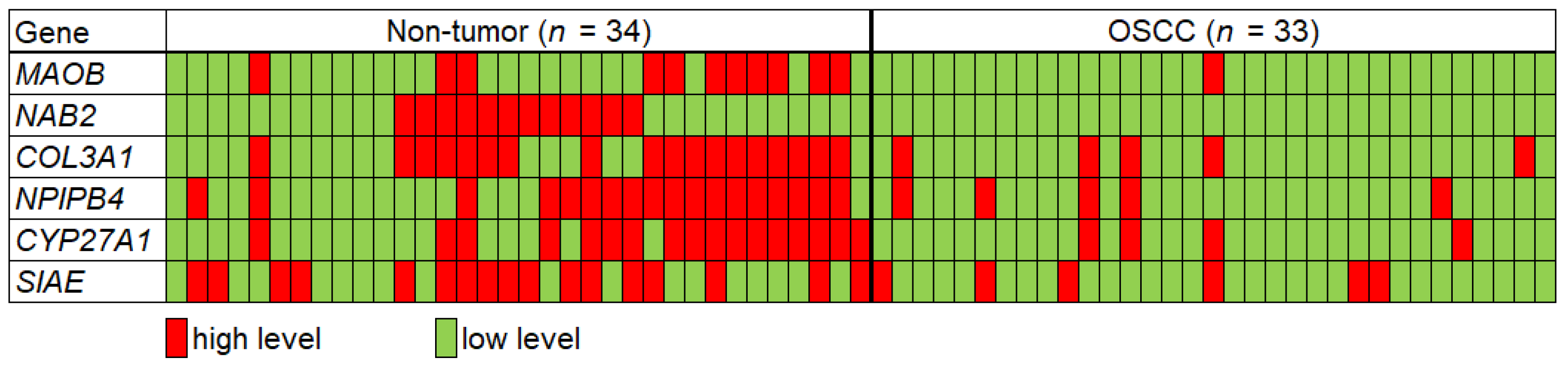
3.1. Candidate mRNA Levels in Saliva from Non-Tumor Control and OSCC Groups
3.2. AUC Analysis with Individual or Combinations of Candidate mRNAs
3.3. AUC Analysis of Subjects under 60 Years of Age in Both Groups
3.4. Expression Profiles of the Candidate Biomarkers in Tumor Tissue Datasets
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Wu, L.; Qu, X. Cancer biomarker detection: Recent achievements and challenges. Chem. Soc. Rev. 2015, 44, 2963–2997. [Google Scholar] [CrossRef] [PubMed]
- Afrifa, J.; Zhao, T.; Yu, J. Circulating mitochondria DNA, a non-invasive cancer diagnostic biomarker candidate. Mitochondrion 2019, 47, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Mercado, M.; Manterola, L.; Larrea, E.; Goicoechea, I.; Arestin, M.; Armesto, M.; Otaegui, D.; Lawrie, C.H. The circulating transcriptome as a source of non-invasive cancer biomarkers: Concepts and controversies of non-coding and coding RNA in body fluids. J. Cell. Mol. Med. 2015, 19, 2307–2323. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Li, X.; Yang, M.; Xu, L.; Deng, S.; Ran, L. Prediction of biomarkers of oral squamous cell carcinoma using microarray technology. Sci. Rep. 2017, 7, 42105. [Google Scholar] [CrossRef]
- Khurshid, Z.; Zafar, M.S.; Khan, R.S.; Najeeb, S.; Slowey, P.D.; Rehman, I.U. Role of Salivary Biomarkers in Oral Cancer Detection. Adv. Clin. Chem. 2018, 86, 23–70. [Google Scholar] [CrossRef]
- Radhika, T.; Jeddy, N.; Nithya, S.; Muthumeenakshi, R.M. Salivary biomarkers in oral squamous cell carcinoma—An insight. J. Oral. Biol. Craniofac. Res. 2016, 6, S51–S54. [Google Scholar] [CrossRef]
- Wu, J.Y.; Yi, C.; Chung, H.R.; Wang, D.J.; Chang, W.C.; Lee, S.Y.; Lin, C.T.; Yang, Y.C.; Yang, W.C. Potential biomarkers in saliva for oral squamous cell carcinoma. Oral. Oncol. 2010, 46, 226–231. [Google Scholar] [CrossRef]
- Gualtero, D.F.; Suarez Castillo, A. Biomarkers in saliva for the detection of oral squamous cell carcinoma and their potential use for early diagnosis: A systematic review. Acta Odontol. Scand. 2016, 74, 170–177. [Google Scholar] [CrossRef]
- Stuani, V.T.; Rubira, C.M.; Sant’Ana, A.C.; Santos, P.S. Salivary biomarkers as tools for oral squamous cell carcinoma diagnosis: A systematic review. Head Neck 2017, 39, 797–811. [Google Scholar] [CrossRef]
- Cheng, Y.L.; Jordan, L.; Chen, H.S.; Kang, D.; Oxford, L.; Plemons, J.; Parks, H.; Rees, T. Chronic periodontitis can affect the levels of potential oral cancer salivary mRNA biomarkers. J. Periodonta Res. 2017, 52, 428–437. [Google Scholar] [CrossRef]
- Horvath, J.; Szabo, A.; Tar, I.; Dezso, B.; Kiss, C.; Marton, I.; Scholtz, B. Oral Health May Affect the Performance of mRNA-Based Saliva Biomarkers for Oral Squamous Cell Cancer. Pathol. Oncol. Res. 2018, 24, 833–842. [Google Scholar] [CrossRef] [PubMed]
- Moraes, R.C.; Dias, F.L.; Figueredo, C.M.; Fischer, R.G. Association between Chronic Periodontitis and Oral/Oropharyngeal Cancer. Braz. Dent. J. 2016, 27, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Javed, F.; Warnakulasuriya, S. Is there a relationship between periodontal disease and oral cancer? A systematic review of currently available evidence. Crit. Rev. Oncol. Hematol. 2016, 97, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Allavena, P.; Sica, A.; Balkwill, F. Cancer-related inflammation. Nature 2008, 454, 436–444. [Google Scholar] [CrossRef] [PubMed]
- SahebJamee, M.; Eslami, M.; AtarbashiMoghadam, F.; Sarafnejad, A. Salivary concentration of TNFalpha, IL1 alpha, IL6, and IL8 in oral squamous cell carcinoma. Med. Oral. Patol. Oral. Cir. Bucal. 2008, 13, E292–E295. [Google Scholar] [PubMed]
- Yan, L.; Tian, L.; Liu, S. Combining large number of weak biomarkers based on AUC. Stat. Med. 2015, 34, 3811–3830. [Google Scholar] [CrossRef]
- Soreide, K. Receiver-operating characteristic curve analysis in diagnostic, prognostic and predictive biomarker research. J. Clin. Pathol. 2009, 62, 1–5. [Google Scholar] [CrossRef]
- Hajian-Tilaki, K. Receiver Operating Characteristic (ROC) Curve Analysis for Medical Diagnostic Test Evaluation. Caspian J. Intern. Med. 2013, 4, 627–635. [Google Scholar]
- Shapiro, D.E. The interpretation of diagnostic tests. Stat. Methods Med. Res. 1999, 8, 113–134. [Google Scholar] [CrossRef]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89 (Suppl. S1), S173–S182. [Google Scholar] [CrossRef]
- Allanach, K.; Mengel, M.; Einecke, G.; Sis, B.; Hidalgo, L.G.; Mueller, T.; Halloran, P.F. Comparing microarray versus RT-PCR assessment of renal allograft biopsies: Similar performance despite different dynamic ranges. Am. J. Transplant. 2008, 8, 1006–1015. [Google Scholar] [CrossRef] [PubMed]
- Rajeevan, M.S.; Ranamukhaarachchi, D.G.; Vernon, S.D.; Unger, E.R. Use of real-time quantitative PCR to validate the results of cDNA array and differential display PCR technologies. Methods 2001, 25, 443–451. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; St John, M.A.; Zhou, X.; Kim, Y.; Sinha, U.; Jordan, R.C.; Eisele, D.; Abemayor, E.; Elashoff, D.; Park, N.H.; et al. Salivary transcriptome diagnostics for oral cancer detection. Clin. Cancer Res. 2004, 10, 8442–8450. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zhou, X.; St John, M.A.; Wong, D.T. RNA profiling of cell-free saliva using microarray technology. J. Dent. Res. 2004, 83, 199–203. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Sun, S.; Zeng, X.; Cui, L. Expression profiles analysis identifies a novel three-mRNA signature to predict overall survival in oral squamous cell carcinoma. Am. J. Cancer Res. 2018, 8, 450–461. [Google Scholar]
- Grunkemeier, G.L.; Jin, R. Receiver operating characteristic curve analysis of clinical risk models. Ann. Thorac. Surg. 2001, 72, 323–326. [Google Scholar] [CrossRef]
- Pepe, M.S.; Thompson, M.L. Combining diagnostic test results to increase accuracy. Biostatistics 2000, 1, 123–140. [Google Scholar] [CrossRef]
- McGrath, S.; Christidis, D.; Perera, M.; Hong, S.K.; Manning, T.; Vela, I.; Lawrentschuk, N. Prostate cancer biomarkers: Are we hitting the mark? Prostate Int. 2016, 4, 130–135. [Google Scholar] [CrossRef]
- Tozzoli, R.; D’Aurizio, F.; Falcomer, F.; Basso, S.M.; Lumachi, F. Serum Tumor Markers in Stage I-II Breast Cancer. Med. Chem. 2016, 12, 285–289. [Google Scholar] [CrossRef]
- Zhou, D.; Tang, W.; Liu, X.; An, H.X.; Zhang, Y. Clinical verification of plasma messenger RNA as novel noninvasive biomarker identified through bioinformatics analysis for lung cancer. Oncotarget 2017, 8, 43978–43989. [Google Scholar] [CrossRef][Green Version]
- Wang, Y.; Zhang, J.; Xiao, X.; Liu, H.; Wang, F.; Li, S.; Wen, Y.; Wei, Y.; Su, J.; Zhang, Y. The identification of age-associated cancer markers by an integrative analysis of dynamic DNA methylation changes. Sci. Rep. 2016, 6, 22722. [Google Scholar] [CrossRef] [PubMed]
- Lewinsohn, R.; Glover, V.; Sandler, M. Beta-phenylethylamine and benzylamine as substrates for human monoamine oxidase A: A source of some anomalies? Biochem. Pharmacol. 1980, 29, 777–781. [Google Scholar] [CrossRef]
- Sharpe, M.A.; Baskin, D.S. Monoamine oxidase B levels are highly expressed in human gliomas and are correlated with the expression of HiF-1alpha and with transcription factors Sp1 and Sp3. Oncotarget 2016, 7, 3379–3393. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.H.; Huang, B.; Shieh, T.Y.; Wang, Y.H.; Chen, Y.K.; Wu, J.H.; Huang, J.H.; Chen, C.C.; Lee, K.W. The influence of monoamine oxidase variants on the risk of betel quid-associated oral and pharyngeal cancer. Sci. World J. 2014, 2014, 183548. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.Y.; Oh, S.Y.; Kang, S.H.; Kang, S.M.; Kim, J.; Lee, H.J.; Kwon, T.G.; Kim, J.W.; Hong, S.H. NAB 2-Expressing Cancer-Associated Fibroblast Promotes HNSCC Progression. Cancers 2019, 11, 388. [Google Scholar] [CrossRef]
- Abdulkadir, S.A.; Carbone, J.M.; Naughton, C.K.; Humphrey, P.A.; Catalona, W.J.; Milbrandt, J. Frequent and early loss of the EGR1 corepressor NAB2 in human prostate carcinoma. Hum. Pathol. 2001, 32, 935–939. [Google Scholar] [CrossRef]
- Kartha, V.K.; Stawski, L.; Han, R.; Haines, P.; Gallagher, G.; Noonan, V.; Kukuruzinska, M.; Monti, S.; Trojanowska, M. PDGFRbeta Is a Novel Marker of Stromal Activation in Oral Squamous Cell Carcinomas. PLoS ONE 2016, 11, e0154645. [Google Scholar] [CrossRef]
- Yuan, L.; Shu, B.; Chen, L.; Qian, K.; Wang, Y.; Qian, G.; Zhu, Y.; Cao, X.; Xie, C.; Xiao, Y.; et al. Overexpression of COL3A1 confers a poor prognosis in human bladder cancer identified by co-expression analysis. Oncotarget 2017, 8, 70508–70520. [Google Scholar] [CrossRef]
- Kimbung, S.; Chang, C.Y.; Bendahl, P.O.; Dubois, L.; Thompson, J.W.; McDonnell, D.P.; Borgquist, S. Impact of 27-hydroxylase (CYP27A1) and 27-hydroxycholesterol in breast cancer. Endocr. Relat. Cancer 2017, 24, 339–349. [Google Scholar] [CrossRef]
- Surolia, I.; Pirnie, S.P.; Chellappa, V.; Taylor, K.N.; Cariappa, A.; Moya, J.; Liu, H.; Bell, D.W.; Driscoll, D.R.; Diederichs, S.; et al. Functionally defective germline variants of sialic acid acetylesterase in autoimmunity. Nature 2010, 466, 243–247. [Google Scholar] [CrossRef]
- Sinha, D.; Mandal, C.; Bhattacharya, D.K. Identification of 9-O acetyl sialoglycoconjugates (9-OAcSGs) as biomarkers in childhood acute lymphoblastic leukemia using a lectin, AchatininH, as a probe. Leukemia 1999, 13, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Ritter, G.; Boosfeld, E.; Markstein, E.; Yu, R.K.; Ren, S.L.; Stallcup, W.B.; Oettgen, H.F.; Old, L.J.; Livingston, P.O. Biochemical and serological characteristics of natural 9-O-acetyl GD3 from human melanoma and bovine buttermilk and chemically O-acetylated GD3. Cancer Res. 1990, 50, 1403–1410. [Google Scholar] [PubMed]
- Marquina, G.; Waki, H.; Fernandez, L.E.; Kon, K.; Carr, A.; Valiente, O.; Perez, R.; Ando, S. Gangliosides expressed in human breast cancer. Cancer Res. 1996, 56, 5165–5171. [Google Scholar] [PubMed]
- Linkov, F.; Lisovich, A.; Yurkovetsky, Z.; Marrangoni, A.; Velikokhatnaya, L.; Nolen, B.; Winans, M.; Bigbee, W.; Siegfried, J.; Lokshin, A.; et al. Early detection of head and neck cancer: Development of a novel screening tool using multiplexed immunobead-based biomarker profiling. Cancer Epidemiol. Biomark. Prev. 2007, 16, 102–107. [Google Scholar] [CrossRef] [PubMed]
- English, P.A.; Williams, J.A.; Martini, J.F.; Motzer, R.J.; Valota, O.; Buller, R.E. A case for the use of receiver operating characteristic analysis of potential clinical efficacy biomarkers in advanced renal cell carcinoma. Future Oncol. 2016, 12, 175–182. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Non-Tumor | OSCC | p Value | |
|---|---|---|---|---|
| Number | 34 | 33 | ||
| Age | Mean ± SD | 53.2 ± 17.4 | 61.2 ± 18.1 | 0.007 |
| Range | 25–83 | 24–97 | ||
| Gender | Male | 15 | 22 | 0.07 |
| Female | 19 | 11 | ||
| Mild periodontitis | Yes | 3 | 10 | 0.02 |
| No | 31 | 23 | ||
| Smoking | Yes 1 | 9 | 9 | 0.94 |
| No 2 | 25 | 24 | ||
| Alcohol history | Yes 3 | 13 | 11 | 0.67 |
| No | 21 | 22 | ||
| Gene | Non-Tumor (ΔΔCt ± SD) | OSCC (ΔΔCt ± SD) | Relative Fold Change (OSCC/Non-Tumor) | p Value | ΔΔCt for Cancer Diagnosis (Non-Tumor−SD) |
|---|---|---|---|---|---|
| MAOB | 4.01 ± 1.20 | 0.70 ± 0.27 | 0.18 | 0.0009 | below 2.80 |
| NAB2 | 2.11 ± 0.42 | 0.49 ± 0.05 | 0.23 | 0.0023 | below 1.69 |
| COL3A1 | 1.55 ± 0.20 | 0.62 ± 0.12 | 0.4 | 0.0002 | below 1.35 |
| NPIPB4 | 1.89 ± 0.26 | 0.77 ± 0.14 | 0.41 | 0.0059 | below 1.62 |
| CYP27A1 | 1.57 ± 0.23 | 0.68 ± 0.12 | 0.44 | 0.0016 | below 1.34 |
| SIAE | 1.18 ± 0.24 | 0.73 ± 0.11 | 0.62 | 0.0370 | below 0.94 |
| Gene No. | Gene(s) | Sensitivity | Specificity | AUC | 95% CI |
|---|---|---|---|---|---|
| One gene | MAOB | 0.97 | 0.35 | 0.63 | 0.44–0.82 |
| NAB2 | 1 | 0.35 | 0.69 | 0.45–0.95 | |
| COL3A1 | 0.85 | 0.53 | 0.67 | 0.47–0.79 | |
| NPIPB4 | 0.85 | 0.53 | 0.64 | 0.47–0.79 | |
| CYP27A1 | 0.88 | 0.5 | 0.64 | 0.43–0.82 | |
| SIAE | 0.79 | 0.5 | 0.7 | 0.56–0.92 | |
| Two genes | MAOB + NAB2 | 0.97 | 0.62 | 0.8 | 0.52–1.0 |
| MAOB + SIAE | 0.82 | 0.76 | 0.76 | 0.63–0.94 | |
| NAB2 + CYP27A1 | 0.88 | 0.71 | 0.81 | 0.70–0.95 | |
| NAB2 + SIAE | 0.82 | 0.59 | 0.78 | 0.62–0.97 | |
| COL3A1 + SIAE | 0.7 | 0.76 | 0.74 | 0.59–0.91 | |
| CYP27A1 + SIAE | 0.73 | 0.8 | 0.84 | 0.67–1.0 |
| Gene No. | Gene (s) | Age < 60 | Age ≥ 60 | ||||
|---|---|---|---|---|---|---|---|
| Sensitivity | Specificity | AUC | Sensitivity | Specificity | AUC | ||
| One gene | MAOB | 0.92 | 0.43 | 0.74 | 1.0 | 0.43 | 0.56 |
| NAB2 | 1.0 | 0.43 | 0.70 | 1.0 | 0.23 | 0.63 | |
| COL3A1 | 0.77 | 0.71 | 0.73 | 0.88 | 0.15 | 0.38 | |
| NPIPB4 | 0.69 | 0.62 | 0.68 | 0.94 | 0.39 | 0.69 | |
| CYP27A1 | 0.77 | 0.62 | 0.73 | 0.94 | 0.31 | 0.56 | |
| SIAE | 0.70 | 0.52 | 0.68 | 0.94 | 0.46 | 0.69 | |
| Two genes | MAOB + NAB2 | 0.92 | 0.86 | 0.91 | 1.0 | 0.39 | 0.69 |
| MAOB + SIAE | 0.70 | 0.76 | 0.83 | 0.88 | 0.46 | 0.70 | |
| NAB2 + CYP27A1 | 0.77 | 0.86 | 0.88 | 1.0 | 0.38 | 0.69 | |
| NAB2 + SIAE | 0.69 | 0.62 | 0.69 | 0.88 | 0.54 | 0.77 | |
| COL3A1 + SIAE | 0.54 | 0.91 | 0.79 | 0.82 | 0.54 | 0.67 | |
| CYP27A1 + SIAE | 0.54 | 0.9 | 0.82 | 0.88 | 0.62 | 0.72 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, S.Y.; Kang, S.-M.; Kang, S.H.; Lee, H.-J.; Kwon, T.-G.; Kim, J.-W.; Lee, S.-T.; Choi, S.-Y.; Hong, S.-H. Potential Salivary mRNA Biomarkers for Early Detection of Oral Cancer. J. Clin. Med. 2020, 9, 243. https://doi.org/10.3390/jcm9010243
Oh SY, Kang S-M, Kang SH, Lee H-J, Kwon T-G, Kim J-W, Lee S-T, Choi S-Y, Hong S-H. Potential Salivary mRNA Biomarkers for Early Detection of Oral Cancer. Journal of Clinical Medicine. 2020; 9(1):243. https://doi.org/10.3390/jcm9010243
Chicago/Turabian StyleOh, Su Young, Sung-Min Kang, Soo Hyun Kang, Heon-Jin Lee, Tae-Geon Kwon, Jin-Wook Kim, Sung-Tak Lee, So-Young Choi, and Su-Hyung Hong. 2020. "Potential Salivary mRNA Biomarkers for Early Detection of Oral Cancer" Journal of Clinical Medicine 9, no. 1: 243. https://doi.org/10.3390/jcm9010243
APA StyleOh, S. Y., Kang, S.-M., Kang, S. H., Lee, H.-J., Kwon, T.-G., Kim, J.-W., Lee, S.-T., Choi, S.-Y., & Hong, S.-H. (2020). Potential Salivary mRNA Biomarkers for Early Detection of Oral Cancer. Journal of Clinical Medicine, 9(1), 243. https://doi.org/10.3390/jcm9010243