Urine E-cadherin: A Marker for Early Detection of Kidney Injury in Diabetic Patients

 ,
,  , ,
, ,  ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
Patients
2.2. Sample Collection and Handling
2.3. Depletion of High Abundant Proteins
2.4. Protein Precipitation and Concentration Estimation
2.5. Two-Dimensional Difference In-Gel Electrophoresis (2D-DIGE)
2.6. In Gel Digestion and Protein Identification from 2D-DIGE
2.7. Filter Aided Sample Prep (FASP)
2.8. Mass Spectrometry Analysis of the Extracted Tryptic Peptides from FASP and Spectral Counts Quantification
2.9. Mass Spectrometry and Label-Free Quantification of the Extracted Tryptic Peptides from FASP
2.10. Western Blot Analysis
2.11. Dot Blot Analysis
2.12. ELISA-Analysis to Validate the Prognosis Value of the Biomarker
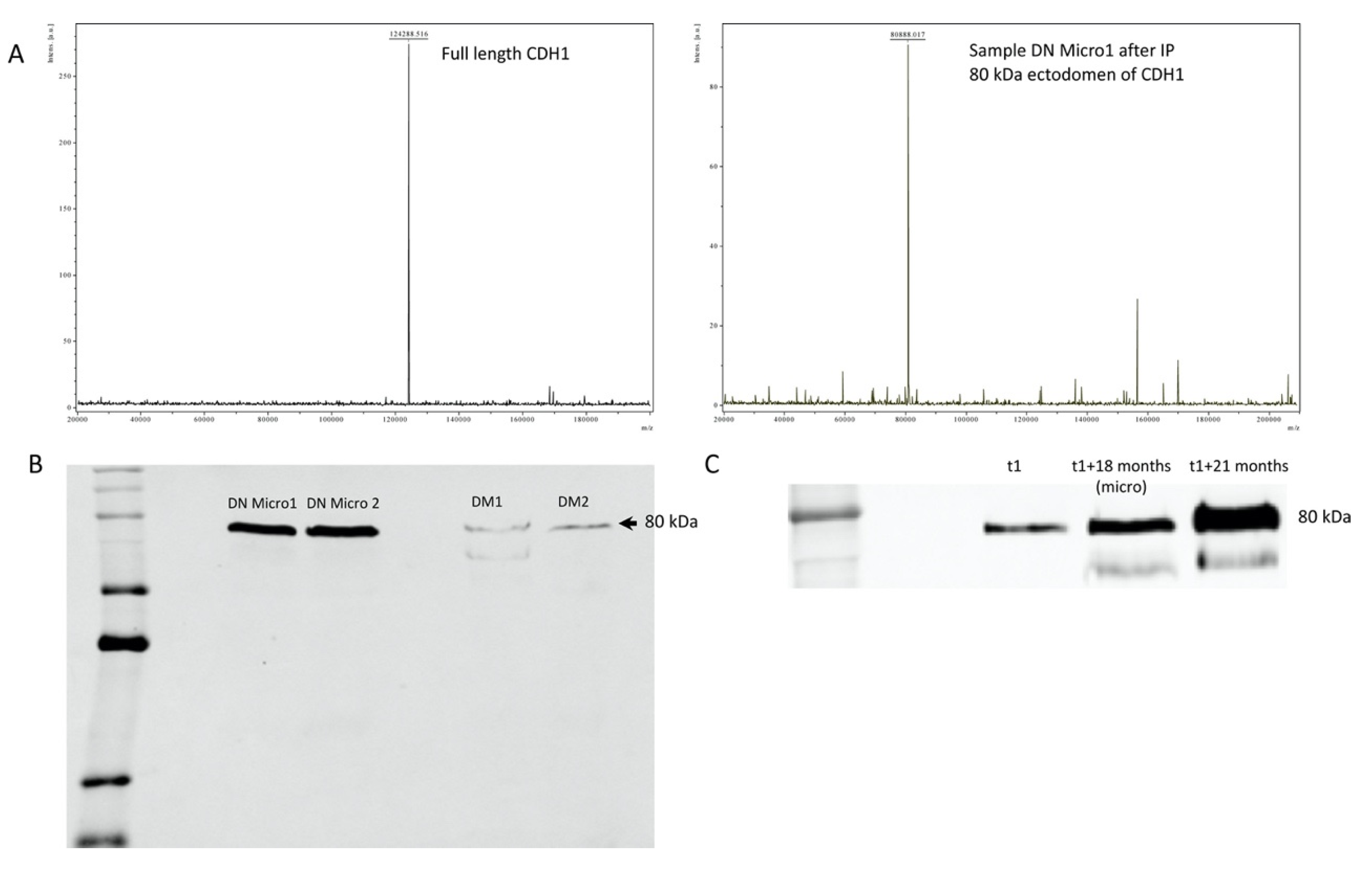
2.13. Protein Immunoprecipitation and MALDI-TOF Mass Spectrometry Analysis
2.14. Statistical Methods
3. Results
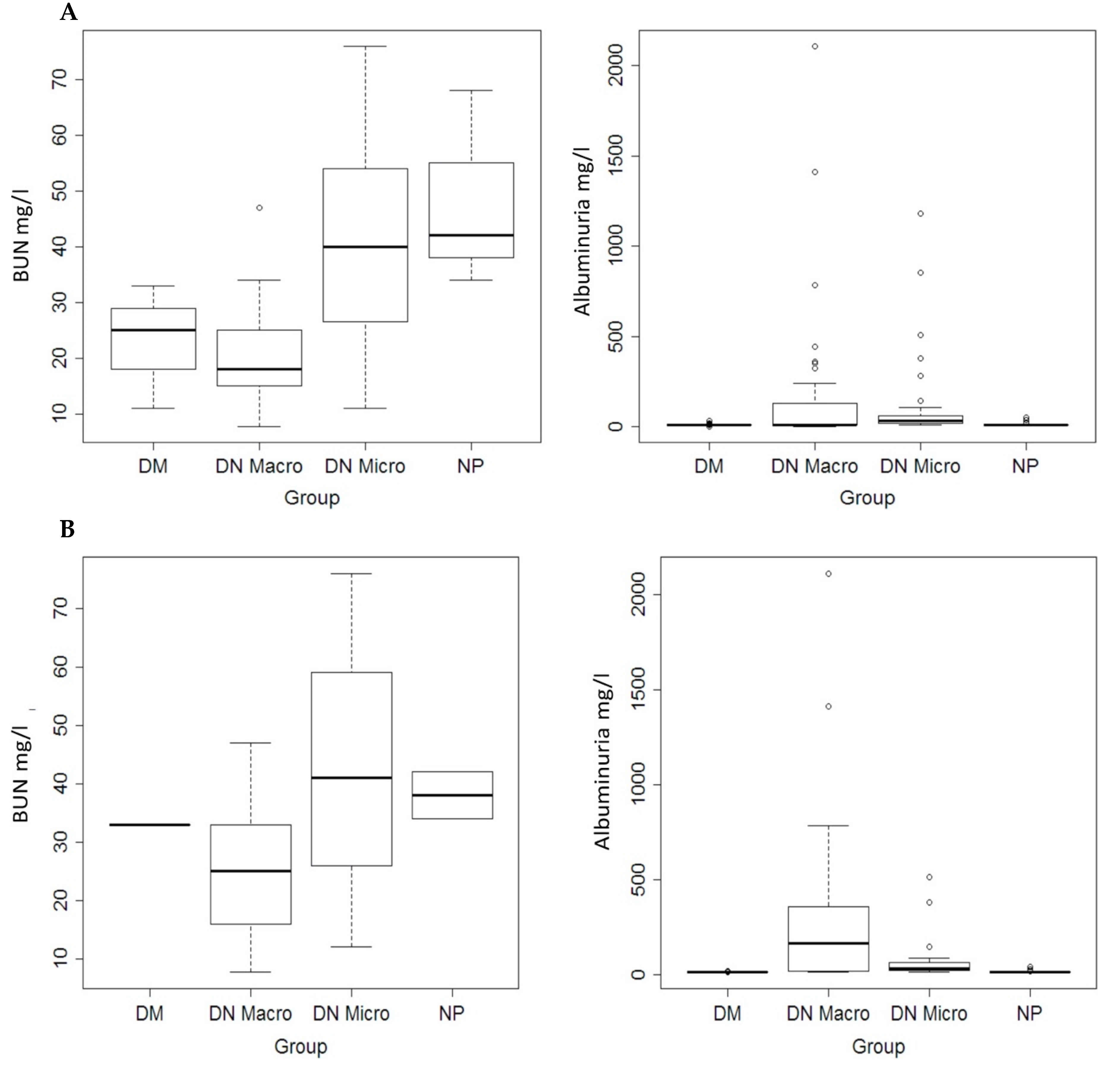
3.1. Clinical Parameters and Medications
3.2. Effect of Depletion of High Abundant Proteins
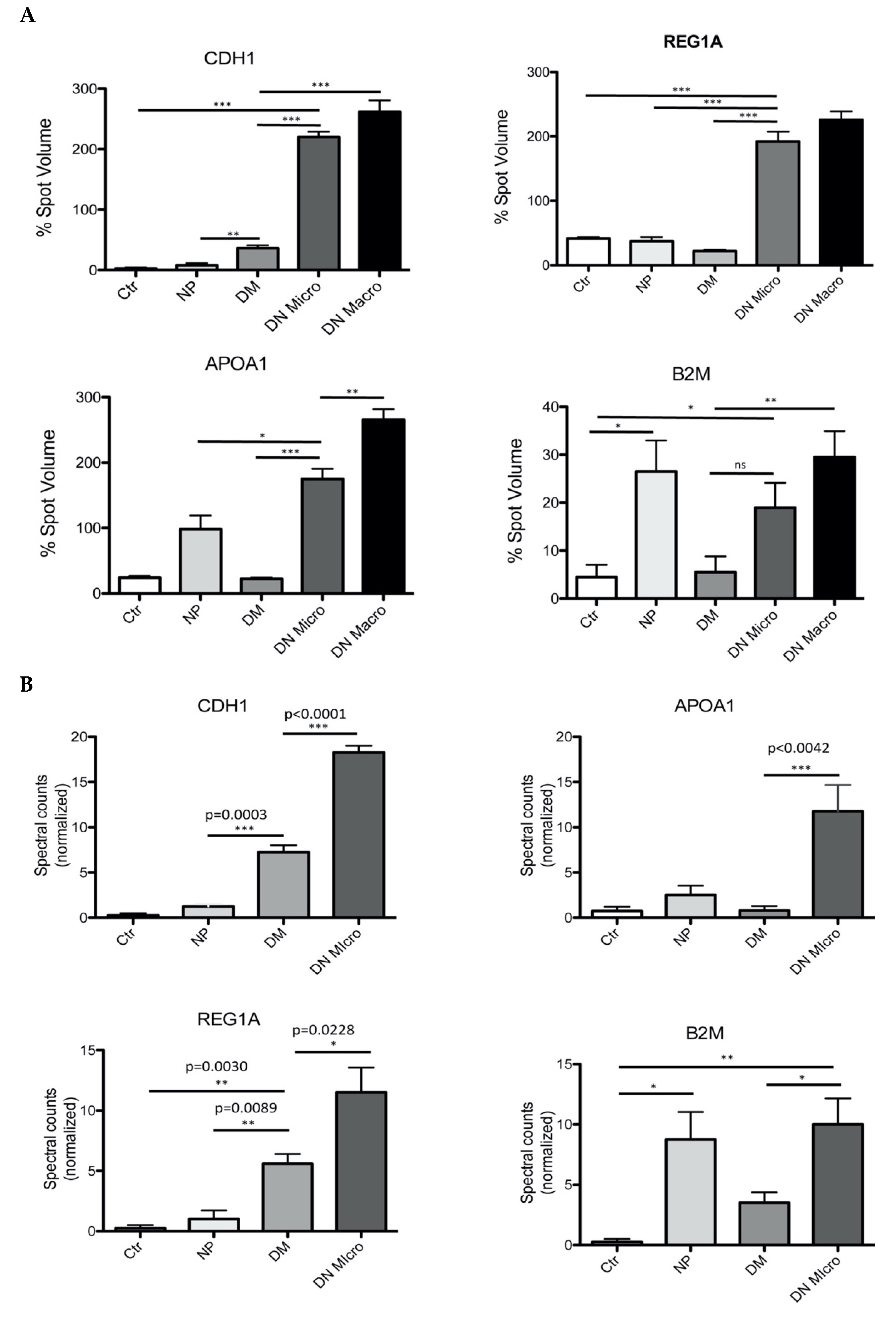
3.3. Mapping DM-NP Urine Proteome and Identification of Potential Proteins Markers
3.4. Filter-Aided Sample Preparation (FASP) of the Urinary Proteome and MS-Based Analysis of the Potential Marker Identified by 2D-DIGE
3.5. Immunological Validation of the Four Identified Protein Markers
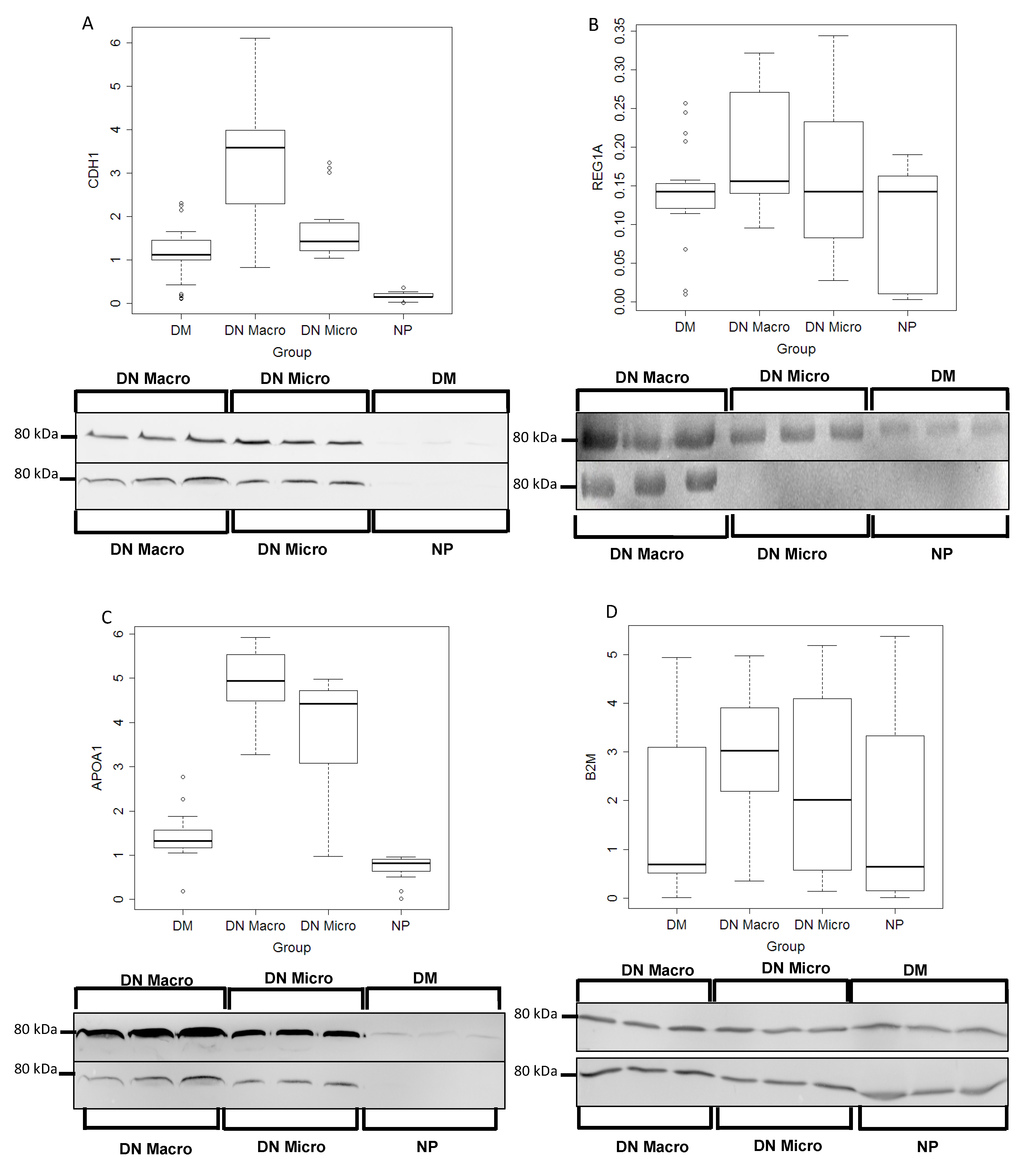
3.5.1. Western Blot Validation
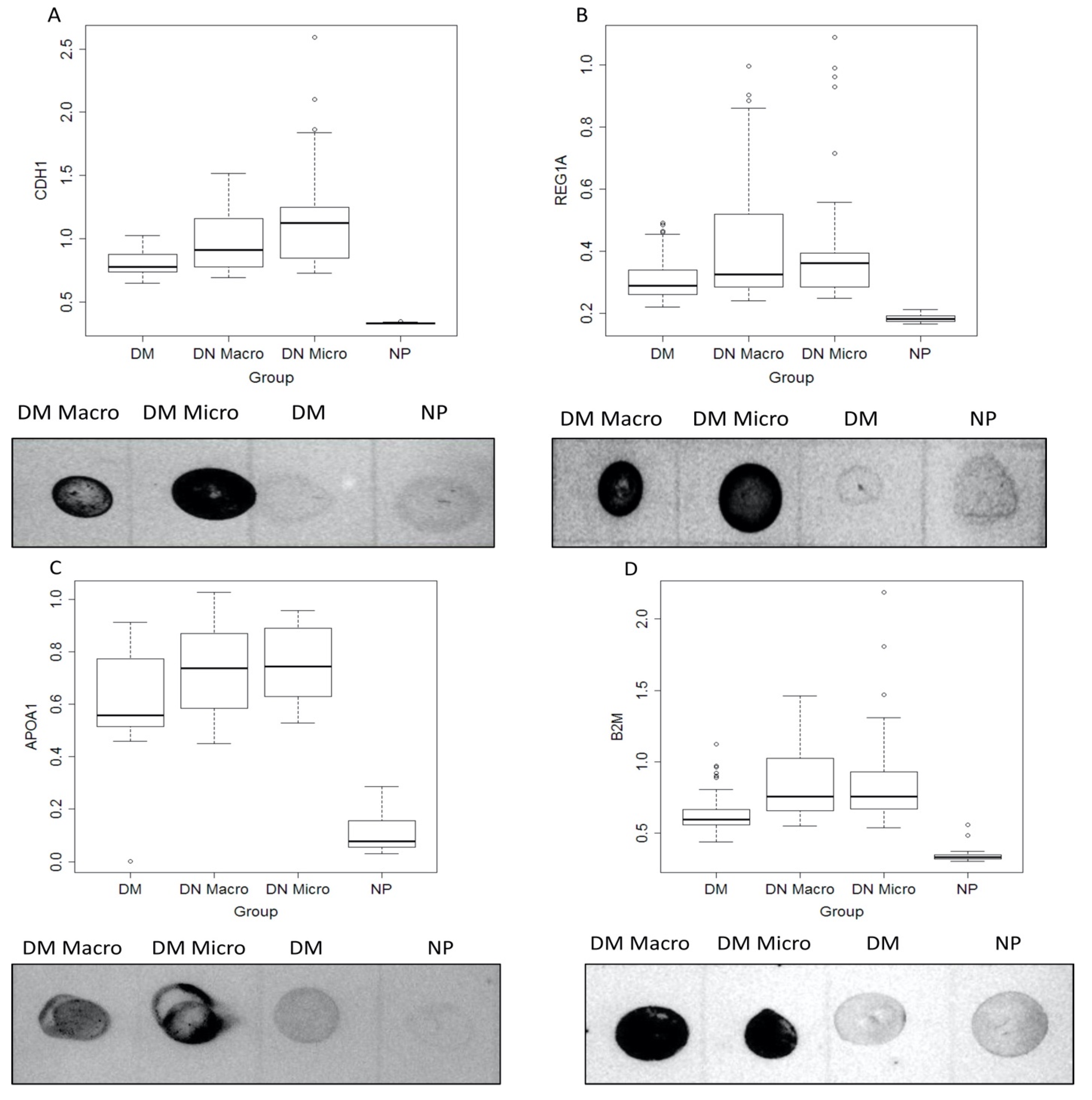
3.5.2. Dot Blot Validation of the Identified Markers
3.5.3. Individual Diagnostic Power
3.5.4. Combination of Parameters
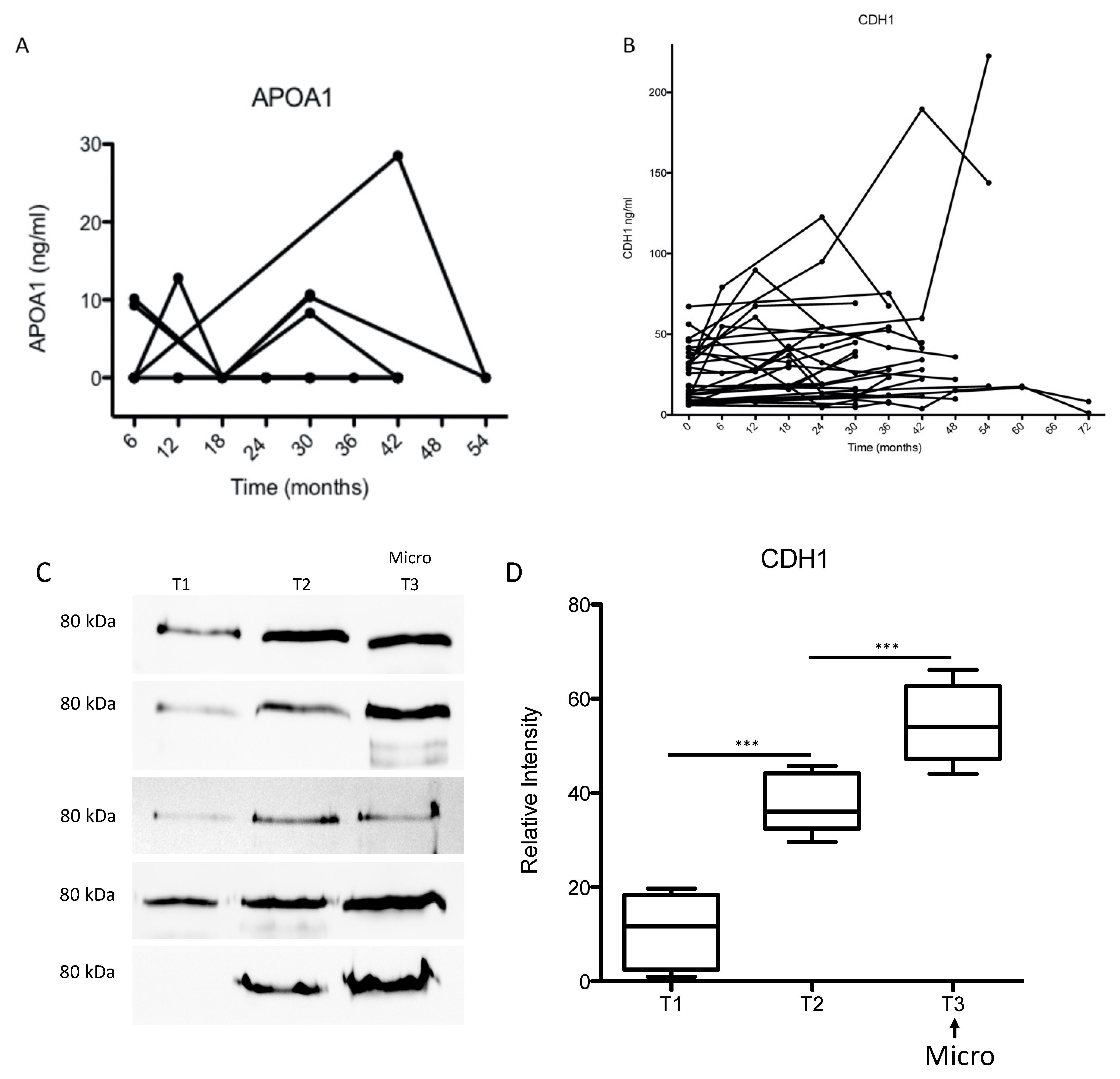
3.6. Longitudinal Study
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ogurtsova, K.; da Rocha Fernandes, J.D.; Huang, Y.; Linnenkamp, U.; Guariguata, L.; Cho, N.H.; Cavan, D.; Shaw, J.E.; Makaroff, L.E. IDF Diabetes Atlas: Global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res. Clin. Pract. 2017, 128, 40–50. [Google Scholar] [CrossRef] [PubMed]
- Alicic, R.Z.; Rooney, M.T.; Tuttle, K.R. Diabetic Kidney Disease: Challenges, Progress, and Possibilities. Clin. J. Am. Soc. Nephrol. CJASN 2017, 12, 2032–2045. [Google Scholar] [CrossRef] [PubMed]
- Rocha, N.A.; McCullough, P.A. Cardiovascular outcomes in diabetic kidney disease: Insights from recent clinical trials. Kidney Int. Suppl. 2018, 8, 8–17. [Google Scholar] [CrossRef]
- Afkarian, M.; Katz, R.; Bansal, N.; Correa, A.; Kestenbaum, B.; Himmelfarb, J.; De Boer, I.H.; Young, B. Diabetes, Kidney Disease, and Cardiovascular Outcomes in the Jackson Heart Study. Clin. J. Am. Soc. Nephrol. CJASN 2016, 11, 1384–1391. [Google Scholar] [CrossRef] [PubMed]
- Afkarian, M.; Sachs, M.; Kestenbaum, B.; Hirsch, I.B.; Tuttle, K.R.; Himmelfarb, J.; De Boer, I.H. Kidney Disease and Increased Mortality Risk in Type 2 Diabetes. J. Am. Soc. Nephrol. JASN 2013, 24, 302–308. [Google Scholar] [CrossRef]
- Persson, F.; Lindhardt, M.; Rossing, P.; Parving, H.-H. Prevention of microalbuminuria using early intervention with renin-angiotensin system inhibitors in patients with type 2 diabetes: A systematic review. J. Renin-Angiotensin-Aldosterone Syst. JRAAS 2016, 17. [Google Scholar] [CrossRef]
- Bilous, R.W.; Chaturvedi, N.; Sjølie, A.K.; Fuller, J.; Klein, A.P.; Orchard, T.; Porta, M.; Parving, H.-H. Effect of candesartan on microalbuminuria and albumin excretion rate in diabetes: Three randomized trials. Ann. Intern. Med. 2009, 151, 11–20. [Google Scholar] [CrossRef]
- Heart Outcomes Prevention Evaluation (HOPE) Study Investigators. Effects of ramipril on cardiovascular and microvascular outcomes in people with diabetes mellitus: Results of the HOPE study and MICRO-HOPE substudy. Lancet Lond. Engl. 2000, 355, 253–259. [Google Scholar] [CrossRef]
- Haller, H.; Ito, S.; Izzo, J.L.; Januszewicz, A.; Katayama, S.; Menne, J.; Mimran, A.; Rabelink, T.J.; Ritz, E.; Ruilope, L.; et al. Olmesartan for the Delay or Prevention of Microalbuminuria in Type 2 Diabetes. N. Engl. J. Med. 2011, 364, 907–917. [Google Scholar] [CrossRef]
- Ruggenenti, P.; Fassi, A.; Ilieva, A.P.; Bruno, S.; Iliev, I.P.; Brusegan, V.; Rubis, N.; Gherardi, G.; Arnoldi, F.; Ganeva, M.; et al. Preventing Microalbuminuria in Type 2 Diabetes. N. Engl. J. Med. 2004, 351, 1941–1951. [Google Scholar] [CrossRef]
- Patel, A.; ADVANCE Collaborative Group; MacMahon, S.; Chalmers, J.; Neal, B.; Woodward, M.; Billot, L. Effects of a fixed combination of perindopril and indapamide on macrovascular and microvascular outcomes in patients with type 2 diabetes mellitus (the ADVANCE trial): A randomised controlled trial. Lancet Lond. Engl. 2007, 370, 829–840. [Google Scholar] [CrossRef]
- Rossing, P.; Hougaard, P.; Parving, H.-H. Risk factors for development of incipient and overt diabetic nephropathy in type 1 diabetic patients: A 10-year prospective observational study. Diabetes Care 2002, 25, 859–864. [Google Scholar] [CrossRef] [PubMed]
- Zürbig, P.; Mischak, H. Capillary Electrophoresis Coupled to Mass Spectrometry for Biomarker Discovery and Diagnosis of Kidney Diseases. Contrib. Nephrol. 2008, 160, 107–126. [Google Scholar] [PubMed]
- Dihazi, H.; Müller, G.A.; Lindner, S.; Meyer, M.; Asif, A.R.; Oellerich, M.; Strutz, F. Characterization of Diabetic Nephropathy by Urinary Proteomic Analysis: Identification of a Processed Ubiquitin Form as a Differentially Excreted Protein in Diabetic Nephropathy Patients. Clin. Chem. 2007, 53, 1636–1645. [Google Scholar] [CrossRef] [PubMed]
- Colhoun, H.M.; Marcovecchio, M.L. Biomarkers of diabetic kidney disease. Diabetologia 2018, 61, 996–1011. [Google Scholar] [CrossRef]
- Jiang, H.; Guan, G.; Zhang, R.; Liu, G.; Cheng, J.; Hou, X.; Cui, Y. Identification of urinary soluble E-cadherin as a novel biomarker for diabetic nephropathy. Diabetes Metab. Res. Rev. 2009, 25, 232–241. [Google Scholar] [CrossRef]
- American Diabetes Association 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2018. Diabetes Care 2018, 41, S13–S27. [Google Scholar] [CrossRef]
- Dihazi, H.; Koziolek, M.; Datta, R.R.; Wallbach, M.; Jung, K.; Heise, D.; Dihazi, G.H.; Markovic, I.; Asif, A.R.; Müller, G.A. FABP1 and FABP3 Have High Predictive Values for Renal Replacement Therapy in Patients with Acute Kidney Injury. Blood Purif. 2016, 42, 202–213. [Google Scholar] [CrossRef]
- Bradford, M.M. A rapid and sensitive method for the quantitation of microgram quantities of protein utilizing the principle of protein-dye binding. Anal. Biochem. 1976, 72, 248–254. [Google Scholar] [CrossRef]
- Patzig, J.; Jahn, O.; Tenzer, S.; Wichert, S.P.; De Monasterio-Schrader, P.; Rosfa, S.; Kuharev, J.; Yan, K.; Bormuth, I.; Bremer, J.; et al. Quantitative and Integrative Proteome Analysis of Peripheral Nerve Myelin Identifies Novel Myelin Proteins and Candidate Neuropathy Loci. J. Neurosci. Off. J. Soc. Neurosci. 2011, 31, 16369–16386. [Google Scholar] [CrossRef]
- Jahn, O.; Hesse, D.; Reinelt, M.; Kratzin, H.D. Technical innovations for the automated identification of gel-separated proteins by MALDI-TOF mass spectrometry. Anal. Bioanal. Chem. 2006, 386, 92–103. [Google Scholar] [CrossRef] [PubMed]
- Wiśniewski, J.R.; Zougman, A.; Nagaraj, N.; Mann, M. Universal sample preparation method for proteome analysis. Nat. Methods 2009, 6, 359–362. [Google Scholar] [CrossRef] [PubMed]
- Nesvizhskii, A.I.; Keller, A.; Kolker, E.; Aebersold, R. A Statistical Model for Identifying Proteins by Tandem Mass Spectrometry. Anal. Chem. 2003, 75, 4646–4658. [Google Scholar] [CrossRef]
- Towbin, H.; Staehelin, T.; Gordon, J. Electrophoretic transfer of proteins from polyacrylamide gels to nitrocellulose sheets: Procedure and some applications. Proc. Natl. Acad. Sci. USA 1979, 76, 4350–4354. [Google Scholar] [CrossRef]
- Dihazi, G.H.; Dihazi, H.; Bibi, A.; Eltoweissy, M.; Mueller, C.A.; Asif, A.R.; Rubel, D.; Vasko, R.; Mueller, G.A. Secretion of ERP57 is important for extracellular matrix accumulation and progression of renal fibrosis, and is an early sign of disease onset. J. Cell Sci. 2013, 126, 3649–3663. [Google Scholar] [CrossRef]
- Tuttle, K.R.; Bakris, G.L.; Bilous, R.W.; Chiang, J.L.; De Boer, I.H.; Goldstein-Fuchs, J.; Hirsch, I.B.; Kalantar-Zadeh, K.; Narva, A.S.; Navaneethan, S.D.; et al. Diabetic kidney disease: A report from an ADA Consensus Conference. Diabetes Care 2014, 37, 2864–2883. [Google Scholar] [CrossRef]
- Ahn, J.H.; Yu, J.H.; Ko, S.-H.; Kwon, H.-S.; Kim, D.J.; Kim, J.H.; Kim, C.S.; Song, K.-H.; Won, J.C.; Lim, S.; et al. Prevalence and Determinants of Diabetic Nephropathy in Korea: Korea National Health and Nutrition Examination Survey. Diabetes Metab. J. 2014, 38, 109–119. [Google Scholar] [CrossRef]
- de Boer, I.H.; Rue, T.C.; Hall, Y.N.; Heagerty, P.J.; Weiss, N.S.; Himmelfarb, J. Temporal trends in the prevalence of diabetic kidney disease in the United States. JAMA 2011, 305, 2532–2539. [Google Scholar] [CrossRef]
- Boussageon, R.; Bejan-Angoulvant, T.; Saadatian-Elahi, M.; Lafont, S.; Bergeonneau, C.; Kassai, B.; Erpeldinger, S.; Wright, J.M.; Gueyffier, F.; Cornu, C. Effect of intensive glucose lowering treatment on all cause mortality, cardiovascular death, and microvascular events in type 2 diabetes: Meta-analysis of randomised controlled trials. BMJ 2011, 343, d4169. [Google Scholar] [CrossRef]
- de Galan, B.E.; Perkovic, V.; Ninomiya, T.; Pillai, A.; Patel, A.; Cass, A.; Neal, B.; Poulter, N.; Harrap, S.B.; Mogensen, C.-E.; et al. Lowering blood pressure reduces renal events in type 2 diabetes. J. Am. Soc. Nephrol. JASN 2009, 20, 883–892. [Google Scholar] [CrossRef]
- Duckworth, W.; Abraira, C.; Moritz, T. Glucose Control and Vascular Complications in Veterans with Type 2 Diabetes. N. Engl. J. Med. 2009, 360, 129–139. [Google Scholar] [CrossRef] [PubMed]
- Ismail-Beigi, F.; Craven, T.; Banerji, M.A.; Basile, J.; Calles, J.; Cohen, R.M.; Cuddihy, R.; Cushman, W.C.; Genuth, S.; Grimm, R.H.; et al. Effect of intensive treatment of hyperglycaemia on microvascular outcomes in type 2 diabetes: An analysis of the ACCORD randomised trial. Lancet Lond. Engl. 2010, 376, 419–430. [Google Scholar] [CrossRef]
- Krolewski, A.S.; Niewczas, M.A.; Skupien, J.; Gohda, T.; Smiles, A.; Eckfeldt, J.H.; Doria, A.; Warram, J.H. Early Progressive Renal Decline Precedes the Onset of Microalbuminuria and Its Progression to Macroalbuminuria. Diabetes Care 2014, 37, 226–234. [Google Scholar] [CrossRef] [PubMed]
- Craig, S.E.; Brady-Kalnay, S.M. Cancer cells cut homophilic cell adhesion molecules and run. Cancer Res. 2010, 71, 303–309. [Google Scholar] [CrossRef]
- Berx, G.; Staes, K.; Van Hengel, J.; Molemans, F.; Bussemakers, M.J.; van Bokhoven, A.; Van Roy, F. Cloning and characterization of the human invasion suppressor gene E-cadherin (CDH1). Genomics 1995, 26, 281–289. [Google Scholar] [CrossRef]
- Shore, E.M.; Nelson, W.J. Biosynthesis of the cell adhesion molecule uvomorulin (E-cadherin) in Madin-Darby canine kidney epithelial cells. J. Boil. Chem. 1991, 266, 19672–19680. [Google Scholar]
- Giroldi, L.A.; Schalken, J.A. Decreased expression of the intercellular adhesion molecule E-cadherin in prostate cancer: Biological significance and clinical implications. Cancer Metastasis Rev. 1993, 12, 29–37. [Google Scholar] [CrossRef]
- Rios-Doria, J.; Day, K.C.; Kuefer, R.; Rashid, M.G.; Chinnaiyan, A.M.; Rubin, M.A.; Day, M.L. The Role of Calpain in the Proteolytic Cleavage of E-cadherin in Prostate and Mammary Epithelial Cells. J. Boil. Chem. 2003, 278, 1372–1379. [Google Scholar] [CrossRef]
- Kuefer, R.; Hofer, M.D.; Gschwend, J.E.; Pienta, K.J.; Sanda, M.G.; Chinnaiyan, A.M.; Rubin, M.A.; Day, M.L. The role of an 80 kDa fragment of E-cadherin in the metastatic progression of prostate cancer. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2003, 9, 6447–6452. [Google Scholar]
- Banks, R.E.; Porter, W.H.; Whelan, P.; Smith, P.H.; Selby, P.J. Soluble forms of the adhesion molecule E-cadherin in urine. J. Clin. Pathol. 1995, 48, 179–180. [Google Scholar] [CrossRef][Green Version]
- Protheroe, A.S.; Banks, R.E.; Mzimba, M.; Porter, W.H.; Southgate, J.; Singh, P.N.; Bosomworth, M.; Harnden, P.; Smith, P.H.; Whelan, P.; et al. Urinary concentrations of the soluble adhesion molecule E-cadherin and total protein in patients with bladder cancer. Br. J. Cancer 1999, 80, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, T.R.L.; Brotherick, I.; Bishop, R.I.; White, M.D.; McKenna, D.M.; Horne, C.H.W.; Shenton, B.; Neal, D.E.; Mellon, J.K. Cell adhesion molecules in bladder cancer: Soluble serum E-cadherin correlates with predictors of recurrence. Br. J. Cancer 1996, 74, 579–584. [Google Scholar] [CrossRef] [PubMed]
- Noë, V.; Fingleton, B.; Jacobs, K.; Crawford, H.C.; Vermeulen, S.; Steelant, W.; Bruyneel, E.; Matrisian, L.M.; Mareel, M. Release of an invasion promoter E-cadherin fragment by matrilysin and stromelysin-1. J. Cell Sci. 2001, 114, 111–118. [Google Scholar] [PubMed]
- Maretzky, T.; Reiss, K.; Ludwig, A.; Buchholz, J.; Scholz, F.; Proksch, E.; De Strooper, B.; Hartmann, D.; Saftig, P. ADAM10 mediates E-cadherin shedding and regulates epithelial cell-cell adhesion, migration, and β-catenin translocation. Proc. Natl. Acad. Sci. USA 2005, 102, 9182–9187. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.H.; Choi, E.Y.; Hyun, M.S.; Jang, B.I.; Kim, T.N.; Kim, S.W.; Song, S.K.; Kim, J.H.; Kim, J.R. Association of Extracellular Cleavage of E-Cadherin Mediated by MMP-7 with HGF-Induced in vitro Invasion in Human Stomach Cancer Cells. Eur. Surg. Res. 2007, 39, 208–215. [Google Scholar] [CrossRef]
- Katayama, M.; Hirai, S.; Kamihagi, K.; Nakagawa, K.; Yasumoto, M.; Kato, I. Soluble E-cadherin fragments increased in circulation of cancer patients. Br. J. Cancer 1994, 69, 580–585. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | DM (n = 24) | DN Macro (n = 24) | DN Micro (n = 24) | NP (n = 24) | p |
|---|---|---|---|---|---|
| Creatinin (mg/dL) | 0.83 ± 0.28 | 1.04 ± 0.39 | 1.03 ± 0.44 | 0.91 ± 0.32 | 0.18 |
| BUN (mg/dL) | 33.0 ± n.a. | 25.3 ± 12.4 | 42.5 ± 26.2 | 38.0 ± 5.7 | 0.43 |
| Albuminuria (mg/L) | 11.7 ± 1.7 | 437.3 ± 682.3 | 73.1 ± 120.1 | 14.0 ± 6.8 | <0.01 |
| HbA1c (%) | 7.4 ± 1.0 | 7.6 ± 1.2 | 8.2 ± 0.8 | – | 0.10 |
| APOA1 | 1.4 ± 0.5 | 5.0 ± 0.6 | 3.8 ± 1.2 | 0.7 ± 0.2 | <0.01 |
| B2M | 1.7 ± 1.6 | 3.0 ± 1.2 | 2.3 ± 2.0 | 1.6 ± 2.0 | 0.02 |
| CDH1 | 1.1 ± 0.6 | 3.3 ± 1.4 | 1.6 ± 0.6 | 0.2 ± 0.1 | <0.01 |
| REG1A | 0.14 ± 0.06 | 0.19 ± 0.07 | 0.16 ± 0.08 | 0.10 ± 0.07 | <0.01 |
| Parameter | DM (n = 60) | DN Macro (n = 60) | DN Micro (n = 60) | NP (n = 32) | p |
|---|---|---|---|---|---|
| Creatinin (mg/dL) | 0.92 ± 0.36 | 0.95 ± 0.33 | 1.07 ± 0.62 | 0.96 ± 0.42 | 0.39 |
| BUN (mg/dL) | 23.0 ± 11.1 | 20.3 ± 9.1 | 40.0 ±21.0 | 48.0 ± 17.8 | < 0.01 |
| Albuminuria (mg/L) | 12.0 ± 4.5 | 195.1 ± 470.9 | 98.0 ± 210.9 | 14.7 ± 9.6 | < 0.01 |
| HbA1c (%) | 7.4 ± 0.9 | 7.6 ± 1.2 | 8.2 ± 0.9 | – | 0.05 |
| APOA1 | 0.62 ± 0.17 | 0.73 ± 0.16 | 0.76 ± 0.14 | 0.11 ± 0.07 | <0.01 |
| B2M | 0.63 ± 0.14 | 0.85 ± 0.24 | 0.84 ± 0.28 | 0.34 ± 0.05 | <0.01 |
| CDH1 | 0.81 ± 0.10 | 0.97 ± 0.20 | 1.13 ± 0.34 | 0.33 ± 0.005 | <0.01 |
| REG1A | 0.31 ± 0.07 | 0.43 ± 0.20 | 0.39 ± 0.18 | 0.18 ± 0.01 | <0.01 |
| Classification: DM versus DN Micro Model: M = –13.44 + 3.22 * APOA1 + 0.87 * B2M + 27.25 * REG1A Cutoff: 0.30, Accuracy: 85 [72, 94], Sensitivity: 83 [63, 95], Specificity: 88 [68, 97] |
| Classification: DN Micro versus DN Macro Model: M = 27.57 –4.51 * APOA1 –0.47 * B2M –2.14 * CDH1 Cutoff: 0.20, Accuracy: 88 [75, 95], Sensitivity: 100 [86, 100], Specificity: 75 [53, 90] |
| Classification: DM versus DN Macro Model: M = –12.49 + 6.03 * APOA1 + 4.51 * B2M + 5.74 * CDH1 Cutoff: 0.50, Accuracy: 76 [68, 84], Sensitivity: 72 [59, 83], Specificity: 80 [67, 89] |
| Classification: DM versus DN Micro Model: M = –18.91 + 9.24 * APOA1 + 5.05 * B2M + 9.48 * CDH1 Cutoff: 0.58, Accuracy: 85 [77, 91], Sensitivity: 79 [66, 89], Specificity: 90 [79, 96] |
| Classification: DN Micro versus DN Macro Model: M = –1.99 + 2.801 * CDH1 -2.34 * REG1A Cutoff: 0.55, Accuracy: 69 [59, 77], Sensitivity: 53 [39, 66], Specificity: 84 [73, 93] |
| Estimate | Std. Error | df | t Value | Pr(>|t|) | |
|---|---|---|---|---|---|
| (Intercept) | 69.13 | 3.493 | 62.85 | 19.79 | <0.0001 |
| AlbU | 0.01262 | 0.01383 | 76.49 | 0.9125 | 0.364 |
| E-Cadherin ng/mL | 0.04521 | 0.0179 | 77.46 | 2.525 | 0.013 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koziolek, M.; Mueller, G.A.; Dihazi, G.H.; Jung, K.; Altubar, C.; Wallbach, M.; Markovic, I.; Raddatz, D.; Jahn, O.; Karaköse, H.; et al. Urine E-cadherin: A Marker for Early Detection of Kidney Injury in Diabetic Patients. J. Clin. Med. 2020, 9, 639. https://doi.org/10.3390/jcm9030639
Koziolek M, Mueller GA, Dihazi GH, Jung K, Altubar C, Wallbach M, Markovic I, Raddatz D, Jahn O, Karaköse H, et al. Urine E-cadherin: A Marker for Early Detection of Kidney Injury in Diabetic Patients. Journal of Clinical Medicine. 2020; 9(3):639. https://doi.org/10.3390/jcm9030639
Chicago/Turabian StyleKoziolek, Michael, Gerhard A. Mueller, Gry H. Dihazi, Klaus Jung, Constanze Altubar, Manuel Wallbach, Ivana Markovic, Dirk Raddatz, Olaf Jahn, Hülya Karaköse, and et al. 2020. "Urine E-cadherin: A Marker for Early Detection of Kidney Injury in Diabetic Patients" Journal of Clinical Medicine 9, no. 3: 639. https://doi.org/10.3390/jcm9030639
APA StyleKoziolek, M., Mueller, G. A., Dihazi, G. H., Jung, K., Altubar, C., Wallbach, M., Markovic, I., Raddatz, D., Jahn, O., Karaköse, H., Lenz, C., Urlaub, H., Dihazi, A., El Meziane, A., & Dihazi, H. (2020). Urine E-cadherin: A Marker for Early Detection of Kidney Injury in Diabetic Patients. Journal of Clinical Medicine, 9(3), 639. https://doi.org/10.3390/jcm9030639