Relationships Among and Predictive Values of Obesity, Inflammation Markers, and Disease Severity in Pediatric Patients with Obstructive Sleep Apnea Before and After Adenotonsillectomy

 , ,
, ,  ,
,  ,
, 
Abstract
1. Introduction
2. Method
2.1. Ethical Considerations
2.2. Participants
2.3. Polysomnography
2.4. Measurement of Inflammatory Biomarkers
2.5. AT
2.6. Statistical Analysis
3. Results
3.1. Patients’ Characteristics at Baseline
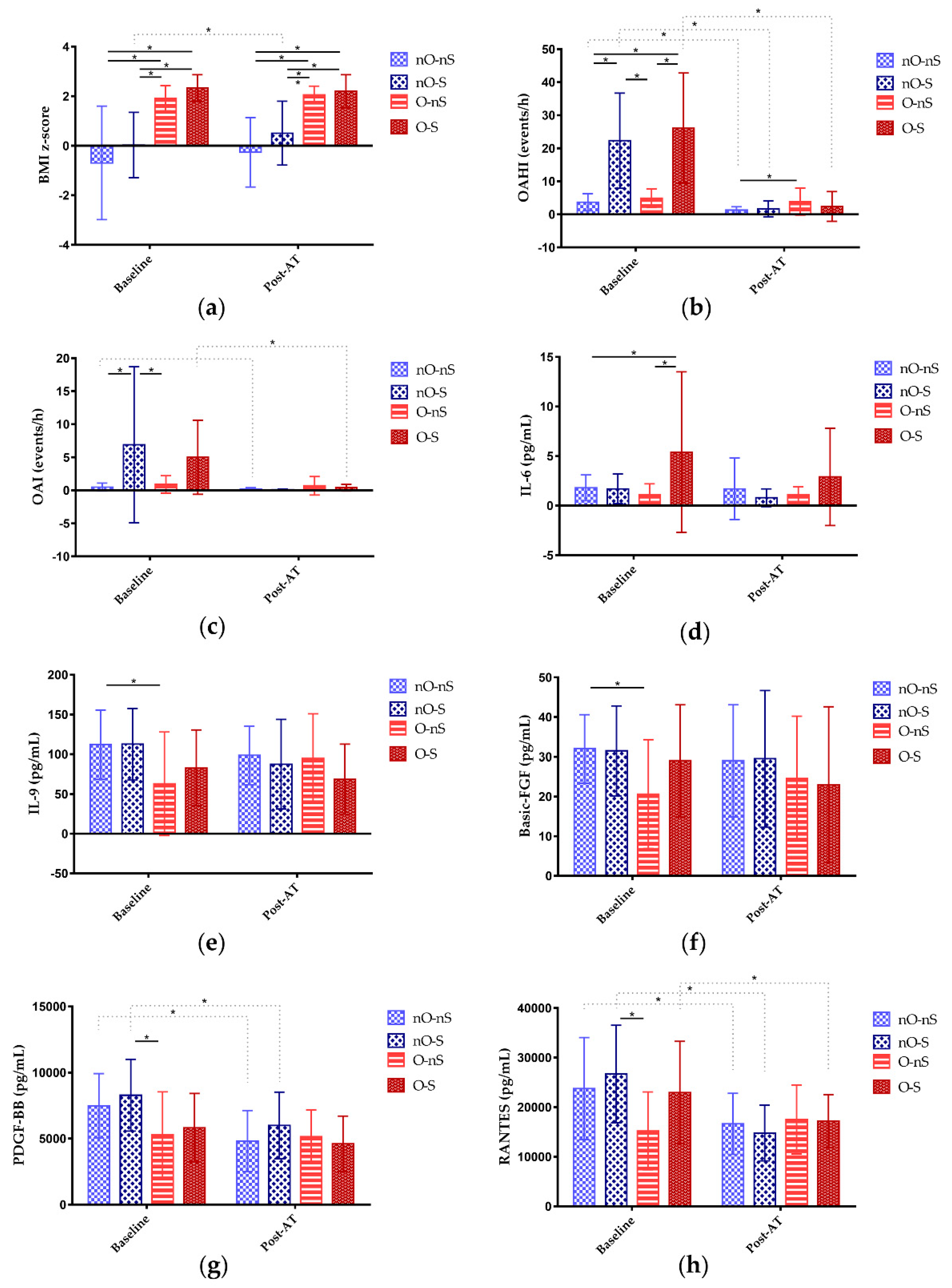
3.2. Inflammatory Biomarkers at Baseline
3.3. Associations between Patients’ Characteristics and Inflammatory Biomarkers at Baseline
3.4. Patients’ Characteristics After AT
3.5. Inflammatory Biomarkers After AT
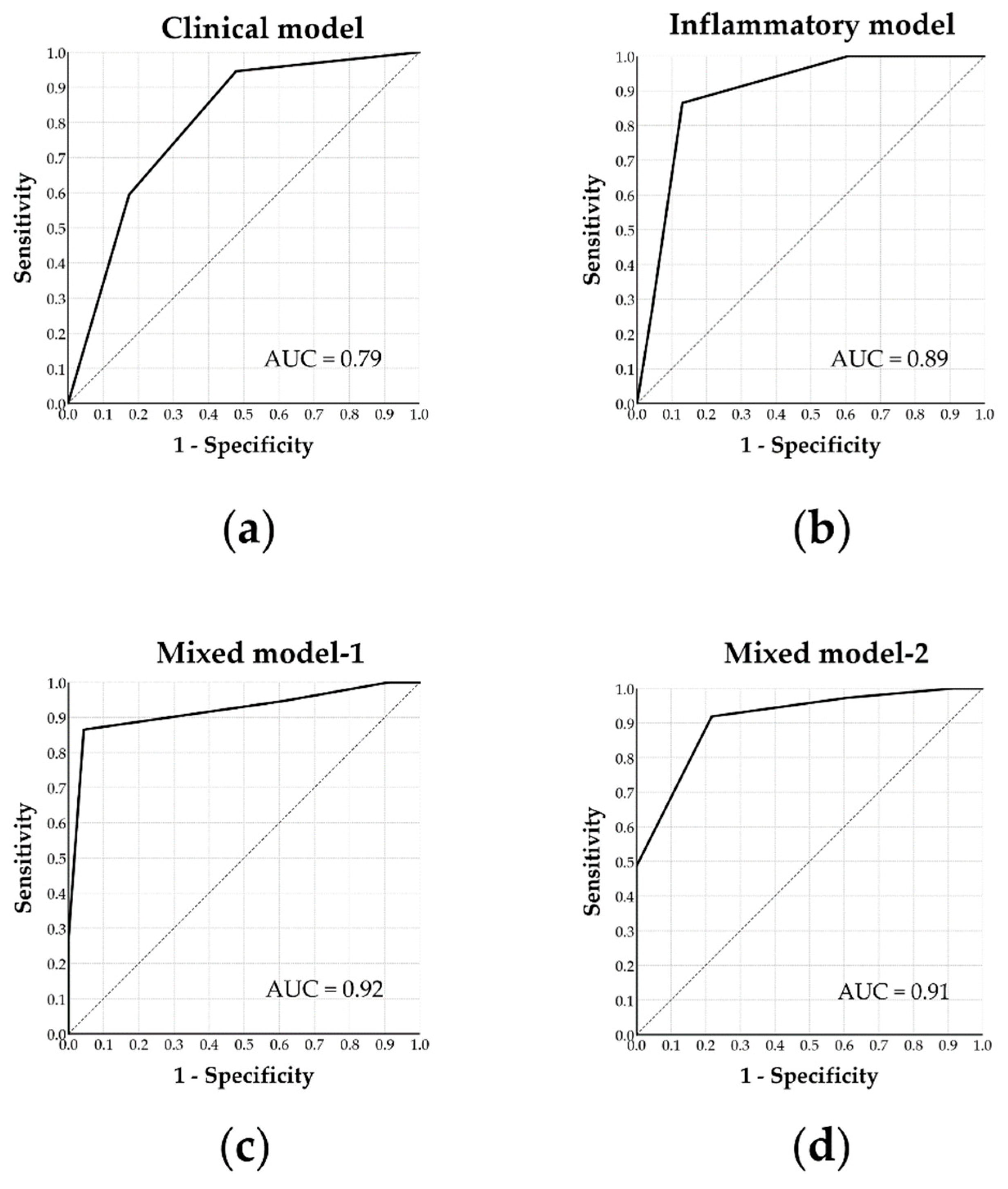
3.6. Predictors and Prediction Models for Surgical Cure
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Peppard, P.E.; Young, T.; Barnet, J.H.; Palta, M.; Hagen, E.W.; Hla, K.M. Increased prevalence of sleep-disordered breathing in adults. Am. J. Epidemiol. 2013, 177, 1006–1014. [Google Scholar] [CrossRef] [PubMed]
- Franklin, K.A.; Lindberg, E. Obstructive sleep apnea is a common disorder in the population-a review on the epidemiology of sleep apnea. J. Thorac. Dis. 2015, 7, 1311–1322. [Google Scholar] [PubMed]
- Heinzer, R.; Vat, S.; Marques-Vidal, P.; Marti-Soler, H.; Andries, D.; Tobback, N.; Mooser, V.; Preisig, M.; Malhotra, A.; Waeber, G.; et al. Prevalence of sleep-disordered breathing in the general population: The HypnoLaus study. Lancet Respir. Med. 2015, 3, 310–318. [Google Scholar] [CrossRef]
- Senaratna, C.V.; Perret, J.L.; Lodge, C.J.; Lowe, A.J.; Campbell, B.E.; Matheson, M.C.; Hamilton, G.S.; Dharmage, S.C. Prevalence of obstructive sleep apnea in the general population: A systematic review. Sleep Med. Rev. 2017, 34, 70–81. [Google Scholar] [CrossRef]
- Martinelli, E.O.; Haddad, F.L.M.; Stefanini, R.; Moreira, G.A.; Rapoport, P.B.; Gregorio, L.C.; Tufik, S.; Bittencourt, L.R.A. Clinicals And Upper Airway Characteristics in Obese Children with Obstructive Sleep Apnea. Sleep Sci. 2017, 10, 1–6. [Google Scholar] [CrossRef]
- Kang, K.T.; Lee, P.L.; Weng, W.C.; Hsu, W.C. Body weight status and obstructive sleep apnea in children. Int. J. Obes. (Lond.) 2012, 36, 920–924. [Google Scholar] [CrossRef]
- Kaditis, A.G.; Alexopoulos, E.I.; Hatzi, F.; Karadonta, I.; Chaidas, K.; Gourgoulianis, K.; Zintzaras, E.; Syrogiannopoulos, G.A. Adiposity in relation to age as predictor of severity of sleep apnea in children with snoring. Sleep Breath. Schlaf Atm. 2008, 12, 25–31. [Google Scholar] [CrossRef]
- Sardon, O.; Perez-Yarza, E.G.; Aldasoro, A.; Bordoy, A.; Mintegui, J.; Emparanza, J.I. Obstructive sleep apnea-hypopnea syndrome in children is not associated with obesity. Arch. Bronconeumol. 2006, 42, 583–587. [Google Scholar] [CrossRef]
- Arens, R.; Sin, S.; Nandalike, K.; Rieder, J.; Khan, U.I.; Freeman, K.; Wylie-Rosett, J.; Lipton, M.L.; Wootton, D.M.; McDonough, J.M.; et al. Upper airway structure and body fat composition in obese children with obstructive sleep apnea syndrome. Am. J. Respir. Crit. Care Med. 2011, 183, 782–787. [Google Scholar] [CrossRef]
- Su, M.S.; Zhang, H.L.; Cai, X.H.; Lin, Y.; Liu, P.N.; Zhang, Y.B.; Hu, W.Z.; Li, C.C.; Xiao, Y.F. Obesity in children with different risk factors for obstructive sleep apnea: A community-based study. Eur. J. Pediatr. 2016, 175, 211–220. [Google Scholar] [CrossRef]
- Nadeem, R.; Molnar, J.; Madbouly, E.M.; Nida, M.; Aggarwal, S.; Sajid, H.; Naseem, J.; Loomba, R. Serum inflammatory markers in obstructive sleep apnea: A meta-analysis. J. Clin. Sleep Med. 2013, 9, 1003–1012. [Google Scholar] [CrossRef] [PubMed]
- Kheirandish-Gozal, L.; Peris, E.; Wang, Y.; Tamae Kakazu, M.; Khalyfa, A.; Carreras, A.; Gozal, D. Lipopolysaccharide-binding protein plasma levels in children: Effects of obstructive sleep apnea and obesity. J. Clin. Endocrinol. Metab. 2014, 99, 656–663. [Google Scholar] [CrossRef] [PubMed]
- Nachalon, Y.; Lowenthal, N.; Greenberg-Dotan, S.; Goldbart, A.D. Inflammation and growth in young children with obstructive sleep apnea syndrome before and after adenotonsillectomy. Mediat. Inflamm. 2014, 2014, 146893. [Google Scholar] [CrossRef] [PubMed]
- Friedman, M.; Wilson, M.; Lin, H.C.; Chang, H.W. Updated systematic review of tonsillectomy and adenoidectomy for treatment of pediatric obstructive sleep apnea/hypopnea syndrome. Otolaryngol. Head Neck Surg. 2009, 140, 800–808. [Google Scholar] [CrossRef]
- Choi, J.H.; Oh, J.I.; Kim, T.M.; Yoon, H.C.; Park, I.H.; Kim, T.H.; Lee, H.M.; Lee, S.H.; Lee, S.H. Long-term Subjective and Objective Outcomes of Adenotonsillectomy in Korean Children With Obstructive Sleep Apnea Syndrome. Clin. Exp. Otorhinolaryngol. 2015, 8, 256–260. [Google Scholar] [CrossRef]
- Bhattacharjee, R.; Kheirandish-Gozal, L.; Spruyt, K.; Mitchell, R.B.; Promchiarak, J.; Simakajornboon, N.; Kaditis, A.G.; Splaingard, D.; Splaingard, M.; Brooks, L.J.; et al. Adenotonsillectomy outcomes in treatment of obstructive sleep apnea in children: A multicenter retrospective study. Am. J. Respir. Crit. Care Med. 2010, 182, 676–683. [Google Scholar] [CrossRef]
- Kaditis, A.; Kheirandish-Gozal, L.; Gozal, D. Algorithm for the diagnosis and treatment of pediatric OSA: A proposal of two pediatric sleep centers. Sleep Med. 2012, 13, 217–227. [Google Scholar] [CrossRef]
- Baugh, R.F.; Archer, S.M.; Mitchell, R.B.; Rosenfeld, R.M.; Amin, R.; Burns, J.J.; Darrow, D.H.; Giordano, T.; Litman, R.S.; Li, K.K.; et al. Clinical practice guideline: Tonsillectomy in children. Otolaryngol. Head Neck Surg. 2011, 144, S1–S30. [Google Scholar] [CrossRef]
- Huang, Y.S.; Guilleminault, C.; Lee, L.A.; Lin, C.H.; Hwang, F.M. Treatment outcomes of adenotonsillectomy for children with obstructive sleep apnea: A prospective longitudinal study. Sleep 2014, 37, 71–76. [Google Scholar] [CrossRef]
- Huang, Y.S.; Hwang, F.M.; Lin, C.H.; Lee, L.A.; Huang, P.Y.; Chiu, S.T. Clinical manifestations of pediatric obstructive sleep apnea syndrome: Clinical utility of the Chinese-version Obstructive Sleep Apnea Questionaire-18. Psychiatry Clin. Neurosci. 2015, 69, 752–762. [Google Scholar] [CrossRef]
- Huang, Y.S.; Guilleminault, C.; Hwang, F.M.; Cheng, C.; Lin, C.H.; Li, H.Y.; Lee, L.A. Inflammatory cytokines in pediatric obstructive sleep apnea. Medicine 2016, 95, e4944. [Google Scholar] [CrossRef] [PubMed]
- Berry, R.B.; Budhiraja, R.; Gottlieb, D.J.; Gozal, D.; Iber, C.; Kapur, V.K.; Marcus, C.L.; Mehra, R.; Parthasarathy, S.; Quan, S.F.; et al. Rules for scoring respiratory events in sleep: Update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine. J. Clin. Sleep Med. 2012, 8, 597–619. [Google Scholar] [CrossRef] [PubMed]
- Marcus, C.L.; Moore, R.H.; Rosen, C.L.; Giordani, B.; Garetz, S.L.; Taylor, H.G.; Mitchell, R.B.; Amin, R.; Katz, E.S.; Arens, R.; et al. A randomized trial of adenotonsillectomy for childhood sleep apnea. N. Engl. J. Med. 2013, 368, 2366–2376. [Google Scholar] [CrossRef]
- Dehlink, E.; Tan, H.L. Update on paediatric obstructive sleep apnoea. J. Thorac. Dis. 2016, 8, 224–235. [Google Scholar]
- Kuczmarski, R.J.; Ogden, C.L.; Guo, S.S.; Grummer-Strawn, L.M.; Flegal, K.M.; Mei, Z.; Wei, R.; Curtin, L.R.; Roche, A.F.; Johnson, C.L. 2000 CDC Growth Charts for the United States: Methods and development. Vital Health Stat. 2002, 11, 1–190. [Google Scholar]
- Lee, L.A.; Huang, C.G.; Chen, N.H.; Wang, C.L.; Fang, T.J.; Li, H.Y. Severity of obstructive sleep apnea syndrome and high-sensitivity C-reactive protein reduced after relocation pharyngoplasty. Otolaryngol. Head Neck Surg. 2011, 144, 632–638. [Google Scholar] [CrossRef]
- Lee, L.A.; Li, H.Y.; Lin, Y.S.; Fang, T.J.; Huang, Y.S.; Hsu, J.F.; Wu, C.M.; Huang, C.G. Severity of childhood obstructive sleep apnea and hypertension improved after adenotonsillectomy. Otolaryngol. Head Neck Surg. 2015, 152, 553–560. [Google Scholar] [CrossRef]
- Lu, C.T.; Li, H.Y.; Lee, G.S.; Huang, Y.S.; Huang, C.G.; Chen, N.H.; Lee, L.A. Snoring sound energy as a potential biomarker for disease severity and surgical response in childhood obstructive sleep apnoea: A pilot study. Clin. Otolaryngol. 2019, 44, 47–52. [Google Scholar] [CrossRef]
- Kaditis, A.G.; Finder, J.; Alexopoulos, E.I.; Starantzis, K.; Tanou, K.; Gampeta, S.; Agorogiannis, E.; Christodoulou, S.; Pantazidou, A.; Gourgoulianis, K.; et al. Sleep-disordered breathing in 3680 Greek children. Pediatr. Pulmonol. 2004, 37, 499–509. [Google Scholar] [CrossRef]
- Febbraio, M.A.; Pedersen, B.K. Contraction-induced myokine production and release: Is skeletal muscle an endocrine organ? Exerc. Sport Sci. Rev. 2005, 33, 114–119. [Google Scholar] [CrossRef]
- Kristiansen, O.P.; Mandrup-Poulsen, T. Interleukin-6 and diabetes: The good, the bad, or the indifferent? Diabetes 2005, 54 (Suppl. S2), S114–S124. [Google Scholar] [CrossRef]
- Smith, P.C.; Hobisch, A.; Lin, D.L.; Culig, Z.; Keller, E.T. Interleukin-6 and prostate cancer progression. Cytokine Growth Factor Rev. 2001, 12, 33–40. [Google Scholar] [CrossRef]
- Swardfager, W.; Lanctot, K.; Rothenburg, L.; Wong, A.; Cappell, J.; Herrmann, N. A meta-analysis of cytokines in Alzheimer’s disease. Biol. Psychiatry 2010, 68, 930–941. [Google Scholar] [CrossRef] [PubMed]
- Nishimoto, N. Interleukin-6 in rheumatoid arthritis. Curr. Opin. Rheumatol. 2006, 18, 277–281. [Google Scholar] [CrossRef] [PubMed]
- Xie, G.; Yao, Q.; Liu, Y.; Du, S.; Liu, A.; Guo, Z.; Sun, A.; Ruan, J.; Chen, L.; Ye, C.; et al. IL-6-induced epithelial-mesenchymal transition promotes the generation of breast cancer stem-like cells analogous to mammosphere cultures. Int. J. Oncol. 2012, 40, 1171–1179. [Google Scholar] [PubMed]
- Fitzgibbons, C.M.; Goldstein, R.L.; Gottlieb, D.J.; Moy, M.L. Physical Activity in Overlap Syndrome of COPD and Obstructive Sleep Apnea: Relationship With Markers of Systemic Inflammation. J. Clin. Sleep Med. 2019, 15, 973–978. [Google Scholar] [CrossRef] [PubMed]
- Matter, C.M.; Handschin, C. RANTES (regulated on activation, normal T cell expressed and secreted), inflammation, obesity, and the metabolic syndrome. Circulation 2007, 115, 946–948. [Google Scholar] [CrossRef] [PubMed]
- Goswami, R.; Kaplan, M.H. A brief history of IL-9. J. Immunol. 2011, 186, 3283–3288. [Google Scholar] [CrossRef]
- Fagerberg, L.; Hallstrom, B.M.; Oksvold, P.; Kampf, C.; Djureinovic, D.; Odeberg, J.; Habuka, M.; Tahmasebpoor, S.; Danielsson, A.; Edlund, K.; et al. Analysis of the human tissue-specific expression by genome-wide integration of transcriptomics and antibody-based proteomics. Mol. Cell. Proteom. 2014, 13, 397–406. [Google Scholar] [CrossRef]
- Sanchez, T.; Castro-Rodriguez, J.A.; Brockmann, P.E. Sleep-disordered breathing in children with asthma: A systematic review on the impact of treatment. J. Asthma Allergy 2016, 9, 83–91. [Google Scholar]
- Trivedi, M.; ElMallah, M.; Bailey, E.; Kremer, T.; Rhein, L.M. Pediatric Obstructive Sleep Apnea and Asthma: Clinical Implications. Pediatr. Ann. 2017, 46, e332–e335. [Google Scholar] [CrossRef] [PubMed]
- Kong, D.L.; Qin, Z.; Shen, H.; Jin, H.Y.; Wang, W.; Wang, Z.F. Association of Obstructive Sleep Apnea with Asthma: A Meta-Analysis. Sci. Rep. 2017, 7, 4088. [Google Scholar] [CrossRef] [PubMed]
- Yun, Y.R.; Won, J.E.; Jeon, E.; Lee, S.; Kang, W.; Jo, H.; Jang, J.H.; Shin, U.S.; Kim, H.W. Fibroblast growth factors: Biology, function, and application for tissue regeneration. J. Tissue Eng. 2010, 2010, 218142. [Google Scholar] [CrossRef] [PubMed]
- Seida, A.; Wada, J.; Kunitomi, M.; Tsuchiyama, Y.; Miyatake, N.; Fujii, M.; Kira, S.; Takahashi, K.; Shikata, K.; Makino, H. Serum bFGF levels are reduced in Japanese overweight men and restored by a 6-month exercise education. Int. J. Obes. Relat. Metab. Disord. 2003, 27, 1325–1331. [Google Scholar] [CrossRef][Green Version]
- Hao, R.H.; Guo, Y.; Dong, S.S.; Weng, G.Z.; Yan, H.; Zhu, D.L.; Chen, X.F.; Chen, J.B.; Yang, T.L. Associations of Plasma FGF2 Levels and Polymorphisms in the FGF2 Gene with Obesity Phenotypes in Han Chinese Population. Sci. Rep. 2016, 6, 19868. [Google Scholar] [CrossRef]
- Kwan, P.; Desmoulière, A.; Tredget, E.E. Chapter 45—Molecular and cellular basis of hypertrophic scarring. In Total Burn Care, 4th ed.; Herndon, D.N., Ed.; W.B. Saunders: London, UK, 2012; pp. 495–505. [Google Scholar] [CrossRef]
- Liu, H.G.; Lin, M.; Guan, P.; Xu, Y.J. The change of platelet derived growth factor in patients with obstructive sleep apnea-hypopnea syndrome. Zhonghua Jie He He Hu Xi Za Zhi 2006, 29, 536–540. [Google Scholar]
- Bishara, N. Chapter 18—The Use of Biomarkers for Detection of Early- and Late-Onset Neonatal Sepsis. In Hematology, Immunology and Infectious Disease: Neonatology Questions and Controversies, 2nd ed.; Ohls, R.K., Maheshwari, A., Eds.; W.B. Saunders: Philadelphia, PA, USA, 2012; pp. 303–315. [Google Scholar] [CrossRef]
- Loux, T.J.; Lotze, M.T.; Zeh, H.J. Chapter Fourteen—NK cells as recipients of cytokine signals. In Natural Killer Cells; Lotze, M.T., Thomson, A.W., Eds.; Academic Press: San Diego, CA, USA, 2010; pp. 189–201. [Google Scholar] [CrossRef]
- Lacy, P. Chapter 12—Eosinophil Cytokines in Allergy. In Cytokine Effector Functions in Tissues; Foti, M., Locati, M., Eds.; Academic Press: Cambridge, MA, USA, 2017; pp. 173–218. [Google Scholar] [CrossRef]
- Arnaud, C.; Beguin, P.C.; Lantuejoul, S.; Pepin, J.L.; Guillermet, C.; Pelli, G.; Burger, F.; Buatois, V.; Ribuot, C.; Baguet, J.P.; et al. The inflammatory preatherosclerotic remodeling induced by intermittent hypoxia is attenuated by RANTES/CCL5 inhibition. Am. J. Respir. Crit. Care Med. 2011, 184, 724–731. [Google Scholar] [CrossRef]
- Testelmans, D.; Tamisier, R.; Barone-Rochette, G.; Baguet, J.P.; Roux-Lombard, P.; Pepin, J.L.; Levy, P. Profile of circulating cytokines: Impact of OSA, obesity and acute cardiovascular events. Cytokine 2013, 62, 210–216. [Google Scholar] [CrossRef]
- Campos-Rodriguez, F.; Asensio-Cruz, M.I.; Cordero-Guevara, J.; Jurado-Gamez, B.; Carmona-Bernal, C.; Gonzalez-Martinez, M.; Troncoso, M.F.; Sanchez-Lopez, V.; Arellano-Orden, E.; Garcia-Sanchez, M.I.; et al. Effect of continuous positive airway pressure on inflammatory, antioxidant, and depression biomarkers in women with obstructive sleep apnea: A randomized controlled trial. Sleep 2019, 42. [Google Scholar] [CrossRef]
- Borges, Y.G.; Cipriano, L.H.C.; Aires, R.; Zovico, P.V.C.; Campos, F.V.; de Araujo, M.T.M.; Gouvea, S.A. Oxidative stress and inflammatory profiles in obstructive sleep apnea: Are short-term CPAP or aerobic exercise therapies effective? Sleep Breath Schlaf Atm. 2019. [Google Scholar] [CrossRef]
- Marcano-Acuna, M.E.; Carrasco-Llatas, M.; Tortajada-Girbes, M.; Dalmau-Galofre, J.; Codoner-Franch, P. Impact of adenotonsillectomy on the evolution of inflammatory markers. Clin. Otolaryngol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Chang, T.S.; Chiang, R.P. Total analysis of clinical factors for surgical success of adenotonsillectomy in pediatric OSAS. Eur. Arch. Otorhinolaryngol. 2017, 274, 561–566. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.H.; Hsu, W.C.; Chang, W.H.; Lin, M.T.; Kang, K.T. Polysomnographic findings after adenotonsillectomy for obstructive sleep apnoea in obese and non-obese children: A systematic review and meta-analysis. Clin. Otolaryngol. 2016, 41, 498–510. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | nO-nS | nO-S | O-nS | O-S | p-Value 1 |
|---|---|---|---|---|---|
| Patients | n = 24 | n = 11 | n = 14 | n = 11 | |
| Age (years) | 6.8 (1.7) | 7.6 (2.5) | 8.3 (2.5) | 7.6 (2.4) | 0.26 |
| Males | 16 (67) | 9 (82) | 13 (93) | 8 (73) | 0.30 |
| BMI (kg/m2) z-score | −0.69 (2.29) 2 | 0.03 (1.32) 3 | 1.92 (0.51) 2,3 | 2.33 (0.54) 2,3 | <0.001 |
| OSA-18 | 78.8 (14.6) | 82.8 (18.4) | 76.6 (15.6) | 88.0 (13.8) | 0.27 |
| OAHI (events/h) | 3.7 (2.6) 2 | 22.3 (14.4) 2,3 | 4.9 (2.8) 3,4 | 26.1 (16.7) 2,4 | <0.001 |
| OAI (events/h) | 0.5 (0.6) 2 | 6.9 (11.8) 2,3 | 0.9 (1.3) 3 | 5.0 (5.6) | 0.01 |
| Mean SpO2 (%) | 97.7 (0.8) 2 | 96.3 (2.6) | 97.5 (0.8) 4 | 96.6 (0.8) 2,4 | 0.02 |
| Minimal SpO2 (%) | 92.0 (2.4) 2 | 82.8 (10.7) 2,3 | 89.3 (3.1) 3,4 | 82.4 (6.6) 2,4 | <0.001 |
| Variables | nO-nS | nO-S | O-nS | O-S | p-Value 1 |
|---|---|---|---|---|---|
| Patients | n = 24 | n = 11 | n = 14 | n = 11 | |
| IL-1β (pg/mL) | 0.7 (0.6) | 0.8 (0.9) | 0.5 (0.8) | 1.0 (0.9) | 0.45 |
| IL-1ra (pg/mL) | 131.3 (69.1) | 157.0 (83.9) | 195.9 (231.0) | 223.9 (128.5) | 0.25 |
| IL-2 (pg/mL) | 3.5 (2.0) | 3.8 (2.6) | 1.9 (2.1) | 3.2 (2.1) | 0.13 |
| IL-4 (pg/mL) | 3.0 (1.2) | 3.1 (0.9) | 2.0 (1.4) | 2.4 (1.2) | 0.07 |
| IL-5 (pg/mL) | 11.9 (9.0) | 14.7 (22.9) | 5.0 (7.8) | 20.2 (23.0) | 0.11 |
| IL-6 (pg/mL) | 1.8 (1.3) 2 | 1.7 (1.5) | 1.1 (1.1) 4 | 5.4 (8.1) 2,4 | 0.02 |
| IL-7 (pg/mL) | 8.6 (5.7) | 8.2 (5.4) | 6.4 (6.9) | 5.9 (3.6) | 0.47 |
| IL-8 (pg/mL) | 7.7 (4.9) | 6.1 (1.9) | 5.1 (2.8) | 5.7 (1.7) | 0.16 |
| IL-9 (pg/mL) | 112.0 (43.4) 2 | 112.6 (44.8) | 62.8 (65.1) 2 | 83.0 (47.5) | 0.02 |
| IL-10 (pg/mL) | 1.4 (2.2) | 1.1 (2.8) | 1.2 (2.0) | 0.9 (1.6) | 0.94 |
| IL-12 (pg/mL) | 2.0 (2.6) | 3.4 (8.4) | 0.7 (0.9) | 2.6 (3.9) | 0.47 |
| IL-13 (pg/mL) | 1.3 (2.7) | 0.8 (1.0) | 1.0 (1.4) | 1.1 (1.4) | 0.93 |
| IL-15 (pg/mL) | 44.0 (55.0) | 50.3 (51.5) | 33.5 (29.1) | 54.3 (51.5) | 0.73 |
| IL-17 (pg/mL) | 17.3 (9.0) | 17.9 (8.4) | 10.2 (9.7) | 18.1 (9.3) | 0.08 |
| Eotaxin (pg/mL) | 68.1 (43.5) | 72.1 (34.6) | 61.7 (39.4) | 64.3 (34.0) | 0.92 |
| Basic-FGF (pg/mL) | 32.0 (8.6) 2 | 31.5 (11.3) | 20.6 (13.7) 2 | 29.0 (14.1) | 0.03 |
| G-CSF (pg/mL) | 108.7 (87.5) | 102.5 (88.0) | 45.0 (77.2) | 39.7 (75.2) | 0.05 |
| GM-CSF (pg/mL) | 1.5 (1.9) | 1.2 (2.1) | 0.7 (1.0) | 2.4 (1.9) | 0.15 |
| Interferon-γ (pg/mL) | 5.4 (4.8) | 6.3 (6.6) | 3.9 (5.0) | 8.7 (5.5) | 0.16 |
| IP-10 (pg/mL) | 920.1 (625.6) | 733.5 (389.6) | 1780.4 (4034.5) | 1330.7 (1135.6) | 0.54 |
| MCP-1 (pg/mL) | 38.5 (16.7) | 36.7 (17.2) | 39.2 (47.6) | 31.3 (10.8) | 0.88 |
| MIP-1α (pg/mL) | 2.1 (1.3) | 1.9 (1.0) | 1.5 (0.9) | 1.9 (0.7) | 0.55 |
| MIP-1β (pg/mL) | 135.5 (36.1) | 126.7 (28.1) | 117.1 (24.2) | 128.2 (25.8) | 0.36 |
| PDGF-BB (pg/mL) | 7490.6 (2432.8) | 8283.6 (2713.4) 3 | 5287.8 (3248.3) 3 | 5821.6 (2592.6) | 0.02 |
| RANTES (pg/mL) | 23757.4 (10285.4) | 26681.1 (9835.8) 3 | 15223.4 (7847.7) 3 | 22973.0 (10319.2) | 0.02 |
| TNF-α (pg/mL) | 45.9 (19.2) | 44.9 (19.3) | 38.8 (22.8) | 47.9 (18.9) | 0.67 |
| VEGF (pg/mL) | 60.8 (91.5) | 33.5 (45.6) | 43.2 (28.7) | 25.4 (33.6) | 0.43 |
| Variables | nO-nS | nO-S | O-nS | O-S | p-Value 1 |
|---|---|---|---|---|---|
| Patients | n = 24 | n = 11 | n = 14 | n = 11 | |
| BMI (kg/m2) z-score | −0.26 (1.40) 2 | 0.51 (1.29) 3,* | 2.06 (0.35) 2,3 | 2.20 (0.67) 2,3 | <0.001 |
| OSA-18 | 52.2 (13.0) * | 55.3 (10.9) * | 51.0 (13.2) * | 51.1 (11.6) * | 0.83 |
| OAHI (events/h) | 1.3 (1.0) 2,* | 1.7 (2.4) * | 3.9 (3.9) 2 | 2.4 (3.1) * | 0.03 |
| OAI (events/h) | 0.2 (0.2) * | 0.1 (0.1) | 0.7 (1.4) | 0.4 (0.5) * | 0.09 |
| Surgical cure | 18 (75%) | 9 (82%) | 5 (36%) | 5 (46%) | 0.03 |
| Mean SpO2 (%) | 97.8 (0.8) * | 97.6 (1.0) | 97.8 (0.6) | 97.4 (0.8) * | 0.51 |
| Minimal SpO2 (%) | 92.3 (2.5) * | 90.2 (3.8) * | 89.6 (2.8) | 89.6 (5.4) * | 0.10 |
| Variables | nO-nS | nO-S | O-nS | O-S | p-Value 1 |
|---|---|---|---|---|---|
| Patients | n = 24 | n = 11 | n = 14 | n = 11 | |
| IL-1β (pg/mL) | 0.3 (0.2) * | 0.3 (0.2) | 0.3 (0.2) | 0.3 (0.3) * | 0.83 |
| IL-1ra (pg/mL) | 93.6 (48.5) * | 94.7 (66.7) * | 146.3 (99.8) | 132.9 (76.4) * | 0.11 |
| IL-2 (pg/mL) | 2.1 (1.4) * | 1.9 (1.3) | 1.5 (1.2) | 2.1 (1.6) | 0.51 |
| IL-4 (pg/mL) | 2.0 (1.0) * | 1.8 (1.0) * | 2.0 (1.0) | 1.5 (0.9) * | 0.49 |
| IL-5 (pg/mL) | 4.1 (4.1) * | 5.1 (9.7) | 4.1 (4.3) | 13.5 (23.9) | 0.13 |
| IL-6 (pg/mL) | 1.7 (3.1) | 0.8 (0.9) | 1.1 (0.8) | 2.9 (4.9) | 0.35 |
| IL-7 (pg/mL) | 8.0 (5.7) | 9.0 (7.4) | 7.9 (6.5) | 3.4 (2.3) | 0.11 |
| IL-8 (pg/mL) | 4.3 (2.3) * | 4.4 (2.2) | 3.6 (1.7) | 4.1 (2.7) | 0.77 |
| IL-9 (pg/mL) | 98.5 (36.6) | 87.5 (56.3) | 94.6 (56.3) | 68.6 (44.0) | 0.36 |
| IL-10 (pg/mL) | 0.4 (0.2) * | 0.4 (0.2) | 0.4 (0.2) | 0.3 (0.2) | 0.29 |
| IL-12 (pg/mL) | 0.9 (1.1) | 2.2 (4.8) | 0.4 (0.4) | 2.5 (4.7) | 0.22 |
| IL-13 (pg/mL) | 0.7 (0.7) * | 0.7 (0.9) | 0.8 (1.0) | 0.8 (1.0) | 0.97 |
| IL-15 (pg/mL) | 23.2 (48.8) * | 21.7 (14.8) | 16.0 (14.1) * | 38.8 (70.1) | 0.63 |
| IL-17 (pg/mL) | 11.7 (6.5) * | 9.0 (5.6) * | 10.9 (7.0) | 13.3 (9.0) | 0.54 |
| Eotaxin (pg/mL) | 46.2 (20.9) * | 44.7 (16.1) * | 50.2 (22.2) | 48.6 (28.2) * | 0.92 |
| Basic-FGF (pg/mL) | 29.0 (14.1) | 29.5 (17.2) | 24.6 (15.6) | 23.0 (19.6) | 0.65 |
| G-CSF (pg/mL) | 84.6 (84.3) | 69.0 (77.5) * | 82.2 (90.1) | 18.0 (36.8) | 0.12 |
| GM-CSF (pg/mL) | 0.6 (0.9) * | 0.5 (0.6) | 0.4 (0.4) | 1.9 (4.0) | 0.18 |
| Interferon-γ (pg/mL) | 4.0 (3.3) | 3.2 (2.9) | 3.5 (2.8) | 7.6 (11.7) | 0.20 |
| IP-10 (pg/mL) | 630.8 (485.9) * | 496.1 (288.9) * | 564.6 (301.9) | 740.4 (392.6) | 0.52 |
| MCP-1 (pg/mL) | 17.9 (9.5) * | 15.2 (8.1) * | 21.1 (12.0) | 16.8 (6.6) * | 0.46 |
| MIP-1α (pg/mL) | 1.5 (1.7) * | 1.8 (1.3) | 1.1 (0.6) | 1.5 (0.7) | 0.61 |
| MIP-1β (pg/mL) | 120.9 (27.2) * | 113.3 (18.6) | 113.2 (19.0) | 124.5 (20.5) | 0.51 |
| PDGF-BB (pg/mL) | 4816.0 (2312.9) * | 6001.3 (2521.4) * | 5150.0 (2025.7) | 4606.8 (2100.4) | 0.45 |
| RANTES (pg/mL) | 16651.8 (6150.8) * | 14805.6 (5618.9) * | 17522.6 (6939.8) | 17204.6 (5330.5) * | 0.71 |
| TNF-α (pg/mL) | 52.8 (24.4) | 50.1 (24.4) | 42.6 (24.1) | 42.9 (19.4) | 0.51 |
| VEGF (pg/mL) | 38.4 (60.7) | 41.1 (34.4) | 27.5 (22.2) | 45.2 (51.3) | 0.81 |
| Predictors | Cut-off Value | AUC | 95% CI | p-Value |
|---|---|---|---|---|
| Clinical variables | ||||
| Age (years) | <7.0 | 0.70 | 0.57–0.84 | 0.01 |
| Boys | Boy | 0.42 | 0.27–0.56 | 0.28 |
| BMI (kg/m2) z-score | <1.44 | 0.74 | 0.61–0.87 | 0.002 |
| OSA-18 | >78.5 | 0.53 | 0.38–0.68 | 0.69 |
| OAHI (events/h) | <4.0 | 0.63 | 0.49–0.77 | 0.09 |
| OAI (events/h) | >0.6 | 0.59 | 0.44–0.74 | 0.25 |
| Mean SpO2 (%) | >97.6 | 0.61 | 0.46–0.75 | 0.18 |
| Minimum SpO2 (%) | >86.5 | 0.58 | 0.43–0.73 | 0.29 |
| Inflammatory biomarkers | ||||
| IL-1β (pg/mL) | >0.3 | 0.56 | 0.41–0.71 | 0.41 |
| IL-1ra (pg/mL) | <149.2 | 0.67 | 0.53–0.81 | 0.03 |
| IL-2 (pg/mL) | >3.4 | 0.62 | 0.48–0.77 | 0.11 |
| IL-4 (pg/mL) | >1.8 | 0.62 | 0.46–0.77 | 0.14 |
| IL-5 (pg/mL) | >1.0 | 0.62 | 0.47–0.77 | 0.12 |
| IL-6 (pg/mL) | <2.0 | 0.55 | 0.40–0.70 | 0.49 |
| IL-7 (pg/mL) | >4.9 | 0.59 | 0.44–0.74 | 0.24 |
| IL-8 (pg/mL) | >3.0 | 0.62 | 0.46–0.77 | 0.13 |
| IL-9 (pg/mL) | >82.8 | 0.67 | 0.52–0.82 | 0.03 |
| IL-10 (pg/mL) | <0.5 | 0.69 | 0.55–0.83 | 0.01 |
| IL-12 (pg/mL) | >0.2 | 0.63 | 0.48–0.78 | 0.10 |
| IL-13 (pg/mL) | <1.4 | 0.58 | 0.43–0.73 | 0.31 |
| IL-15 (pg/mL) | <11.8 | 0.71 | 0.58–0.84 | 0.01 |
| IL-17 (pg/mL) | >4.7 | 0.66 | 0.51–0.81 | 0.04 |
| Eotaxin (pg/mL) | >36.8 | 0.61 | 0.45–0.76 | 0.17 |
| Basic-FGF (pg/mL) | >15.9 | 0.65 | 0.50–0.80 | 0.06 |
| G-CSF (pg/mL) | >69.5 | 0.64 | 0.50–0.78 | 0.07 |
| GM-CSF (pg/mL) | <0.2 | 0.68 | 0.54–0.81 | 0.02 |
| Interferon-γ (pg/mL) | >1.9 | 0.51 | 0.36–0.66 | 0.91 |
| IP-10 (pg/mL) | <818.6 | 0.56 | 0.41–0.71 | 0.45 |
| MCP-1 (pg/mL) | <51.2 | 0.67 | 0.52–0.82 | 0.03 |
| MIP-1α (pg/mL) | <1.2 | 0.51 | 0.36–0.66 | 0.87 |
| MIP-1β (pg/mL) | <121.6 | 0.53 | 0.38–0.68 | 0.74 |
| PDGF-BB (pg/mL) | <10201.7 | 0.62 | 0.46–0.77 | 0.13 |
| RANTES (pg/mL) | >15435.5 | 0.71 | 0.56–0.85 | 0.01 |
| TNF-α (pg/mL) | >27.9 | 0.65 | 0.50–0.80 | 0.06 |
| VEGF (pg/mL) | <42.1 | 0.70 | 0.57–0.84 | 0.01 |
| Logistic Regression | Receiver Operator Characteristic Curve | |||||
|---|---|---|---|---|---|---|
| Predictors | Odds Ratio | 95% CI | p-Value | Cut-off Value | Sensitivity | Specificity |
| Univariate models | ||||||
| Age | 5.8 | 1.9–18.2 | 0.002 | <7.0 | 76% | 65% |
| BMI z-score | 8.3 | 2.5–27.1 | <0.001 | <1.44 | 78% | 70% |
| OSA-18 | 1.3 | 0.5–3.6 | 0.64 | >78.5 | 54% | 52% |
| OAHI | 3.6 | 1.0–12.7 | 0.045 | <4.0 | 43% | 83% |
| OAI | 2.0 | 0.7–5.9 | 0.19 | >0.6 | 57% | 61% |
| Mean SpO2 | 2.4 | 0.8–7.2 | 0.12 | >97.6 | 51% | 70% |
| Minimal SpO2 | 2.1 | 0.7–6.2 | 0.19 | >86.5 | 73% | 43% |
| IL-1ra | 4.2 | 1.4–12.7 | 0.01 | <149.2 | 73% | 61% |
| IL-9 | 5.9 | 1.7–20.4 | 0.01 | >82.8 | 87% | 48% |
| IL-10 | 5.1 | 1.6–15.6 | 0.01 | <0.5 | 73% | 65% |
| IL-15 | 11.1 | 2.3–54.2 | 0.003 | <11.8 | 51% | 91% |
| IL-17 | 19.2 | 2.2–167.2 | 0.01 | >4.7 | 97% | 35% |
| GM-CSF | 6.3 | 1.6–25.0 | 0.01 | <0.2 | 49% | 87% |
| MCP-1 | 11.3 | 2.2–58.7 | 0.004 | <51.2 | 95% | 39% |
| RANTES | 9.0 | 2.4–33.7 | 0.001 | >15435.5 | 89% | 52% |
| VEGF | 5.8 | 1.9–18.2 | 0.002 | <42.1 | 76% | 65% |
| Clinical model | ≥1 | 95% | 52% | |||
| Age < 7.0 years | 4.4 | 1.2–15.2 | 0.03 | |||
| BMI z-score < 1.44 | 6.6 | 1.9–22.8 | 0.003 | |||
| Inflammatory model | ≥3 | 87% | 87% | |||
| IL-1ra < 149.2 pg/mL | 8.3 | 1.3–53.9 | 0.03 | |||
| IL-17 > 4.7 pg/mL | 43.3 | 3.7–504.3 | 0.003 | |||
| GM-CSF < 0.2 pg/mL | 7.9 | 1.1–58.4 | 0.04 | |||
| MCP-1 < 51.2 pg/mL | 11.0 | 1.4–83.6 | 0.02 | |||
| Mixed model-1 | ≥3 | 87% | 96% | |||
| Age < 7.0 years | 11.6 | 2.3–90.8 | 0.004 | |||
| GM-CSF < 0.2 pg/mL | 8.1 | 1.2–54.9 | 0.03 | |||
| MCP-1 < 51.2 pg/mL | 23.8 | 2.6–229.8 | 0.01 | |||
| RANTES > 15435.5 pg/mL | 14.6 | 2.3–90.8 | 0.004 | |||
| Mixed model-2 | ≥3 | 92% | 78% | |||
| Age < 7.0 years | 2.1 | 1.3–56.0 | 0.02 | |||
| BMI z-score < 1.44 | 2.1 | 1.4–50.8 | 0.02 | |||
| MCP-1 < 51.2 pg/mL | 3.6 | 2.9–432.5 | 0.01 | |||
| RANTES > 15435.5 pg/mL | 3.1 | 2.7–191.5 | 0.004 | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chuang, H.-H.; Huang, C.-G.; Chuang, L.-P.; Huang, Y.-S.; Chen, N.-H.; Li, H.-Y.; Fang, T.-J.; Hsu, J.-F.; Lai, H.-C.; Chen, J.-Y.; et al. Relationships Among and Predictive Values of Obesity, Inflammation Markers, and Disease Severity in Pediatric Patients with Obstructive Sleep Apnea Before and After Adenotonsillectomy. J. Clin. Med. 2020, 9, 579. https://doi.org/10.3390/jcm9020579
Chuang H-H, Huang C-G, Chuang L-P, Huang Y-S, Chen N-H, Li H-Y, Fang T-J, Hsu J-F, Lai H-C, Chen J-Y, et al. Relationships Among and Predictive Values of Obesity, Inflammation Markers, and Disease Severity in Pediatric Patients with Obstructive Sleep Apnea Before and After Adenotonsillectomy. Journal of Clinical Medicine. 2020; 9(2):579. https://doi.org/10.3390/jcm9020579
Chicago/Turabian StyleChuang, Hai-Hua, Chung-Guei Huang, Li-Pang Chuang, Yu-Shu Huang, Ning-Hung Chen, Hsueh-Yu Li, Tuan-Jen Fang, Jen-Fu Hsu, Hsin-Chih Lai, Jau-Yuan Chen, and et al. 2020. "Relationships Among and Predictive Values of Obesity, Inflammation Markers, and Disease Severity in Pediatric Patients with Obstructive Sleep Apnea Before and After Adenotonsillectomy" Journal of Clinical Medicine 9, no. 2: 579. https://doi.org/10.3390/jcm9020579
APA StyleChuang, H.-H., Huang, C.-G., Chuang, L.-P., Huang, Y.-S., Chen, N.-H., Li, H.-Y., Fang, T.-J., Hsu, J.-F., Lai, H.-C., Chen, J.-Y., & Lee, L.-A. (2020). Relationships Among and Predictive Values of Obesity, Inflammation Markers, and Disease Severity in Pediatric Patients with Obstructive Sleep Apnea Before and After Adenotonsillectomy. Journal of Clinical Medicine, 9(2), 579. https://doi.org/10.3390/jcm9020579