Extent of Mucosal Inflammation in Ulcerative Colitis Influences the Clinical Remission Induced by Vedolizumab


 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Aim
2.2. Patients
2.3. Statistical Analysis
3. Results
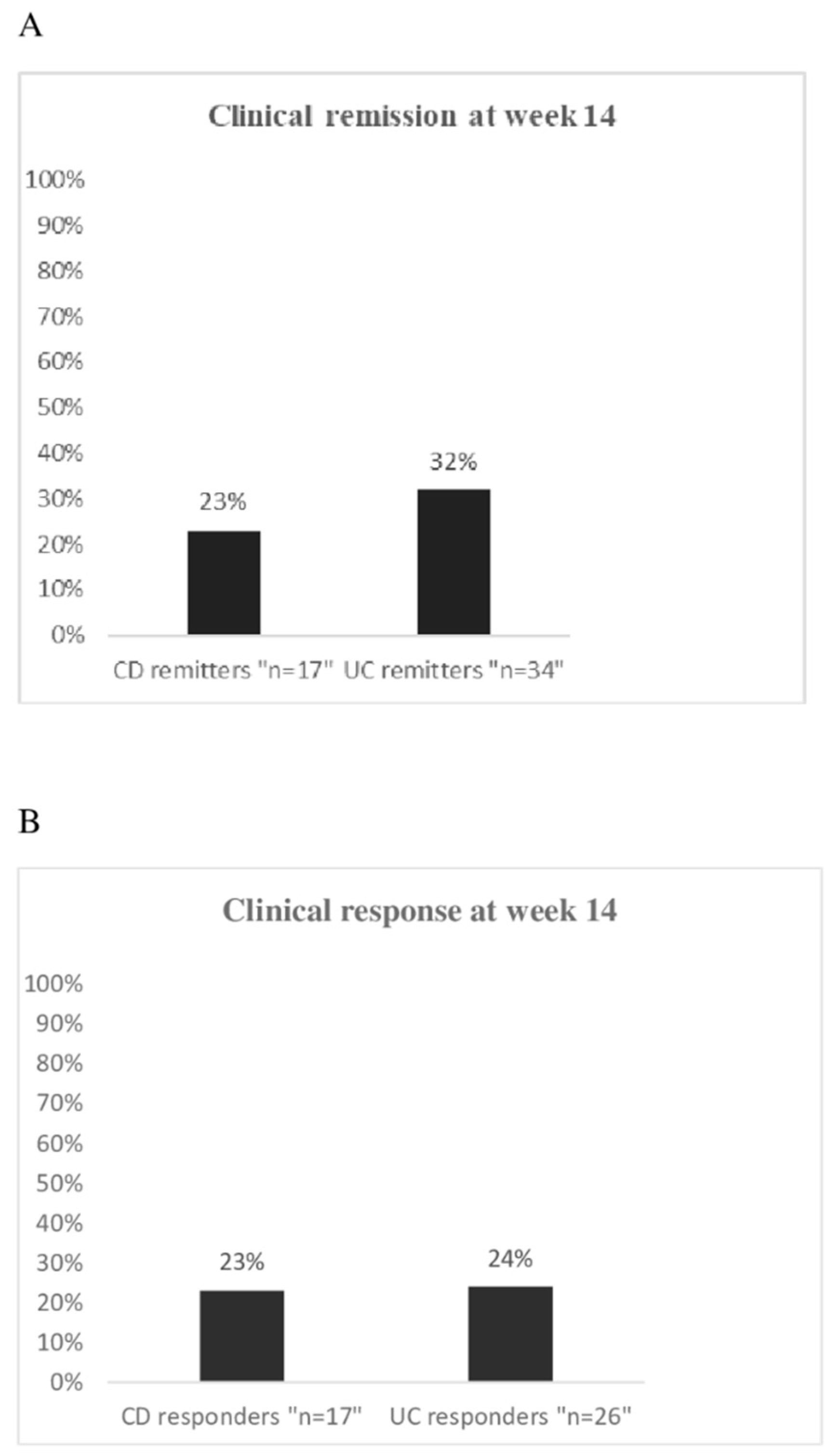
3.1. Induction of Clinical Remission
3.2. Predictive Factors of Remission
3.3. Clinical Response and Predictors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- Duijvestein, M.; Battat, R.; Vande, C.N.; D’Haens, G.R.; Sandborn, W.J.; Khanna, R.; Jairath, V.; Feagan, B.G. Novel Therapies and Treatment Strategies for Patients with Inflammatory Bowel Disease. Curr. Treat. Options Gastroenterol. 2018, 16, 129–146. [Google Scholar] [CrossRef]
- Argollo, M.; Fiorino, G.; Hindryckx, P.; Peyrin-Biroulet, L.; Danese, S. Novel therapeutic targets for inflammatory bowel disease. J. Autoimmun. 2017, 85, 103–116. [Google Scholar] [CrossRef] [PubMed]
- Katsanos, K.H.; Papadakis, K.A. Inflammatory Bowel Disease: Updates on Molecular Targets for Biologics. Gut Liver 2017, 11, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Chudy-Onwugaje, K.O.; Christian, K.E.; Farraye, F.A.; Cross, R.K. A State-of-the-Art Review of New Emerging Therapies for the Treatment of, I.B.D. Inflamm. Bowel Dis. 2019, 25, 820–830. [Google Scholar] [CrossRef] [PubMed]
- Danese, S.; Vuitton, L.; Peyrin-Biroulet, L. Biologic agents for IBD: Practical insights. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 537–545. [Google Scholar] [CrossRef]
- Soler, D.; Chapman, T.; Yang, L.L.; Wyant, T.; Egan, R.; Fedyk, E.R. The binding specificity and selective antagonism of vedolizumab, an anti-alpha4beta7 integrin therapeutic antibody in development for inflammatory bowel diseases. J. Pharm. Exp. 2009, 330, 864–875. [Google Scholar] [CrossRef]
- Erle, D.J.; Briskin, M.J.; Butcher, E.C.; Garcia-Pardo, A.; Lazarovits, A.I.; Tidswell, M. Expression and function of the MAdCAM−1 receptor, integrin alpha 4 beta 7, on human leukocytes. J. Immunol. 1994, 153, 517–528. [Google Scholar]
- Fedyk, E.R.; Wyant, T.; Yang, L.-L.; Csizmadia, V.; Burke, K.; Yang, H.; Kadambi, V.J. Exclusive antagonism of the α4β7 integrin by vedolizumab confirms the gut-selectivity of this pathway in primates. Inflamm. Bowel Dis. 2012, 18, 2107–2119. [Google Scholar] [CrossRef]
- Feagan, B.G.; Greenberg, G.R.; Wild, G.; Fedorak, R.N.; Paré, P.; McDonald, J.W.; Dubé, R.; Cohen, A.; Steinhart, A.H.; Landau, S.; et al. Treatment of ulcerative colitis with a humanized antibody to the alpha4beta7 integrin. N. Engl. J. Med. 2005, 352, 2499–2507. [Google Scholar] [CrossRef]
- Feagan, B.G.; Rutgeerts, P.; Sands, B.E.; Hanauer, S.; Colombel, J.F.; Sandborn, W.J.; Van Assche, G.; Axler, J.; Kim, H.J.; Danese, S.; et al. Vedolizumab as induction and maintenance therapy for ulcerative colitis. N. Engl. J. Med. 2013, 369, 699–710. [Google Scholar] [CrossRef]
- Sandborn, W.J.; Feagan, B.G.; Rutgeerts, P.; Hanauer, S.; Colombel, J.F.; Sands, B.E.; Lukas, M.; Fedorak, R.N.; Lee, S.; Bressler, B.; et al. Vedolizumab as induction and maintenance therapy for Crohn’s disease. N. Engl. J. Med. 2013, 369, 711–721. [Google Scholar] [CrossRef] [PubMed]
- Sands, B.E.; Feagan, B.G.; Rutgeerts, P.; Colombel, J.F.; Sandborn, W.J.; Sy, R.; D’Haens, G.; Ben-Horin, S.; Xu, J.; Rosario, M.; et al. Effects of vedolizumab induction therapy for patients with Crohn’s disease in whom tumor necrosis factor antagonist treatment had failed. Gastroenterology 2014, 147, 618–627. [Google Scholar] [CrossRef] [PubMed]
- Engel, T.; Ungar, B.; Yung, D.E.; Ben-Horin, S.; Eliakim, R.; Kopylov, U. Vedolizumab in IBD-lessons from real-world experience; a systematic review and pooled analysis. J. Crohns Colitis 2018, 12, 245–257. [Google Scholar] [CrossRef] [PubMed]
- Baumgart, D.C.; Bokemeyer, B.; Drabik, A.; Stallmach, A.; Schreiber, S.; Vedolizumab, G.C. Vedolizumab induction therapy for inflammatory bowel disease in clinical practice–a nationwide consecutive German cohort study. Aliment Pharm. 2016, 43, 1090–1102. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, C.; Marsal, J.; Bergemalm, D.; Vigren, L.; Björk, J.; Eberhardson, M.; Karling, P.; Söderman, C.; SWIBREGVedolizumab Study Group; Myrelid, P.; et al. Long-term effectiveness of vedolizumab in inflammatory bowel disease: A national study based on the Swedish National Quality Registry for Inflammatory Bowel Disease (SWIBREG). Scand. J. Gastroenterol. 2017, 52, 722–729. [Google Scholar] [CrossRef] [PubMed]
- Amiot, A.; Grimaud, J.C.; Peyrin-Biroulet, L.; Filippi, J.; Pariente, B.; Roblin, X.; Buisson, A.; Stefanescu, C.; Trang-Poisson, C.; Altwegg, R.; et al. Effectiveness and safety of vedolizumab induction therapy for patients with inflammatory bowel disease. Clin. Gastroenterol. Hepatol. 2016, 14, 1593–1601. [Google Scholar] [CrossRef]
- Kopylov, U.; Ron, Y.; Avni-Biron, I.; Koslowsky, B.; Waterman, M.; Daher, S.; Ungar, B.; Yanai, H.; Maharshak, N.; Ben-Bassat, O.; et al. Efficacy and safety of vedolizumab for induction of remission in inflammatory bowel disease-the Israeli real-world experience. Inflamm. Bowel Dis. 2017, 23, 404–408. [Google Scholar] [CrossRef]
- Vivio, E.E.; Kanuri, N.; Gilbertsen, J.J.; Monroe, K.; Dey, N.; Chen, C.H.; Gutierrez, A.M.; Ciorba, M.A. Vedolizumab effectiveness and safety over the first year of use in an IBD clinical practice. J. Crohns Colitis 2016, 10, 402–409. [Google Scholar] [CrossRef]
- Dulai, P.S.; Singh, S.; Jiang, X.; Peerani, F.; Narula, N.; Chaudrey, K.; Whitehead, D.; Hudesman, D.; Lukin, D.; Swaminath, A.; et al. The real-world effectiveness and safety of vedolizumab for moderate-severe Crohn’s disease: Results from the US VICTORY consortium. Am. J. Gastroenterol. 2016, 111, 1147–1155. [Google Scholar] [CrossRef]
- Narula, N.; Peerani, F.; Meserve, J.; Kochhar, G.; Chaudrey, K.; Hartke, J.; Chilukuri, P.; Koliani-Pace, J.; Winters, A.; Katta, L.; et al. Vedolizumab for ulcerative colitis: Treatment outcomes from the VICTORY consortium. Am. J. Gastroenterol. 2018, 113, 1345–1354. [Google Scholar] [CrossRef]
- Vermeire, S.; Loftus, E.V.; Colombel, J.F.; Feagan, B.G.; Sandborn, W.J.; Sands, B.E.; Danese, S.; D’Haens, G.R.; Kaser, A.; Panaccione, R.; et al. Long-term effectiveness and safety of vedolizumab in patients with Crohn’s disease: 5-year cumulative exposure of GEMINI 2 completers rolling into the GEMINI open-label extension study. Gastroenterology 2017, 152, S601. [Google Scholar]
- Amiot, A.; Serrero, M.; Peyrin-Biroulet, L.; Filippi, J.; Pariente, B.; Roblin, X.; Buisson, A.; Stefanescu, C.; Trang-Poisson, C.; Altwegg, R.; et al. One-year effectiveness and safety of vedolizumab therapy for inflammatory bowel disease: A prospective multicentre cohort study. Aliment Pharm. 2017, 46, 310–321. [Google Scholar] [CrossRef] [PubMed]
- Amiot, A.; Serrero, M.; Peyrin-Biroulet, L.; Filippi, J.; Pariente, B.; Roblin, X.; Buisson, A.; Stefanescu, C.; Trang-Poisson, C.; Altwegg, R.; et al. Three-year effectiveness and safety of vedolizumab therapy for inflammatory bowel disease: A prospective multi-centre cohort study. Alim. Pharm. Ther. 2019, 50, 40–53. [Google Scholar] [CrossRef] [PubMed]
- Feagan, B.G.; Rubin, D.T.; Danese, S.; Vermeire, S.; Abhyankar, B.; Sankoh, S.; James, A.; Smyth, M. Efficacy of vedolizumab induction and maintenance therapy in patients with ulcerative colitis, regardless of prior exposure to tumor necrosis factor antagonists. Clin. Gastroenterol. Hepatol. 2017, 15, 229–239. [Google Scholar] [CrossRef] [PubMed]
- Sands, B.E.; Sandborn, W.J.; Van Assche, G.; Lukas, M.; Xu, J.; James, A.; Abhyankar, B.; Lasch, K. Vedolizumab as induction and maintenance therapy for Crohn’s disease in patients naïve to or who have failed tumor necrosis factor antagonist therapy. Inflamm. Bowel Dis. 2017, 23, 97–106. [Google Scholar] [CrossRef] [PubMed]
- Stallmach, A.; Langbein, C.; Atreya, R.; Bruns, T.; Dignass, A.; Ende, K.; Hampe, J.; Hartmann, F.; Neurath, M.F.; Maul, J.; et al. Vedolizumab provides clinical benefit over 1 year in patients with active inflammatory bowel disease—A prospective multicenter observational study. Aliment. Pharm. 2016, 44, 1199–1212. [Google Scholar] [CrossRef]
- Danese, S.; Sandborn, W.J.; Colombel, J.F.; Vermeire, S.; Glover, S.C.; Rimola, J.; Siegelman, J.; Jones, S.; Bornstein, J.D.; Feagan, B.G. Endoscopic; radiologic; and histologic healing with vedolizumab in patients with active Crohn’s disease. Gastroenterology 2019, 157, 1007–1018. [Google Scholar] [CrossRef]
- Shelton, E.; Allegretti, J.R.; Stevens, B.; Lucci, M.; Khalili, H.; Nguyen, D.D.; Sauk, J.; Giallourakis, C.; Garber, J.; Hamilton, M.J.; et al. Efficacy of vedolizumab as induction therapy in refractory IBD patients: A multicenter cohort. Inflamm. Bowel Dis. 2015, 21, 2879–2885. [Google Scholar] [CrossRef]
- Allegretti, J.R.; Barnes, E.L.; Stevens, B.; Storm, M.; Ananthakrishnan, A.; Yajnik, V.; Korzenik, J. Predictors of clinical response and remission at 1 year among a multicenter cohort of patients with inflammatory bowel disease treated with vedolizumab. Dig. Dis. Sci. 2017, 62, 1590–1596. [Google Scholar] [CrossRef]
- Lenti, M.V.; Levison, S.; Eliadou, E. A real-world, long-term experience on effectiveness and safety of vedolizumab in adult patients with inflammatory bowel disease: The Cross Pennine study. Dig. Liver Dis. 2018, 50, 1299–1304. [Google Scholar] [CrossRef]
- Digby-Bell, J.L.; Atreya, R.; Monteleone, G.; Powell, N. Interrogating host immunity to predict treatment response in inflammatory bowel disease. Nat. Rev. Gastroenterol. Hepatol. 2019, 17, 9–20. [Google Scholar] [CrossRef] [PubMed]
- Rosario, M.; Dirks, N.L.; Gastonguay, M.R.; Fasanmade, A.A.; Wyant, T.; Parikh, A.; Sandborn, W.J.; Feagan, B.G.; Reinisch, W.; Fox, I. Population pharmacokinetics-pharmacodynamics of vedolizumab in patients with ulcerative colitis and Crohn’s disease. Aliment Pharm. 2015, 42, 188–202. [Google Scholar] [CrossRef] [PubMed]
- Rosario, M.; French, J.L.; Dirks, N.L.; Sankoh, S.; Parikh, A.; Yang, H.; Danese, S.; Colombel, J.F.; Smyth, M.; Sandborn, W.J.; et al. Exposure-efficacy relationships for vedolizumab induction therapy in patients with ulcerative colitis or Crohn’s disease. J. Crohn’s Colitis 2017, 11, 921–929. [Google Scholar] [CrossRef] [PubMed]
- Williet, N.; Boschetti, G.; Fovet, M.; Di Bernado, T.; Claudez, P.; Del Tedesco, E.; Jarlot, C.; Rinaldi, L.; Berger, A.; Phelip, J.M.; et al. Association between low trough levels of vedolizumab during induction therapy for inflammatory bowel diseases and need for additional doses within 6 months. Clin. Gastroenterol. Hepatol. 2016, 15, 1750–1757. [Google Scholar] [CrossRef] [PubMed]
- Pouillon, L.; Rousseau, H.; Busby-Venner, H.; De Carvalho Bittencourt, M.; Choukour, M.; Gauchotte, G.; Zallot, C.; Danese, S.; Baumann, C.; Peyrin-Biroulet, L. Vedolizumab Trough Levels and Histological Healing During Maintenance Therapy in Ulcerative Colitis. J. Crohns Colitis 2019, 13, 970–975. [Google Scholar] [CrossRef] [PubMed]
- Liefferinckx, C.; Minsart, C.; Cremer, A.; Amininejad, L.; Tafciu, V.; Quertinmont, E.; Tops, S.; Devière, J.; Gils, A.; van Gossum, A.; et al. Early vedolizumab trough levels at induction in inflammatory bowel disease patients with treatment failure during maintenance. Eur. J. Gastroenterol. Hepatol. 2019, 31, 478–485. [Google Scholar] [CrossRef]
- Al-Bawardy, B.; Ramos, G.P.; Willrich, M.A.V.; Jenkins, S.M.; Park, S.H.; Aniwan, S.; Schoenoff, S.A.; Bruining, D.H.; Papadakis, K.A.; Raffals, L.; et al. Vedolizumab Drug Level Correlation with Clinical Remission, Biomarker Normalization, and Mucosal Healing in Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2019, 25, 580–586. [Google Scholar] [CrossRef]
- Dreesen, E.; Verstockt, B.; Bian, S.; de Bruyn, M.; Compernolle, G.; Tops, S.; Noman, M.; Van Assche, G.; Ferrante, M.; Gils, A.; et al. Evidence to Support Monitoring of Vedolizumab Trough Concentrations in Patients with Inflammatory Bowel Diseases. Clin. Gastroenterol. Hepatol. 2018, 16, 1937–1946. [Google Scholar] [CrossRef]
- Pouillon, L.; Vermeire, S.; Bossuyt, P. Vedolizumab trough level monitoring in inflammatory bowel disease: A state-of-the-art overview. Bmc. Med. 2019, 17, 89. [Google Scholar] [CrossRef]
- Rath, T.; Billmeier, U.; Ferrazzi, F.; Vieth, M.; Ekici, A.; Neurath, M.F.; Atreya, R. Effects of Anti-Integrin Treatment with Vedolizumab on Immune Pathways and Cytokines in Inflammatory Bowel Diseases. Front Immunol. 2018, 31, 1700. [Google Scholar] [CrossRef]
- Dulai, P.S.; Singh, S.; Vande Casteele, N.; Boland, B.S.; Rivera-Nieves, J.; Ernst, P.B.; Eckmann, L.; Barrett, K.E.; Chang, J.T.; Sandborn, W.J. Should We Divide Crohn’s Disease into Ileum-Dominant and Isolated Colonic Diseases? Clin. Gastroenterol. Hepatol. 2019, 19, 304–306. [Google Scholar] [CrossRef] [PubMed]
- Ichikawa, R.; Lamb, C.A.; Eastham-Anderson, J.; Scherl, A.; Raffals, L.; Faubion, W.A.; Bennett, M.R.; Long, A.K.; Mansfield, J.C.; Kirby, J.A.; et al. AlphaE Integrin Expression Is Increased in the Ileum Relative to the Colon and Unaffected by Inflammation. J. Crohns Coliti. 2018, 12, 1191–1199. [Google Scholar] [CrossRef] [PubMed]
- Elewaut, D.; Van Damme, N.; De Keyser, F.; Scherl, A.; Raffals, L.; Faubion, W.A.; Bennett, M.R.; Long, A.K.; Mansfield, J.C.; Kirby, J.A.; et al. Altered expression of alpha E beta 7 integrin on intra-epithelial and lamina propria lymphocytes in patients with Crohn’s disease. Acta. Gastroenterol. Belg. 1998, 61, 288–294. [Google Scholar] [PubMed]
- Zundler, S.; Fischer, A.; Schillinger, D.; Binder, M.T.; Atreya, R.; Rath, T.; Lopez-Pósadas, R.; Voskens, C.J.; Watson, A.; Atreya, I.; et al. The α4β1 Homing Pathway Is Essential for Ileal Homing of Crohn’s Disease Effector T Cells In Vivo. Inflamm. Bowel Dis. 2017, 23, 379–391. [Google Scholar] [CrossRef] [PubMed]
- Gomollón, F.; Dignass, A.; Annese, V.; Tilg, H.; Van Assche, G.; Lindsay, J.O.; Peyrin-Biroulet, L.; Cullen, G.J.; Daperno, M.; Kucharzik, T.; et al. 3rd European Evidence-based Consensus on the Diagnosis and Management of Crohn’s Disease 2016: Part 1: Diagnosis and Medical Management. J. Crohn’s Colitis 2017, 11, 3–25. [Google Scholar]
- Magro, F.; Gionchetti, P.; Eliakim, R.; Ardizzone, S.; Armuzzi, A.; Barreiro-de Acosta, M.; Burisch, J.; Gecse, K.B.; Hart, A.L.; Hindryckx, P.; et al. Third European Evidence-based Consensus on Diagnosis and Management of Ulcerative Colitis. Part 1: Definitions, Diagnosis, Extra-intestinal Manifestations, Pregnancy, Cancer Surveillance, Surgery, and Ileo-anal Pouch Disorders. J. Crohn’s Colitis 2017, 11, 649–670. [Google Scholar]
- Lewis, J.D.; Chuai, S.; Nessel, L.; Lichtenstein, G.R.; Aberra, F.N.; Ellenberg, J.H. Use of the noninvasive components of the Mayo score to assess clinical response in ulcerative colitis. Inflamm. Bowel Dis. 2008, 14, 1660–1666. [Google Scholar] [CrossRef]
- Harvey, R.F.; Bradshaw, J.M. A simple index of Crohn’s Disease activity. Lancet 1980, 1, 514. [Google Scholar] [CrossRef]
- Zundler, S.; Becker, E.; Schulze, L.L.; Neurath, M.F. Immune cell trafficking and retention in inflammatory bowel disease: Mechanistic insights and therapeutic advances. Gut 2019, 68, 1688–1700. [Google Scholar] [CrossRef]
- De Bruyn, J.R.; Becker, M.A.; Steenkamer, J.; Wildenberg, M.E.; Meijer, S.L.; Buskens, C.J.; Bemelman, W.A.; Löwenberg, M.; Ponsioen, C.Y.; van den Brink, G.R.; et al. Intestinal fibrosis is associated with lack of response to Infliximab therapy in Crohn’s disease. PLoS ONE 2018, 13, e0190999. [Google Scholar] [CrossRef]
- Gisbert, J.P.; Chaparro, M. Predictors of primary response to biologic treatment (anti-TNF, vedolizumab and ustekinumab) in patients with inflammatory bowel disease: From basic science to clinical practice. J. Crohns Colitis 2019. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.M.; Randall, C.; Betancourt, R.; Keene, S.; Lilly, A.; Fowler, M.; Dellon, E.S.; Herfarth, H.H. Mucosal Eosinophilia Is an Independent Predictor of Vedolizumab Efficacy in Inflammatory Bowel Diseases. Inflamm. Bowel Dis. 2019, 21. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Crohn’s Disease (n = 74) | Ulcerative Colitis (n = 107) |
|---|---|---|
| median age, years (IQR) | 42 (33–55) | 46 (32–56) |
| median disease duration from IBD diagnosis, years (IQR) | 14 (10–23) | 11 (7–19) |
| male gender, n (%) | 34 (46%) | 56 (52%) |
| smoking status, n (%) | ||
| never | 34 (46%) | 74 (69%) |
| former | 19 (26%) | 19 (18%) |
| current | 21 (28%) | 14 (13%) |
| Montreal disease location, n (%) | ||
| L1 (ileal disease) | 20 (27%) | |
| L2 (colonic disease) | 7 (9%) | |
| L3 (ileo-colonic disease) | 47 (64%) | |
| E1 (proctitis) | 3 (3%) | |
| E2 (left-sided colitis) | 37 (34%) | |
| E3 (extensive colitis) | 67 (63%) | |
| upper disease location, n (%) | 15 (20%) | |
| Montreal disease behavior, n (%) | ||
| B1 (non-stricturing, non-penetrating) | 24 (32%) | |
| B2 (stricturing) | 23 (31%) | |
| B3 (penetrating) | 27 (37%) | |
| Mild Clinical Activity | 26 (35%) | 31 (29%) |
| Moderate Clinical Activity | 45 (61%) | 64 (60%) |
| Severe Clinical Activity | 3 (4%) | 12 (11%) |
| perianal disease, n (%) | 23 (31%) | |
| prior ileo-colonic resection, n (%) | 44 (59%) | |
| prior TNF antagonists, n (%) * | 63 (85%) | 86 (80%) |
| Variable | Estimate (CD) | p-Value (CD) | Estimate (UC) | p-Value (UC) |
|---|---|---|---|---|
| prior anti-TNF | 6.293 | 0.111 | 2.298 | 0.259 |
| prior immunosuppressive therapy | 1.563 | 0.734 | 0.927 | 0.910 |
| concomitant steroids | 3.126 | 0.265 | 0.889 | 0.838 |
| concomitant immunosuppressive therapy | 17.467 | 0.112 | 2.296 | 0.437 |
| male gender | 59.636 | 0.010 | 1.983 | 0.227 |
| CRP > 5 mg/L | 5.428 | 0.122 | 1.396 | 0.558 |
| current smoker | 3.206 | 0.361 | 1.210 | 0.831 |
| ex smoker | 0.283 | 0.357 | 0.976 | 0.976 |
| clinical activity | 0.356 | 0.0007 | 0.676 | 0.037 |
| disease duration from IBD diagnosis | 1.144 | 0.062 | 0.987 | 0.663 |
| colonic disease | 2.941 | 0.445 | ||
| Ileo-colonic disease | 8.801 | 0.148 | ||
| Distal/left-sided colitis | 2.154 | 0.0003 | ||
| Extensive colitis | 0.116 | 0.0003 | ||
| upper disease | 4.776 | 0.297 | ||
| stricturing disease | 22.079 | 0.047 | ||
| penetrating disease | 1.709 | 0.727 | ||
| perianal disease | 1.507 | 0.743 | ||
| prior ileo-colonic resection | 0.715 | 0.802 |
| Variable | Estimate (CD) | p-Value (CD) | Estimate (UC) | p-Value (UC) |
|---|---|---|---|---|
| prior anti-TNF | 0.118 | 0.411 | 2.111 | 0.341 |
| prior immunosuppressive therapy | 8.920 | 0.159 | 1.144 | 0.830 |
| concomitant steroids | 3.705 | 0.187 | 0.814 | 0.721 |
| Concomitant immunosuppressive therapy | 21.030 | 0.024 | 4.533 | 0.121 |
| male gender | 1.942 | 0.484 | 0.714 | 0.537 |
| CRP >5 mg/L | 4.276 | 0.153 | 0.742 | 0.595 |
| current smoker | 1.268 | 0.813 | 2.494 | 0.250 |
| ex smoker | 0.398 | 0.491 | 1.349 | 0.692 |
| clinical activity | 0.687 | 0.021 | 1.052 | 0.798 |
| disease duration from IBD diagnosis | 0.996 | 0.953 | 0.951 | 0.156 |
| colonic disease | 3.610 | 0.445 | ||
| Ileo-colonic disease | 0.768 | 0.814 | ||
| Distal/left-sided colitis | 1.081 | 0.084 | ||
| Extensive colitis | 0.339 | 0.084 | ||
| upper disease | 2.712 | 0.403 | ||
| stricturing disease | 1.352 | 0.791 | ||
| penetrating disease | 0.033 | 0.037 | ||
| perianal disease | 7.565 | 0.133 | ||
| prior ileo-colonic resection | 0.756 | 0.828 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scarozza, P.; Marafini, I.; Laudisi, F.; Troncone, E.; Schmitt, H.; Lenti, M.V.; Costa, S.; Rocchetti, I.; De Cristofaro, E.; Salvatori, S.; et al. Extent of Mucosal Inflammation in Ulcerative Colitis Influences the Clinical Remission Induced by Vedolizumab. J. Clin. Med. 2020, 9, 385. https://doi.org/10.3390/jcm9020385
Scarozza P, Marafini I, Laudisi F, Troncone E, Schmitt H, Lenti MV, Costa S, Rocchetti I, De Cristofaro E, Salvatori S, et al. Extent of Mucosal Inflammation in Ulcerative Colitis Influences the Clinical Remission Induced by Vedolizumab. Journal of Clinical Medicine. 2020; 9(2):385. https://doi.org/10.3390/jcm9020385
Chicago/Turabian StyleScarozza, Patrizio, Irene Marafini, Federica Laudisi, Edoardo Troncone, Heike Schmitt, Marco Vincenzo Lenti, Stefania Costa, Irene Rocchetti, Elena De Cristofaro, Silvia Salvatori, and et al. 2020. "Extent of Mucosal Inflammation in Ulcerative Colitis Influences the Clinical Remission Induced by Vedolizumab" Journal of Clinical Medicine 9, no. 2: 385. https://doi.org/10.3390/jcm9020385
APA StyleScarozza, P., Marafini, I., Laudisi, F., Troncone, E., Schmitt, H., Lenti, M. V., Costa, S., Rocchetti, I., De Cristofaro, E., Salvatori, S., Frezzati, L., Di Sabatino, A., Atreya, R., Neurath, M. F., Calabrese, E., & Monteleone, G. (2020). Extent of Mucosal Inflammation in Ulcerative Colitis Influences the Clinical Remission Induced by Vedolizumab. Journal of Clinical Medicine, 9(2), 385. https://doi.org/10.3390/jcm9020385