Multidisciplinary Approach for the Management and Treatment of Diabetic Foot Infections with a Resorbable, Gentamicin-Loaded Bone Graft Substitute



 and
and
Abstract
1. Introduction
2. Experimental Section
2.1. Patients
2.2. Surgical Technique
2.3. Surgical and Post-Operative Management
2.4. Data collection and Outcome Parameters
3. Results
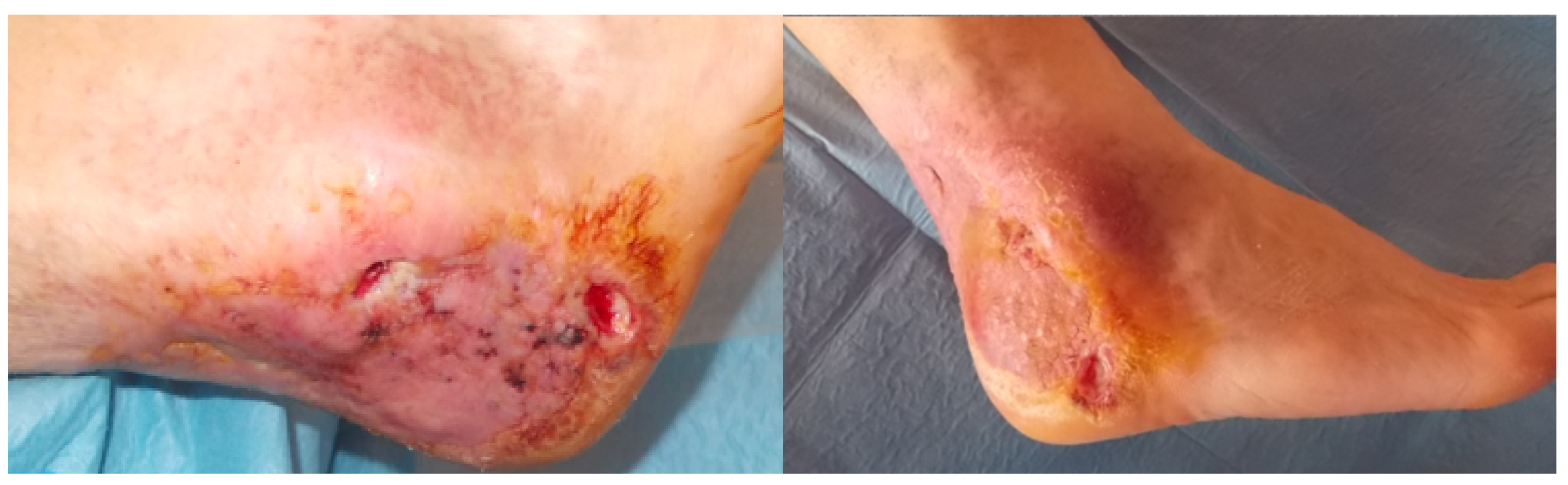
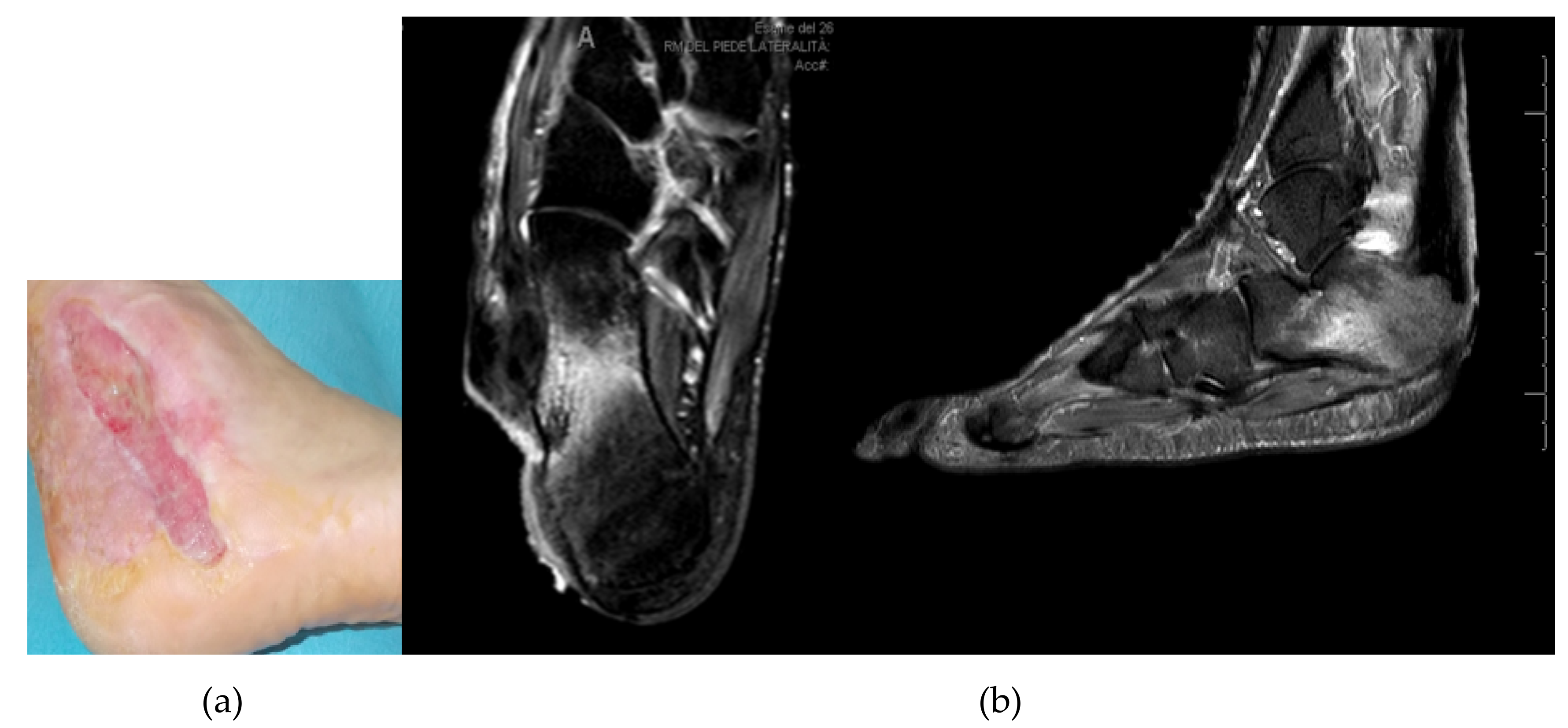
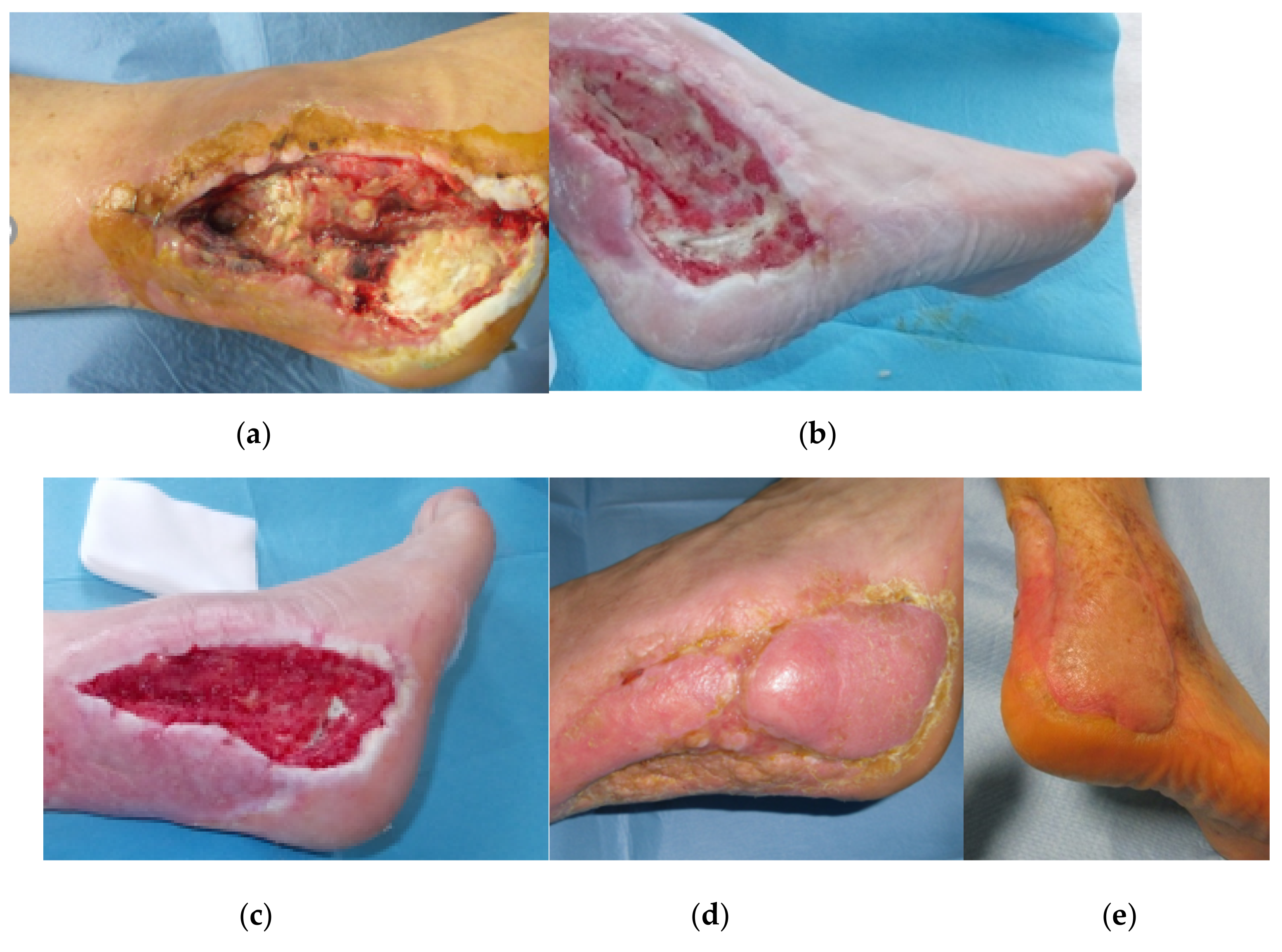
3.1. Calcaneal Lesions
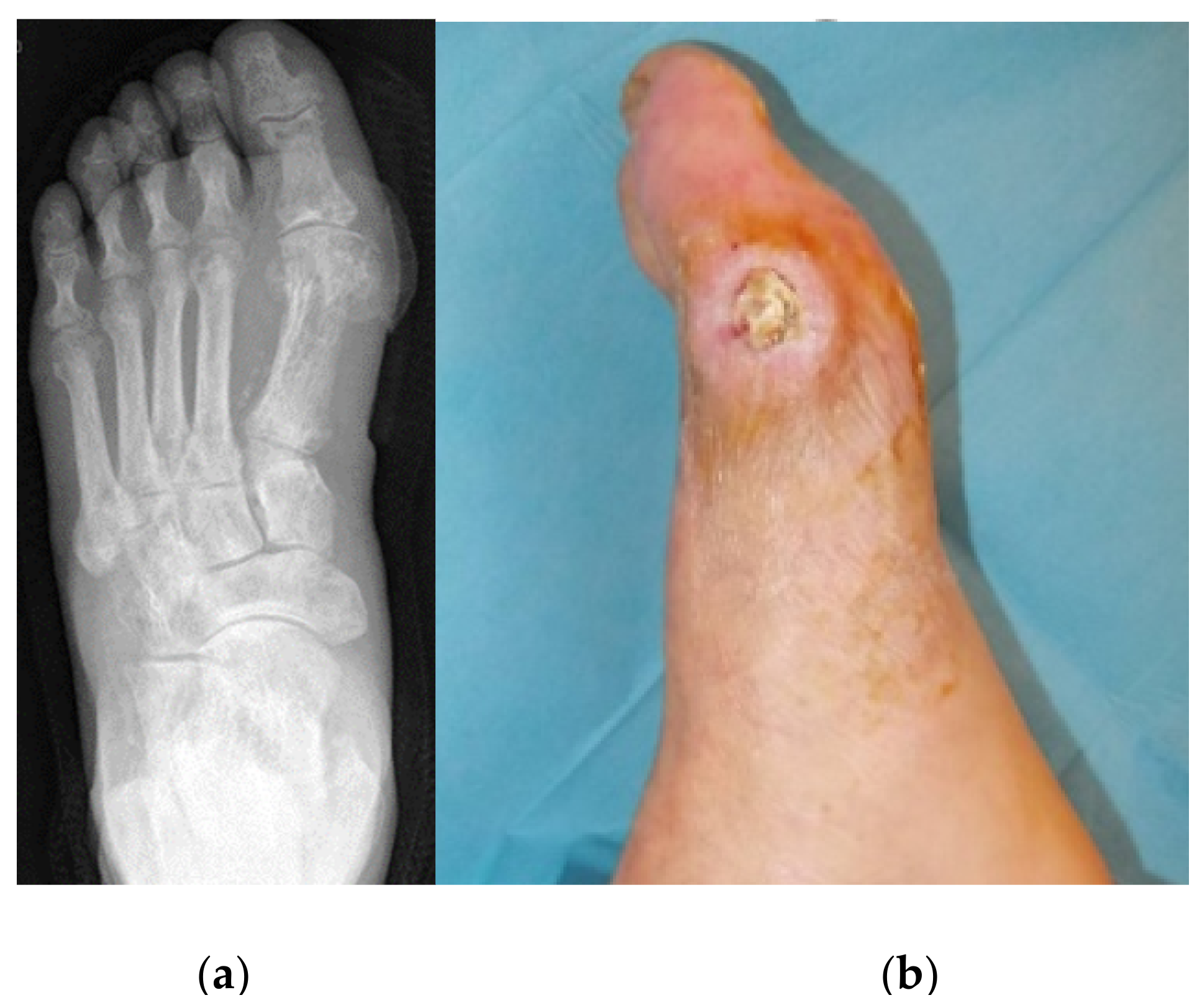
3.2. Metatarsal Lesions
3.3. Lesions Involving Distal Tarsus & Talus
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Margolis, D.J.; Kantor, J.; Berlin, J.A. Healing of diabetic neuropathic foot ulcers receiving standard treatment. A meta-analysis. Diabetes Care 1999, 22, 692–695. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization—Global Report on Diabetes. Available online: https://www.who.int/diabetes/global-report/en/ (accessed on 15 August 2020).
- Ertugrul, B.M.; Lipsky, B.A.; Savk, O. Osteomyelitis or Charcot neuro-osteoarthropathy? Differentiating these disorders in diabetic patients with a foot problem. Diabet. Foot Ankle 2013, 4. [Google Scholar] [CrossRef] [PubMed]
- Elraiyah, T.; Domecq, J.P.; Prutsky, G.; Tsapas, A.; Nabhan, M.; Frykberg, R.G.; Hasan, R.; Firwana, B.; Prokop, L.J.; Murad, M.H. A systematic review and meta-analysis of débridement methods for chronic diabetic foot ulcers. J. Vasc. Surg. 2016, 63, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Reiber, G.; Lipsky, B.; Gibbons, G. The burden of diabetic foot ulcers. Am. J. Surg. 1998, 176, 5–10. [Google Scholar] [CrossRef]
- American Diabetes Association. Consensus Development Conference on Diabetic Foot Wound Care: 7-8 April 1999, Boston, Massachusetts. Diabetes Care 1999, 22, 1354–1360. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, D.G.; Lavery, L.A.; Harkless, L.B. Validation of a diabetic wound classification system: The contribution of depth, infection, and ischemia to risk of amputation. Diabetes Care 1998, 21, 855–859. [Google Scholar] [CrossRef]
- Wagner, F.W., Jr. The dysvascular foot: A system for diagnosis and treatment. Foot Ankle Int. 1981, 2, 64–122. [Google Scholar] [CrossRef]
- Parisi, M.C.; Godoy-Santos, A.L.; Ortiz, R.T.; Sposeto, R.B.; Sakaki, M.H.; Nery, M.; Fernandes, T.D. Radiographic and functional results in the treatment of early stages of Charcot neuroarthropathy with a walker boot and immediate weight bearing. Diabet. Foot Ankle 2013, 4, 22487. [Google Scholar] [CrossRef] [PubMed]
- Kaynak, G.; Birsel, O.; Fatih Güven, M.; Öğüt, T. An overview of the Charcot foot pathophysiology. Diabetes Foot Ankle 2013, 4, 21117. [Google Scholar] [CrossRef]
- Siebachmeyer, M.; Boddu, K.; Bilal, A.; Hester, T.W.; Hardwick, T.; Fox, T.P.; Edmonds, M.; Kavarthapuet, V. Outcome of one-stage correction of deformities of the ankle and hindfoot and fusion in Charcot neuroarthropathy using a retrograde intramedullary hindfoot arthrodesis nail. Bone Jt. J. 2015, 97, 76–82. [Google Scholar] [CrossRef]
- Boyko, E.J.; Ahroni, J.H.; Stensel, V.; Forsberg, R.C.; Davignon, D.R.; Smith, D.G. A prospective study of risk factors for diabetic foot ulcer. The Seattle Diabetic Foot Study. Diabetes Care 1999, 22, 1036–1042. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, N.; Vaughan, P.; Varty, K.; Coll, A.P.; Robinson, A.H.N. Outcome of limited forefoot amputation with primary closure in patients with diabetes. Bone Jt. J 2013, 95, 1083–1087. [Google Scholar] [CrossRef] [PubMed]
- Jeffcoate, W.J.; Harding, K.G. Diabetic foot ulcers. Lancet 2003, 361, 1545–1551. [Google Scholar] [CrossRef]
- Gates, L.; Blume, P.A.; Sumpio, B.E. Surgical treatment principles for diabetic wounds complicated by osteomyelitis. In Osteomyelitis of the Foot and Ankle; Boffeli, T., Ed.; Springer: Cham/Heidelberg, Germany, 2015; pp. 99–111. [Google Scholar] [CrossRef]
- Dubský, M.; Jirkovská, A.; Bem, R.; Fejfarová, V.; Skibová, J.; Schaper, N.C.; Lipsky, B.A. Risk factors for recurrence of diabetic foot ulcers: Prospective follow-up analysis in the Eurodiale subgroup. Int. Wound J. 2013, 10, 555–561. [Google Scholar] [CrossRef]
- Brocco, E.; Ninkovic, S.; Marin, M.; Whisstock, C.; Bruseghin, M.; Boschetti, G.; Viti, R.; Forlini, W.; Volpe, A. Diabetic foot management: Multidisciplinary approach for advanced lesion rescue. J. Card. Surg. 2018, 59, 670–684. [Google Scholar] [CrossRef]
- Boulton, A.J.; Vileikyte, L.; Ragnarson-Tennvall, G.; Apelqvist, J. The global burden of diabetic foot disease. Lancet 2005, 366, 1719–1724. [Google Scholar] [CrossRef]
- Stravinskas, M.; Horstmann, P.; Ferguson, J.; Hettwer, W.; Nilsson, M.; Tarasevicius, S.; Petersen, M.M.; McNally, M.A.; Lidgren, L. Pharmacokinetics of gentamicin eluted from a regenerating bone graft substitute: In vitro and clinical release studies. Bone Jt. Res 2016, 5, 427–435. [Google Scholar] [CrossRef]
- Stravinskas, M.; Nilsson, M.; Horstmann, P.; Petersen, M.M.; Tarasevicius, S.; Lidgren, L. Antibiotic containing bone substitute in major hip surgery: A long term gentamicin elution study. J. Bone Jt. Infect 2018, 3, 68. [Google Scholar] [CrossRef][Green Version]
- Stravinskas, M.; Tarasevicius, S.; Laukaitis, S.; Nilsson, M.; Raina, D.B.; Lidgren, L. A ceramic bone substitute containing gentamicin gives good outcome in trochanteric hip fractures treated with dynamic hip screw and in revision of total hip arthroplasty: A case series. BMC Musculoskelet Disord 2018, 19, 438. [Google Scholar] [CrossRef]
- McNally, M.A.; Ferguson, J.Y.; Lau, A.C.K.; Diefenbeck, M.; Scarborough, M.; Ramsden, A.J.; Atkins, B.L. Single-stage treatment of chronic osteomyelitis with a new absorbable, gentamicin-loaded, calcium sulphate/hydroxyapatite biocomposite: A prospective series of 100 cases. Bone Jt. J 2016, 98, 1289–1296. [Google Scholar] [CrossRef]
- Acharya, S.; Soliman, M.; Egun, A.; Rajbhandari, S.M. Conservative management of diabetic foot osteomyelitis. Diabetes Res. Clin. Pract. 2013, 101, 18–20. [Google Scholar] [CrossRef] [PubMed]
- Senneville, E.; Lombart, A.; Beltrand, E.; Valette, M.; Legout, L.; Cazaubiel, M.; Yazdanpanah, Y.; Fontaine, P. Outcome of diabetic foot osteomyelitis treated nonsurgically: A retrospective cohort study. Diabetes Care 2008, 31, 637–642. [Google Scholar] [CrossRef] [PubMed]
- Game, F.L.; Jeffcoate, W.J. Primarily non-surgical management of osteomyelitis of the foot in diabetes. Diabetologia 2008, 51, 962–967. [Google Scholar] [CrossRef] [PubMed]
- Peters, E.J.; Lipsky, B.A. Diagnosis and management of infection in the diabetic foot. Med. Clin. N. Am. 2013, 97, 911–946. [Google Scholar] [CrossRef] [PubMed]
- Gogia, J.S.; Meehan, J.P.; Di Cesare, P.E.; Jamali, A.A. Local antibiotic therapy in osteomyelitis. In Seminars in Plastic Surgery; Colen, L., Salgado, C., Eds.; Thieme Medical Publishers: New York, NY, USA, 2009; Volume 23, pp. 100–107. [Google Scholar] [CrossRef]
- Malhotra, R.; Chan, C.S.Y.; Nather, A. Osteomyelitis in the diabetic foot. Diabet. Foot Ankle 2014, 5, 24445. [Google Scholar] [CrossRef] [PubMed]
- Paola, L.D.; Ceccacci, T.; Ninkovic, S.; Sorgentone, S.; Marinescu, M.G.; Volpe, A. Limb salvage in Charcot foot and ankle osteomyelitis: Combined use single stage/double stage of arthrodesis and external fixation. Foot Ankle Int. 2009, 30, 1065–1070. [Google Scholar] [CrossRef]
- Shojaiefard, A.; Khorgami, Z.; Mohajeri-Tehrani, M.R.; Larijani, B. Large and deep diabetic heel ulcers need not lead to amputation. Foot Ankle Int. 2013, 34, 215–221. [Google Scholar] [CrossRef]
- Faglia, E.; Clerici, G.; Caminiti, M.; Curci, V.; Somalvico, F. Influence of osteomyelitis location in the foot of diabetic patients with transtibial amputation. Foot Ankle Int. 2013, 34, 222–227. [Google Scholar] [CrossRef] [PubMed]
- Pickwell, K.M.; Siersma, V.D.; Kars, M.; Holstein, P.E.; Schaper, N.C. Eurodiale Concortium. Diabetic foot disease: Impact of ulcer location on ulcer healing. Diabetes Metab. Res. Rev. 2013, 29, 377–383. [Google Scholar] [CrossRef]
- Buchholz, H.W.; Engelbrecht, H. Depot effects of various antibiotics mixed with Palacos resins. Chirurg 1970, 41, 511–515. [Google Scholar]
- Schade, V.L.; Roukis, T.S. The role of polymethylmethacrylate antibiotic–loaded cement in addition to debridement for the treatment of soft tissue and osseous infections of the foot and ankle. J. Foot Ankle Surg. 2010, 49, 55–62. [Google Scholar] [CrossRef]
- Walenkamp, G.H.; Kleijn, L.L.; de Leeuw, M. Osteomyelitis treated with gentamicin-PMMA beads: 100 patients followed for 1–12 years. Acta Orthop. Scand. 1998, 69, 518–522. [Google Scholar] [CrossRef]
- Chang, W.; Colangeli, M.; Colangeli, S.; Di Bella, C.; Gozzi, E.; Donati, D. Adult osteomyelitis: Debridement versus debridement plus Osteoset T pellets. Acta Orthop. Belg. 2007, 73, 238. [Google Scholar]
- Ferguson, J.Y.; Dudareva, M.; Riley, N.D.; Stubbs, D.; Atkins, B.L.; McNally, M.A. The use of a biodegradable antibiotic-loaded calcium sulphate carrier containing tobramycin for the treatment of chronic osteomyelitis: A series of 195 cases. Bone Jt. J. 2014, 96, 829–836. [Google Scholar] [CrossRef]
- Ferguson, J.Y.; Mifsud, M.; Stubbs, D.; McNally, M.A. The choice of local antibiotic carrier significantly affects outcome in treatment of chronic bone infection. Orthop. Proc. 2018, 100, 3. [Google Scholar]
- Karr, J.C. Management of a Diabetic Patient Presenting with Forefoot Osteomyelitis: The use of Cerament™| Bone Void Filler Impregnated with Vancomycin—An Off Label Use. J. Diabet. Foot Complicat. 2009, 1, 94–100. [Google Scholar]
- Drampalos, E.; Mohammad, H.R.; Kosmidis, C.; Balal, M.; Wong, J.; Pillai, A. Single stage treatment of diabetic calcaneal osteomyelitis with an absorbable gentamicin-loaded calcium sulphate/hydroxyapatite biocomposite: The Silo technique. Foot 2018, 34, 40–44. [Google Scholar] [CrossRef]
- Niazi, N.S.; Drampalos, E.; Morrissey, N.; Jahangir, N.; Wee, A.; Pillai, A. Adjuvant antibiotic loaded bio composite in the management of diabetic foot osteomyelitis—A multicentre study. Foot 2019, 39, 22–27. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion criteria |
|---|
|
|
|
| Exclusion criteria |
|
|
|
| Region | Sex | Age | Microbiology | Sensitive to Gentamicin | Systemic Antibiotic Regime | Relevant Comorbidities | Time to Healing [months] |
|---|---|---|---|---|---|---|---|
| Calcaneal | M | 59 | S. aureus | Yes | Sulfamethoxazole/Trimethoprim, Levofloxacin | Diabetes type 2, arterial hypertension, diabetic neuropathy, Charcot foot | 7.3 |
| Calcaneal | M | 69 | S. aureus | Yes | Sulfamethoxazole/Trimethoprim, Levofloxacin | Diabetes type 2, hypertension, dyslipidaemia | 4.5 |
| Calcaneal | M | 79 | S. aureus | Yes | Sulfamethoxazole/Trimethoprim, Levofloxacin | Diabetes type 2, renal impairment | Pat. died |
| Calcaneal | F | 54 | S. aureus | Yes | Sulfamethoxazole/Trimethoprim, Levofloxacin | Diabetes type 2, chronic atrial fibrillation, hypertension, kidney disease, Charcot foot | 9.7 |
| Calcaneal | M | 65 | S. aureus | Yes | Sulfamethoxazole/Trimethoprim, Levofloxacin | Diabetes type 2, hypertension, chronic kidney disease, ischemic coronary heart disease | Lost-to-follow-up (reason unknown) |
| Calcaneal | M | 49 | No growth | - | Ciprofloxacin, Cefepime | Dyslipidaemia | 14.9 |
| Calcaneal | M | 62 | P. aeruginosa | Yes | Piperacillin/Tazobactam | Diabetes type 2, coronary heart disease, chronic kidney disease, arterial hypertension, chronic hepatopathy | Not healed, below-knee-amputation |
| Calcaneal | M | 60 | P. aeruginosa | Yes | Sulfamethoxazole/Trimethoprim, Ceftazidime | Diabetes type 2, HIV, neuro-vasculopathy, chronic renal insufficiency, hypertension | 9.5 |
| Calcaneal | M | 49 | C. striatum | Not tested | Ciprofloxacin, Teicoplanin | Diabetes type 2, chronic renal insufficiency, arterial hypertension, dyslipidaemia, diabetic neuropathy, critical limb ischemia | 12.7 |
| Calcaneal | M | 74 | S. aureus | Resistant | Sulfamethoxazole/Trimethoprim, Ciprofloxacin | Critical limb ischemia, foot deformity, ischemic cardiomyopathy, hypertension, renal impairment | Not healed; suggested amputation |
| Metatarsal | M | 70 | S. xylosus | Yes | Teicoplanin, Amoxicillin/Clavulanic Acid | Diabetes type 2, arterial hypertension, ischemic cardiomyopathy | 2.3 |
| Metatarsal | M | 70 | E. coli, C. minutissimum | Resistant/not tested | Sulfamethoxazole/Trimethoprim, Piperacillin/Tazobactam | Diabetes type 2, arterial hypertension, ischemic cardiomyopathy | 5 |
| Metatarsal | F | 71 | S. aureus | Yes | Sulfamethoxazole/Trimethoprim, Levofloxacin | Diabetes type 2, hypertension | 4.5 |
| Metatarsal | M | 54 | S. agalactiae, S. epidermidis | Not tested/Yes | Sulfamethoxazole/Trimethoprim, Ciprofloxacin | Diabetes type 2, hypertension, dyslipidaemia, | 9.5 |
| Metatarsal | F | 75 | S. aureus | Yes | Teicoplanin, Amoxicillin/Clavulanic Acid | Diabetes type 2, critical limb ischemia, ischemic heart disease, arterial hypertension, atrial fibrillation | 1.9 |
| Metatarsal | M | 78 | S. aureus | Yes | Sulfamethoxazole/Trimethoprim, Levofloxacin | Diabetes type 2, arterial hypertension, ictus cerebri, peripheral arterial disease | 3.9 |
| Distal Tarsus/Talus | M | 52 | S. aureus | Yes | Sulfamethoxazole/Trimethoprim, Levofloxacin | Diabetes type 1, arterial hypertension, peripheral arterial disease, chronic kidney disease | 7.5 |
| Distal Tarsus/Talus | F | 46 | S. aureus | Yes | Sulfamethoxazole/Trimethoprim, Levofloxacin | Diabetes type 1, hypothyroidism, myasthenia gravis | 13.2 |
| Distal Tarsus/Talus | F | 68 | S. aureus | Yes | Sulfamethoxazole/Trimethoprim, Levofloxacin | Diabetes type 2, hypertension, chronic kidney disease | 7.4 |
| Distal Tarsus/Talus | F | 44 | S. aureus | Yes | Sulfamethoxazole/Trimethoprim, Levofloxacin | Diabetes type 1, arterial hypertension, chronic kidney disease | 8.2 |
| Distal Tarsus/Talus | F | 51 | S. aureus | Yes | Sulfamethoxazole/Trimethoprim, Levofloxacin | Diabetes type 2, arterial hypertension, atrial fibrillation | Not healed |
| Distal Tarsus/Talus | M | 48 | S. maltophilia, S. aureus | Resistant/Yes | Sulfamethoxazole/Trimethoprim, Levofloxacin | Diabetes type 2 | 4.5 |
| Distal Tarsus/Talus | M | 60 | No growth | - | Teicoplanin, Ciprofloxacin | Diabetes type 2, arterial hypertension, cardiopathy ischemia, dyslipidemia, peripheral arterial disease | 5.4 |
| Distal Tarsus/Talus | F | 69 | E. faecalis, A. baumannii, S. aureus | Yes/Yes/Yes | Teicoplanin, Amoxicillin/Clavulanic Acid | Diabetes type 2, atrial fibrillation. Charcot foot, dyslipidaemia | Not healed |
| Distal Tarsus/Talus | M | 73 | No growth | - | Levofloxacin, Clindamycin | Diabetes type 2, arterial hypertension, Dyslipidemia, chronic kidney disease, Charcot foot | Not healed, Chopart amputation |
| Distal Tarsus/Talus | M | 64 | Corynebacterium spp. | Not tested | Amoxicillin/Clavulanic Acid | Diabetes type 1, ischemic cardiopathy | 9.5 |
| Distal Tarsus/Talus | M | 76 | S. lugdunensis | Yes | Teicoplanin, Ciprofloxacin | Diabetes type 2, ischemic cardiopathy, hypertension, cardiac failure, atrial fibrillation, dyslipidaemia, peripheral arterial disease | Not healed, below-knee-amputation |
| Distal Tarsus/Talus | M | 67 | No growth | - | Ciprofloxacin | Diabetes type 2, arterial hypertension, Charcot foot | 0.1 |
| Distal Tarsus/Talus | M | 76 | Morganella morganii, S. agaleactie, S. aureus | Yes/not tested/yes | Ciprofloxacin, Vancomycin | Diabetes type 2, hypertension, cirrhosis, peripheral arterial disease | 2.4 |
| Distal Tarsus/Talus | M | 69 | E. faecalis, A. baumannii | Yes/Yes | Teicoplanin, Ciprofloxacin | Diabetes type 2, Charcot foot, arterial hypertension, dyslipidaemia | 9.5 |
| Distal Tarsus/Talus | M | 65 | E. faecalis, E. coli | Yes/Yes | Amoxicillin/Clavulanic Acid | Diabetes type 2, coronary heart disease, hypertension, critical limb ischemia, Charcot foot | 9.5 |
| Distal Tarsus/Talus | F | 70 | Enterococcus spp., P.aeruginosa | Resistant/resistant | Amoxicillin/Clavulanic Acid | Diabetes type 2, chronic kidney disease, hypertension, Charcot foot | 9.5 |
| Distal Tarsus/Talus | M | 69 | A. baumannii | Resistant | Rifampicin, Colistin | Diabetes type 2, atrial fibrillation, hypertension, ischemic cardiopathy, critical limb ischemia | 9.5 |
| Distal Tarsus/Talus | M | 53 | No growth | - | Sulfamethoxazole/Trimethoprim, Ciprofloxacin | Diabetes type 2, neuropathy | Lost-to-follow-up (no information) |
| Distal Tarsus/Talus | M | 75 | No growth | - | Levofloxacin | Diabetes type 2, hypertension, critical limb ischemia | 4.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Whisstock, C.; Volpe, A.; Ninkovic, S.; Marin, M.; Meloni, M.; Bruseghin, M.; Boschetti, G.; Brocco, E. Multidisciplinary Approach for the Management and Treatment of Diabetic Foot Infections with a Resorbable, Gentamicin-Loaded Bone Graft Substitute. J. Clin. Med. 2020, 9, 3586. https://doi.org/10.3390/jcm9113586
Whisstock C, Volpe A, Ninkovic S, Marin M, Meloni M, Bruseghin M, Boschetti G, Brocco E. Multidisciplinary Approach for the Management and Treatment of Diabetic Foot Infections with a Resorbable, Gentamicin-Loaded Bone Graft Substitute. Journal of Clinical Medicine. 2020; 9(11):3586. https://doi.org/10.3390/jcm9113586
Chicago/Turabian StyleWhisstock, Christine, Antonio Volpe, Sasa Ninkovic, Mariagrazia Marin, Marco Meloni, Marino Bruseghin, Giovanni Boschetti, and Enrico Brocco. 2020. "Multidisciplinary Approach for the Management and Treatment of Diabetic Foot Infections with a Resorbable, Gentamicin-Loaded Bone Graft Substitute" Journal of Clinical Medicine 9, no. 11: 3586. https://doi.org/10.3390/jcm9113586
APA StyleWhisstock, C., Volpe, A., Ninkovic, S., Marin, M., Meloni, M., Bruseghin, M., Boschetti, G., & Brocco, E. (2020). Multidisciplinary Approach for the Management and Treatment of Diabetic Foot Infections with a Resorbable, Gentamicin-Loaded Bone Graft Substitute. Journal of Clinical Medicine, 9(11), 3586. https://doi.org/10.3390/jcm9113586